
Abstract
Liver cirrhosis is a serious and potentially life-threatening condition. This life-threatening condition usually arises from complications of cirrhosis. While variceal bleeding is the most acute and probably best studied, several other complications of liver cirrhosis are more insidious in their onset but nevertheless more important for the long-term management and outcome of these patients. This review summarizes the topics discussed during the UEG-EASL Hepatology postgraduate course of the United European Gastroenterology Week 2013 and discusses emergency surgical conditions in cirrhotic patients, the management of hepatic encephalopathy, ascites and hepatorenal syndrome, coagulation disorders, and liver cancer.
Keywords
Emergency surgical conditions in cirrhotic patients
Whatever the surgical condition, its risk is increased in cirrhotic patients. Contributing factors include portal hypertension, thrombocytopenia, coagulopathy, poor nutritional status, altered response to stress or shock and impaired kidney function. In addition, thickening of the peritoneum, splenomegaly and spontaneous collateral shunts increase the technical difficulty. The postoperative course is traditionally characterized by liver dysfunction, ascites (that may leak through the abdominal wound or compromise healing of a digestive anastomosis and therefore become superinfected) and multiple organ failure, which is frequently lethal in a cirrhotic patient. There has therefore been reluctance to perform elective surgery in cirrhotic patients.
Survival of cirrhotic patients has increased as a result of improved medical management; the ensuing risk is therefore to operate on these patients in emergency. Emergency surgery in cirrhotic patients is associated with a seven-fold increased risk of mortality compared with elective surgery. 1 In addition, cirrhotic patients are exposed to specific surgical conditions, in particular umbilical hernia, ruptured hepatocellular carcinoma (HCC) and ectopic variceal bleeding. It is estimated that 10% of cirrhotic patients will undergo surgery during their last year of life.
There are relatively few data on surgery in cirrhotic patients. A systematic review published in 2012 covered 46 studies and the scientific evidence provided by these was relatively poor. 2
Overall risk assessment
Overall risk assessment is correlated both with the Child-Pugh, the MELD score and the MELD-Na score. The Child score was initially developed to predict mortality after shunt surgery, while the MELD score (which is more objective because it weights the variables and does not rely on arbitrary cut-off values) was developed to predict the risk after transjugular intrahepatic portosystemic shunt (TIPS) placement. The Child-Pugh and MELD-Na appear superior to the MELD. 3 Portal hypertension and the presence of active hepatitis (whether viral or alcohol related) also independently increase the risk. There is also an obvious influence of the difficulty of the surgical procedure, and this in particular applies to cardiac surgery and some abdominal procedures such as pancreatic or oesophageal resections.
In a retrospective study of 92 patients, the risk of mortality after elective and emergency surgery was 10% and 22% in Child A patients, 30% and 38% in Child B patients and 82% and 100% in Child C patients. 4 When applied in a large retrospective study of 772 patients who underwent a variety of procedures, the MELD score and emergency procedures were independent risk factors for mortality. 5 Evidence that portal hypertension is also a risk factor is suggested by the observation that morbidity after elective abdominal surgery was decreased in Child A (and possibly Child B–C) patients with portal hypertension who previously had a neoadjuvant TIPS placement to reduce portal pressure.6–8
Besides the liver, attention should also be paid to other frequently associated conditions. Cirrhotic cardiomyopathy is characterized by a baseline increase in cardiac output but blunted systolic contractile response to stress, diastolic dysfunction, absence of overt left ventricular failure at rest and electrophysiological abnormalities. It therefore requires specific perioperative monitoring. Poor nutritional status is virtually constantly associated in the context of surgery with intravascular volume depletion, poor wound healing and increased vulnerability to infection.
Specific conditions in cirrhotic patients
Umbilical hernia
Umbilical hernia is frequent in cirrhotic patients and is correlated with previous ascites, poor nutritional status and therefore advanced cirrhotic disease. In patients with ascites, the incidence is 20% in the course of the disease. The two main complications are incarceration of small bowel and rupture of the hernia with ascites leak and its inherent risk of ascites superinfection. In patients with compensated liver cirrhosis, elective treatment can be performed safely after optimization of ascites treatment with diuretics and albumin; this strategy appears to reduce the risk of complications compared with a conservative strategy. 9 In patients awaiting a liver transplantation, hernia repair should be performed at the time of transplantation. 10 In patients with uncontrolled ascites, elective hernia repair after placement of a TIPS has been suggested. 11 Uncontrolled ascites exposes the patient to a high risk of hernia recurrence.
Ruptured HCC
Ruptured HCC is associated with reduced survival compared with non-ruptured HCC, 12 but active emergency treatment is justified. This relies mainly on arterial embolization. 13
Ectopic variceal bleeding
The main location is oesophageal variceal bleeding for which treatment is standardized. 14 It mainly relies on a combination of pharmaceutical and endoscopic treatment. Porto-systemic shunts are a second-line treatment, except for ‘early TIPS’ in high-risk variceal bleeding, 15 and are currently mainly performed by the TIPS technique rather than by open surgery, although the latter seem to be associated with superior functional results and long-term patency. 16 Variceal rupture may occur in other locations, most commonly the duodenum and rectum, but also at the level of previous abdominal scars. Most of these patients with ectopic varices have a previous history of oesophageal varices. 17 Treatment relies on the same principle as that of oesophageal varices, but as the exact location of bleeding may prove difficult, there might be a greater place for TIPS or interposition meso- or porto-caval shunts. Other less frequent sources of bleeding are bleeding from portal hypertensive gastropathy and portal hypertension-associated gastric or small intestine polypoid lesions that may be responsive to adequate treatment of portal hypertension.
