
Abstract
Following legal recognition of marriages for same-sex couples, new topics have emerged in debates over LGBT rights. While numerous studies of public opinion about gay and transgender rights have been examined, some emergent issues remain underexamined. Two prominent issues are conversion therapy and denials of service based on religious beliefs in a variety of settings. These areas of LGBT rights are dynamic, with some states recently banning conversion therapy on minors, the Trump Administration’s guidance on denials of service by health professionals, and some states funding adoption and foster agencies that refuse to provide services to same-sex couples and LGBT adults. In this study, we assess factors associated with public attitudes on these issues. While we find patterns that are consistent with previous studies, we also find inconsistencies when examining the effects of age, race, partisanship, educational attainment, and interpersonal contact. We further find that being a parent moderates the effects of interpersonal contact. Sometimes the moderated contact effects are large and positive but other times contact effects are negative. The contact effect depends on the particular type of contact such as with LGB people, transgender people, or knowing parents who have a transgender child.
Introduction
Since same-sex marriage was legalized by the Supreme Court of the United States, the number of policies proposed that affect lesbian, gay, bisexual, and transgender (LGBT) populations has grown in state legislatures. In 2014, there were 45 bills introduced that affect LGBT rights in state legislatures compared to 110 bills in 2016 (ACLU, 2020a). These policies include protections from discrimination based on sexual orientation and gender identity (e.g., state bills and the federal Equality Act), bills to prohibit or support access to bathrooms and locker rooms that align with gender identity versus sex assigned at birth, and bills to limit access to gender-affirming medical care for transgender minors (ACLU, 2020b). These emergent policies create open questions about public opinion, as opinion on LGBT rights generally corresponds with policies that are enacted (Flores et al., 2015; Lax and Phillips, 2009). Two policy areas that have seen a lot of activity at federal, state, and municipal levels are whether entities should have the ability to deny services to LGBT people for religious reasons and whether licensed health care providers should be barred from using conversion therapy on minors. In this study, we report findings on the attitudes of American adults about these issues.
A diverse set of policies enacted at various levels allow individuals, businesses, and non-profit organizations to deny services to others if the provision of services would violate the “sincerely held” religious beliefs or moral convictions of the provider. In 2019, the US Department of Housing and Human Services adopted an administrative regulation that enables agency-funded service providers to deny services to LGBT people based on their religious beliefs (US Department of Health and Human Services, 2019). Presently, 11 states permit child welfare agencies to deny placement and services; Kansas and Mississippi permit private businesses to deny services to same-sex couples; Mississippi and North Carolina allow state and local officials to decline to marry same-sex couples; and four states permit medical practitioners to decline to treat LGBT people based on religious objections (Movement Advancement Project, 2020b).
Conversion therapy refers to practices intended to change a person’s sexual orientation or gender identity (Glassgold et al., 2009). Conversion therapy may be conducted by licensed professionals in the context of providing health care or by religiously affiliated individuals in the context of religious practice (Morrow and Beckstead, 2004). These practices have been deemed harmful and ineffective to people (American Psychological Association, 2013; Jacob, 2015). Policies have been enacted at state and local levels to ban licensed health care providers from using this practice on minors who may not be able to decline such therapy (Byne, 2016). Presently, 21 states and the District of Columbia ban some or all licensed health care providers from using conversion therapy on minors (Movement Advancement Project, 2020a).
These policies have been underexamined in relation to public opinion. Peer-reviewed research on beliefs about the origins of sexual orientation and gender identity have found that people who embrace a biological basis tend to hold more favorable attitudes towards LGBT rights (Hegarty, 2020). However, opinions about the regulation of conversion therapy may be distinct from etiological beliefs, and our scan of the literature was unable to identify a single peer-reviewed article on the topic. Policies expanding religious refusals reflect a new development in the culture wars (Lewis, 2017). For example, Castle (2019) finds that segments of the public are polarized in their opinions on religious liberties largely driven by religion and partisanship. Thus, research is needed to develop a knowledge base.
In addition to demographics, we consider whether experiential characteristics such as having children and types of interpersonal contact affect social attitudes. Previous studies suggest the unique experience of being a parent should increase compassion for numerous LGBT rights that touch on the family (Becker, 2012), as both religious refusals and conversion therapy do. Previous studies also suggest that interpersonal contact with LGBT people may increase support for LGBT rights (Hoffarth and Hodson, 2020), and that such contact effects may be moderated by personal characteristics (Dyck and Pearson-Merkowitz, 2014; Skipworth et al., 2010). In their review, Hoffarth and Hodson (2020) note that there are vastly fewer studies examining contact beyond lesbians, gay men, and bisexuals; particularly for transgender and gender nonconforming persons. In the present study, we examine LGB contact and transgender contact. Our study further investigates the effect of people who know parents of transgender children. We further examine whether these contact effects are moderated by whether someone is a parent.
