
Abstract
Background and aims
Multiple medications are associated with an increased risk of incident hepatic encephalopathy. Despite this known risk, medications such as opioids, benzodiazepines, gabapentin/pregabalin, and/or proton pump inhibitors are increasingly prescribed to persons with cirrhosis. Deprescribing is a promising intervention to reduce the burden of hepatic encephalopathy. Given that deprescribing has not been trialed in cirrhosis, we evaluated the barriers and facilitators to safe and successful deprescribing in cirrhosis.
Methods
We conducted, transcribed, and analyzed semi-structured interviews using qualitative methodology with 22 subjects. This included eight patients with cirrhosis and recent use of opiates, benzodiazepines, gabapentin/Lyrica, and/or proton pump inhibitors as well as 14 providers (primary care, transplant surgery, transplant hepatology). Interviews explored opinions, behaviors, and understanding surrounding the risks and benefits of deprescribing.
Results
Major provider-specific barriers included deferred responsibility of the deprescribing process, knowledge gaps regarding the risk of hepatic encephalopathy associated with medications (e.g. proton pump inhibitors) as well as the safe method of deprescription (i.e. benzodiazepines), and time constraints. Patient-specific barriers included knowledge gaps regarding the cirrhosis-specific risks of their medications and anxiety about the recurrence of symptoms after medication discontinuation. Patients uniformly reported trust in their provider’s opinions on risks and wished for more comprehensive education during or after visits. Providers uniformly reported support for deprescription resources including pharmacist or nurse outreach.
Conclusion
Given knowledge of medication risks related to hepatic encephalopathy in patients with cirrhosis, deprescribing is universally seen as important. Knowledge gaps, inaction, and uncertainty regarding feasible alternatives prevent meaningful implementation of deprescription. Trials of protocolized pharmacy-based deprescribing outreach and patient-facing education on risks are warranted.
Key Summary
Summarize the established knowledge on this subject
Hepatic encephalopathy (HE) is a morbid complication of cirrhosis. The risk of HE may be increased by psychoactive medications and proton pump inhibitors. Deprescribing is felt to be a promising approach to HE prevention.
What are the significant and/or new findings of this study?
Patients are unaware of how their medications influence the risk of HE. Patients are willing to follow physician recommendations regarding deprescribing but are afraid of worsening symptoms. Physicians do not feel comfortable deprescribing opioids or benzodiazepines. Physicians do not feel responsible or equipped with the resources for deprescribing.
Introduction
Hepatic encephalopathy (HE) is a common and devastating complication of cirrhosis. HE occurs in up to 40% of patients with cirrhosis, diminishes health-related quality of life (HRQOL)1–3 and increases both hospitalizations 4 and mortality.4–6 Several classes of commonly prescribed medications influence the risk of HE episodes.7–9 These include benzodiazepines, gamma-aminobutyric acid (GABA)-ergics, opioids, and proton-pump inhibitors (PPIs).7–9
While patients with cirrhosis often have genuine indications for these medications, there are two problems. First, the risk-benefit of such medications changes for those with or at high-risk for HE. Second, there has been a recent and marked increase in prescriptions for medications linked to HE such as benzodiazepines, GABA-ergics, and PPIs. 9 From 2008–2014, we found that, among US Medicare enrollees with cirrhosis, the share of person-years with prescriptions for benzodiazepines, gabapentin, opioids, and PPIs rose by 242%, 210%, 124%, and 33%, respectively. 9 Safely deprescribing such medications is part of effective HE management. 10
Deprescribing is the deliberate process of discontinuing medications by the healthcare team with the intention of reducing risk or improving health outcomes. 11 In the general population, the vast majority of patients believe their medications are necessary but would stop if instructed. Deprescription for patients with cirrhosis, however, is hampered by a lack of data. Patient and provider attitudes/knowledge of its risks and benefits are unknown. The infrastructure for implementing safe deprescribing, particularly for benzodiazepines where there is a risk of severe withdrawal, is similarly lacking. Herein, we performed a qualitative study to characterize both prescriber and patient opinions and knowledge regarding the use and adverse effects of medications that influence the risk of HE in patients with cirrhosis.