Other surgical conditions
Cholecystectomy
The prevalence of gallbladder lithiasis is increased in cirrhotic patients but this is rarely symptomatic. A thickened gallbladder wall does not necessarily indicate cholecystitis and may simply reflect peritoneal thickening as a result of portal hypertension. Cholecystectomy can be safely performed by laparoscopy with reduced morbidity and hospital stay compared with the open route. 18 Compared with non-cirrhotic patients, the risk of conversion and of bleeding complications are increased.
Trauma including splenic trauma
Cirrhosis increases four-fold the risk of splenic rupture associated with trauma.19,20 This risk is correlated with the MELD score, and a MELD score ≥17 predicts postoperative mortality with a sensitivity of 92% and a specificity of 88%. 20 While conservative treatment is the management of choice in haemodynamically stable patients, therapeutic intervention may be indicated with a lower threshold due to portal hypertension in cirrhotic patients. 21
Colectomy
Elective colectomy is associated with an in-hospital mortality of 14% in cirrhotic patients (29% when there is addition portal hypertension) as compared with 5% in patients without cirrhosis. In the emergency setting, the risk is 21% in cirrhotic patients and 36% when there is portal hypertension. 2
In conclusion, an elective (early) surgical treatment may be better than an urgent (late) treatment and should be performed in hospital structures with an intensive care unit and, when possible, experience in the management of cirrhotic patients.
Update in overt hepatic encephalopathy: Approach to the patient and review of treatment
Introduction and classification
Overview
Hepatic encephalopathy (HE) is a frequent and serious complication of liver cirrhosis. 22 HE has been classified into different types depending on the severity of hepatic dysfunction, the presence of portal-systemic shunts and the number of prior episodes or persistent manifestations.23,24 The large clinical spectrum of manifestations, its variability among patients with overt HE and the complexity of the multi-organ manifestations in cirrhotic patients explain why it is so difficult to perform quality clinical trials for assessing the efficacy of the treatments proposed.
Classification
The first step in the approach to HE is to establish the presence or absence of underlying hepatic failure as well as its severity. Imaging methods (ultrasound, CT, MRI) are especially useful in those patients with large portal-systemic shunts, in which cirrhosis may not be obvious. In addition, HE may develop in the absence of cirrhosis in patients with vascular disorders, such as congenital portal-systemic shunts or portal vein thrombosis. HE associated with acute liver failure or with acute-on-chronic liver failure is the manifestation of a serious disorder with high mortality.
HE associated with cirrhosis and portal hypertension can appear as an isolated episode with or without a precipitating event. The relapse of the episode of HE after a period free of neurological manifestations defines recurrent HE. Those patients with manifestations that persist over time are considered affected by chronic HE; this term should not be confused with the existence of chronic liver failure.
25
Those patients with cirrhosis that exhibit neuropsychological disturbances that are not obvious in the clinical exam, but are revealed by psychometric tests, are defined as exhibiting minimal HE (Figure 1).
24
Classification of hepatic encephalopathy.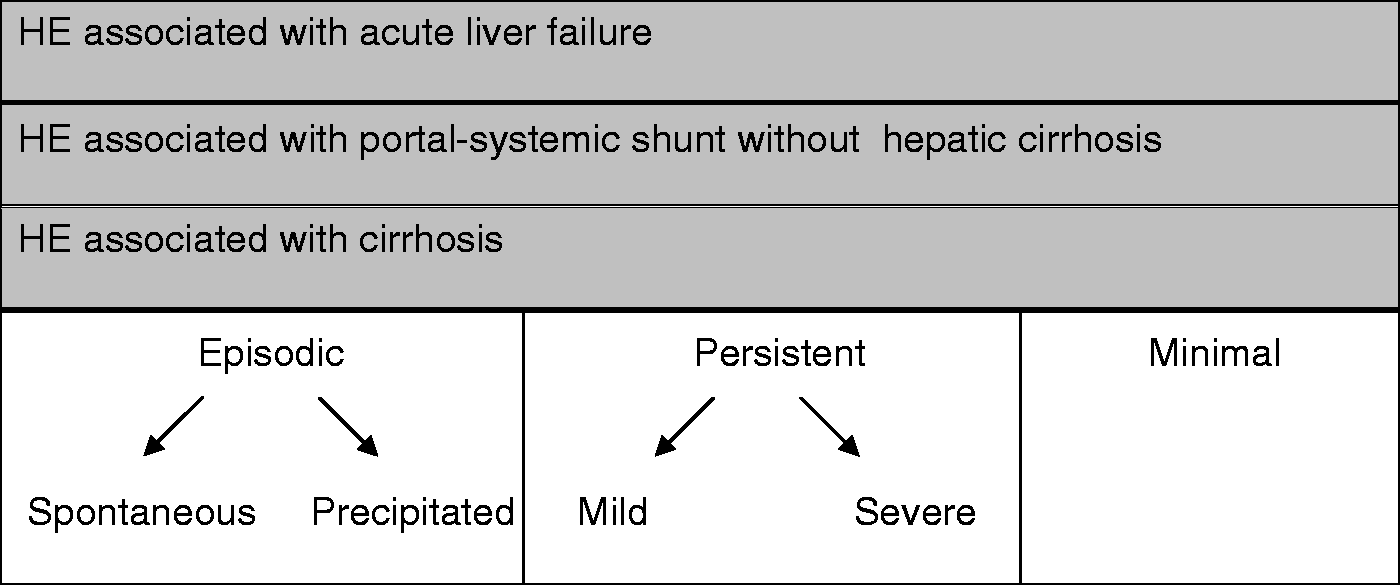
Approach to the patient with overt hepatic encephalopathy
The diagnosis of HE is based on the presence of neurological manifestations that are obvious on clinical exam. The term overt is used to emphasize the presence of clear neurological manifestations and the term covert refers to disturbances that are difficult to recognize without specialized tests (EEG, evoked potentials, etc). The traditional view is that HE progresses from unimpaired cognition (normal psychometric tests and normal clinical examination), to minimal HE (abnormal psychometric tests and normal clinical examination), grade I–II HE (abnormal psychometric tests and abnormal clinical examination), and to grade III–IV HE (psychometric tests cannot be applied due to decreased consciousness). However, the current trend is to interpret the neurocognitive impairment as a continuum and promote the use of cognitive ratings instead of categorical divisions that are based on arbitrary criteria.