Interpersonal contact with LGB people tends to be a strong and positive correlate of attitudes towards LGBT rights (Hoffarth and Hodson, 2020), and people with predispositions to be more favorable to LGBT rights tend to have larger LGB contact effects while the effect is muted among those who lack those predispositions (Dyck and Pearson-Merkowitz, 2014; Skipworth et al., 2010). If compassion for family-related policies on LGBT rights is increased among parents, then we would expect to see LGB contact effects to be stronger for parents than those who are not. The literature on transgender contact is mixed with some studies finding no effect and others finding positive effects (Flores, 2015; Jones et al, 2018; Tadlock et al., 2017). Thus, we add to this discussion anticipating, similar to LGB contact, that parents will respond more strongly to having transgender contact. Parents who report knowing other parents who have a child who is transgender may have competing considerations—increased compassion for LGBT rights and personal thoughts on what it might be like if their own child is transgender and experiencing bullying, rejection, and consequent poor mental health (McGuire et al., 2010). When people have competing considerations, they may become more ambivalent about policies (Alvarez and Brehm, 2002), which results in greater response variability and expressions of non-attitudes. Thus, parents who know other parents with a transgender child may be more likely to not have an opinion on conversion therapy.
Data and method
We assessed public attitudes on conversion therapy and religious refusals from the Stonewall Anniversary Poll sponsored by Reuters and developed in collaboration with Ipsos. The poll was conducted online in English between 29 May and 5 June 2019, with 2237 US adults. Participants were randomly sampled from among Ipsos’ empaneled members and partner organization panels in addition to river sampling. Thus, the poll is a non-probability sample, which vary substantially in their representativeness to probability-based samples (Kennedy et al., 2016). The data are weighted to the 2016 American Community Survey for gender, age, region, race or ethnicity, and income. About 52% of the sample was female, 64% White, 12% Black, 16% Latino, 7% identified as LGBT, 44% were married, 27% had a college degree or more, 24% resided in rural places, and the average age was 47 years (SD = 16.6).
Dependent variables
The poll asked respondents their opinions on a variety of religious refusal scenarios with the following prompt: “Please indicate how much, if at all, you agree or disagree with the following statements.” Participants evaluated four scenarios in random order consisting of businesses, medical professionals, employers, and adoption or foster agencies denying service or employment on religious grounds (see Table 1). Most respondents did not agree with allowing religious refusals in any of these scenarios. We created a religious refusal index averaging these responses ranging from one to five with larger values indicating less support for permitting denials of service
Summary statistics of the dependent variables.

For conversion therapy, participants were first provided the following definition of conversion therapy: “Conversion therapy is when mental health practitioners try to change a LGBTQ person’s sexual orientation or gender identity.” Afterward, they were asked their opinions on whether conversion therapy should be legal or illegal to use on LGBTQ children under age 18 as in Table 1. A majority thought the practice should be illegal, while one-fourth did not know their opinions on the issue. By defining conversion therapy, there may have been an exposure effect that may lead people to be more opposed to the policy (e.g., Flores et al., 2018a, 2018b), but it seemed necessary to define the concept to ensure that people had sufficient information to render an opinion. The information was tailored to be as neutral as possible.
We show in SI 6 that opinions on these questions relate to opinions on other LGBT rights, though the correlations are not extremely large, suggesting there is variation that is unique to these questions. Importantly, regression models on those other variables explain more variation than on our current dependent variables, with traditional demographics consistently and strongly predicting attitudes (e.g., partisanship and educational attainment).
Analysis
The dependent variables are analyzed relying on the survey weights provided by Ipsos. A linear regression is used for the religious refusals index and a multinomial logistic regression is used to analyze conversion therapy attitudes. In addition to traditional respondent characteristics such as age, gender, race, education, LGBT identification, partisanship, marital status, and urbanicity, we include four additional measures. First, we consider whether the respondents have children living in their own home. In the present study, 27% of the sample currently has children in the home. Second and third, we consider whether the respondent personally knows an LGB person or a transgender person. Lewis (2011) shows that contact effects tend to be stronger and more consistently significant when the LGB person is a close friend or family member rather than a coworker or other acquaintance, so contact measures likely reflect a person’s social network as opposed to incidental encounters. The rates of interpersonal contact vary, with 77% of the respondents knowing an LGB person and 28% of the respondents knowing a transgender person. These prevalence rates are similar, though slightly lower than those found in other studies (LGB contact: 82%, MTV, 2017; transgender contact: 36%, Kaiser Family Foundation, 2020). Finally, we consider whether the respondent personally knows parents who are raising a transgender or gender nonconforming child. Like the contact hypothesis, personally knowing parents of transgender children may reduce stigma toward transgender people, particularly on issues affecting transgender youth. About 11% of the respondents reported knowing parents of a transgender child. This measure is unique to the current survey, so there are no comparable measures to validate it. Since both dependent variables consider children, it is important to consider how the experience of parenthood moderates experiences of interpersonal contact. Thus, we conduct additional models interacting having kids with our three contact measures.
