
Abstract
Background and aim
The incidence of gastroesophageal reflux disease (GERD) is high after per-oral endoscopic myotomy (POEM). GERD after POEM may be qualitatively different from GERD in patients without motility disorders. In this study, we aimed to analyze and compare different aspects of GERD between patients with post-POEM GERD and non-achalasia GERD.
Methods
The data of patients with GERD after POEM (January 2018 to June 2019) was compared with that of a control group (non-achalasia GERD group), which included patients presenting with typical reflux symptoms without associated major motility disorders. Patients with lower esophageal sphincter pressure lower than 10 mmHg were excluded from the study. GERD was evaluated at 3 months after POEM. Esophageal acid exposure time higher than 4.2% was used to define GERD. The primary outcome of the study was comparison of GERD related quality of life and reflux symptom severity between the two groups. In addition, the severity of erosive esophagitis and reflux-symptom association were also recorded in the two groups.
Results
A total of 100 patients were included in the study, with 50 patients in each group (post-POEM GERD vs. controls). The baseline parameters were comparable between the two groups. Median interquartile range of GERD related quality of life score was significantly lower in the post-POEM group (11 (0–23.3) vs. 34 (24–44); p < 0.001). The post-POEM GERD group had significantly lower median heartburn (6.0 (0–16.3) vs. 15.5 (7.5–24.8); p = 0.001) and regurgitation scores (0 (0–6.0) vs. 20.0 (12.3–25.0); p < 0.001). Erosive esophagitis was more frequent in the post-POEM group (28 (56%) vs. 10 (20.4%), p = 0.001). Only three (6%) patients in the post-POEM group had a positive reflux-symptom association as compared with 28 (56%) patients in the control group (p < 0.001).
Conclusion
In selected patients with pH positive GERD after POEM, the symptoms are milder and reflux-symptom association is poor in spite of more severe esophagitis as compared with controls.
Study highlights
What is known:
Gastroesophageal reflux disease (GERD) after per-oral endoscopic myotomy (POEM) is common and subclinical. Data on GERD related quality of life and reflux-symptom association after POEM is limited. Reflux symptoms after POEM are milder and have poor association with reflux episodes. Triviality of symptoms despite high acid exposure and severe esophagitis suggests esophageal hyposensitivity.
What is new here:
Introduction
Per-oral endoscopic myotomy (POEM) has emerged as an effective therapy for the management of achalasia and esophageal spastic disorders.1–3 While POEM is being increasingly used, a high incidence of post-operative gastroesophageal reflux disease (GERD) has become an irking problem.4–6 When left untreated, GERD can lead to potential complications such as Barrett’s esophagus and adenocarcinoma. 7 The objective evidence of GERD is found in up to two-thirds of the patients undergoing POEM.5,8–10
In contrast to GERD in patients without associated motility disorders, there is limited data on reflux-symptom association in patients who develop GERD after POEM. In the majority of cases, GERD is usually subclinical after POEM and symptoms do not correlate well with esophagitis or increased esophageal acid exposure. 10 We presume that the presentation and severity of GERD may be different in post-POEM patients as compared with patients with GERD in absence of a co-existing esophageal motility disorder. However, there is no convincing evidence to support this hypothesis. Therefore, we conducted a retrospective case–control study to compare GERD related quality of life, severity of symptoms and erosive esophagitis, and reflux-symptom association between patients with post-POEM GERD and non-achalasia GERD.
Methods
In this study, we analyzed the data of patients who underwent evaluation for GERD at our center from January 2018 to June 2019. The patients presenting with GERD after POEM were included as cases (post-POEM GERD) and those with non-achalasia GERD were recruited as controls in the ratio of 1:1. The cases and controls were matched for age, gender and esophageal acid exposure time (AET) as measured by 24-h ambulatory pH impedance study.
Eligibility criteria
Consecutive patients with idiopathic achalasia and diagnosed with GERD after POEM were screened for possible inclusion into cases. Exclusion criteria were: patients with sigmoid achalasia, clinical failure after POEM, significant stasis after POEM defined by <50% improvement in esophageal emptying, post-POEM resting lower esophageal sphincter (LES) pressure <10 mmHg and a history of endoscopic or surgical myotomy prior to POEM.
The patients attending the out-patient department of Gastroenterology with typical reflux symptoms (heartburn and/or regurgitation) and well controlled on proton pump inhibitors (PPIs) for at least 3 months were screened for potential controls. GERD was diagnosed using the standard criteria as mentioned in the following. Exclusion criteria for controls were atypical manifestations of GERD, partial symptom resolution on PPI therapy, esophageal reflux hypersensitivity, functional heartburn, concomitant dysphagia, large hiatus hernia (>3 cm in length), resting LES pressure <10 mmHg, esophagogastric junction outflow obstruction, major esophageal motility disorders, esophageal malignancy and previous esophageal or gastric surgery.
Pre-procedure evaluation
A standard battery of investigations was performed prior to POEM and included esophago-gastro-duodenoscopy (EGD), sub-typing of achalasia using high resolution manometry (HRM) and timed barium swallow (TBS). Symptom severity was assessed using the Eckardt score, which has scores for dysphagia, chest pain, regurgitation and weight loss (range 0–12). 11 The POEM procedure was carried out under general anesthesia using a standard technique as described in our previous studies. 12 The selection of site (anterior or posterior) and the length of myotomy were left to the discretion of the endoscopist.