Patients with cirrhosis and acute change in mental state should be evaluated carefully for other neurological disorders with similar clinical expression such as nervous system lesions, intake of pharmacological substances, metabolic encephalopathy, such as respiratory failure and hypoglycaemia, nutritional deficits or epileptic status. A detailed medical history and physical exam as well as complementary analytical and imaging procedures if appropriate can avoid diagnostic mistakes.
HE, especially episodic forms, has been traditionally related to precipitating events which can be defined as a clinical condition that does not cause direct injury to the liver or portal-systemic circulation but is responsible for the acute change in mental status. Precipitating factors include: upper gastrointestinal bleeding, infections, use of drugs with central nervous system effects, constipation, renal failure, hydro and electrolytic disturbances. All these conditions appear to act by increasing the generation of putative toxins or enhancing the effects of toxins on the central nervous system; the treatment of the precipitating event is a key element for re-establishing normal consciousness. 26 However, some episodes of overt HE have no recognizable precipitating event. 27
Another important point in the assessment of HE is establishing the severity of liver failure through laboratory tests and imaging of the liver and portal-systemic circulation. Overt HE may develop without parameters of liver dysfunction. These cases should prompt the search for portal-systemic shunts using radiological techniques. HE is usually present in terminal cirrhosis; it is important to distinguish this situation, which may be difficult, to avoid futility. Liver failure can develop over a short period of time in relation to an insult that usually causes a severe, but potentially reversible, inflammatory injury. This situation has been proposed to be termed acute-on-chronic liver failure (ACLF) and should be managed separately from episodic HE, this condition conferring a poor vital prognosis and is usually associated with multiple organ failures. 28
Therapy for hepatic encephalopathy
General aspects
Treatment of HE requires a multi-factorial approach; it is important to guarantee the vital support of the patient, correct the precipitating event and provide drugs with anti-encephalopathy effects. Several disturbances should be corrected; among them the most relevant are the increase in plasma ammonia and correction of inflammatory mediators.
For many years the administration of a low-protein diet was considered a cornerstone of treatment. However, the value of this therapy has been questioned, as a randomized study demonstrated that patients with episodic HE that receive treatment aimed at multiple precipitating factors tolerate well proteins in the diet. Since then, the recommendation is to keep a balanced enteric diet that provides 0.8–1.2 g proteins/kg bw/day. 29
Patients with a good liver function and the presence of large portal-systemic shunts should be evaluated for occlusion. Recently, a multicentre study demonstrated that this intervention in patients with chronic HE and MELD ≤11 is safe and effective. 30 If the portal-systemic shunts are congenital, severe hypoplasia of the portal vein should be discarded in order to avoid massive upper gastrointestinal bleeding following occlusion. 31
Non-absorbable disaccharides
Non-absorbable disaccharides (lactulose, lactitol) are considered a mainstay of treatment. These drugs act on the colonic flora to exert cathartic effects and modify the intestinal pH, leading to a decrease in ammonia absorption and an increase its elimination in stool. It is common practice to use enemas (non-absorbable disaccharides diluted in tap water) in patients that exhibit overt HE or in the prevention of HE in high-risk circumstances (e.g. gastrointestinal bleeding). In spite of insufficient clinical studies, they are considered especially effective in patients with colonic retention of faeces. A comparison in a meta-analysis of the efficacy of no-intervention, non-absorbable disaccharides and treatment with antibiotics did not find differences between groups. 32 Most recent studies have demonstrated the efficacy of non-absorbable disaccharides compared with placebo in the prevention of HE in primary and secondary prophylaxis.33–35 Unfortunately, there are no randomized studies of good quality showing beneficial effects for overt HE. In spite of these limitations, the use of non-absorbable disaccharides is considered the standard of care for treating HE, based on potential mechanisms and large experience of use. 23
Antibiotics
The use of antibiotics in the treatment of HE is based on their action in the intestinal flora. Different mechanisms for their beneficial effect have been proposed. Inhibition in the gut of intestinal glutaminase, an enzyme that is over-activated in cirrhotic patients, can be responsible in part for the rise in plasma ammonia. 36 The decrease in intestinal bacterial translocation with antibiotics can decrease the exacerbation of the immune response triggered by bacterial products in plasma. 37
Neomycin was the first non-absorbable antibiotic showing efficacy in chronic HE. 38 This drug is relative cheap, but has the potential of being absorbed in part after more than 6 months of use. For this reason it is seldom used long term, in spite of efficacy similar to rifaximin. 39 Other antibiotics that have previously been used (metronidazole, vancomycin) have a potential toxic effect, which has led their use being abandoned. 40
Rifaximin has wide antibacterial action without intestinal absorption, minimizing the toxic effects and allowing a prolonged use. Studies comparing rifaximin (1200 mg/d) with non-absorbable disaccharides,41–44 or to neomycin or paromomycin,45–47 have found similar efficacy. Only three of these studies42–44 were performed during an overt episode of HE and none of them had a placebo group. A meta-analysis that compares rifaximin with non-absorbable disaccharides shows similar efficacy (OR = 1.92, 95%CI: 0.79–4.98, p = 0.15). Similar results were found when comparing rifaximin with other antibiotics (OR = 2.77, 95%CI: 0.35–21.83, p = 0.21). Nevertheless, there was a trend in favour of rifaximin. No statistically significant differences were observed in decreasing plasma ammonia42–44,46,47 or improving psychometric tests, 47 but rifaximin exhibited a better safety profile based on the lower frequency of diarrhoea (OR = 0.27, 95%CI: 0.15–0.59, p < 0.01). The only randomized trial that compared rifaxim plus lactulose (if necessary) with placebo was performed for secondary prophylaxis, proving higher effectiveness of rifaximin ± lactulose in preventing new episodes of HE.
