
Abstract
Background
The role of sexual activity on gastroesophageal reflux disease (GERD) is an under-recognized concern of patients, and one rarely assessed by physicians.
Objective
The objective of this article is to determine the influence of sexual activity on the intraesophageal acid exposure and acid reflux events in GERD patients.
Methods
Twenty-one patients with the diagnosis of GERD were prospectively enrolled. Intraesophageal pH monitoring was recorded for 48 hours with a Bravo capsule. All patients were instructed to have sexual intercourse or abstain in a random order two hours after the same refluxogenic dinner within two consecutive nights. Patients were requested to have sex in the standard “missionary position” and women were warned to avoid abdominal compression. The patients completed a diary reporting the time of the sexual intercourse and GERD symptoms. The percentage of reflux time and acid reflux events were compared in two ways: within 30 and 60 minutes prior to and after sexual intercourse on the day of sexual intercourse and in the same time frame of the day without sexual intercourse.
Results
Fifteen of 21 GERD patients were analyzed. The percentage of reflux time and number of acid reflux events did not show a significant difference within the 30- and 60-minute periods prior to and after sexual intercourse on the day of sexual intercourse and on the day without sexual intercourse, as well.
Conclusion
Sexual activity does not predispose to increased intraesophageal acid exposure and acid reflux events. Larger studies are needed to confirm our findings in patients who define reflux symptoms during sexual intercourse.
Introduction
Gastroesophageal reflux disease (GERD) is a common health problem associated with increased incidence and potential complications. GERD symptoms have a broad range of effects extending from a nuisance to disabling. Therefore, it has been shown that GERD impairs the quality of life because of various troublesome symptoms.
Sexual activity is an important factor in determining the physical, mental, emotional and social well-being; however, most of the quality of life assessment measures do not comprise sexual life. Chronic diseases such as diabetes, ischemic heart disease, irritable bowel syndrome, inflammatory bowel disease and liver diseases may be associated with sexual dysfunction due to the symptoms or due to the feeling of being chronically ill.1–7 Regarding cultural and social limitations, the impact of chronic diseases on sexual life is not usually considered unless the patients suffer from sexual dysfunction. Sexual intercourse by itself may predispose to reflux symptoms due to the positional change or partner’s pressure, particularly in women. 8 However, other factors may trigger reflux symptoms during sexual intercourse when intercourse is performed at night following dinner and sometimes after alcohol and smoking, which are clearly noxious for the esophageal epithelium.9,10 Furthermore, medications that decrease the lower esophageal sphincter pressure such as sildenafil may contribute to acid exposure. 11 On the other hand, the satisfaction of sexual activity may lead to a decreased sense of reflux symptoms with a lower pain perception, eventually enhancing the quality of life.
The term “reflux dyspareunia” was first proposed for the sexual dysfunction associated with GERD in a prospective follow-up study of 100 women because of the high rate of dyspareunia in patients with GERD. 12 Patients with a diagnosis of GERD were reported to have impairment in sexual behavior with greater difficulty in attaining orgasm and greater frequency of painful intercourse. 13 However, the impact of sexual intercourse on the clinical activity of GERD is still unknown, and an objective assessment of the severity of reflux during sexual intercourse with intraesophageal pH monitoring has not been established so far.
In the present study, we aimed to compare intraesophageal acid exposure (i) within 30 and 60 minutes prior to and after sexual intercourse, (ii) on the day of sexual intercourse and on same time frame of the day without sexual intercourse during 48-hour intraesophageal pH monitoring using a wireless pH capsule. Wireless capsule technology provides an opportunity to perform this kind of study, if taking into account the challenges of sexual intercourse with catheter-based systems.
Materials and methods
Patients with typical reflux symptoms who were seen in the Reflux Clinic of Ege University Hospital Reflux Center between 2007 and 2008 were asked to participate in the study. Patients between 18 and 65 years of age and who had the diagnosis of GERD based on typical reflux symptoms for at least six months, a validated GERD questionnaire, an upper gastrointestinal (GI) endoscopy, and a proton-pump inhibitor (PPI) test were prospectively enrolled.
