
Abstract
Albumin is currently employed as a plasma expander to prevent and treat specific complications of cirrhosis with ascites, such as the prevention of paracentesis-induced circulatory dysfunction and renal dysfunction induced by spontaneous bacterial peritonitis, as well as the diagnosis and treatment of acute kidney injury and hepatorenal syndrome. Recently, evidence has shown that long-term albumin administration in patients with decompensated cirrhosis reduces mortality and incidence of complications, eases the management of ascites, is cost effective, and has a good safety profile.
Keywords
Brief clinical case
A 69-year-old female with cirrhosis was hospitalized due to development of ascites. In total, 5 L of fluid were removed by paracentesis. The ascites leukocyte count showed 380 neutrophils per µL. Subsequently, renal function progressively worsened and acute kidney injury (AKI) stage 1B was diagnosed. Once the infection and renal impairment were resolved, the patient was discharged under diuretic therapy. In the following months, as ascites persisted despite diuretics, long-term treatment with human albumin (HA) was instituted.
Diagnostic framework of ascites in decompensated cirrhosis
In developed countries, cirrhosis is the most frequent cause of ascites, accounting for almost 80% of cases. Malignant neoplasms, heart failure, tuberculosis, pancreatic disease, and other uncommon diseases are responsible for the remaining cases. 1 Ascites is the most frequent complication of cirrhosis, occurring in 5–10% of compensated patients every year.
An appropriate evaluation of patients with cirrhosis and ascites includes detailed anamnesis collection, physical examination, abdominal ultrasound, and laboratory analyses. Diagnostic paracentesis is essential for differential diagnosis and recommended in all patients developing moderate to severe ascites and in those hospitalized for any cause. 2 Mandatory analyses of ascitic fluid consists of the assessment of differential leukocyte counts, protein and albumin concentrations, and cultures.2,3
The serum-ascites albumin gradient should also be calculated and a result of ≥1.1 g/dL suggests portal hypertension is involved in ascites formation with a very high accuracy.
4
Although evidence is not conclusive, total protein concentration < 1.5 g/dL is considered a risk factor spontaneous bacterial peritonitis (SBP).
5
Other tests, such as cytology and amylase and for mycobacteria (polymerase chain reaction and culture) and carcinoembryonic antigen should be evaluated on a case-by-case basis (Figure 1).2,6
Diagnostic algorithm for new onset ascites. Among the additional tests on ascitic fluid, low glucose levels are associated with tuberculosis or peritoneal carcinomatosis and bacterial peritonitis. High concentrations of lactic dehydrogenase (LDH) should lead to the suspicion of a non-hepatic cause, in particular a malignant etiology, peritonitis secondary to intestinal perforation, acute pancreatitis, and tuberculous peritonitis. The combined determination of total proteins, glucose, and LDH has also been proposed to differentiate forms of spontaneous from secondary bacterial peritonitis (proteins > 1 g/dL, glucose <50 mg/dL, high LDH). High levels of amylase can be found in pancreatic ascites or intestinal perforation, ischemia, and mesenteric thrombosis, whereas the dosages of creatinine and bilirubin are useful in the suspicion presence of urine and biliary or intestinal perforation respectively. Opalescent ascitic fluid would require the dosage of triglycerides, as levels higher than 200 mg/dL indicate chylous ascites. An activity of the adenosine-deaminase enzyme (ADA) greater than 39 IU/L suggests the diagnosis of tuberculous ascites, although this dosage is only useful in areas with high prevalence and in the absence of liver cirrhosis.