Future prospects
Glycerol phenylbutyrate (HPN-100) is a pro-drug of phenylbutyric acid (PBA), which is absorbed from the intestine and converted by way of b-oxidation to the active moiety, phenylacetic acid (PAA). PAA is conjugated with glutamine in the liver and kidney by way of N acylcoenzyme A-L-glutamine N-acyltransferase to form phenylacetylglutamine (PAGN), a water-soluble molecule that can be eliminated through the urine. This molecule has proven its safety in cirrhotic patients. 48 In a recent randomized double-blind study the administration of HPN-100, which enhanced the urinary excretion of ammonia equivalents, resulted in a lower number of recurring HE episodes. A significant number received rifaximin in addition to HPN-100. In this subgroup, the combination of rifaximin and HPN-100 did not show better results than rifaximin alone. 49
Ornithine phenylacetate (OP) is a new proposal for decreasing ammonia in cirrhosis through the combined administration of phenylacetate (PA) and ornithine. This therapy is based on the capacity of ornithine to stimulate the activity of glutamine synthetase, hence incorporating ammonia into a ‘non-toxic’ molecule. The newly formed glutamine will combine with PA, allowing the elimination of ammonia in the urine by its conversion into PAGN. This strategy prevents the degradation of glutamine by intestinal glutaminase and avoids new formation of ammonia. 50 This molecule has been demonstrated to be safe in decompensate cirrhotic patients, and the current data seem to confirm its efficacy in decreasing plasma ammonia. 51
Conclusion
The approach to a patient with HE requires a multiple-level assessment. It is necessary to recognize the presence of a confusional syndrome, in conjunction with the assessment of precipitating factors and severity of liver failure. Management of the patient should be multifaceted and requires measures to decrease ammonia, investigation of infections and prevention of kidney failure. There are several drugs that may be beneficial, but their major efficacy has been demonstrated in preventing HE. Assessment of potential for liver transplantation should be part of the evaluation.
From ascites to hepatorenal syndrome
Refractory ascites
Refractory ascites occurs in 5–10% of patients with cirrhosis and ascites.52,53 This prevalence, identified in clinical trials, is probably higher in unselected series of patients as observed in clinical practice. According to the criteria of The International Ascites Club, refractory ascites is defined as “ascites that cannot be mobilized or the early recurrence of which (i.e. after paracentesis) cannot be satisfactorily prevented by medical therapy”. The term refractory ascites includes two different subtypes: diuretic-resistant ascites (ascites that cannot be mobilized or the early recurrence of which cannot be prevented because of lack of response to dietary sodium restriction and intensive diuretic treatment) and diuretic-intractable ascites (ascites that cannot be mobilized or the early recurrence of which cannot be prevented because of the development of diuretic-induced complications).52,53 Treatment includes large-volume paracentesis with volume support with plasma expanders, continuing diuretic therapy, insertion of TIPS, liver transplantation, and use of new therapeutic options such as vasoconstrictors or implantation of automated pump.
Large-volume paracentesis
Repeated large-volume paracentesis is an effective therapy of refractory ascites although it does not affect the underlying pathophysiology. Total paracentesis has been shown to be as effective and safe as repeated partial paracentesis. 54 Paracentesis causes an acute increase of cardiac output and a reduction in systemic vascular resistance and arterial blood pressure, an immediate fall in right atrial pressure, and a delayed fall in left atrial pressure. 55 This paracentesis-induced central hypovolaemia has been termed the post-paracentesis-induced circulatory dysfunction (PICD) and may occur for up to several days after the procedure, and its severity correlates with the mortality rate. 53 PICD can be prevented by volume expansion. A single controlled trial has compared therapeutic paracentesis with or without volume expansion, where patients were randomized to receive repeated paracentesis of 5 l/day together with or without human albumin. 56 Significantly more side effects, including renal impairment and hyponatraemia, occurred in patients treated without volume expansion. PICD may therefore occur if volume expansion is not given. The effectiveness of synthetic plasma expanders is lower than that of albumin when the paracentesis volume is higher than 5 l.57,58 Ascites will recur in more than 90% of patients after a large-volume paracentesis, thus cirrhotic patients with ascites treated with paracentesis should immediately receive diuretics, when tolerated, to prevent early recurrence of ascites. 59
TIPS
The effects of TIPS on the control of ascites and transplantation-free survival have been evaluated in five randomized controlled trials. The first trial from 1996 included 25 patients, of whom 13 were treated with TIPS. 60 In this trial, ascites was controlled only in Child-Pugh class B patients and survival was poorer in the TIPS group. In a second trial the control of ascites was better in the TIPS group, but albumin was not given to all in the paracentesis group. 61 Whereas the frequency of HE was equal in the two groups, TIPS was independently associated with a trend towards an improved survival. 61 Results from a third trial showed a better control of ascites in the TIPS group at the cost of a higher frequency of encephalopathy. 62 The risk of developing hepatorenal syndrome was lower in the TIPS group, whereas survival between the two groups was similar. In the fourth trial, 63 ascites was controlled better in the TIPS group than in a paracentesis/medical treatment group, and there was a trend towards more severe encephalopathy in the TIPS group. In addition, TIPS insertion did not improve survival or quality of life. In the fifth trial survival was significantly higher in the TIPS group.
The included patients in the five abovementioned studies have been included in five meta-analyses, yielding almost similar conclusions.64–69 All meta-analyses agree that recurrence of ascites is lower in patients treated with TIPS than with large-volume paracentesis after 3 and 12 months. The frequency of HE was reported equally higher in all studies. An increased transplant-free survival was found in the TIPS group in only one meta-analysis. 67
Liver transplantation
Once the ascites becomes refractory to medical treatment, the 6 months survival is reduced to 50%.70–72 In general, any patient with cirrhosis should be considered as a potential candidate for liver transplantation after the appearance of ascites, but patients with their first episode of ascites may not necessarily benefit from liver transplantation. However, with increasing MELD scores and when the ascites becomes refractory to medical treatment, the patient should immediately be considered for liver transplantation since treatment with TIPS and large-volume paracentesis does not significantly affect the prognosis.
Vasoconstrictors
Administration of vasoconstrictors may primarily ameliorate splanchnic and arterial vasodilatation by increasing arterial blood pressure and thereby improve renal perfusion and filtration. In patients with ascites, a single oral dose of the α1-adrenergic agonist midodrine increases arterial blood pressure, renal perfusion, glomerular filtration rate, and sodium excretion and reduces the level of vasopressin. 73 Comparable effects were seen after a 7-day midodrine treatment, including suppression of the renin–angiotensin system, indicating that the increased diuresis and natriuresis were related to improvement of central hypovolaemia. 74 Addition of the somatostatin analogue octreotide has been suggested to further improve systemic and renal haemodynamics, but recent data do not support this concept. 75 In a randomized trial, the additive diuretic effect of the centrally acting α2-agonist clonidine was studied for 3 months. 76 The time needed for diuretic response and the time for readmission for tense ascites were significantly shorter in the clonidine group, and the diuretic dose and the frequency of complications were significantly lower in the clonidine group. Terlipressin, a vasopressin 1 (V1) receptor agonist, is a potent vasoconstrictor that has been shown in a small pilot study to be effective in the treatment of refractory ascites. 77 However, in a recent meta-analysis albumin reduced morbidity and mortality among patients with tense ascites undergoing large-volume paracentesis, as compared with alternative treatments investigated thus far, including vasoconstrictors. 57
Automated pump system
The placement of a pump for the automated removal of ascites from the peritoneal cavity into the bladder, from where it was eliminated through normal urination, has recently been evaluated in a pilot study in patients with cirrhosis and refractory ascites. The automated pump seems an efficacious tool to treat refractory ascites, although its efficacy and safety versus large-volume paracentesis should be proven in a randomized clinical trial, which is underway. 78
Refractory hydrothorax
Approximately 21–26% of cases of hepatic hydrothorax are refractory to salt and fluid restriction and diuretics, and warrant consideration of additional treatment measures. Several groups have reported a beneficial effect of TIPS in patients with hepatic hydrothorax.79,80 Despite the shortcoming associated with a poor definition of the refractoriness of the hydrothorax, most series have demonstrated response rates in the range of 70–80% of patients with refractory hepatic hydrothorax; 59% had a complete response, 20% had a partial response, and 21% had no response to TIPS. The short-term survival rates at 30, 60 and 90 days were 81%, 78% and 72%, respectively. 81 These survival rates are equivalent to those previously reported by other authors who found that the 30-, 90-, and 150-day mortality was 14%, 25% and 53%, respectively, after TIPS placement. 82
Managing coagulation disorders in cirrhotic patients
There has been increased interest in coagulation disorders associated with cirrhosis, as new data have questioned the view that cirrhosis is associated with a bleeding diathesis.83–85 Furthermore, evidence has been recently provided that prothrombin time (PT) as assessed by international normalized ratio (INR) is not adapted to the context of chronic liver disease.86,87 Last, attention has recently been focused on the risk and significance of superimposed portal vein thrombosis.88,89
Coagulation disorders in patients with cirrhosis and their clinical correlates
Primary haemostasis appears to be preserved in most patients with cirrhosis. 85 Platelet counts below 150,000/µl are common, and are explained by a combination of splenic pooling, increased destruction through immunological mechanisms, and decreased production due to inappropriate thrombopoietin levels. However, platelet counts below 50,000/µl are seen in <1% of patients. Von Willebrandt factor levels are increased in cirrhosis, in parallel with the severity of the disease, which is probably instrumental in maintaining normal primary haemostasis. Altered platelet function may occasionally be found, as indicated by prolonged bleeding time. However, prolongation of bleeding time is of questionable relevance to the risk of clinically significant bleeding.
Coagulation appears to be similarly preserved.83,84 It is now well established that, despite the decreased plasma levels of most coagulation factors, thrombin generation in vitro is maintained in patients with cirrhosis and platelet counts above 60,000/µl, due to a simultaneous decrease in coagulation inhibitors (protein C, protein S and antithrombin). Features of accelerated intravascular coagulation and fibrinolysis (increased levels of D-dimers, thrombin–antithrombin complexes, fibrinopeptide A and soluble fibrin, and shortened clot lysis time) may be found in patients with cirrhosis. Endotoxinaemia is common in this context. 90 The clinical relevance of these anomalies is unclear.
An increased risk of bleeding in patients with cirrhosis has mostly been related to portal hypertension or highly vascularized tumours, either spontaneously or at surgery. 83 There is little evidence for an increased risk of bleeding in the brain or skull, retina, joints, muscles or other solid organs, independent from the increased risk of fall or accident, or from a specific effect of the cause for cirrhosis on haemostasis.
A procoagulant state has been observed in vitro due to the marked decrease in protein C levels. 91 Plasma levels of factor VIII are elevated in patients with acute or chronic liver disease. As high factor VIII levels have a major procoagulant effect, they probably also contribute to the procoagulant state documented in vitro. 84 Moreover, there is some epidemiological evidence for a slightly increased risk of deep, non-splanchnic vein thrombosis in patients with cirrhosis. 83 Thus, patients with cirrhosis, are not ‘spontaneously anticoagulated’, and may even be ‘prothrombotic’.
Cirrhosis is a major risk factor for portal vein thrombosis. 92 The risk is in part related to the severity of liver disease.88,89 A decreased velocity of portal vein flow likely play an independent role. Underlying prothrombotic mutations (particularly Factor II Leiden) may also be involved. Although portal vein thrombosis is associated with the severity of cirrhosis, it is still unclear whether it plays a causal role in the progression of the disease or it is a mere indicator for advanced liver disease.
The evaluation of haemostasis and coagulation in patients with cirrhosis is challenging. Platelet counts are not related to the risk of bleeding from oesophageal varices. 85 Thrombin generation is not related to conventional tests for the assessment of the risk of bleeding (e.g. PT or INR, or activated partial thromboplastin time).83,84 The risk of bleeding from gastroesophageal varices is only indirectly related to PT or INR, as a component of Child-Pugh score in describing severity of liver disease.87,88 Furthermore INR, which has been devised for vitamin K antagonist monitoring, is not appropriate to evaluate the prolongation of PT induced by liver disease.86,87 Likewise, investigating prothrombotic conditions is challenging. The interpretation of decreased levels of coagulation inhibitors (protein C, protein S or antithrombin), antiphospholipid antibodies or hyperhomocysteinaemia as primary or secondary to liver disease is almost impossible. 92
Prevention and treatment of bleeding in patients with cirrhosis
Several means have been proposed for the prevention and for the control of active bleeding, either provoked by trauma or interventions, or spontaneous.
Preventing bleeding
As stated above, bleeding in patients with cirrhosis is mostly related to portal hypertension, not to defective haemostasis. 83 Indeed, means whose efficacy has been proven for preventing per-operative or spontaneous bleeding, or reducing expected blood losses, have targeted portal pressure reduction (portosystemic shunting, non-selective beta adrenergic blockade) or local control of potential sources for bleeding (endoscopic ligation, careful surgical dissection).93,94 Furthermore, attempts at preventing bleeding with pharmacological agents shown otherwise to correct the anomalies of coagulation tests have met with little success. Despite well-documented effect on various coagulation tests, evidence is lacking of a clinical benefit for prophylactic desmopressin, 95 antifibrinolytic agents (aprotinine or antifibrinolyticaminoacids), 96 vitamin K 97 and recombinant factor VIIa. 98 The role of prophylactic platelet transfusion or coagulation factor infusion (whether as fresh frozen plasma or coagulation factor concentrates) has not been addressed in randomized controlled trials. 85 The available evidence does not suggest a favourable benefit–risk ratio with platelet or fresh frozen plasma transfusion.99–101 An increased risk of acute lung injury may even result from these interventions. Increasing platelet counts with eltrombopag in patients with counts below 50,000/µl prior to an elective invasive procedure did not significantly reduce the incidence of clinically significant bleeding, and may increase the risk of developing portal vein thrombosis. 102 Although a platelet count below 50,000/µl is generally taken as a trigger for platelet transfusion prior to liver biopsy or endoscopic ligation of oesophageal varices, the evidence for this is weak.85,103
Aspirin and non-steroidal anti-inflammatory agents are generally considered contraindicated in patients with decompensated cirrhosis, mostly based on a well-documented increase in the risk of ruptured gastroesophageal varices on the one hand, and functional renal failure on the other.104,105 Antithrombotic drugs must be interrupted, whenever possible, before planned interventions or invasive procedures. It is generally recommended to interrupt anticoagulation therapy briefly at the time of endoscopic ligation of oesophageal varices.
Control of active bleeding
When tested in randomized control trials, desmopressin 106 and recombinant factor VIIa 107 have not been found to ameliorate the control of bleeding from gastroesophageal varices. The other means, aprotinin and antifibrinolytic amino acids, platelets, fresh frozen plasma, and coagulation factor concentrates, have not been evaluated. There has been no clinical trial on these agents in active bleeding occurring from sources other than gastroesophageal varices in patients with cirrhosis.
Prevention and treatment of thrombosis in patients with cirrhosis
Extrasplanchnic deep vein thrombosis and portal vein thrombosis have to be considered separately. Prevention of extrasplanchnic deep vein thrombosis has not been addressed in clinical trials. A retrospective analysis in patients undergoing surgical resection for HCC was inconclusive as to the risk and benefits of low molecular weight heparin given prophylactically. 108 Data on the safety and efficacy of anticoagulant agents given for established deep vein thrombosis are limited to retrospective uncontrolled studies which did not show unexpectedly high bleeding rates.109,110
A randomized controlled trial has shown that the administration of enoxaparin, 4000 anti-Xa units per day for 48 weeks, prevented the development of portal vein thrombosis in patients with moderately severe cirrhosis (Child-Pugh B7 to C10). 111 The findings from this trial were remarkable in that enoxaparin prevented decompensation and decreased mortality to a greater extent than it prevented portal vein thrombosis. Studies on the mechanism for this effect are eagerly awaited.
Treatment of established portal vein thrombosis has been assessed only in retrospective cohort studies.88,89 Anticoagulation with low molecular weight heparin and/or vitamin K antagonists has been associated with recanalization rates of about 50%. The actual impact on the outcome of cirrhosis has not been assessed. Rare cases of treatment-related fatalities have been reported. 110 The optimal anticoagulation therapy and the appropriate way to monitor it raise many unresolved issues. 112 Available data in patients who received a TIPS while they had portal vein thrombosis suggest that TIPS is feasible when intrahepatic portal veins are visible, and that portal vein thrombi can be cleared following TIPS insertion in the absence of associated anticoagulation therapy.113,114 Here again, the actual impact of TIPS on the outcome has not been assessed. Therefore, the place for anticoagulation and TIPS in patients with established cirrhosis needs further assessment in randomized controlled trials. Currently, there appears to be some consensus to consider anticoagulation in patients with portal vein thrombosis who are candidates for liver transplantation, as there are indications that more extensive portal vein thrombosis jeopardizes post-transplant outcome, particularly in patients with low MELD scores.
Managing hepatocellular carcinoma
Liver cancer (HCC) is the fifth most common cancer worldwide and the third most common cause of cancer-related mortality. Its prevalence in European countries is variable but mostly increasing due to the epidemic of viral hepatitis during the last three decades.115,116 Treatment for liver cancer in Europe occurs mostly according to the current EASL guidelines
117
for the management of liver cancer (see Figure 2).
Management of hepatocellular carcinoma.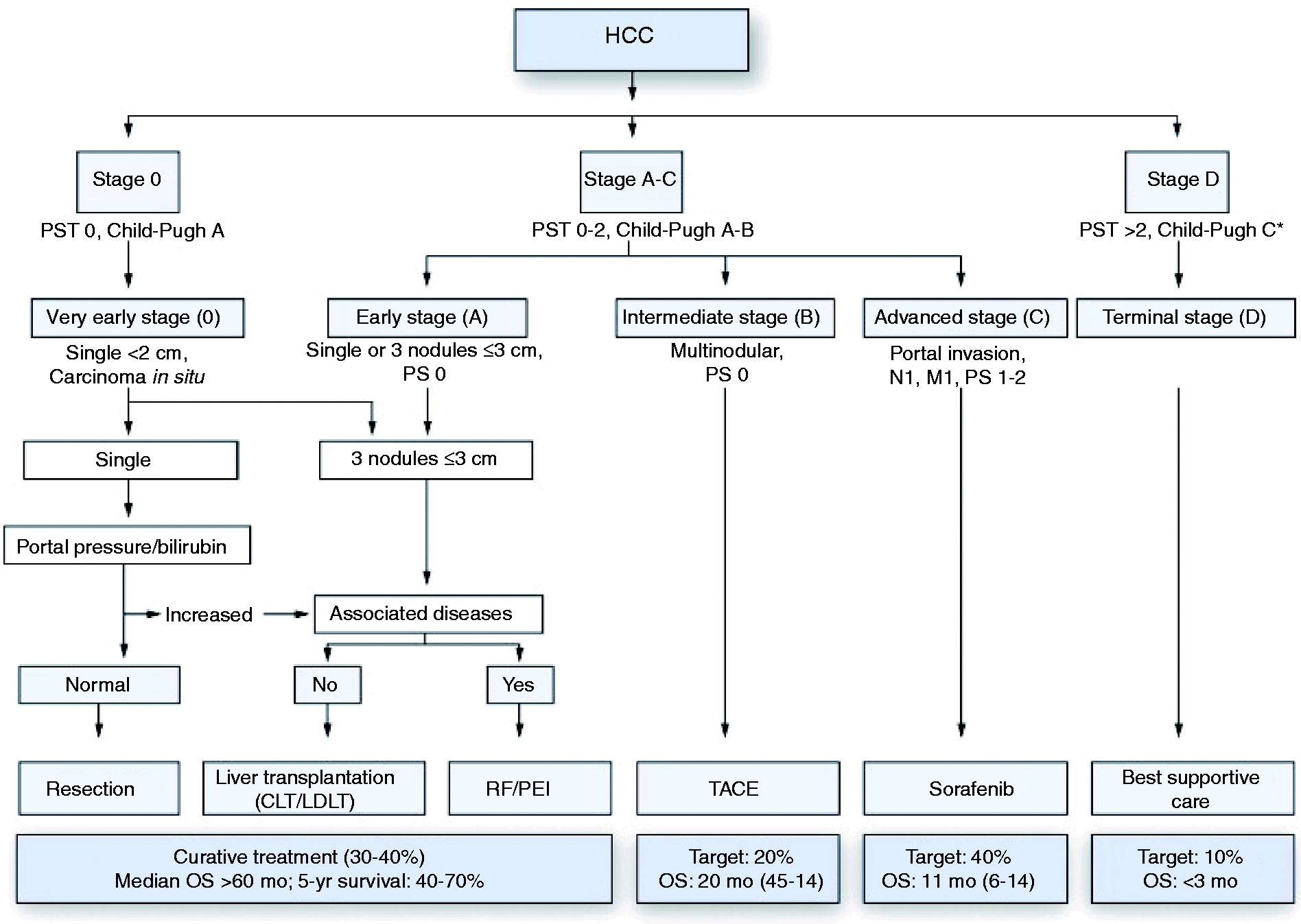
Early stage HCC
Patients with small tumours, normal bilirubin, and no clinically significant portal hypertension are usually evaluated for surgical resection. If surgical resection is not possible, or the risk for surgical resection is increased, then local ablation with radiofrequency ablation is an adequate substitute. Some authors even recommend a local ablation even in resectable patients as long as the patient is not scheduled to undergo liver transplantation at a later stage, but this is controversial. 118
If the tumour is not resectable due to either size, location, or liver function but still within the Milan criteria (one tumour ≤5 cm in the diameter or up to three tumours ≤3 cm in diameter), these patients can be referred for liver transplantation with excellent outcome as long as they are suitable candidates for the procedure. Extension of the transplant criteria beyond the Milan criteria has been advocated by several people but leads to an increased recurrence rate of HCC post-transplant. 119 Compared with resection, radiofrequency ablation is associated with similar survival but higher recurrence rates.
Intermediate stage HCC