Patients were excluded if they had: (1) severe esophagitis (Los Angeles (LA) Classification 14 Grade C and D), (2) Barrett’s esophagus (>3 cm by Prague criteria 15 ), (3) chronic renal disease, coronary artery disease, cardiac rhythm abnormalities, diabetes mellitus, chronic obstructive pulmonary disease, hypothyroidism, (4) bleeding or coagulation disorders, (5) previous abdominal surgery, (6) chronic treatment that could influence sexual function and gastric emptying, (7) treatment history for erectile dysfunction, (8) gastric motility disorders, or (9) no informed consent.
PPI and H2-blocker therapy were stopped 10 and two days before the study, respectively. The Institutional Review Board of Ege University Hospital approved the study and informed consent was obtained from each patient.
Bravo pH monitoring
After an overnight fast, a complete upper endoscopic examination was performed in the left lateral decubitus position, under sedation using midazolam (1–5 mg intravenously (i.v.)) and topical lidocaine for oropharyngeal anesthesia, using a flexible endoscope (GIF145; Olympus Optical Co., Hamburg, Germany). The Bravo capsule delivery system (Bravo pH monitoring system, Medtronic, Shoreview, MN, USA) was passed transorally and the capsule was attached 6 cm above the squamocolumnar junction by applying a vacuum suction pressure of >500 mmHg. 16 The location of the capsule was confirmed endoscopically following the procedure. Data recording was carried out for 48 hours. Data analysis was performed using commercially available computer software (Medtronic Inc, Fridley, MN, USA). The same endoscopist performed the procedures and placed the wireless capsules.
Study design
A standard refluxogenic high-fat diet was given to all patients on the day of Bravo capsule placement and the following day of the study. The diet included tea, egg, cheese, honey or jam, a slice of bread for breakfast; 60 gr fried meat, two medium-sized french fries, a bowl of soup, a cup of high-fat yogurt for lunch; a cup of coffee and 40 gr brownie in the afternoon; legumes, a dish of boiled pounded wheat, a cup of yogurt with cucumber and garlic and a slice of white bread for dinner; and two pieces of baklava two hours after the dinner. The diet included 2600 calories with a lipid content of 40%.
The patients were instructed to have sexual intercourse once preferably two hours after the dinner. The patients were requested to have sex in a standard “missionary position” avoiding abdominal pressure on female patients. Missionary position is the most common and classical sex position usually denoting the act in which a woman lies on her back and the man lies on top of her while they face each other and engage in sexual intercourse. All patients were asked to complete a diary reporting the exact time of the sexual intercourse with a hidden code and also to write down the heartburn and regurgitation symptoms. A blinded investigator analyzed the recording of the Bravo pH monitoring and the clinical data obtained from the diaries.
Assessment of reflux symptoms and reflux events
“Heartburn” was defined as a burning sensation arising from the stomach or lower part of the chest toward the neck.
17
“Regurgitation” was defined as the perception of flow of refluxed gastric content into the mouth or hypopharynx.
17
An acid reflux event was defined as a pH drop below 4.0 persisting for at least 4 seconds. Reflux time was measured as the percentage of time pH<4.0 (%). On the day of sexual intercourse, total time pH<4.0 (%) within 30 and 60 minutes prior to and after sexual intercourse was compared. On the day without sexual intercourse, the pH<4.0 (%) was determined within the 30- to 60-minute period after the corresponding time of the sexual intercourse on the previous day, and compared with the values on the day with sexual intercourse (Figure 1).