Post-POEM evaluation: GERD and clinical success
All the patients were prescribed PPIs (equivalent to 20 mg rabeprazole or 40 mg pantoprazole/day) for a period of about 3 months after POEM. Clinical success (Eckardt score ≤3) was assessed at pre-specified intervals, that is, 3 months, 6 months, 1 year and yearly thereafter. Objective evaluation for clinical success and GERD was performed at 3 months using EGD, TBS, esophageal HRM and 24-h pH impedance study. The patients were instructed to stop PPI medications for 2 weeks before the planned 24-h pH impedance testing. GERD related quality of life (using GERD-HRQL validated questionnaire) was evaluated at 3 months while the patients were off PPI.
Evaluation of controls
The potential controls underwent EGD, esophageal HRM and 24-h pH impedance study. The past medical records were reviewed and a detailed history of disease duration and acid suppression medication intake was noted. Evaluation of GERD-HRQL and esophageal acid exposure using 24-h pH impedance study was performed after withholding PPIs for 1–2 weeks.
24-h pH impedance study
We followed a standard protocol for esophageal pH testing in all the cases and potential controls. 13 On the test day, a calibrated multi-channel intraluminal impedance pH probe was placed into the stomach trans-nasally, which was connected to a data acquisition device (ZepHr pH monitor, Sandhill Scientific, Highlands Ranch, Colorado, USA). The pH and impedance measurements were recorded for 24 h. The occurrence and timing of symptoms were registered during the study by instructing the patients to press pre-specified buttons on the data logger at the onset of symptoms. The median percentage time of esophageal pH less than 4 or AET, DeMeester score, number of reflux episodes, and the symptom index and the symptom association probability (SAP) of reflux episodes were noted. The reflux episodes measured by impedance were further classified into acidic (pH <4) or non-acidic (pH >4) based on pH monitoring. Non-acidic reflux episodes included weakly alkaline (negligible drop in baseline pH) and weakly acidic (drop in pH below baseline but >4) reflux episodes.
Outcomes
The primary outcome of the study was to evaluate the difference in the GERD related quality of life, heartburn and regurgitation severity between post-POEM GERD and control groups. The secondary outcomes of the study included differences in the endoscopic severity of esophagitis and reflux-symptom association between both the groups. GERD was evaluated at 3 months after the POEM procedure.
Definitions
Clinical success
A post-operative Eckardt score ≤3 and >3 after POEM defined clinical success and failure, respectively.
GERD
The diagnosis of GERD was established by AET >4.2% and/or DeMeester score >14.7 on 24-h pH impedance study in both groups. 14 Sub-analysis was done as per the recent Lyon consensus on GERD, which defines AET >6% as definitely abnormal. 15
GERD-HRQL score
A questionnaire including 16 Likert-type questions, with responses ranging from 0 (no symptoms) to 5 (worst symptoms) to each question was used to calculate GERD-HRQL score. 16 The total score was calculated by summing the individual scores to questions 1–15. The heartburn and regurgitation severity scores were calculated by summing the individual scores to questions 1–6 and 10–15, respectively. The greatest possible total score (worst symptoms) was 75 and the worst possible symptom score for each symptom was 30.
Erosive esophagitis
Esophagitis on EGD was graded according to the Los Angeles classification. 17
Symptom–reflux association
Symptom index and SAP were used to define the temporal association between symptoms and reflux episodes. The symptom index is the percentage of symptom events preceded by reflux episodes and an index of more than 50% is considered positive. The SAP is the probability of association between symptom events and reflux episodes and is considered positive if the probability of the observed association not occurring by chance is >95%.
Statistical analysis
The continuous data was expressed as median (interquartile range) and the categorical data as frequencies unless otherwise specified. The normality of distribution of continuous data was tested using Shapiro–Wilk test. In the post-POEM GERD group (cases), comparison of paired continuous data between pre- and post-POEM was done using Wilcoxon Signed Rank test. Comparison of continuous data between groups (cases and controls) was done using unpaired t test or Mann–Whitney U test. Comparison of categorical data between groups was performed using chi-square test with Yates correction. All the tests of significance were two tailed and a p value of <0.05 was considered to indicate statistical significance.
Results
Patient characteristics
The study design and the distribution of patients are summarized in Figure 1. A total of 63 patients with objective diagnosis of GERD after POEM were screened for inclusion into cases. Of these, 13 cases were excluded: two patients with sigmoid achalasia, five with incomplete esophageal emptying on TBS or clinical failure, four with resting LES pressure <10 mmHg after POEM and two with past history of failed Heller’s myotomy. The remaining 50 patients (median age 41.5 years (interquartile range 36.5–52 years), 31 (62%) males) were included as cases in the post-POEM GERD group. The sub-types of achalasia according to the Chicago classification were: type I, eight (16%); type II, 38 (76%) and type III, four (8%). Prior treatment history with pneumatic balloon dilatation (PBD) was noted in 10 patients (20%).