Results
The regression results are provided in Table 2. Consistent with previous studies on LGBT rights, women, LGBT people, and more Democratic individuals are more opposed to permitting the denial of service to LGBTQ people (Model 1); whereas, those who are married, reside in a rural location or are more Republican are less opposed. Identifying as LGBT and partisanship have the largest effects of these characteristics with both representing about half a standard deviation change in attitudes from their minimum to maximum values. Racial or ethnic background, educational attainment, and age are not statistically significant. Parents are more opposed to permitting service denials. Those who personally know LGB people are more opposed to permitting service denials, while knowing transgender people or parents of transgender children are not statistically significant.
Regression results on attitudes about religious refusals and conversion therapy.

p < .10; * p < .05; ** p < .01; *** p < .001 (two-tailed).
DK: don’t know; MSE: mean square error.
The effect of interpersonal contact occasionally is moderated by whether the respondents have kids (Model 2). The main effect of LGB contact is positive and statistically significant, and the interaction, though not significant suggests that parents have a slightly stronger positive effect of LGB contact. The main effect of transgender contact is also positive and significant; however, the interactive effect is negative and significant, suggesting that parents who know a transgender person are more favorable of permitting service denials. Figure 1 conveys these patterns by predicting average scores on the religious refusals scale varying whether or not someone has kids across the different types of contact, holding all the other variables at their means. While scores are higher for having LGB contact than not regardless of having children, the predicted score is significantly greater for those who have children and have LGB contact than those who do not have children and have LGB contact (difference [diff.] = 0.26, se = .10, p < .01). Transgender contact increases scores for those without children, but there is no significant difference among parents. Whether or not knowing parents of a transgender child is no different among those without children, but among parents, there is a decrease in scores though not statistically significant (diff. = −0.26, se = .16, p = .11).
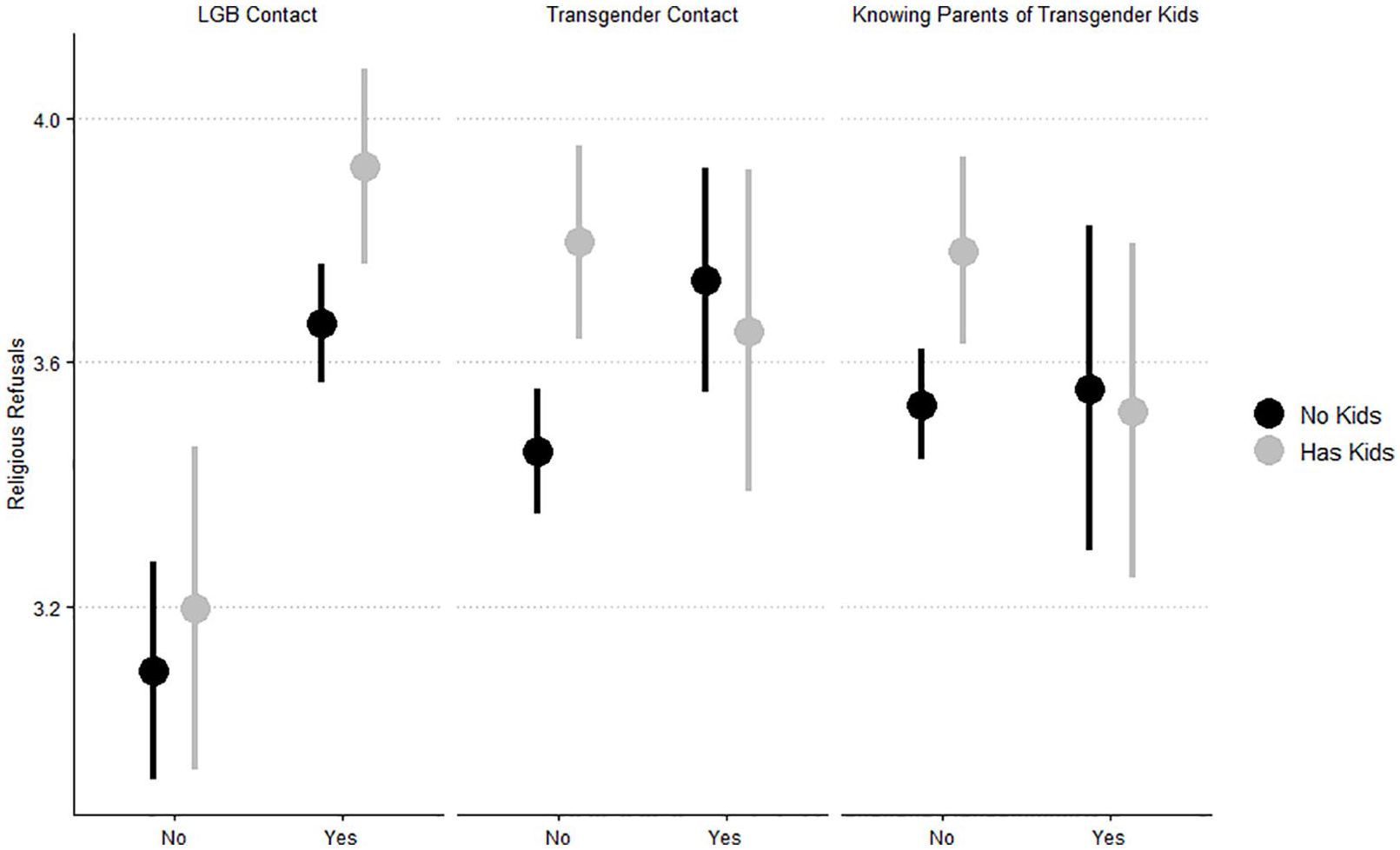
Predicted religious refusal scores by interpersonal contact and having kids.
Table 2 also contains regression results on conversion therapy relying on a multinomial logistic regression with the baseline category being that people think conversion therapy should be legal (Model 3). Women, LGBT people, and older individuals are more likely to think conversion therapy should be illegal, but Black people, Latinos, and married people are less likely to think conversion therapy should be illegal. Older individuals were more likely to not have an opinion on conversion therapy, but Black people, Latinos, married people, college graduates, and LGBT people were less likely to say they did not have an opinion. Partisanship and having kids did not relate to conversion therapy attitudes. LGB contact was positively associated with thinking conversion therapy should be illegal and negatively associated with not expressing an opinion.