Study design. All patients had the same standard refluxogenic dinner, and two hours later patients were asked to have sexual intercourse for one day and not having sex on the following day. The eating period was started at the same hour on the following day.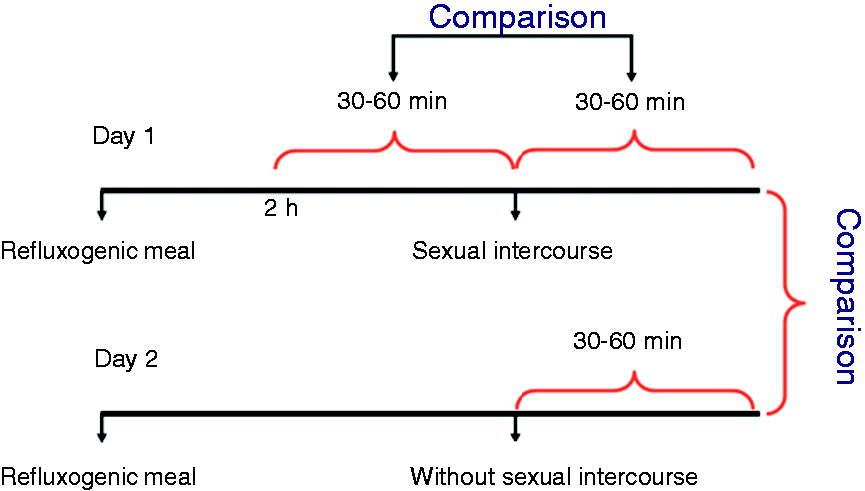
Statistical analysis
Statistical analysis was performed by using the SPSS 18.0 software program (SPSS, Chicago, IL, USA). Data are expressed as mean ± SD, median (range) and percentages. Appropriate tests were used for comparing data including the Student’s paired t test, the chi-square test, and Wilcoxon’s signed rank test. p values less than 0.05 were accepted as statistically significant.
Results
A total of 21 patients were enrolled. Six patients were excluded as two had lack of pH monitoring due to the placement of the Bravo data receiver apart from the body during sexual intercourse, one did not have sexual intercourse because of initiation of menstrual period, two did not perform sexual intercourse for personal reasons after consent to participate the study and one was excluded because of technical problems with the system. Of the 15 patients included in the analysis, mean age was 43 ± 8 years, and roughly two-thirds of the patients (10 patients) were men. Eleven (73%) patients had normal endoscopy while four had esophagitis; of these, three had grade B esophagitis and one had grade A esophagitis. Mean 24-hour pH was 17.3 ± 8.7 on the worst day of recording. Median reflux time and reflux events at the time of sexual intercourse and on the corresponding time without sexual intercourse were comparable.
Intraesophageal pH values prior to and after sexual intercourse
The median (range) reflux time percentage within the period of 30 minutes prior to and after sexual intercourse was 21.3 (0–61.7) and 10 (0–70.3), respectively. The median (range) reflux time percentage within the period of 60 minutes prior to and after sexual intercourse was 16 (0–51) and 5.7 (0–61.7), respectively. Compared to the reflux time prior to sexual intercourse, percentage of reflux time tended to be lower within the 30 and 60 minutes after sexual intercourse. However, paired analysis comparing the individual changes of the patients prior to and after sexual intercourse did not show a statistically significant difference. The changes of pH monitoring before and after sexual intercourse in the 15 individual patients are shown in Figure 2.
Bar chart comparing the percentage of reflux time (a) within 30 minutes prior to and after sexual intercourse, (b) within 60 minutes prior to and after sexual intercourse.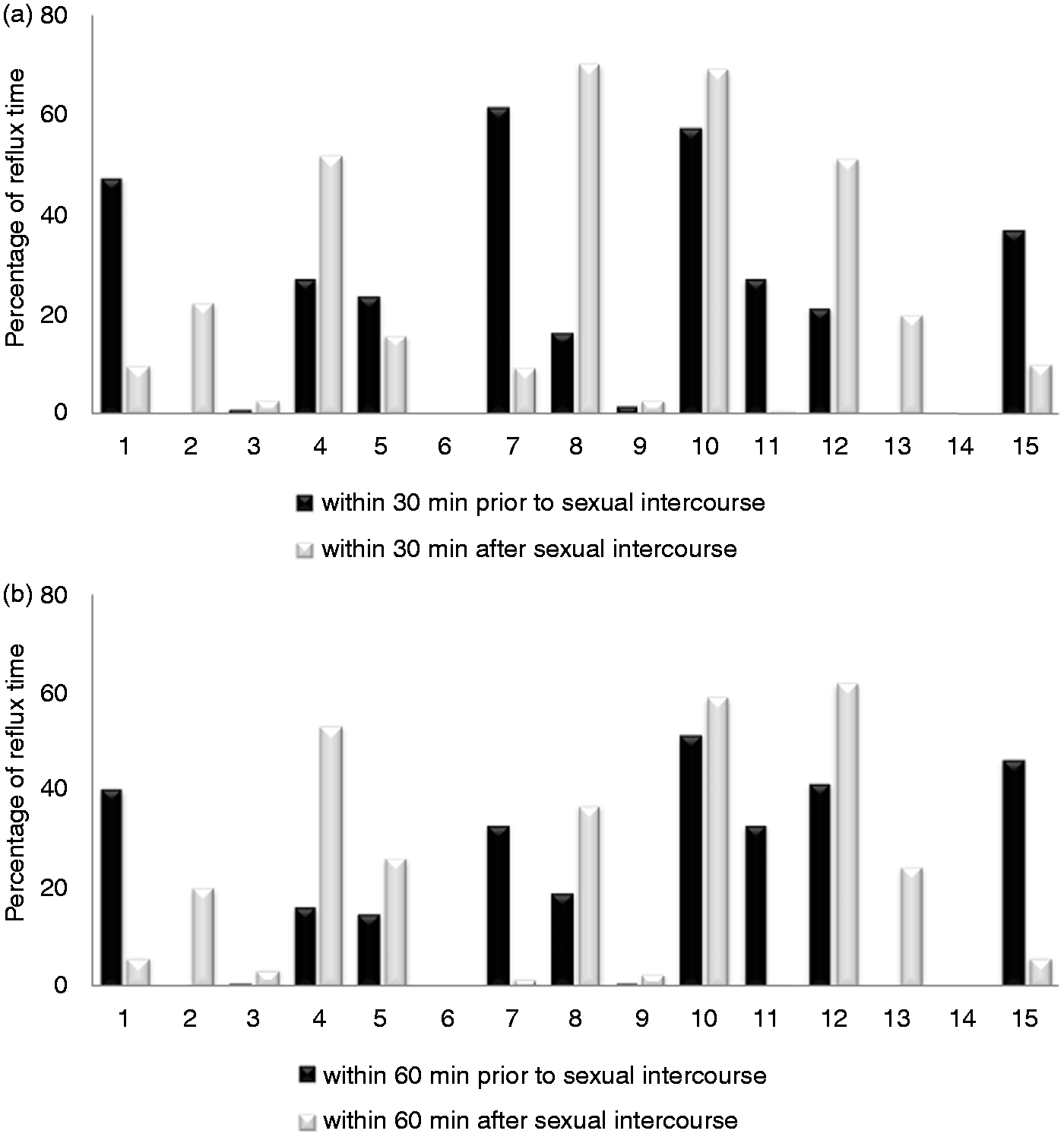
Comparison of intraesophageal pH values on the day with and without sexual intercourse
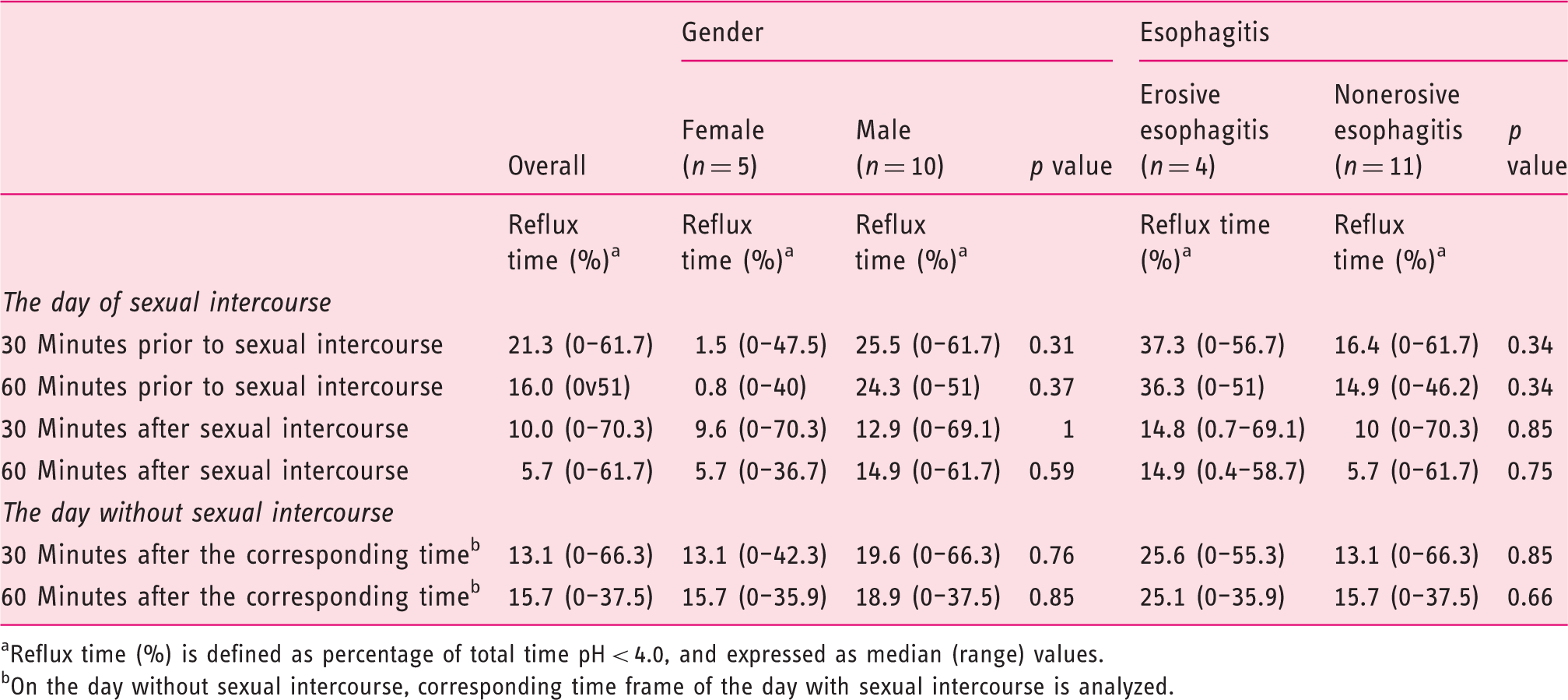
The median (range) reflux time percentage within the 30-minute period after sexual intercourse on the day of sexual intercourse and in the corresponding time frame of the day without any intercourse was 10 (0–70.3) and13.1 (0–66.3), respectively. The median (range) reflux time percentage within the 60-minute period after sexual intercourse on the day of sexual intercourse and on the corresponding time frame of the day without sexual intercourse was 5.7 (0–61.7) and 15.7 (0−37.5), respectively. Although women tended to have higher reflux after sexual intercourse, subgroup analysis based on gender and presence or absence of esophagitis did not show a significant difference of reflux % prior to or after sexual intercourse and on the day with and without sexual intercourse (Table 1). The individual changes in pH monitoring on the day with and without sexual intercourse are shown in Figure 3.
The comparison of percentage of reflux time on the day with and without sexual intercourse (a) within 30 minutes after sexual intercourse, and (b) within 60 minutes after sexual intercourse. Percentage of reflux time on the day of sexual intercourse and on the day without sexual intercourse Reflux time (%) is defined as percentage of total time pH < 4.0, and expressed as median (range) values. On the day without sexual intercourse, corresponding time frame of the day with sexual intercourse is analyzed.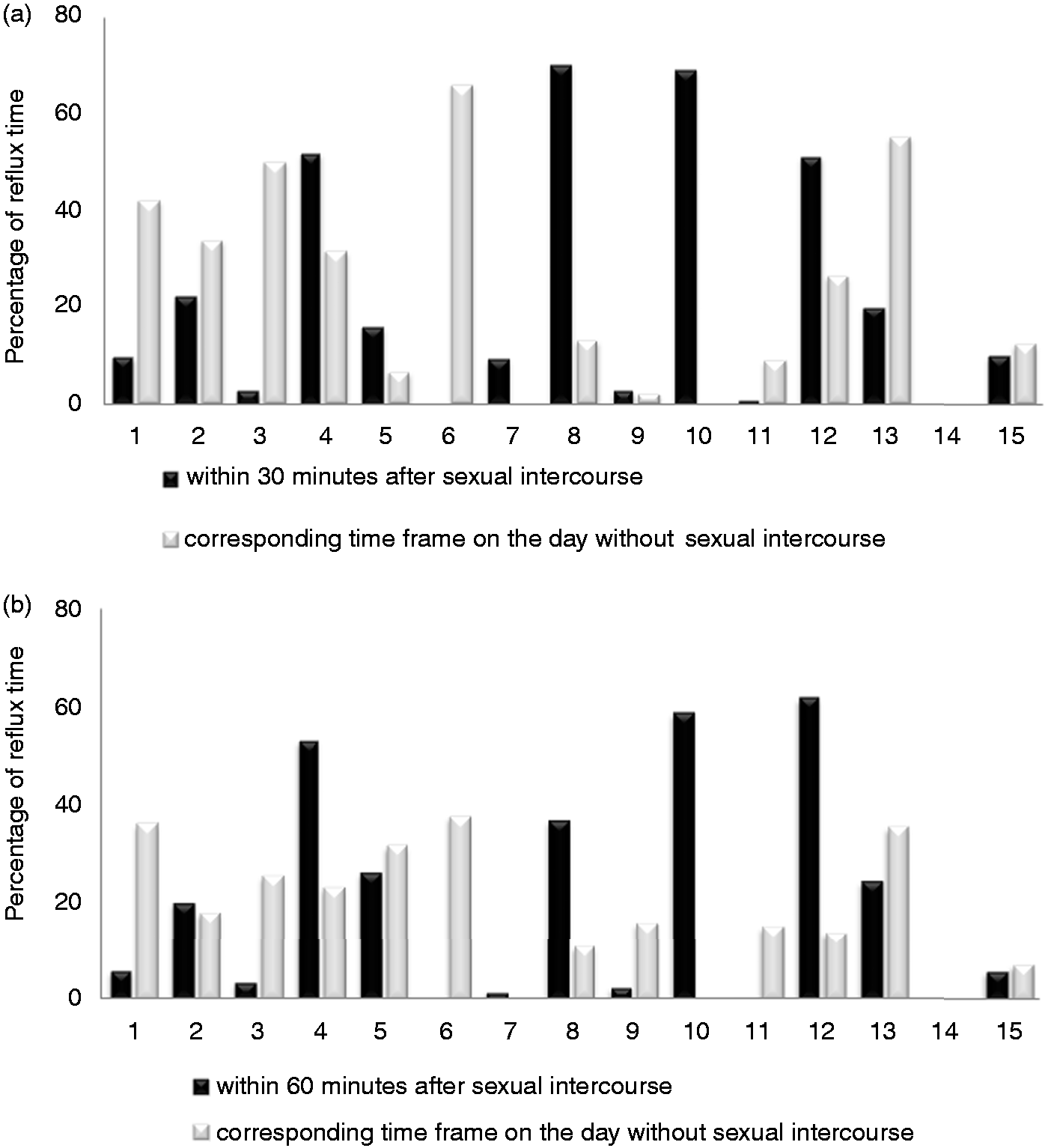
Number of reflux events
Number of reflux events on the day of sexual intercourse and on the day without sexual intercourse
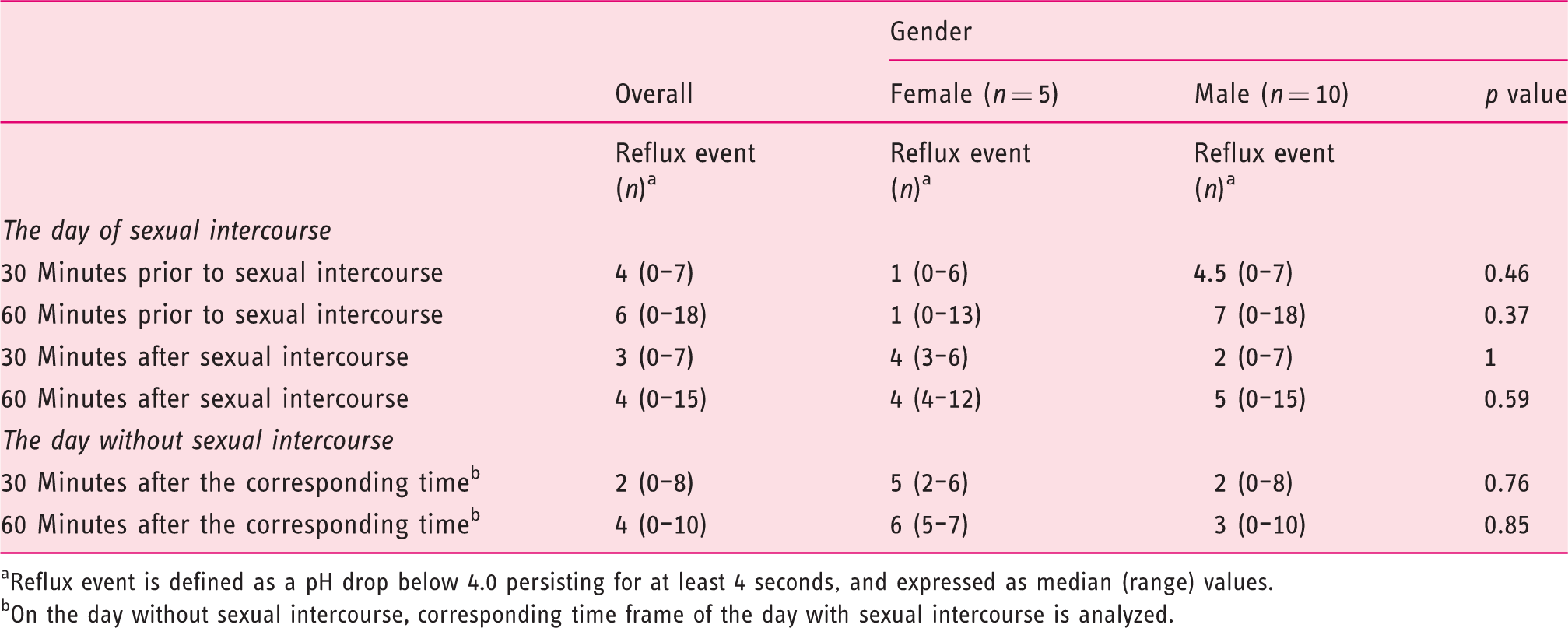
Reflux event is defined as a pH drop below 4.0 persisting for at least 4 seconds, and expressed as median (range) values.
On the day without sexual intercourse, corresponding time frame of the day with sexual intercourse is analyzed.
Discussion
It is not unusual that patients may suffer from GERD symptoms during and after sexual intercourse. To the best of our knowledge, this study therefore represents one of the first attempts to examine the changes of reflux episodes and intraesophageal acid exposure during sexual intercourse, providing objective evidence based on wireless pH monitoring. The majority of the studies that assessed the effects of sexual intercourse on GERD were focused on questionnaire-based studies about GERD, sexual behavior and quality of life. This study found that sexual intercourse was not a predisposing factor in increasing the intraesophageal acid reflux episodes; moreover, symptomatic reflux episodes and intraesophageal acid exposure were similar on the day of sexual intercourse and on the day without sexual intercourse.