Methods
Subject recruitment
We conducted a prospective qualitative study that aimed to recruit patients and providers for recorded semi-structured interviews between June–September 2019. First, we screened all appointments at the University of Michigan hepatology clinics for patients who had a history of decompensated cirrhosis and had an active prescription for benzodiazepines, gabapentin/pregabalin, opioids, or PPIs. Second, we used a stratified purposeful sampling approach to recruit clinicians including hepatologists, liver transplant surgeons, hospitalists, and primary care providers, non-randomly selecting participants thought to be representative of the intended patient or provider population. All interviews were conducted in-person or by phone, recorded, and transcribed verbatim by a transcription service. Written, informed consent was obtained from each patient in this study. This study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a priori approval by the institution's human research committee. This study was approved by the University of Michigan Ethical Review Board on 5/2/2019 (HUM00161296).
Interviews
A semi-structured interview guide was developed with the purpose of assessing the barriers, facilitators, and methods to overcoming challenges to deprescribing (Supplementary Material). The interview guide was developed by the study team according to the theoretical domains framework 9 and workshopped with experts in qualitative methodology. Patients and providers were asked open-ended interview questions by a single interviewer. The interviewer also documented detailed notes during all interviews, to be used in the event of poor audio quality.
During the interview, we sought to better understand patients’ and providers’ understanding of the risks, consequences, and prevention of HE, knowledge of the medications being explored, and experience with these medications. Patients were asked to recall any personal experiences involving these medications as well as discuss any provider education given regarding their uses. Similarly, we asked providers to describe their practice for prescribing these medications as well as the education that they provide to their patients during prescription. Both patients and providers were asked to provide feedback on barriers, facilitators, and potential methods to deprescribing.
Qualitative analytic approach
All interviews were recorded, transcribed verbatim, de-identified and analyzed systematically12–15 using an inductive approach that replicates well-established qualitative methodology.12–15 When analyzing the transcripts, our research team employed a three-step group coding process that was informed by experts in qualitative analysis. The three steps were: (a) developing the codebook, (b) coding (open and axial), and (c) determining themes and relationships. The codebook was developed by conducting a thorough review of transcripts to identify recurrent concepts and generate preliminary codes.12–15 The codebook was continuously refined and expanded in an iterative process to reflect emerging themes throughout the data collection and analysis phases. 10 The coding team developed open codes using six interviews separately on the NVivo software platform. 16 Axial coding categories (see Tables 1 and 2) were developed and we completed an inter-rater reliability exercise designed to ensure the consistent interpretation of each code. Once optimal agreement was achieved (kappa coefficient ≥0.60), the remainder of the coding was completed by a single coder. Once recurring themes and relationships were identified and characterized using exemplary quotes, a conceptual model displaying our theory of the primary barriers was developed (Figure 1).
Themes from patients.
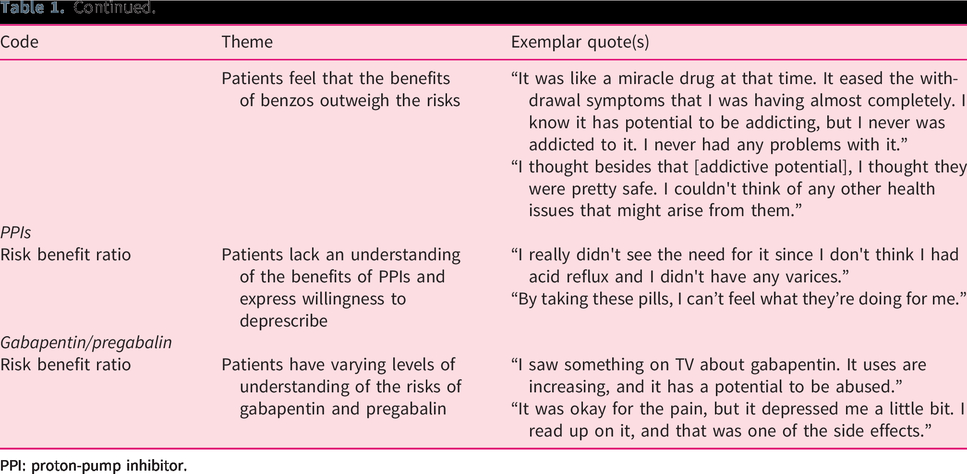
PPI: proton-pump inhibitor.