Transarterial chemoembolization (TACE) is the standard of care for patients with intermediate stage HCC, good performance status, and lack of major portal vein thrombosis. 120 TACE is able to improve the median survival from 16–20 months to about 24 months, but has only an objective response rate of around 40% and does not benefit patients that are not responding to treatment. 121 New developments such as drug-eluting beads TACE (DEB-TACE) have improved side effects but not patient outcomes so far. 122 Improving the outcome of TACE by combining TACE with drug treatment such as sorafenib has so far not yielded positive results. Unfortunately, TACE is also able to harm patients. In order to predict which patients would benefit from repeated TACE applications, the ART score was recently developed and validated. 123 The simple score is calculated immediately before the second TACE and helps in selecting patients for continued TACE treatment, if a viable and treatable tumour can still be found on imaging. The ART score is calculated using the radiologic response, the change in AST levels, and the change in Child-Pugh score between the first and the second TACE. Patients with an ART score >2.5 should not undergo further TACE treatments and should be considered for other management options.
Advanced stage HCC
In advanced stage HCC, the multikinase inhibitor sorafenib has been shown to increase overall survival in two phase III trials,124,125 making it the standard of care in this tumour stage. Sorafenib is able to improve patient survival independently of the underlying disease aetiology or any prior treatment received by the patient before reaching the advanced stage. Its effectiveness is definitely proven for patients without cirrhosis or with Child A cirrhosis, while fewer data are available for patients with HCC and more advanced stage liver disease.126–128 Sorafenib is fairly well tolerated but causes diarrhoea in around 40% of patients and dermatological problems (hand–foot skin reaction) in about 20% of patients. These side effects can usually be managed quite easily. The survival benefit conferred by sorafenib is about 3 months in Western patients, and with a HR of 0.69 is equally effective compared with trastuzumab for metastatic breast cancer or bevacizumab for metastatic colon cancer.
Future developments in HCC management
In the last 2 years several other targeted agents have been tested for the management of advanced stage HCC (sunitinib, brivanib, linifanib) but all of them have failed in first and brivanib even in second-line treatment of HCC. Also, combination treatment using sorafenib together with erlotinib did not improve patients’ survival. Currently, sorafenib is being tested in combination with doxorubicin in a phase III trial, and several drugs are being tested in second-line trials in patients that have failed sorafenib treatment. Everolimus and ramucirumab have already completed phase III trials, while the c-met inhibitor tivantinib is currently one of the more interesting drugs being tested in ongoing phase III studies.
In addition to drug treatments several interventional radiological techniques have also been developed, and radioembolization with 90 Yttrium seems to be an interesting candidate approach for management of advanced stage and maybe even intermediate stage HCC. 129
Summary
While effective treatment principles for HCC have been clearly established, the therapy of intermediate and advanced HCC is still far from optimal. Despite the fact that several drugs are being developed in these disease stages, the most important aspect of treating liver cancer would be a higher rate of early detection to allow more patients to undergo curative treatments such as resection, radiofrequency ablation or liver transplantation. So far, no country in Europe has established a nation-wide screening programme of patients at risk of developing liver cancer, which are all patients with liver cirrhosis. It remains to be seen whether more emphasis will be put on prevention and early detection of liver cancer in the years to come.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
MP-R. acts as an investigator for Bayer, Lilly, Novartis, Boehringer-Ingelheim, Arqle-Daiichi, and Abbott, as an advisor for Bayer, Lilly, Arqle, and Boehringer-Ingelheim, as a speaker for Bayer, Lilly, and Novartis, and received grant support from Bayer. All other authors report no conflict of interest.