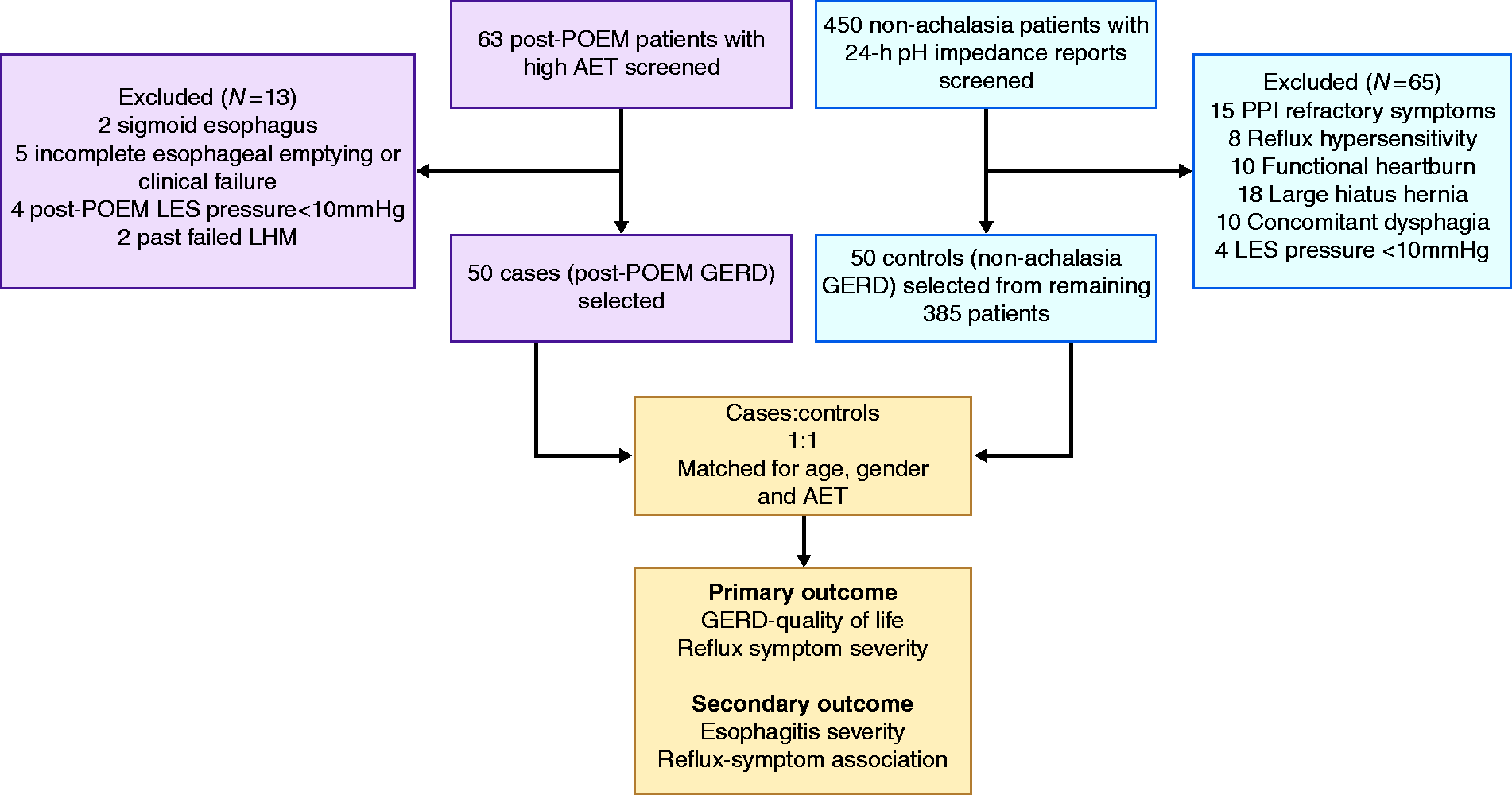
Study design and distribution of patients.
A total of 450 controls with typical reflux symptoms and who had undergone 24-h pH impedance testing off PPI were initially screened for enrollment into the control group. Of these, 65 were excluded for various reasons, including PPI refractory symptoms (15), reflux hypersensitivity (8), functional heartburn (10), large hiatus hernia (18), concomitant dysphagia (10) and resting LES pressures <10 mmHg (4). Finally, 50 controls were selected from the remaining 385 patients after matching with the cases for age, gender, resting LES pressure and esophageal AET. The median duration of PPI use in the controls was 9 months (range 3–16).
Comparison of cases and controls
The cases and controls were comparable with respect to age, gender, resting LES pressure, 24-h esophageal AET, DeMeester score and the number of non-acid reflux episodes (Table 1). Esophageal motility patterns, interpreted after POEM in the post-POEM GERD group, were significantly different between the two groups. Failed esophageal contractility (distal contractile index (DCI) <100 mmHg.s.cm in 100% swallows) was noted in 43 (86%) patients in the post-POEM group, and none in the control group. Normal and ineffective (DCI <450 mmHg.s.cm in >50% swallows) esophageal contractility were observed in two (4%) and five (10%) patients, respectively, in the post-POEM group compared with 35 (70%) and 15 (30%), respectively, in the control group (p < 0.001).
Comparison of demographic, esophageal manometric and 24-h pH impedance reflux parameters between post-POEM GERD (3 months) and control (non-achalasia GERD) groups.