6
CT: computed-tomography; MR: magnetic resonance.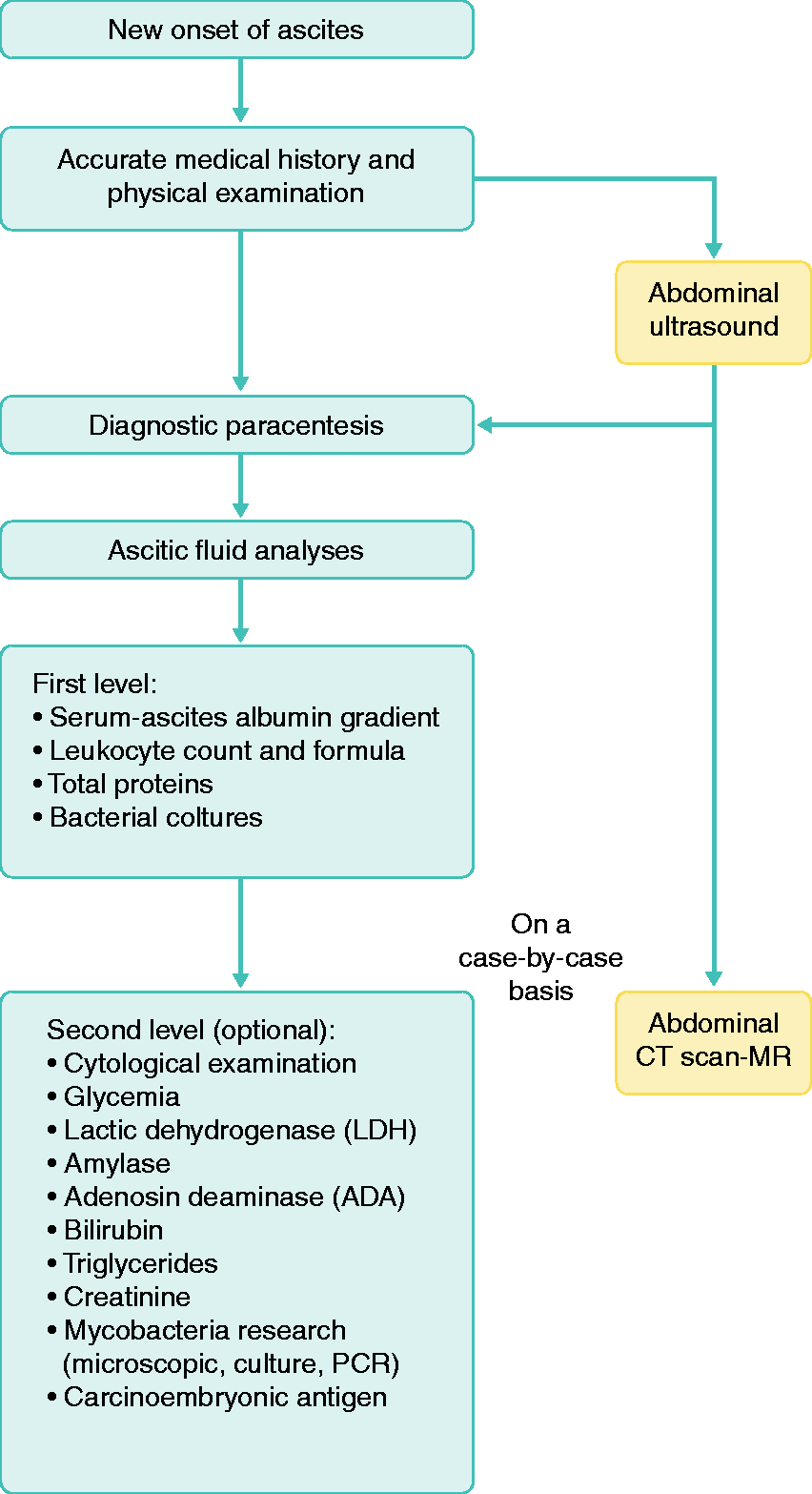
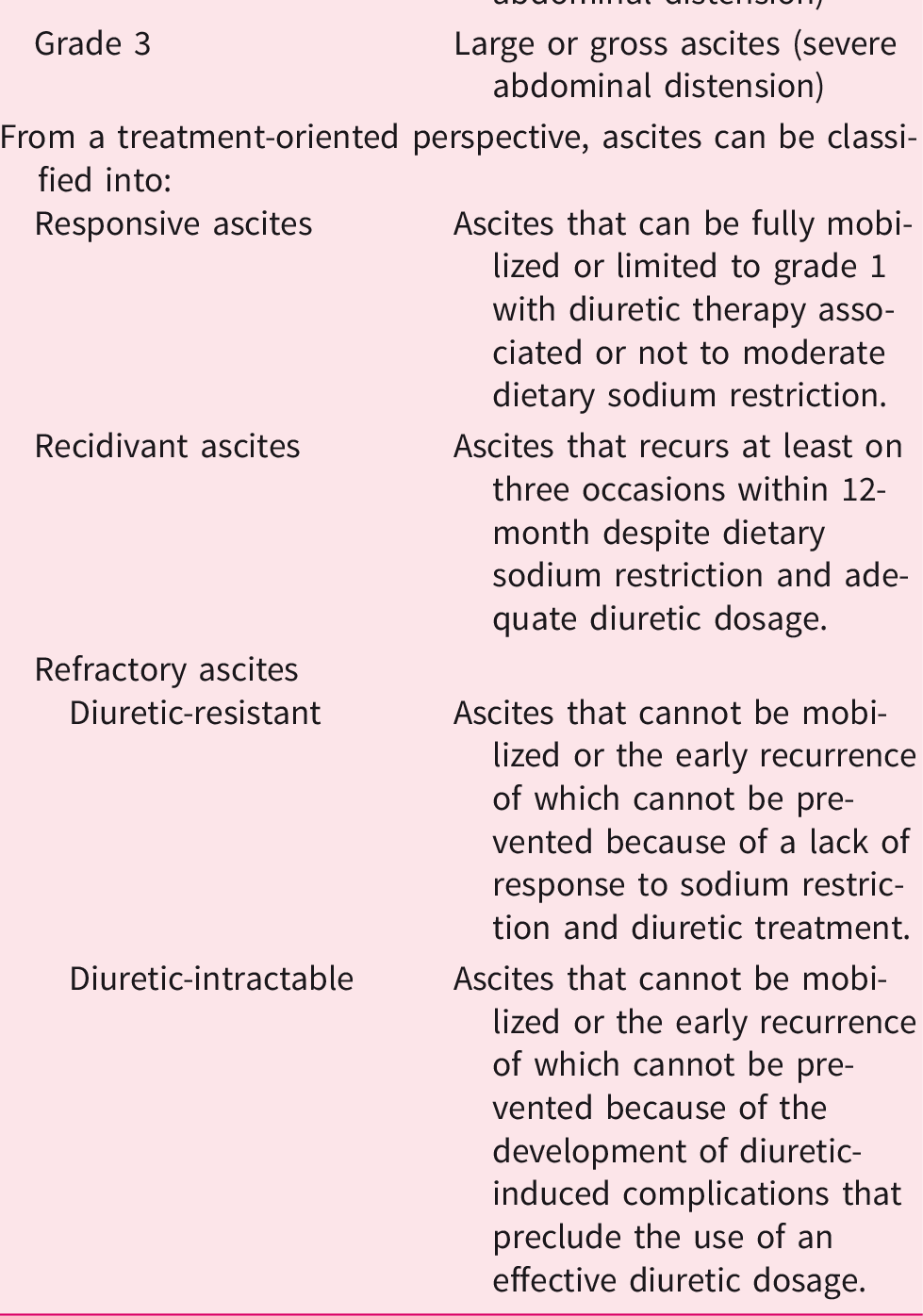
Classification of ascites.
Clinical manifestations of ascites affects patients’ working and social lives, requires chronic treatment and recurrent hospitalizations, and can lead to further complications. 3 Large volume paracentesis (LVP) is the current treatment of choice for managing grade 3 ascites. 2 LVP carries the risk of paracentesis-induced circulatory dysfunction (PICD), which is denoted by an increase >50% in plasma renin activity 4–6 days after paracentesis, witnessing a decline of effective volemia, 7 including an abrupt fall in abdominal pressure, and a boost in venous return, and, consequently, cardiac output. This leads to an excessive drop in peripheral vascular resistance being responsible for a decline in effective volemia. PICD clinical manifestations are arterial hypotension, renal dysfunction, dilutional hyponatremia, hepatic encephalopathy (HE), and lower survival. 7
SBP is the most common bacterial infection in patients with ascites. Diagnosis is made when the ascites neutrophil count exceeds 250 cells per µL in the absence of any intra-abdominal source of infection.2,5
Due to its frequency and potential severe prognosis, SBP should be ruled out in all patients with cirrhosis and ascites at every hospital admission and at the development of HE, worsening of liver and/or renal function, fever, shock, gastrointestinal symptoms, and gastrointestinal bleeding, as bacterial infections frequently occur in this setting. 2
International Club of Ascites (ICA-AKI) definitions for the diagnosis and management of acute kidney injury in patients with cirrhosis.
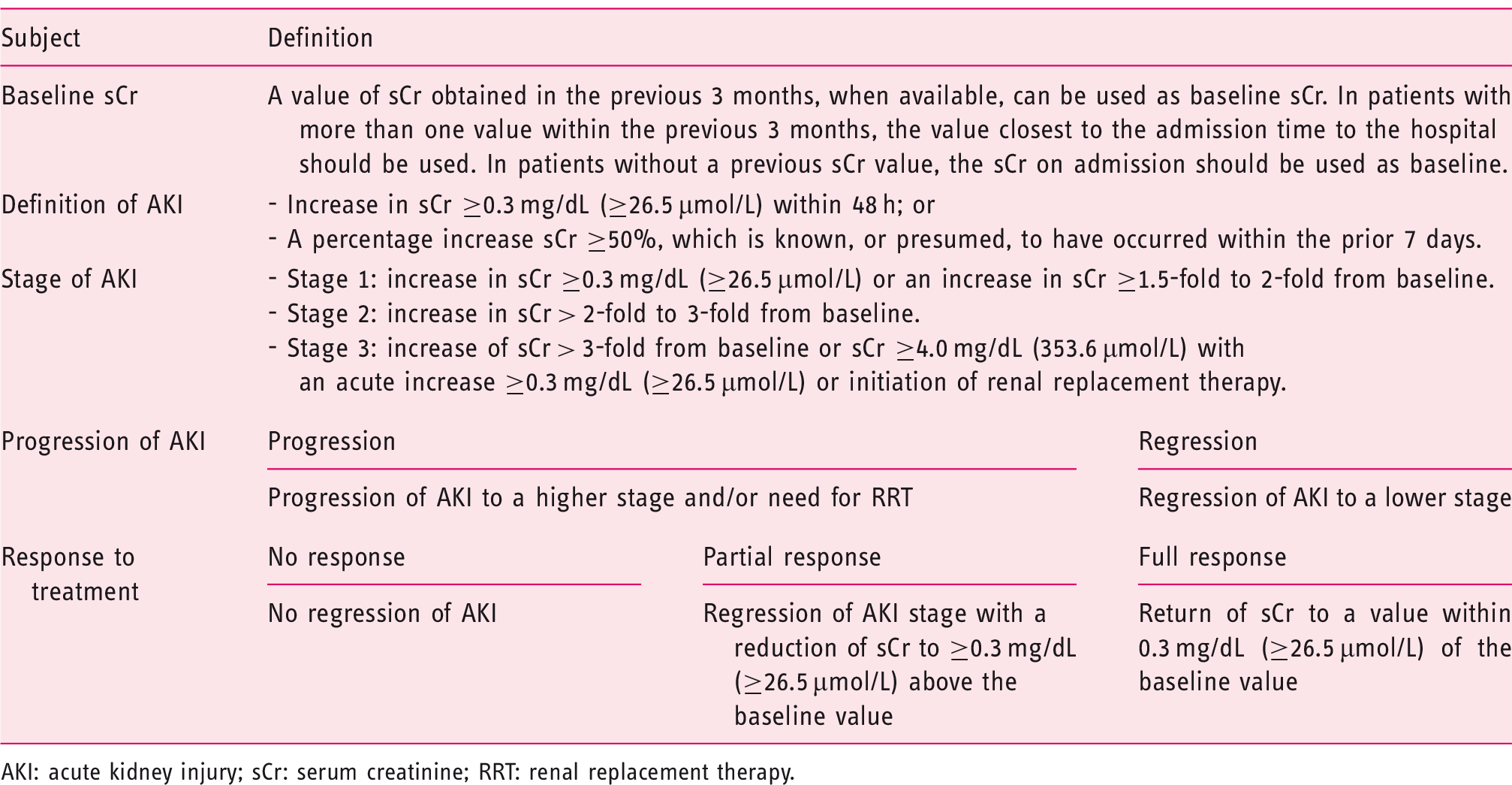
AKI: acute kidney injury; sCr: serum creatinine; RRT: renal replacement therapy.
All types of AKI can occur in decompensated cirrhosis, the most frequent being pre-renal. It accounts for almost 70% of cases and is corrected by plasma volume expansion. In addition to intrarenal or intrinsic (acute tubular necrosis, ATN) and, rarely, post-renal AKI, patients with cirrhosis can present a distinctive form named hepatorenal syndrome (HRS-AKI), which is often precipitated by hepatic (e.g. alcohol abuse, drugs) and extrahepatic insults (e.g. bacterial infections). 10 HRS-AKI is recognized by the lack of response to plasma volume expansion with HA, absence of shock, and no evidence of parenchymal disease. 9 Once the diagnosis is established, treatment with vasoconstrictors (mainly terlipressin) and HA, which leads to the resolution or improvement of HRS-AKI in 50–60% of cases, should be instituted. The differential diagnosis between HRS-AKI and ATN is not always easy, especially in cases precipitated by sepsis. The use of biomarkers of tubular damage such as urinary neutrophil gelatinase-associated lipocalin has been suggested, but this shortcoming has not yet been fully overcome. 2
Natural history of ascites and decompensated cirrhosis
The onset of ascites represents a clear watershed on the course of cirrhosis, leading to a dramatic worsening of prognosis as the 1, 2, and 5-year mortality rates rise to about 40%, 50%, and 70%, respectively. 1 Thus, patients with ascites should be evaluated for liver transplantation. 2 It should be considered that these patients may not be given proper priority in transplant lists because underscoring by the most widely used prognostic tools (Model For End-Stage Liver Disease (MELD) and MELD-Na), which do not include powerful predictors of mortality such as arterial hypotension, low renal filtration rate, and sodium excretion. 11 Thus, superior methods to estimate prognosis in cirrhosis with ascites are desirable. 2
The clinical course of patients with ascites is heterogeneous due to many interplaying factors: response to etiologic treatments of the underlying cirrhosis, efficacy of and patients’ compliance to the therapy of ascites (diuretics), onset of complications, and progression of liver dysfunction and portal hypertension. Ascites recurring at least thrice yearly despite appropriate treatment is defined recidivant, whereas refractoriness refers to the lack of response to diuretics (diuretic resistant) or to the failure to reach effective diuretic dosages without inducing side-effects (diuretic intractable). 2 Although patients with recidivant ascites seem to have a survival comparable with those with responsive ascites, 12 refractory ascites is associated with a substantial reduction in survival probability, which does not exceed 6 months. 13
SBP is an ominous event, potentially leading to severe circulatory dysfunction, deterioration of liver function, HE, and HRS-AKI. Early diagnosis and prophylaxis with HA reduce mortality from approximately 30% to 10%. 14 Patients recovering from an episode of SBP are at high risk of recurrence (approximately 70% at 1 year) and their probability of survival falls to 30–50% at 1 year and 25–30% at 2 years. 6 Thus, prophylaxis with Norfloxacin (400 mg/day) is recommended. 2
The onset of AKI also worsens the prognosis of patients with cirrhosis, due to the higher probability of a longer hospital stay, need to transfer to an intensive care unit, and increased mortality. 9
Finally, about one-third of patients with cirrhosis hospitalized because of acute decompensation present, either at admission or during hospitalization, a distinct clinical syndrome, acute-on-chronic liver failure (ACLF), characterized by hepatic and/or extrahepatic organ failure, intense systemic inflammation, and high 28-day mortality. 15
Current indications of albumin in decompensated cirrhosis
The traditional medical management of decompensated cirrhosis aims to prevent and treat specific complications (Figure 2). Based on the peripheral arterial vasodilation hypothesis,
16
HA has been employed as a plasma expander to improve effective volemia.
2
Indeed, HA represents the primary regulator of fluid partition in different body compartments by sustaining plasma oncotic pressure at almost 80%.
Albumin in decompensated cirrhosis with ascites.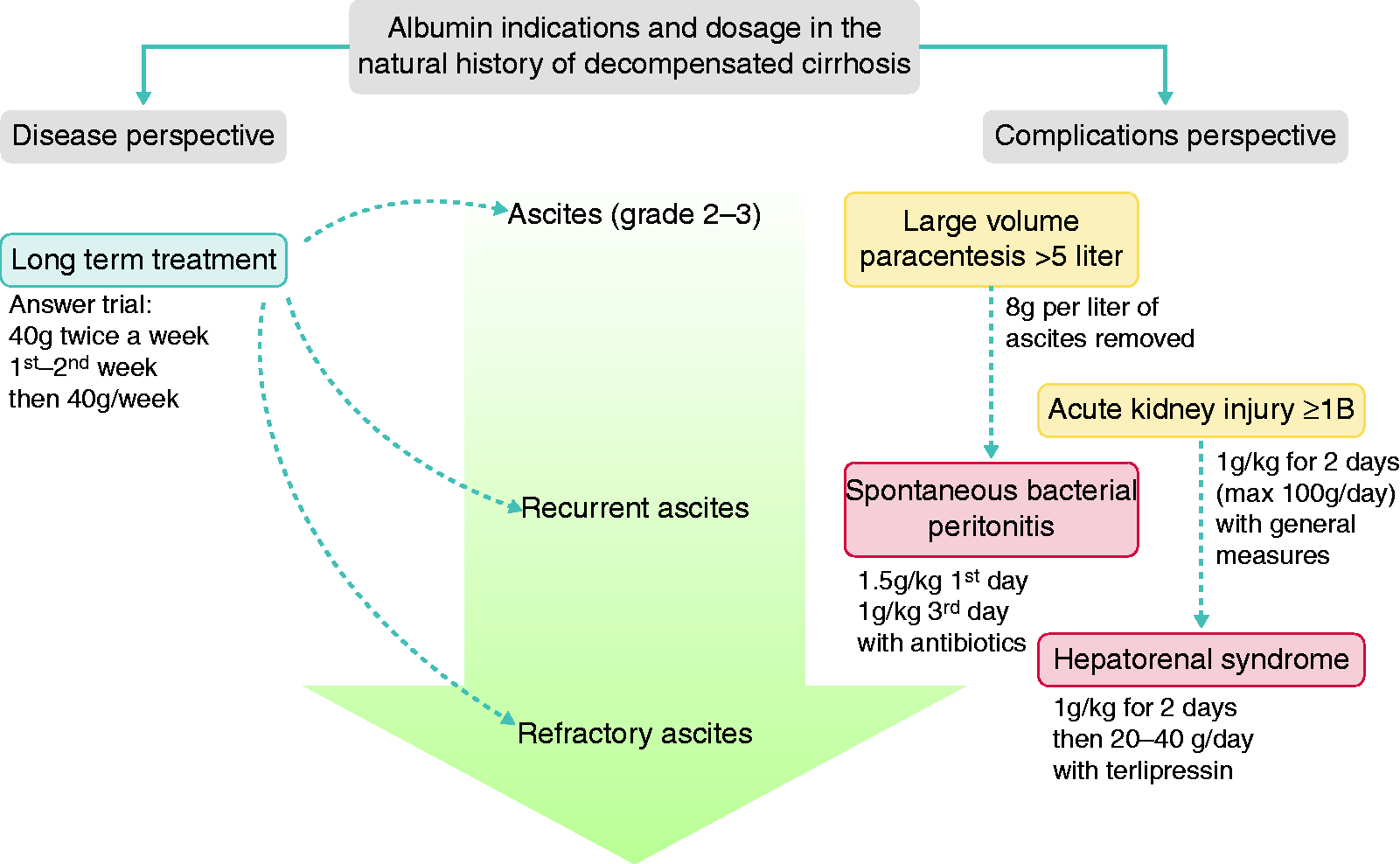
More recently, the knowledge of the pathophysiological background of decompensated cirrhosis has improved. It is now clear this condition is characterized by a sustained pro-inflammatory and pro-oxidant milieu resulting from the systemic spread of pathogen-associated molecular patterns (PAMPs) and damage-associated molecular patterns (DAMPs) from the gut and the diseased liver, respectively. 17 Enhancements of these mechanisms are the primary drivers of acute decompensation and ACLF. 18
In this context, HA could play a relevant therapeutic role, far above mere volume expansion. Indeed, thanks to its non-oncotic properties potentially counteracting several pathophysiological mechanisms, long-term HA administration is emerging as a disease-modifying treatment in decompensated cirrhosis. 19 In fact, HA is the main antioxidant in the human body that counteracts reactive oxygen and nitrogen species, exerts an essential role of transport and detoxification, contributes to the integrity of endothelia, and regulates inflammatory and immunological pathways.20–22 In vitro studies and experimental models of cirrhosis shed light on the mechanisms contributing to the immunomodulatory properties of HA, such as binding a wide range of offending molecules, including PAMPs and DAMPs, and modulating antigen-presenting cell functions and cytokine synthesis and release. 23 These effects have been confirmed in patients with decompensated cirrhosis, as the administration of high (but not low) doses of HA reduced the plasma levels of several cytokines. 24 Finally, HA also exerts a crucial role in preserving endothelial functions by binding the interstitial matrix and interacting with the sub-endothelium space.23,25
The display of non-oncotic properties requires the structural and functional integrity of the HA molecule, which is endangered by systemic inflammation and oxidative stress. Circulating oxidized forms of HA increase in decompensated cirrhosis and, to a greater extent, ACLF.26,27 Interestingly, in these settings, oxidized HA enhances the inflammatory response by peripheral blood mononuclear cells. 28 Besides oxidation, many other structural changes of HA were described, so the circulating amount of native, functionally intact HA can be dramatically reduced. 27 Notably, HA abnormalities are closely associated with patient outcomes and mortality.26,27
Albumin for the prevention of PICD
To prevent PICD after LVP, HA is infused to expand plasma volume. 2 When more than 5 L are removed, randomized trials and meta-analyses showed that HA administration (8 g/L of ascites evacuated) is better than any alternative volume expander or vasoconstrictor, as it can reduce PICD-related complications, hospital costs, and mortality. 29 When less than 5 L of ascites are removed, the risk of PICD is low and an advantage with HA has not been clearly demonstrated. 29 However, expert opinions favor HA because of concerns about the side effects of alternative plasma expanders, mainly represented by allergic reactions and renal dysfunction. 2
Albumin administration in bacterial infections
Based on a randomized, controlled trial the infusion of HA (1.5 g/kg at diagnosis and 1 g/kg on day 3) is recommended in patients with SBP, as the combination of HA and cefotaxime reduced the incidence of renal dysfunction and mortality (from 29% to 10%) compared with cefotaxime alone.2,30
Although the efficacy of HA administration is evident in patients at a high risk of developing SBP-induced renal dysfunction (baseline serum bilirubin ≥4 mg/dL or SCr ≥1 mg/dL), whether HA is needed in patients not meeting these criteria is still unclear. 30 A non-randomized study confirmed that HA administration improves high-risk patient survival, but suggested HA is unnecessary in low-risk patients (urea < 66 mg/dL and bilirubin < 4 mg/dL). 31 Thus, further investigation on this matter is warranted.
In bacterial infections other than SBP, available randomized trials showed some beneficial effect of HA infusion (improvement of renal and circulatory functions, ACLF resolution) but provided conflicting results on survival.32–34 Thus, routinely HA use is currently not recommended in this context. 2 Furthermore, attention is needed in patients at risk of volume overload (heart failure, pulmonary hypertension, severe pneumonia) to avoid pulmonary edema. 33
Albumin in the management of AKI and hepatorenal syndrome
Patients diagnosed with AKI, along with general measures (removal/correction of risk factors including diuretics, nephrotoxic drugs, bleedings, and infections), should undergo volume expansion. 9 In AKI stage 1 A this can be performed according to cause and severity of fluid loss (e.g. HA, crystalloids, or red blood cells). 2
In AKI stage ≥1B, expert opinion indicates that HA should be preferred to crystalloids and administered at the dose of 1 g/kg of body weight (up to 100 g) for 2 consecutive days. In this context, HA is able to resolve pre-renal AKI or allow the differentiation of types of AKI.2,9
Once HRS-AKI is diagnosed, HA administration should be started in addition to terlipressin, and continued until total or partial response or for a maximum of 2 weeks. Although the optimal HA dose is not fully established, the recommended dose is 20–40 g/day. 35 Central venous pressure monitoring can help to optimize HA dose and prevent circulatory overload. 2
Long-term albumin treatment in decompensated cirrhosis
Recently, evidence has shown that long-term albumin administration in patients with decompensated cirrhosis reduces 18-month mortality and the incidence of complications and hospitalizations, eases the management of ascites, is cost effective and has a good safety profile.36,37 Therefore, it could be included in the treatment options for patients with cirrhosis and ascites.