The effect of interpersonal contact is also occasionally moderated by whether or not people have kids (Model 4). The main effect of LGB contact, while positive, is not statistically significant on expressions that conversion therapy should be illegal, suggesting that those who are not parents are not significantly affected by knowing an LGB person. The interaction effect is positive and significant, suggesting that parents who know LGB people are far more likely to think conversion therapy should be illegal. Transgender contact does not have a relationship with conversion therapy attitudes. Parents who know parents with a transgender child are more likely to not have an opinion on conversion therapy. Predicted probabilities are plotted in Figure 2 varying types of interpersonal contact and whether a person has kids. The most telling patterns are between those who know parents of transgender youth. While there is no difference between parents and non-parents in their probability of thinking that conversion therapy should be illegal among those who do not know parents of transgender youth, there is a significant gap among those who do with parents less likely to think conversion therapy should be legal than non-parents (diff. = −0.24, se = .10, p < .05). The decrease in the probability in thinking conversion therapy should be illegal seems to be associated with an increase in not having an opinion on the issue. There is an increase in the probability of not having an opinion between parents who know parents of transgender youth and parents who do not (diff. = 0.18, se = .10, p = .07).

Predicted probabilities of attitudes about conversion therapy by interpersonal contact and having kids.
Discussion
Following the enactment of marriage equality, new issues have risen to the top of the LGBT policy agenda, though studies of public opinion have lagged. Overall, we tend to find patterns consistent with previous works on public opinion about LGBT rights. However, age, race, partisanship, educational attainment, and interpersonal contact were occasionally inconsistent.
Generally, older age cohorts are more opposed to LGBT rights than younger cohorts (Andersen and Fetner, 2008; Twenge et al., 2015). That we do not see any significant patterns for age on religious refusals is noteworthy. 1 We also observe positive effects of age on banning conversion therapy, suggesting that older individuals are more likely to think conversion therapy should be banned than younger individuals. Older individuals were also more likely to not express an opinion, which likely relates to these issues being relatively new, so there may be a greater lack of familiarity among older individuals.