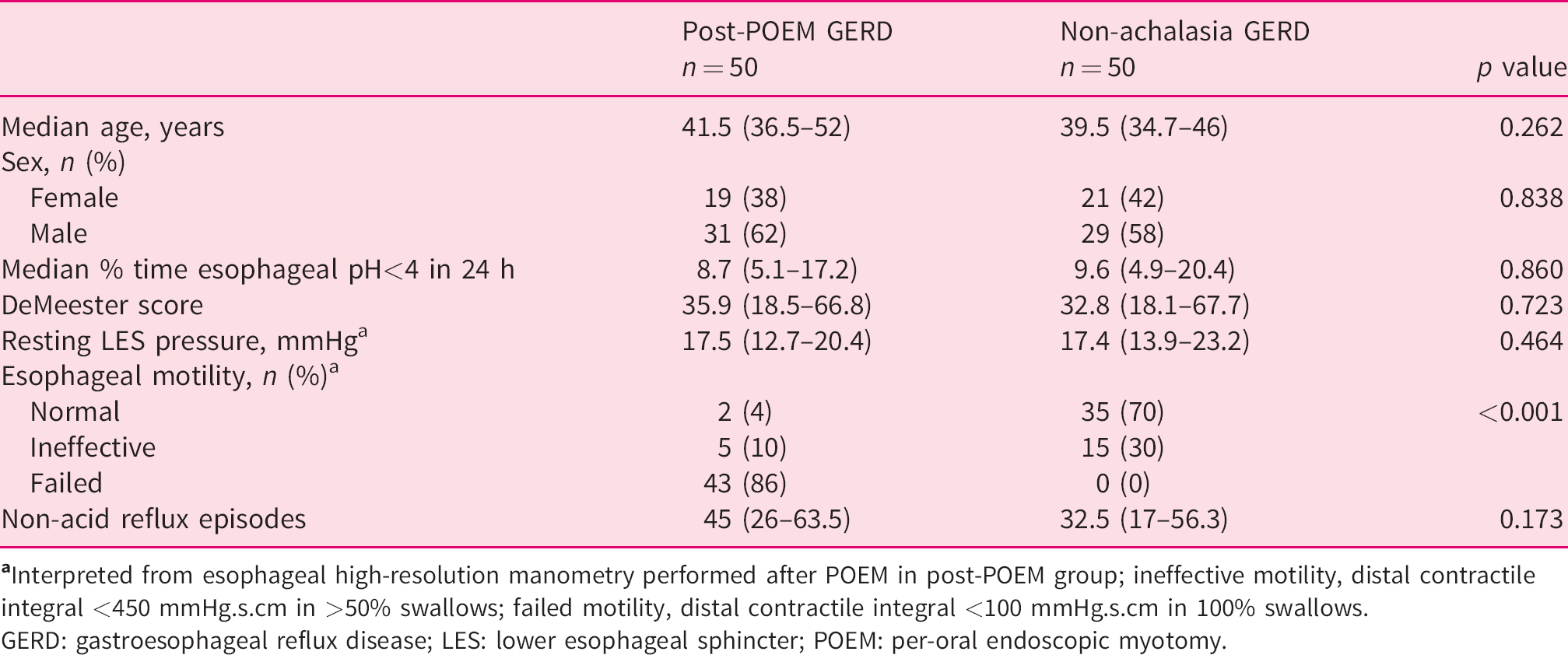
GERD: gastroesophageal reflux disease; LES: lower esophageal sphincter; POEM: per-oral endoscopic myotomy.
POEM: operative details and outcomes
POEM was performed via posterior approach (∼5 o’clock position) in 40 (80%) patients. The median time of POEM procedure was 38 min (30.7–46.2 min). The median length of total myotomy was 10 cm (range 7–20). The median length of myotomy on the esophageal and gastric sides was 7 cm (range 4–18) and 3 cm (range 1–3), respectively.
There was significant reduction in the Eckardt score from 7 (6–8) at baseline to 0 (0–1) at 3 months (p < 0.001). Median resting LES pressure and integrated relaxation pressure reduced significantly after POEM (35.7 (24.2–48.7) to 17.5 (12.7–20.4); p < 0.001) and (26.1 (20.5–34.7) to 8.9 (6.9–12.4); p < 0.001). While 30 (60%) patients reported heartburn with or without regurgitation, only three (6%) reported isolated regurgitation in the absence of heartburn at 3 months after POEM.
Primary outcome
The median GERD-HRQL total score was significantly lower in the post-POEM GERD group compared with the control group (11 (0–23.3) vs. 34 (2–44); p <0.001). As compared with the control group, the post-POEM GERD group had significantly lower median heartburn (6.0 (0–16.3) vs. 15.5 (7.5–24.8); p = 0.001) and regurgitation (0 (0–6.0) vs. 20.0 (12.3–25.0); p <0.001) symptom scores (Figure 2).
