
Abstract
Objective
The link between central adiposity and osteopenia has not been extensively studied in Latina women. In particular, the association between abdominal weight and bone mineral content (BMC) and bone mineral density (BMD), independent of total weight and aerobic capacity, remains uncertain, especially in overweight and obese individuals.
Methods
Trunk weight, total body fat mass, fat-free mass, BMC, and BMD of 33 premenopausal Latina women age 22 to 51 years from Los Angeles, California were measured using dual-energy X-ray absorptiometry (DXA). Waist circumference (WC) was measured without clothing at the smallest circumference of the torso. Peak aerobic capacity (peak VO2) was determined by treadmill ergometry with direct measurement of oxygen consumption.
Results
Partial correlations controlling for total body fat mass, fat-free mass, and peak VO2 revealed a significant inverse relationship between BMC and WC (r = −0.54, P < 0.05) but not between BMD and WC (r = −0.18, P = 0.41). Similarly, while controlling for total body fat, fat-free mass, and peak VO2, BMC was inversely associated with trunk fat (r = −0.75, P < 0.001), with trunk lean (r = −0.61, P < 0.05) and with total trunk weight (r = −0.75, P < 0.001); results were non-significant for BMD. When these analyses were repeated separately in overweight (n = 10) versus in the obese (n = 18) women, inverse relationships between BMC and trunk fat as well as between BMC and total trunk weight became stronger in the obese compared with the overweight women.
Conclusion
Although general obesity may prevent osteoporosis, these findings suggest that abdominal obesity (ie, trunk weight) specifically and independently may adversely influence bone mass.
Introduction
In the decade between 2000 and 2010, more than half of the growth in the total population of the United States was due to the increase in the Latino population. 1 A recent study 2 has reported that Latinos living in the United States are more likely to be overweight and obese, physically inactive, and diabetic than are white or black adults. Furthermore, the continuing increases in overweight and obesity expected in other ethnic groups will also be observed in Latinos. 3 Research studies investigating the manifestations of a sedentary lifestyle and energy imbalance in Latinos are scarce. In particular, whether or not unhealthy fat accumulation in the abdomen is a risk factor for low bone mass has not been addressed extensively in Latina women, who are especially susceptible to the health burdens of obesity.
The protective influence of general overweight or obesity on BMC and BMD is well established. However, the role of abdominal fat independent of overall obesity has been much less scrutinized or understood. In our previous published work, we have shown that abdominal fat is inversely associated with BMC in African-American and white children 4 as well as in Latino children. 5 Similarly, in overweight and obese adolescents, Russell et al 6 and Pollock et al 7 found visceral fat to be a negative predictor of BMC and BMD. In Dutch adults, Zillikens et al 8 found inverse associations between waist-to-hip ratio and bone and in a sample of Puerto Ricans. Bhupathiraju et al 9 concluded that higher abdominal fat is associated with poor bone health. Furthermore, in a small group of obese premenopausal women in the Boston area, Bredella et al 10 found that visceral adipose tissue is inversely associated with BMD. However, in each of their analyses, none of these studies adjusted for physical activity or aerobic fitness, which are important predictors of BMC and BMD as well as that of overweight and android body habitus. Therefore, in this study, the aim was to take this important confounder of body weight and bone mass into account. It was hypothesized that independent of fat mass, fat-free mass, and aerobic capacity, abdominal obesity is inversely associated with BMC and BMD in a group of premenopausal overweight and obese Latina women. Moreover, we believe that any observed inverse relationship between BMC/BMD and abdominal obesity will be exacerbated in the obese group compared with the overweight group.
Materials
Subject description
Thirty-nine Latina women were recruited through the elementary school of a low income Latino community in the County of Los Angeles in Southern California for the purpose of participating in a pilot study assessing the feasibility of a family-based health risk reduction program. Subjects underwent a screening procedure consisting of a telephone interview, health history questionnaire, and physical examination by a board-certified physician. Volunteers were invited to participate if they had no physical disability or chronic systemic illness.
The University of Southern California Institutional Review Board approved study protocols. Written informed consent was required to participate. In order to convey the intended messages, consent forms and questionnaires were written or compiled in English, and then translated to Spanish and back-translated into English by professional translators. Participants were given the option of receiving materials in either English or Spanish. Eighty-nine percent chose the Spanish-language option.
One woman was excluded because she indicated she might be pregnant. From the remaining 38 who were tested, 5 were postmenopausal and were excluded from the data analyses reported here. The current report is based on data collected from 33 premenopausal women between the ages of 22 and 51 (mean, 36.5 years).
Bone mineral content and density
Whole body DXA scans (Hologic QDR-1500, software version 7.10, Hologic Inc, Waltham, MA) were performed to provide whole body BMC (grams) and BMD (grams/cm2). Whole body scans require the subject to be placed supine with the arms and legs positioned according to the manufacturer's specifications. Scans took 15 minutes. Quality control was performed daily using a phantom. Measurements were maintained within the manufacturers precision standards of ≤1.5%. Reproducibility of BMD values, assessed in ten healthy volunteers, ranged from 0.8% to 2.0%.
Anthropometric measurements
Weight was measured in kilograms using a Healthometer calibrated scale (Continental Scale Corporation, Bridgeview, IL). Subjects were weighed in light clothing without shoes; weight was recorded to the nearest 0.1 kg. Height was measured by a stadiometer and recorded to the nearest 0.1 centimeters. Subjects were measured barefoot or wearing thin socks. The ratio of body weight to height squared (kg/m2) was used to calculate body mass index (BMI). Overweight was defined as BMI values between 25 and 29.9 kg/m2; obesity was defined as BMIs greater than or equal to 30 kg/m2. 11
Waist circumference was measured at the smallest circumference of the torso, which is at the level of the natural waist, while hip circumference was measured at the level of maximum extension of the buttocks posteriorly 12 ; values were recorded to the nearest 0.1 centimeters. To ensure correct positioning of tape, subjects wore no clothing except underwear. Waist-to-hip ratio (WHR) was calculated by dividing waist circumference by hip circumference.
Aerobic Capacity
Peak VO2 was determined using a continuous, incremental protocol on a motorized treadmill. The initial speed and grade were 2.5 mph and 0%, respectively, with increases of 0.5 mph and 2% every 2 minutes of exercise. The volume of expired air, volume of oxygen consumption, and volume of carbon dioxide production were determined by SensorMedics metabolic system (SensorMedics Corporation, Yorba Linda, CA). Subjects exercised to volitional fatigue, with 12-lead electrocardiogram (EKG) monitoring heart rate taken at the end of each minute during exercise and at peak VO2 for determination of HRmax. Peak VO2 was said to be achieved if the test met two of the following criteria: (1) respiratory exchange ratio (RER) value was greater than 1.05, (2) heart rate = ±10 bpm of the age-predicted HRmax, or (3) a plateau in VO2 was reached with increasing workloads. Criteria for terminating the test prior to completion included indications of distress, arrhythmia, or S-T abnormalities. Because the third criteria (plateau or leveling off in oxygen uptake) was not met in every subject, a “true VO2max” was not achieved and the tests were therefore called “peak VO2.” All electrocardiographic tracings and metabolic system outputs were reviewed by the same investigator (AA).
Data Analysis
All analyses were performed using SPSS version 20.0 (SPSS Inc, Chicago, IL), with a type I error set at P < 0.05. As determined by Kolmogorov-Smirnov test of normality, BMC and BMD were normally distributed and no transformations were necessary. Descriptive statistics, Pearson and partial correlations were used to estimate the effect of variables on the dependent variables, BMC and BMD.
Results
Mean and standard deviations of participant characteristics are shown in Table 1. The youngest woman was 22 years old; the oldest was 51. Mean age was 36.5 years. Mean BMI was 31.1 kg/m2 with a median of 30.5 kg/m2. Only 5 (15%) women had a BMI < 25 kg/m2, 10 (30%) women were overweight (BMI ≥ 25 to 30 kg/m2), and another 18 (55%) were obese (BMI > 30 kg/m2). Mean waist circumference was 91.4 cm with a range of 67 cm to 111 cm. Mean hip circumference was 109.1 cm with a range of 75 cm to 138 cm. Mean WHR was 0.84. Mean fat-free mass was 44.3 kg with a range of 30.9 kg to 59.0 kg. Mean fat mass was 28.5 kg with a range of 13.8 kg to 55.7 kg. Mean percent fat was 36.9%. Peak VO2 had a mean of 26.5 mL • kg–1 • min–1 with a range of 15.8 mL • kg–1 • min–1 to 48.9 mL • kg–1 • min–1. Mean trunk fat and mean trunk lean were 12.9 kg and 23.9 kg, respectively. Mean of total trunk weight was 36.8 kg with a range of 23.0 kg to 53.2 kg. Mean of total body BMC and BMD were 2348.8 grams and 1.121 g/cm2, respectively.
Descriptive characteristics (mean ± SD).

The strongest correlates (Table 2) of total body BMC and BMD were total body fat mass (r = 0.84 with BMC; r = 0.69 with BMD), BMI (r = 0.71 with BMC; r = 0.66 with BMD), trunk fat (r = 0.71 with BMC; r = 0.63 with BMD), and total trunk weight (r = 0.68 with BMC; r = 0.66 with BMD).
Pearson correlations with BMC and BMD.
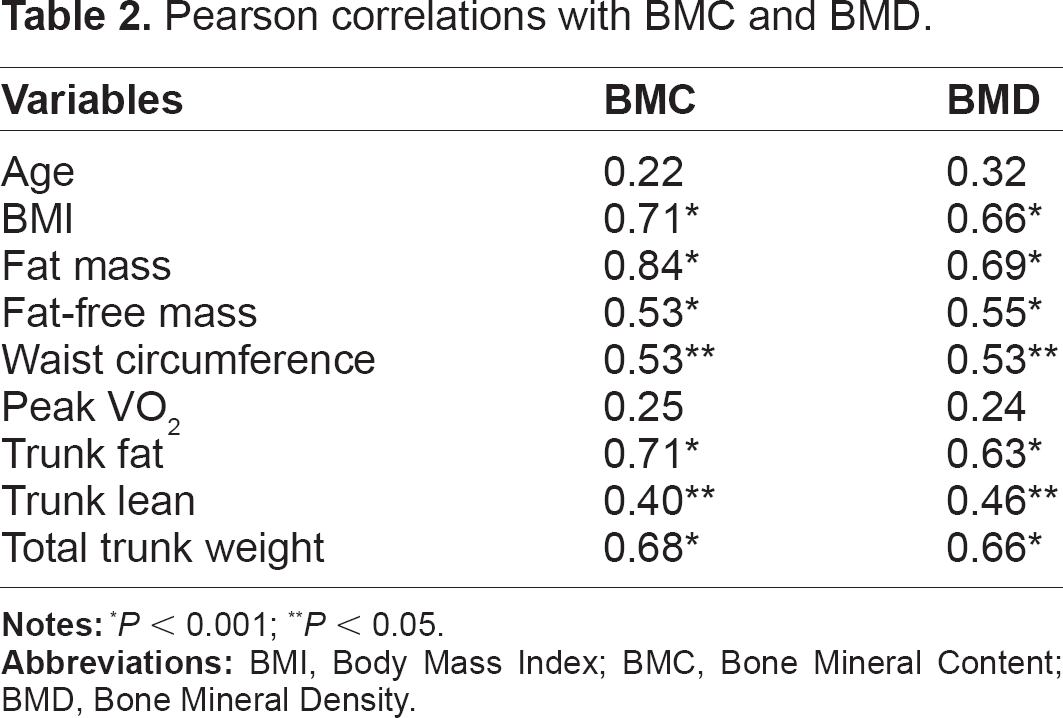
P < 0.001;
P < 0.05.