Namely, the ANSWER study (a multicenter, randomized, open-label, pragmatic study on 431 patients with uncomplicated ascites) showed that long-term HA administration (40 g twice weekly for the initial 2 weeks then 40 g per week) reduced the mortality hazard ratio by 38%. 36 Moreover, multivariable Cox regression analysis estimated that seven patients had to be treated to avoid a death and Cox proportional hazard model showed HA was the sole protective factor against all-cause mortality. HA was also able to reduce the need of paracentesis as well as the incidence of refractory ascites and other complications of cirrhosis by 30–67.5%. Finally, besides a lower number of hospitalizations, patients receiving HA spent about half the number of days in hospital per year compared to those who underwent standard medical treatment. 36
Similar results were reported by a subsequent non-randomized study including 70 patients with refractory ascites and comparing the effects of HA administration (20 g twice weekly) versus standard medical treatment. 37
However, variant results were provided by a placebo-controlled study (Midodrine-albumin in cirrhotic patients awaiting liver transplantation) that enrolled 173 patients with ascites. 38 Treatment with the combination of HA plus the α1-receptor agonist midodrine failed to demonstrate any benefit on the incidence of complications or survival. However, this study was affected by important limitations, particularly the low HA dosage (40 g/15 days) and the brief median duration of treatment due to a high transplant rate. 38
What needs to be defined
The role, if any, of HA administration in some acute complications of cirrhosis still requires investigation. Besides non-SBP bacterial infections, discussed above, HE represents a most interesting topic. Variant results are currently available: some studies reported beneficial effects on the resolution of overt HE,39,40 whereas others showed no effect, but an improvement in survival. 41 Evidence for a preventing effect of long-term HA administration seems to be stronger. A reduced incidence of severe HE was reported in the ANSWER study and a non-randomized study in patients with refractory ascites.36,37 Furthermore, a recent investigation based on retrospective and meta-analysis data suggested that HA infusion might prevent overt HE and improve its severity. 42
Although promising, the role of HA in treating ACLF is not yet established, but ongoing clinical trials will likely provide relevant information on this matter.
Differences in the trial designs, severity of cirrhosis, HA dosage, and the schedule of administration likely explain the variant outcomes of the two randomized studies assessing the effects of long-term HA administration in decompensated cirrhosis.
The Pilot-PRECIOSA study highlighted the crucial importance of the amount of HA administered. 24 This open-label, non-randomized study aimed at defining the optimal HA dosage and schedule for designing a subsequent controlled trial evaluating the validity of 1-year HA treatment in decompensated cirrhosis (PRECIOSA study, ClinicalTrials.gov: NCT03451292). In this pilot-study, a 12-week treatment with high-dose HA (1.5 g/kg/week), but not with low-dose (1 g/kg/2 weeks), normalized serum albumin concentration (SA), ameliorated cardiocirculatory function, and reduced the serum concentrations of pro-inflammatory cytokines. 24
The importance of increasing SA with HA administration also emerged from a post-hoc analysis of the ANSWER trial. Namely, on-treatment SA at 1 month was closely associated with survival, which exceeded 90% when SA of 4.0 g/dL was reached. 43
Considering the repercussions that long-term HA administration may have on clinical practice, the clarification of some aspects is still needed to optimize this therapy, such as the optimal dose and schedule, the definition of the patient populations that would most benefit from it, the role of SA during treatment, and the possibility of stopping HA administration. 44
Footnotes
Ethics Approval
For the studies/experiments with human or animal subjects mentioned in this review, please refer to the original articles.
Informed Consent
For informed consent required for human studies mentioned in this review, please refer to the original articles.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Declaration of Conflicting Interests
MT is part of the speakers‘ bureau for Grifols SA and Octapharma AG. GZ is part of the speakers‘ bureau for Octapharma. OR is part of speakers‘ bureau for Baxalta. PC is part of the speakers‘ bureau for Grifols SA, Octapharma AG, Baxalta, and Kedrion Biopharma, is consultant for Kedrion Biopharma, is on the advisory board for Grifols SA, and has a research grant from Octapharma AG. MB is a consultant and speaker for Baxalta / Shire, CLS Behring GmbH, and Grifols SA, a consultant for Martin Pharmaceuticals; and a speaker for Octapharma AG, Takeda and PPTA.