Quotes from providers about barriers, facilitators, and methods of deprescribing.
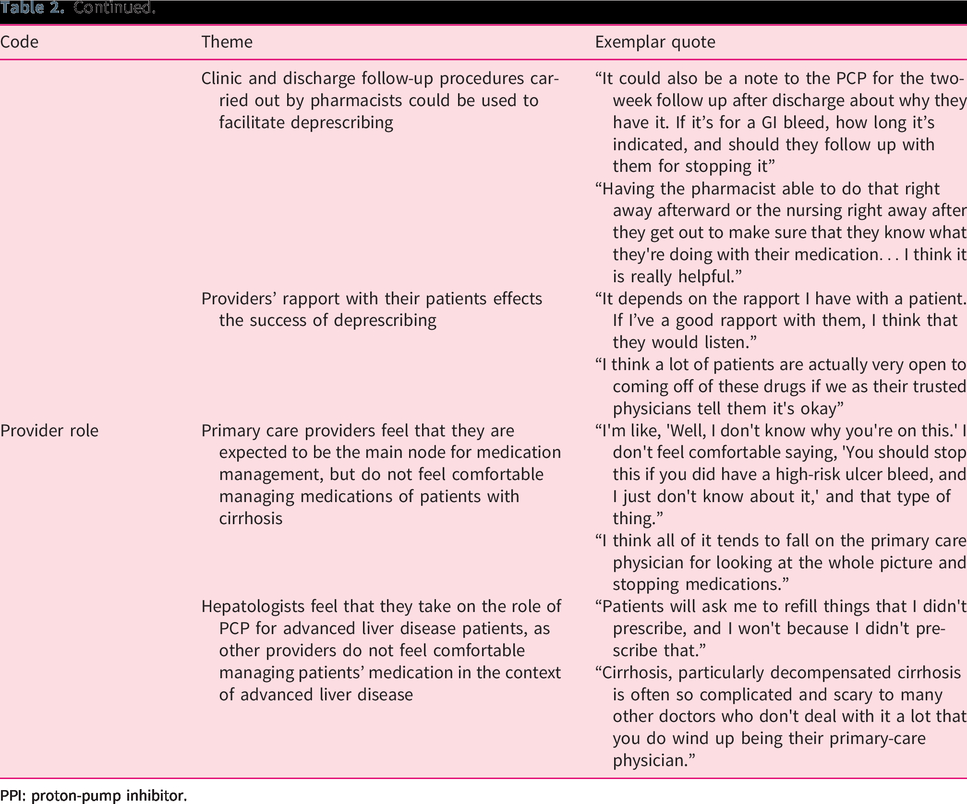
PPI: proton-pump inhibitor.
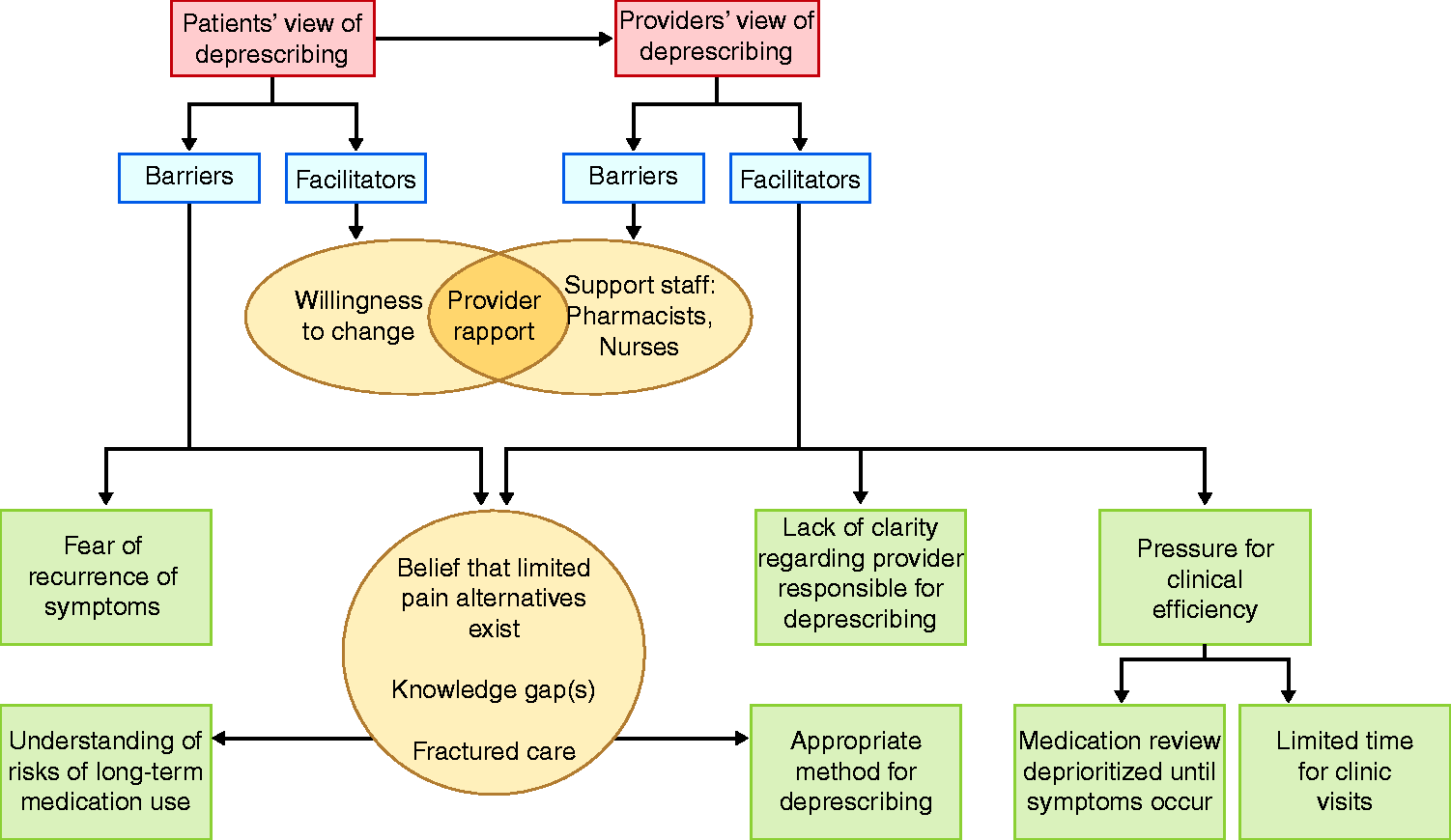
Conceptual model of barriers to deprescribing from patient and provider perspectives.
Results
We interviewed a total of 22 individuals. We contacted 19 providers, five declined (four primary care doctors, one hepatologist), and interviewed seven hepatologists (median experience 4 years, range 2–30), two transplant surgeons (12 and 13 years of experience), and five primary care physicians (median 5 years experience, range 3–15). We contacted 15 patients, two declined, and transcribed eight interviews. The patients were 50% female, average 52 ± 16 years old, and one (12.5%) had a college degree. The etiology of liver disease was alcohol-related in four (50%) patients and nonalcoholic fatty liver disease in two (25%) patients. The mean model for end-stage liver disease sodium (MELD-Na) was 13±4 and 75% had prior episodes of overt HE. The proportion of patients receiving prescriptions for gabapentin/pregabalin, opioids, PPIs, or benzodiazepines were 37.5%, 100%, 87.5%, and 62.5%, respectively. Of the eight patients interviewed, eight (100%), five (62.5%), eight (100%), and seven (87.5%) patients reported that they did not recall prior counseling on the risks (as they relate to HE) of gabapentin/pregabalin, opioids, PPIs, and benzodiazepine, respectively. Four (50%) patients had prior experience with deprescribing that was either self-initiated or initiated by their provider.
Overarching patient-reported themes
In Table 1 we characterize the major themes that emerged from transcripts of patient interviews. In general, patients report following doctors’ orders and adhering to all prescribed medications. One of the main drivers of this behavior was the belief that their prescribers adequately weighed the risks and benefits on an on-going basis, “I let him be in charge. I trust him in what he’s doing and saying.” Patients reported dismay when doctors disagreed about the risk/benefits of medications and did not communicate to resolve conflicts. However, if the hepatologist suggested significant risks of decompensation from one of their medications, patients would be willing to discontinue, for example saying “I’d stop ‘em all in a heartbeat,” or “But if somebody told me that, ‘Hey, that gabapentin is not making your liver–doing it any favors,’ okay, let’s get rid of it.” Most patients interviewed did not understand why they were prescribed PPIs. I really didn't need to be on that … It seemed like they just had a protocol that they followed. Then they just prescribed those drugs no matter what. I was prescribed on that from basically day one of my diagnosis to prevent varices or acid reflux that could cause varices, I guess.
Patients are unaware of the potential risk of HE associated with psychoactive medications and PPIs, “I thought besides that [addictive potential], I thought they were pretty safe. I couldn't think of any other health issues that might arise from them.” Patient understanding of risk appears to be couched in terms of laboratory patterns (e.g. model for end-stage liver disease (MELD) scores, liver enzymes), “I ask all the time, ‘Well, is there something else I could take … that’s not an opioid’ … it’s proven to be a fact … my numbers have not gone up.”
Patients who see strong benefits from a medications are hesitant regarding deprescribing. My anxiety was in the morning … I liked it [benzodiazepine] … It was like a miracle drug. If they were to take that pill away at bedtime, I would be devastated because I would be in real bad pain.
Overarching physician-reported themes
In Table 2 we characterize the major codes and themes that emerged from transcripts of physician interviews. We found that patients with cirrhosis are co-managed by multiple clinicians, none of whom feel comfortable deprescribing. One hepatologist mentioned “I generally defer that to primary care physician (PCP),” while another acknowledged “decompensated cirrhosis is often so complicated and scary to many other doctors who don't deal with it a lot that you do wind up being their primary-care physician.” Ownership is also deferred due to the perceived difficulty of the deprescribing conversation regarding medications with addictive potential, “Patients that have tried them are absolutely convinced they’re the only things that work, period.” Providers think it may be easier to deprescribe PPIs, “For benzos and narcotics, I think there will probably be more patient-attitude barriers or patients desiring to stay on these medications than for PPIs.”
Providers are less comfortable deprescribing for fear of unintended consequences, “I didn't know that you shouldn't pull people off benzos until I talked to our psychiatrist.” Additionally, providers have concerns about how to address symptoms that may return after medication discontinuation, “Pain is probably the most difficult thing to treat because we don’t have great options.” Providers do not believe effective alternative therapeutics exist, “Lotta patients can't take NSAIDs [non-steroidal anti-inflammatory drugs] because for cirrhotics, bleeding risks, and kidney function … so the option is taking a narcotic … or give them gabapentin.”
Physicians are generally aware of the risk of HE associated with medications. If an adverse event was attributed to a medication, providers feel comfortable stopping it. In contrast, pre-emptive deprescribing is felt to be a low priority. I know I overlook it all the time. When I don't overlook it is when there's a symptom, right? When a symptom comes up like they're more confused or they feel sleepier, then you start really looking at their med list.
Discussion
HE is a debilitating complication of cirrhosis with serious implications on hospitalizations, mortality, and quality of life. 3 It is known that episodes of HE are linked to opioids, benzodiazepines, gabapentin/pregabalin, and PPIs, 13 , 14 all of which are commonly, and increasingly, prescribed. 15 , 16 Deprescribing interventions can safely reduce polypharmacy for at-risk populations. 17 None, however, have been trialed in patients with cirrhosis. Additional data was needed to inform the needs of both patients and providers. We conducted the first qualitative assessment of provider and patient-level barriers and facilitators to deprescribing potentially harmful medications in cirrhosis. As summarized in Figure 1, we found that the barriers to deprescribing started with the delegation of responsibility and were further exacerbated by knowledge gaps and time constraints. In general, providers endorsed a reactive approach to medication risk management – removing a medication known to trigger HE in a given patient – rather than a proactive approach – stopping a medication with the potential to trigger HE. In Figure 2, we summarize some potentially successful deprescribing interventions that were identified to address these barriers.
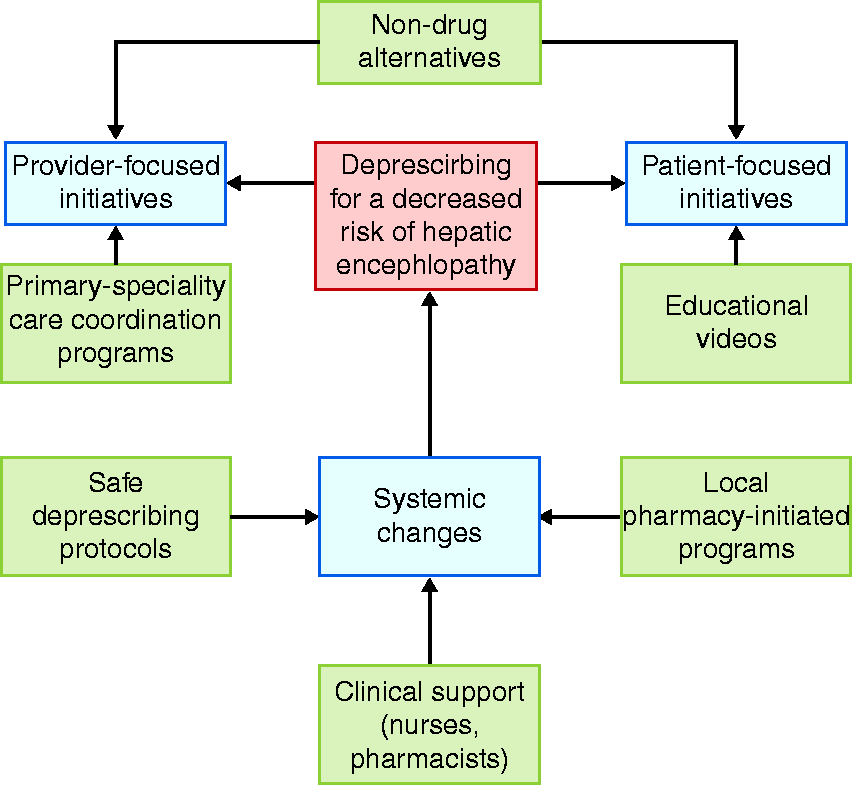
Conceptual model of solutions to overcome barriers to deprescribing.
Who owns medication risk management?
One of the most important barriers to deprescribing is determining the responsible party. Although some patients preferred the deprescribing process be led by their hepatologist, most welcomed involvement of all care-team members, including nurses and pharmacists. Consistent with prior studies, most felt the initial prescriber should manage or discontinue the medications in question. 18 In contrast, both patients and providers deferred deprescribing discussions in cirrhosis care to hepatologists owing to the complexity of cirrhosis. However, hepatologists and transplant surgeons felt ill-equipped for this responsibility. Conversations are often avoided due to perceived time constraints, fears of upsetting the patient, opinions that other topics are of higher priority, and discomfort around discussing sensitive or stigmatized medications. 19 The latter is further exacerbated in cirrhosis due to the high rates of comorbid substance abuse and psychiatric disorders. Our results, however, show that both patients and physicians value open communication in regard to medication safety and use. Time remains a major barrier. For these reasons, deprescribing efforts require either actively assuming responsibility for medication management (as in the case of a recent pharmacist-led trial) 17 or a behavioral intervention to encourage and support responsibility amongst hepatologists.
Knowledge gaps
Physicians are unsure how to safely discontinue medications and they fear unintended consequences. Sudden discontinuation of opiates can lead to unpleasant symptoms. An inappropriate tapering of benzodiazepines can be fatal. Patient knowledge gaps compound this problem. Patients remain unaware of the increased risk of incident HE that our queried medications carry. Patients report being informed by commercials and websites. However, these sources do not speak to the cirrhosis-specific risks. Furthermore, websites may contain incomplete or inaccurate information. Multiple methods are available to address the knowledge gaps preventing deprescribing. Targeted education will raise awareness of risks. 20 Shared decision-making aids may facilitate a tough discussion by adding structure to the discussion while clarifying risks. Even simply offering to discontinue a medication is sufficient. Three-quarters of residents of a nursing facility taking benzodiazepines agreed to attempt medication discontinuation when simply presented with this option by their provider. 21 By addressing the needs for both education and dedicated time, pharmacist-led initiatives may be the most promising. 17 , 22
Limited alternatives
Compounding the problem of knowledge barriers are patient and provider concerns about a recurrence of symptoms after describing, as well as uncertainty about the availability and efficacy of alternative interventions. This extends to the use of non-pharmacological interventions, such as mindfulness, support groups, and physical therapy, which have shown benefits in decreasing anxiety, reducing sleep disturbances, and alleviating chronic pain. 23 Patient engagement in the deprescribing process is diminished when there is limited information provided about the process of deprescribing and how recurrent symptoms will be managed. However, willingness to attempt deprescribing can be improved when patients have confidence in the tapering regimen, knowledge of the available alternatives, and reassurance that resumption of the original medication can be considered should alternatives fail. 21 Patients reported both a willingness to follow recommendations and hesitancy regarding worsening of symptoms. To assuage patient concerns, deprescription must be paired with a deliberate alternative approach to symptom control.
Contextual factors
Our data must be interpreted within the context of the study design. First, our single-center study may limit generalizability. Second, deprescribing patterns and behaviors were reported by physicians themselves and may have introduced attribution bias. It is plausible that other explanatory reasons for deprescribing behaviors were withheld due to concerns of how they would be perceived. Similarly, while most patients endorsed significant willingness to discuss the deprescribing of high-risk medications, this may not reflect their actual behaviors during real-time clinic discussions. Third, many risky medications may predate the diagnosis of cirrhosis. While PPIs are generally prescribed because of cirrhosis (even if inappropriately), opioids or benzodiazepines are not. Cirrhotic complications make long-standing medications riskier, but duration of use is a dimension that may have implicitly influenced discussions.
Conclusion
Despite mounting evidence of the increased risk of HE with the use of opioids, benzodiazepines, gabapentin/pregabalin, and PPIs, these medications remain commonly found on medication lists. Patients and providers mutually view deprescribing as an important clinical goal, but the process is hindered by deferred prescriber responsibility, uncertainty about the deprescribing process, and time constraints. Deprescribing interventions must account for these concerns.
Footnotes
Acknowledgements
Elliot Tapper is the guarantor of this article. Roles of the authors were (a) concept: E Tapper, S Williams; (b) data acquisition and analysis: S Williams, S Nikirk, J Louissaint, E Tapper; (c) writing: S Williams, J Louissaint, E Tapper; (d) revision: JS Bajaj, S Nikirk.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Elliot Tapper has served as a consultant to Novartis, Kaleido, and Allergan, and Axcella, has served on advisory boards for Mallinckrodt, Rebiotix, Novo Nordisk and Bausch Health, and has received unrestricted research grants from Gilead.
Ethics approval
This study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a priori approval by the institution's human research committee. This study was approved by the University of Michigan Ethical Review Board on 5/2/2019 (HUM00161296).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Elliot Tapper receives funding from the National Institutes of Health through the NIDDK (1K23DK117055-01A1). Jeremy Louissaint is supported by T32DK062708.
Informed consent
Written, informed consent was obtained from each patient in this study.
Supplemental material
Supplemental material for this article is available online.