Prior studies suggest racial and ethnic minorities are more socially conservative on numerous issues, including LGBT rights (Abrajano, 2010; Lewis, 2003). While we can only conjecture about the null effect of race or ethnicity on religious refusals, we suspect that the denial of service on religious grounds may have implications for the treatment of racial and ethnic minorities. For example, racial minority elected officials raised concerns about how these bills may allow certain religions aligned with white supremacist organizations to deny services to people of color. 2 Thus, permitting denials of service may be understood as categorical discrimination by racial and ethnic minorities. Religious refusal attitudes appear to be distinct from conversion therapy among Black people and Latinos. For the latter, there was consistently lower support for banning conversion therapy. While among white individuals, the predicted probability is 0.60 for conversion therapy to be illegal, those probabilities are 0.49 and 0.47 for Black people and Latinos, respectively.
It is surprising that partisanship did not have a significant role in predicting attitudes on conversion therapy, given how traditionally sorted partisans are on LGBT rights (e.g., Dyck and Pearson-Merkowitz, 2014). Many states, including “red states,” have recently banned conversion therapy, such as Utah in 2020, and most of this legislative activity has occurred following marriage equality with 19 out of the 21 states banning the practice after 2015 (Movement Advancement Project, 2020a). Perhaps conversion therapy has transcended partisanship, and perhaps there are value orientations that both Democrats and Republicans hold that can structure their attitudes to align on the conclusion that conversion therapy should be a banned practice.
We consistently find that interpersonal contact with LGB people is a strong predictor of pro-LGBTQ attitudes on both religious refusals and conversion therapy. This is consistent with numerous prior studies. Importantly, we tend to find LGB contact to be stronger among parents. Becker (2012) made the case that parenting should increase support for LGBTQ rights affecting family formation. We add to this by showing that not only the experience of parenting, but also the experience of interpersonal contact corresponds with greater support for LGBTQ rights. While we do not observe an overall significant effect of contact with transgender people, we do find that such contact increases favorable attitudes on banning conversion therapy among those who do not have kids. One potential explanation for these patterns is the way transgender rights are framed in the United States. Arguments in opposition to transgender rights frequently reference harms to children (Stone, 2019), so it may be the case that contact and being a parent create competing considerations. Similarly, we do not observe many significant patterns for people who know parents of transgender children. We do find that parents who know other parents who have a transgender child are more likely to express that they do not know their position on conversion therapy. This may be due to value conflict (Alvarez and Brehm, 2002) because of a parents’ role in the well-being of their children and the likely struggles the parents they know have a transgender child undergo combined with the struggles of the transgender child. Encountering these experiences as a parent may induce greater reflexive thinking about, “what if my child was transgender?”, which induces ambivalence on policies like conversion therapy. While not examined here, similar patterns may be present for people who know parents of a child who is LGB.
The present study uncovered unique insights into the factors that shape adult opinions on emergent issues in LGBT rights. It is limited in that the sample was not recruited in a traditional way, the questions asking about religious refusals were not counterbalanced, and we only had a single measure of conversion therapy attitudes. The cross-sectional and observational data also limited our ability to make causal claims. Importantly, there is the possibility that individuals who have contact experiences may have previously held more pro-LGBT views resulting in having a network that is inclusive of LGB and transgender people. A recent review highlights the promises and limitations of existing research on interpersonal contact (Paluck et al., 2019), though there typically tends to be a positive effect of contact. The close relationship between public opinion on LGBT rights and public policies in place that affect LGBT people warranted this initial assessment (Flores et al., 2015; Lax and Phillips, 2009). Future work should investigate whether the opinion-policy link exists on these emergent issues, and experimental studies may identify interventions that change opinions on these matters (e.g., Flores et al., 2018a, 2018b; Harrison and Michelson, 2017).
Following marriage equality, the movement for LGBT rights and its countermovement tactically innovated to address ongoing issues (Stone, 2012). For the LGBT rights movement this has included securing antidiscrimination protections and banning practices such as conversion therapy. The countermovement immediately following marriage equality pursued policies to protect religious freedoms, adopting a minority politics rights framework (Lewis, 2017). As public policy continues to develop, it is important to understand the attitudes of American adults and the factors that structure those attitudes.
Supplemental Material
Supporting_Information – Supplemental material for Public attitudes about emergent issues in LGBTQ rights: Conversion therapy and religious refusals
Supplemental material, Supporting_Information for Public attitudes about emergent issues in LGBTQ rights: Conversion therapy and religious refusals by Andrew R. Flores, Christy Mallory and Kerith J. Conron in Research & Politics
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental materials
Notes
Carnegie Corporation of New York Grant
The open access article processing charge (APC) for this article was waived due to a grant awarded to Research & Politics from Carnegie Corporation of New York under its ‘Bridging the Gap’ initiative.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.