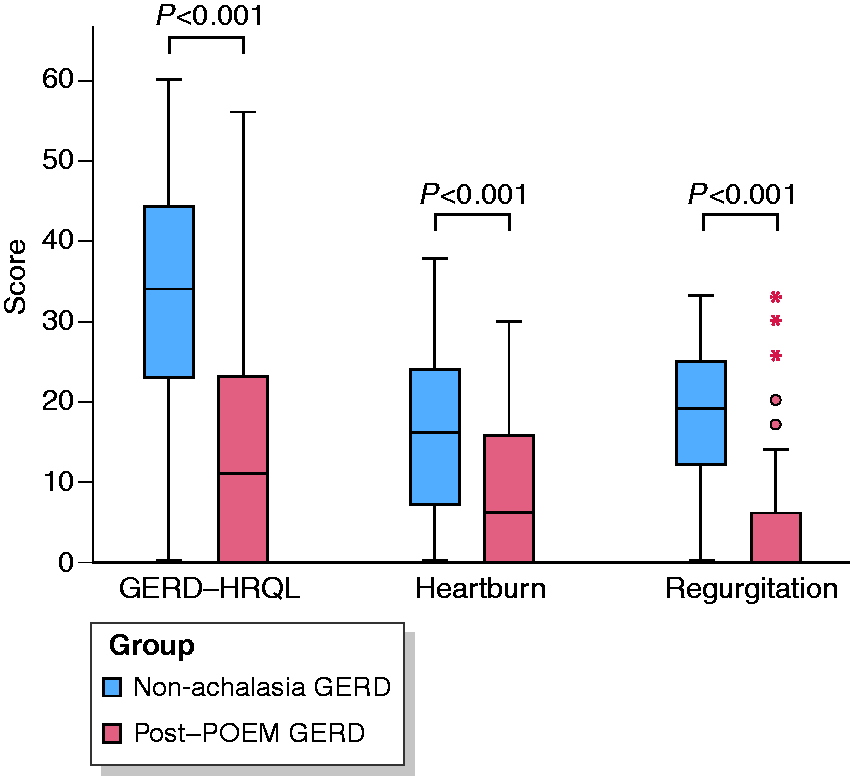
GERD related quality of life (GERD-HRQL) and symptom severity. Post-POEM GERD group had significantly lower median GERD-HRQL total score, heartburn and regurgitation symptom scores at 3 months as compared with control (non-achalasia GERD) group. Error bars indicate 95% confidence interval.
In the subgroup of patients with esophageal AET >6%, patients in the post-POEM group (n = 34) had significantly lower median GERD-HRQL total score (16 (6–24) vs. 38 (25–46); p < 0.001) with milder heartburn (10.5 (0–18.0) vs. 19.0 (9.0–25.0); p = 0.008) and regurgitation (0 (0–6) vs. 20 (14–24); p < 0.001) symptom severity as compared with the control group (n = 33) (Table 2).
Comparison of GERD related quality of life (GERD-HRQL), reflux symptom severity, grade of esophagitis, and reflux-symptom association parameters between post-POEM GERD (3 months) and control (non-achalasia GERD) groups in patients with esophageal acid exposure time >6%.
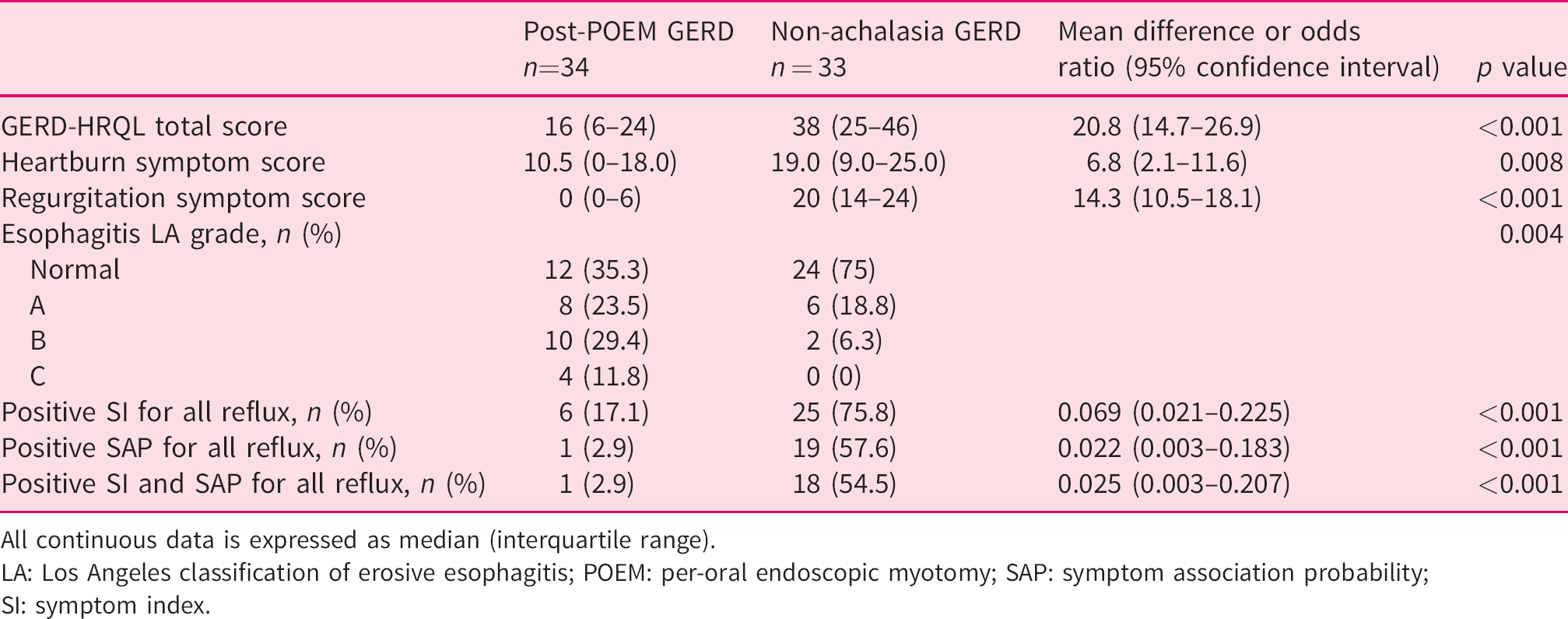
All continuous data is expressed as median (interquartile range).