In this study of 15 patients with the diagnosis of GERD, we focused on the 30- and 60-minute time period before and after sexual intercourse and compared the intraesophageal pH values and reflux events before and after sexual intercourse following a refluxogenic meal. The wireless pH monitoring system was used to allow the patients to maintain their regular activities, including the sexual activity. Intraesophageal pH measurements were assessed on the day without sexual intercourse in the corresponding time frame. We did not find a significant difference related to sexual intercourse either “before and after sexual intercourse” or “on the day with and without sexual intercourse.” To assess the reflux perception, heartburn and regurgitation symptoms were recorded in a diary by patients; only one patient had heartburn 30 and 60 minutes before sexual intercourse, while none of the other patients had heartburn or regurgitation. However, inclusion of patients having reflux symptoms during sexual activity may allow a better assessment of reflux perception. Although women tended to have a higher percentage of reflux, subgroup analysis based on gender and presence or absence of esophagitis did not reveal any difference in the percentage of reflux time and number of reflux events. Iovino et al. reported that untreated GERD patients had difficulty in attaining orgasm and experienced pain during intercourse compared to healthy controls. 13 They also reported improved sexual behavior in patients who underwent surgical treatment for GERD compared to those who were on medical treatment. It is an important concern whether these patients had sexual behavioral disorders due to reflux during sexual intercourse or due to the psychological burden of chronic illness. Apart from the pathological acid exposure, changes in sexual behavior, which were reported in the previous studies, may be related to the feeling of being chronically ill or non-acid refluxes.
Sexual activity is a vigorous action and may involve different positions that may predispose to acid reflux. Physical activity may lead to a decrease in GI blood flow as a result of sympathetic stimulation.17–19 It has been shown that physical activity may decrease contraction pressures at the mid-esophagus and peristaltic motility at the mid and distal esophagus and may delay gastric emptying.19–21 Moreover, exaggerated pressure fluctuations between the thorax and abdomen during the exercise may challenge the gastroesophageal barrier and allow reflux of gastric juice into the esophagus.8,22 It is hard to determine the level of physical activity during sexual activity. Kirk’s study that first defined the term “reflux dyspareunia” proposed that the supine position and the increased abdominal pressure may be responsible for symptoms during intercourse. 12 Following a management plan including lifestyle changes, they observed an improvement in 79% of patients who suffer from reflux symptoms during sexual intercourse. However, this study was conducted before the clinical use of intraesophageal pH monitoring tools, and the definition of GERD was based on any complaint of heartburn investigated by contrast radiography or endoscopy. Kirk’s conservative management plan also included that the “female superior position” may be an alternative position to “missionary position” to decrease the reflux symptoms. He found an improvement of reflux symptoms, but the contribution of the position change among the other recommendations was not clearly defined. In our study, missionary position was chosen to standardize the position, as this is the most common position and was feasible to explain to the patients. Although the patients were warned to avoid abdominal pressure, there might still be an inevitable degree of abdominal compression. The vast majority of the patients were male, female patients were in the supine position and the males were on top. Earlier studies reported more frequent reflux episodes in the supine position during sleep.23,24 In our study group, intraesophageal acid exposure and reflux events were comparable in both genders and the role of the sexual position on reflux couldn’t be confirmed with our findings.
There were limitations to this study. First, the small number of participants and the lack of a patient group with reflux symptoms during sexual intercourse were the main limitations of this study. However, cultural and social limitations were the major challenges for participation of volunteers. Second, the exact time, period and the position of the sexual intercourse were self-reported, if performed. Third, we investigated acidic reflux events only by Bravo pH monitoring. In a recent study, we showed that number of acid reflux episodes decreases while non-acid reflux episodes increase one hour after meals. 25 Twenty-four-hour impedance-pH monitoring was another option to detect weak and non-acid refluxes since patients were asked to have intercourse two hours following the meal. However, it would not be physiologically feasible to perform sexual activity with a catheter-based system for volunteers, and the likelihood of non-acid reflux producing a different symptom profile might be lower than acidic reflux in this setting. Finally, as Bravo pH monitoring is contraindicated in patients with severe esophagitis, patients with grade C and D esophagitis were excluded, which may lead to a selection bias.
In conclusion, this study of GERD patients who underwent 48-hour Bravo pH monitoring showed that sexual activity did not lead to increased intraesophageal acid exposure and reflux events. However, confirmation of these results in larger studies evaluating the role of weakly acidic and non-acid reflux events and among patients who have reflux symptoms during sexual intercourse is warranted.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.