As shown in Table 3, partial correlations controlling for total body fat mass, fat-free mass, and peak VO2 revealed a significant inverse relationship between BMC and waist circumference (r = −0.54, P < 0.05) but not between BMD and waist circumference
Partial correlations controlling for fat, fat-free mass, and aerobic capacity.
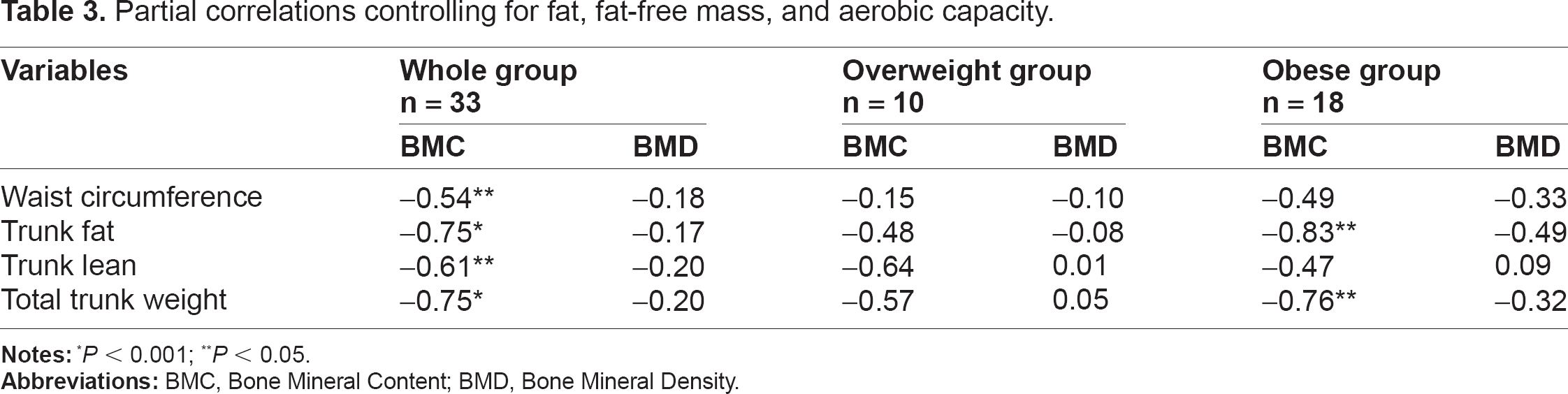
P < 0.001;
P < 0.05.
Discussion
A previous study 13 by our group examining the significant predictors of bone density in these Latina women revealed that fat mass, fat-free mass, and aerobic capacity explain 55%, 10%, and 8% of the variance in BMD, respectively. Also, when evaluating coronary artery disease risk factors in these same women, 14 peak VO2 was negatively correlated with general obesity (r = −0.65) and with central adiposity (r = −0.58). In addition, we showed 14 that higher levels of peak VO2 were accompanied by lower levels of BMI and waist circumference. For these reasons, to test the hypothesis that abdominal fat is inversely associated with BMC or BMD in these women, our analyses here carefully adjusted for the important predictors (fat mass, fat-free mass, and aerobic capacity). With this adjustment, a significant inverse relationship between BMC and waist circumference but not between BMD and WC was found (Table 3). Similarly, while controlling for the predictors, BMC was inversely associated with trunk fat, with trunk lean, and with total trunk weight; results were nonsignificant for BMD (Table 3). Witzke and Snow 15 have also found a stronger BMC model compared with a BMD model for anthropometric measures, leg power, and leg strength in adolescent girls. Similarly, in 400 postmenopausal African-American women, we 16 previously found a stronger BMC model compared with a BMD model for age, resting energy expenditure, and grip strength. This is plausible because skeletal content (ie, BMC) is influenced by factors that track into adulthood more so than skeletal density (ie, BMD). 17
The findings of this study confirm the notion that abdominal fat appears to have a strong inverse association with bone mass that is beyond the established and simple effect of mechanical loading. Production of proinflammatory molecules such as IL-6 and TNF-α has been proposed as one possible mechanism explaining the adverse independent role of abdominal fat on bone mass as the release of these inflammatory adipocytes seems to be enhanced in obese individuals. 18 In addition, abdominal fat is known to be more metabolically and biologically active, and many of the hormones and cytokines that affect bone metabolism are produced by fat in the central region. Bredella et al 10 and Afghani and Goran 5 concluded that IGF-I and leptin, respectively, may be the mediators of the deleterious effects of abdominal fat on bone. Therefore, since the inverse relationships found were independent of general obesity (Table 3), they have to be explained by other factors (eg, adipocytes, hormones, and cytokines) and not simply because of a load-bearing phenomenon on the skeleton. The fact that the inverse associations were exacerbated (Table 3) in the obese women compared with the overweight women confirms these conclusions.
Regarding recruitment of this population, it is noteworthy that we faced several barriers similar to those experienced by others who had minority inclusion in their research. Naranjo and Dirksen, 19 in a study of breast cancer survivors, encountered a high refusal rate and found culture to be contributing to the challenge of Hispanic women recruitment. Similarly, in this group of Latina women of low socioeconomic status, possible factors that played a role in recruitment and retention were fear of loss of health benefits (ie, Medicaid), inability to afford child care or transportation, immigration status, fear of deportation, and the need to work overtime or hold additional jobs when data were being collected. Because of the challenges faced with this population, time with each subject was limited and performing separate spine and hip scans was not possible. Trabecular bone (lumbar spine) has been shown to be more sensitive to metabolic changes 20 compared with cortical bone (hip). Furthermore, there are differences in the timing of bone loss in healthy women, trabecular bone diminishing with every decade of life but cortical bone levels being similar in the third, fourth, and fifth decades. 21 Therefore, although it would seem more logical that trabecular bone would be more sensitive to metabolic changes in these Latina women, measurement of both cortical and trabecular bone is necessary in our future work.
Regarding the abdominal fat measures, because waist circumference and DXA were used, we were unable to differentiate between visceral and subcutaneous fat that could be obtained from computed tomography. However, our measures are highly correlated with those obtained by CT scans. In one study
22
of 29 adults, waist circumference was highly correlated with CT-measured visceral fat (r = 0.85) as well as with deep subcutaneous fat (r = 0.54). Similarly, a study
23
in adolescent girls has shown that percentage trunk fat from DXA is significantly associated with visceral
Because this study was cross-sectional in nature, inferences regarding causality cannot be made. However, encouraging overweight and obese Latina women to exercise on a treadmill to their maximal effort was a challenge that ultimately became the strength of this study. Attempts should be made to replicate this methodology, and results from larger minority populations are warranted. In conclusion, the findings of this study support and underscore the adverse role of android body habitus on not only increasing the risk for cardiovascular disease and diabetes (as previously documented) but also the risk of osteopenia. Strategies and programs to prevent and treat the current crisis of abdominal obesity are urgently needed.
Footnotes
Author Contributions
Conceived and designed the experiments: AA. Analysed the data: AA. Wrote the first draft of the manuscript: AA. Contributed to the writing of the manuscript: AA. Agree with manuscript results and conclusions: AA. Jointly developed the structure and arguments for the paper: AA. Made critical revisions and approved final version: AA. All authors reviewed and approved of the final manuscript.
Funding
Author(s) disclose no funding sources.
Competing Interests
Author(s) disclose no potential conflicts of interest.
Disclosures and Ethics
As a requirement of publication author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest. Provenance: the authors were invited to submit this paper.