LA: Los Angeles classification of erosive esophagitis; POEM: per-oral endoscopic myotomy; SAP: symptom association probability; SI: symptom index.
Secondary outcomes
The patients in the post-POEM GERD group had a more severe degree of esophagitis compared with those in the control group. Esophagitis grades A, B and C were more frequently observed in the post-POEM GERD group compared with the control group (A: nine (18%) vs. seven (14.3%), B: 13 (26%) vs. three (6.1%), C: six (12%) vs. none (0%); p = 0.001) (Figure 3). No patient in either of the groups had grade D esophagitis. In the subgroup of patients with esophageal AET >6% (post-POEM: 34; and controls: 32), esophagitis grade A, B and C were observed in eight (23.5%), 10 (29.4%) and four (11.8%) patients, respectively, in the post-POEM group compared with six (18.8%), two (6.3%) and none (0%), respectively, in the control group (p = 0.004) (Table 2).
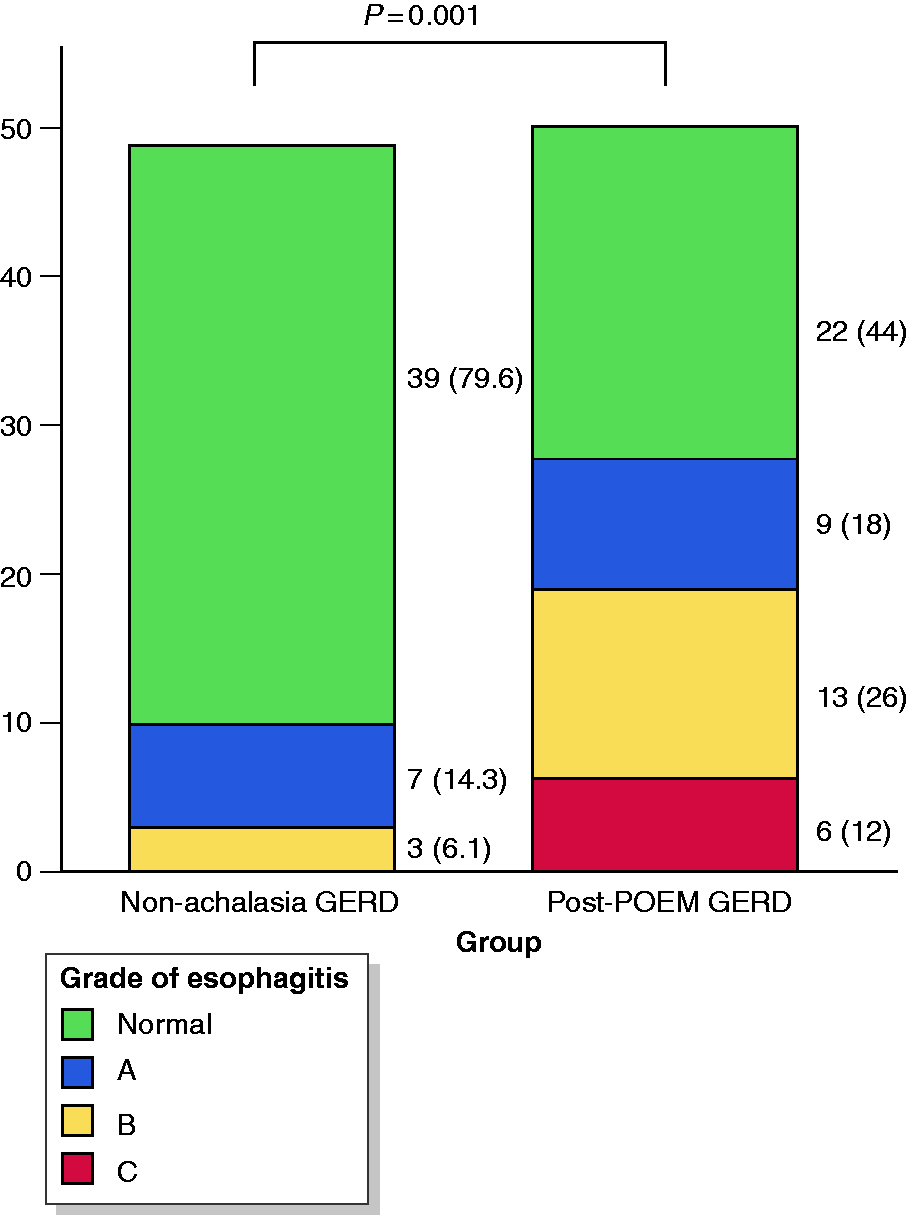
Endoscopic severity of esophagitis. Post-POEM GERD group had severe degree of esophagitis more frequently compared with control (non-achalasia GERD) group. Numbers in parentheses indicate percentage of patients in each group with respective grade of esophagitis. Grade of esophagitis was assessed according to Los Angeles classification.
The patients in the post-POEM GERD group had poor temporal association between symptoms and acid reflux episodes compared with controls (positive symptom index (five (10%) vs. 31 (62%); p < 0.001) and positive SAP (six (12%) vs. 27 (54%); p < 0.001). Similarly, fewer patients in the post-POEM group had positive symptom index (11 (22%) vs. 39 (78%); p < 0.001) and positive SAP (three (6%) vs. 29 (58%); p < 0.001) for all reflux episodes (Figure 4). There was no difference in the reflux-symptom association with non-acid reflux episodes. Only three (6%) patients in the post-POEM group had the combination of a positive symptom index and positive SAP for all reflux episodes compared with 28 (56%) patients in the control group (p < 0.001).
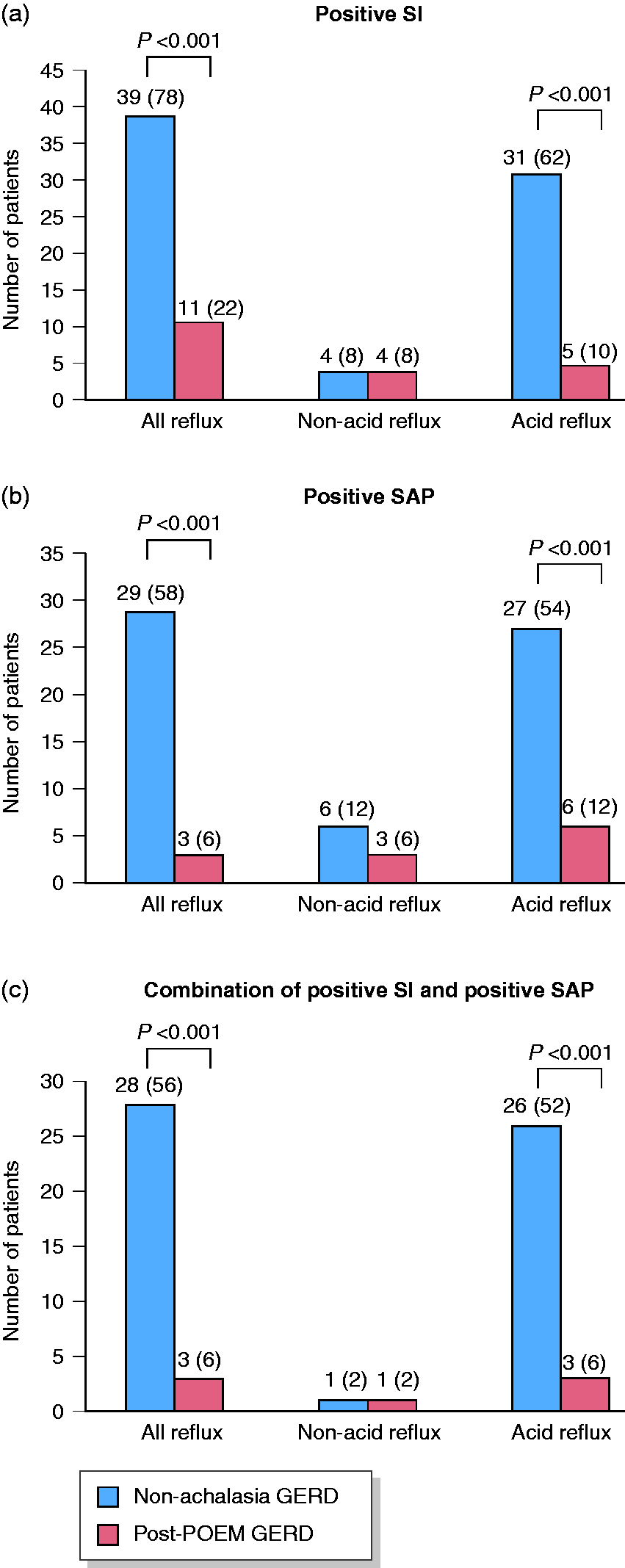
Reflux-symptom association. (a) Number of patients with positive symptom index. (b) Number of patients with positive symptom association probability. (c) Number of patients with the combination of positive symptom index and positive symptom association probability. Numbers in parentheses indicate percentage of patients in each group with positive reflux-symptom association; non-achalasia GERD indicates the control group.
In the subgroup with esophageal AET >6%, six (17.1%), one (2.9%) and one (2.9%) patients in the post-POEM group (n = 34), compared with 25 (75.8%), 19 (57.6%) and 18 (54.5%) in the control group (n = 33), had positive symptom index, positive SAP and the combination of a positive symptom index and SAP, respectively, for all reflux episodes (p < 0.001) (Table 2).
Discussion
In this study, we found that patients in the post-POEM GERD group had milder reflux symptoms as defined by GERD-HRQL scores. In addition, the post-POEM group had poor reflux-symptom association and more severe grade of esophagitis as compared with those in the non-achalasia GERD group.
GERD is considered as one of the most important delayed adverse events after POEM. 5 Recent studies indicate that the incidence of GERD is higher after POEM as compared with PBD and laparoscopic Heller's myotomy.18, 19 However, there is a paucity of literature on the qualitative analysis of GERD after POEM. GERD after POEM may be qualitatively different as compared with GERD in patients without any motility disorders. One possible reason for this difference is aperistalsis, which may affect esophageal acid clearance after POEM. 3
In this study, we compared GERD between two matched group of patients, that is, post-POEM group versus patients with GERD without an associated esophageal motility disorder. The patients with sigmoid achalasia and those with persistent stasis on TBS after POEM were excluded to avoid confounding related to stasis esophagitis.
Patients in the post-POEM group had significantly lower GERD-HRQL and reflux symptom scores compared with those in the non-achalasia GERD group. The difference in GERD-HRQL and symptom scores persisted even after re-defining GERD according to the recent Lyon consensus (AET >6%). 15 This implies that the majority of patients with post-POEM reflux remain asymptomatic in spite of having objective evidence of GERD on EGD or 24-h pH study. The results of our study are in concordance with the published literature where the incidence of symptomatic GERD after POEM is uncommon as compared with increased esophageal acid exposure or erosive esophagitis.8,12,20, 21
In the current study, heartburn was the predominant reflux symptom in the post-POEM group and only a minority (6%) of patients had isolated regurgitation. The low incidence of regurgitation in our study might be due to strict selection criteria where we excluded patients with low post-POEM LES pressures (<10 mmHg), which can predispose to volume reflux and lead to high GERD-HRQL total score.
At similar esophageal acid exposure, patients in the post-POEM group had more severe esophagitis compared with those in the non-achalasia group and the difference was maintained in the subgroup with esophageal AET >6%. This implies that reduced esophageal acid clearance due to aperistalsis may have a synergistic effect on the incidence and severity of erosive esophagitis after POEM. There were only two patients with significant recovery of peristalsis after POEM, supporting the observations of the study. On the other hand, there is a poor association between AET and the grade of esophagitis. Our observation is consistent with previous studies which conclude that there is a poor correlation between the severity of esophagitis and esophageal acid exposure.8,12,22, 23 We performed the majority of the POEM procedures via a posterior approach, which may affect the incidence of GERD by inclusion of sling fibers during myotomy. 13 However, randomized trials comparing anterior versus posterior myotomy suggest that there is no significant difference in the incidences of GERD between the two techniques of POEM.9, 24 In addition, other technical variations have not been shown to have a major impact on the incidence of post-POEM GERD.5, 8
The other important observation in our study was a poor reflux-symptom association as found using symptom index and SAP. Only 6% of patients in the post-POEM group had the combination of a positive symptom index and SAP compared with 56% in the non-achalasia group (p < 0.001); the significance persisted in the subgroup with AET >6% (p < 0.001). The combination of a positive symptom index and positive SAP is clinically more relevant in establishing a definitive association between reflux episodes and symptoms. 25 Previous studies did not report reflux-symptom association in patients with achalasia after POEM. The triviality of reflux symptoms and poor reflux-symptom association in patients after POEM in spite of a high AET and severe erosive esophagitis suggest esophageal hyposensitivity. Whether mucosal denervation during submucosal tunneling and myotomy results in esophageal hyposensitivity remains a subject of research for future studies.
There are several important implications of our study. First, GERD is qualitatively different after POEM when compared with GERD in the general population. Since the cases with low LES pressures (<10 mmHg) were excluded the difference cannot be attributed solely to hypotensive LES after POEM. Second, there is poor association between esophageal acid exposure and symptoms of GERD. Third, erosive esophagitis is more severe after POEM (versus GERD in general) at similar levels of esophageal acid exposure. This means that the patients in clinical remission after POEM should be evaluated for GERD. Early treatment should be initiated in cases with GERD to avoid delayed complications like Barrett’s esophagus and esophageal adenocarcinoma. 26
There are several strengths of our study. To the best of our knowledge, this is the first study to report and compare reflux-symptom association in patients after POEM versus non-achalasia patients. The controls were meticulously selected from a large prospectively maintained database and matched with the cases. We excluded cases with sigmoid achalasia and those with persistent stasis after POEM to avoid confounding as a result of fermentation induced drop in esophageal pH. The noteworthy limitations of the study include retrospective design and possibility of referral bias in the control group. As our hospital is a tertiary care referral center, patients presenting with symptoms of GERD are expected to have severe and poorly controlled symptoms; however, we selected only those who had their symptoms well controlled on medical therapy. Moreover, based on pH study, patients with reflux hypersensitivity and functional heartburn, who constitute approximately one-half of the PPI non-responders, were excluded. 27
In conclusion, when compared with those with non-achalasia GERD, patients with GERD after POEM have milder symptoms and poor reflux-symptom association. However, these patients have more severe esophagitis at a given rate of esophageal acid exposure. Therefore, patients in clinical remission after POEM should undergo regular surveillance irrespective of symptoms to prevent long-term complications of GERD. Large, prospective, trials are required to validate our results. In addition, the sensory perceptions of the esophagus need to be evaluated to explain the relative esophageal hyposensitivity after POEM.
Footnotes
Declaration of conflicting interests
The authors have no conflicts of interest to declare.
Ethics approval
The study was approved by the institutional ethical review board (AIG/IEC-Post BH & R 03/05.2020-03).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written, informed consent was obtained from all the study subjects and the study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki.