
Abstract
Background
Spontaneous bacterial peritonitis (SBP) is defined as an ascitic polymorphonuclear cell count (A-PMN) > 250 cells/µl.
Objective
We aimed to investigate the prognostic value of ascitic fluid cell counts in patients without SBP.
Patients and methods
A total of 178 patients were included and stratified by ascitic cell counts at index paracentesis: A-LEUK-low (<250/µl), A-LEUK-intermediate (250–500/µl) and A-LEUK-SBP (>500/µl) for leukocytes; A-PMN-low (<125/µl), A-PMN-intermediate (125–250/µl) and A-PMN-SBP (>250/µl) for PMN cells.
Results
One-year mortality was comparable between group A-LEUK-SBP (53.9%) and patients with subclinical cell counts (34.5% for A-LEUK-low, 43.5% for A-LEUK-intermediate, log-rank p = 0.547). However, we observed an increase in one-year mortality already in group A-PMN-intermediate with 75% and A-PMN-SBP with 80.9% (vs 40.5% for A-PMN-low, log-rank p = 0.016).
Importantly, increases of A-PMN cell counts between two paracenteses were associated with increased mortality: per 100 cells/µl increase of absolute A-PMN cell count: hazard ratio (HR): 1.03 (95% confidence interval (CI): 1.01–1.06), p = 0.005; per 5% increase of relative PMN cell count: HR: 1.15 (95% CI: 1.06–1.26), p = 0.001.
Conclusion
Patients with PMN cell counts of 125–250/µl are at high risk for mortality, which was very similar to SBP patients with PMN cell counts >250/µl. This highlights the need for preventive strategies. The prognostic value of changes in relative ascitic PMN cell counts should be evaluated in future studies.
Key summary
Summary
Spontaneous bacterial peritonitis (SBP) is the most frequent infection among patients with cirrhosis and ascites. SBP is defined by an ascitic polymorphonuclear (A-PMN) cell count higher than 250/µl in the absence of an intraabdominal source of infection. Development of bacteriascites was associated with an increase of relative A-PMN cell counts. New findings of this study
Increased mortality among patients with an A-PMN cell count between 125 and 250/µl. Increase of the absolute or relative A-PMN cell count between two paracentesis sessions was associated with mortality. The threshold for antimicrobial treatment may need reconsideration.
Introduction
Cirrhosis is the result of chronic or repetitive liver injury and consecutive development of fibrosis and parenchymal dysfunction, and is responsible for approximately 170,000 deaths per year in Europe.1,2 Development of ascites, renal dysfunction and variceal bleeding represent critical events in the natural history of cirrhosis and indicate worse prognosis.3,4 Most of these complications are related to portal hypertension and may subsequently lead to hepatic decompensation and acute-on-chronic liver failure.5–7 In general, bacterial infections are more common in patients with cirrhosis than in the healthy population and increase mortality fourfold.8–10 Spontaneous bacterial peritonitis (SBP) is the most frequent infection among patients with cirrhosis and ascites, and is associated with poor outcome.9,11 Risk factors for SBP include low serum sodium levels, Child-Turcotte-Pugh (CTP) stage C and elevated ascites polymorphic nuclear (A-PMN) cell counts (≥100 cells/µl). 12 According to international consensus, SBP is defined by an ascitic polymorphonuclear (A-PMN) cell count higher than 250/µl in the absence of an intraabdominal source of infection or any other explanation for an elevated A-PMN count.13–15 However, in some centers, ascitic fluid leukocyte counts >500/µl rather than A-PMN cell counts are used to establish the diagnosis of SBP and initiate empiric antibiotic treatment. Traditionally, A-PMN cell counts were assessed by manual counting of cells and were considered the gold standard for the assessment of A-PMN counts. 13 However, newly emerging automated assessments of A-PMN counts showed promising results in regard to accuracy and time efficiency.16,17 In contrast, bacterial cultures are of limited value for diagnosing SBP, since its results are not readily available and the detection rate ranges only between 33% and 73%. 18 Interestingly, a recent study showed that relative A-PMN counts (i.e. percentage of overall leukocytes) increased when patients developed bacteriascites (BA) (i.e. positive bacterial culture of ascites fluid but an A-PMN cell count < 250/μl). 19
In our study, we aimed to investigate the prognostic value of ascitic fluid leukocyte and A-PMN cell counts for the development of SBP and mortality.
Patients and methods
Study design
A total of 178 patients with cirrhosis and ascites who underwent abdominal paracentesis between 2015 and 2018 were included in this monocentric retrospective analysis of prospectively collected data. Patients with secondary peritonitis and/or malignant diseases were excluded. Patients received standard of care treatment for portal hypertension, including primary 20 and secondary prophylaxis 4 of variceal bleeding.
Total ascitic fluid leukocyte and A-PMN cell counts were assessed at inclusion, along with Model for End-Stage Liver Disease (MELD), CTP score, blood cell counts, and C-reactive protein (CRP) levels. According to national guidelines, ascitic fluid was also inoculated into blood culture bottles at bedside, which is in line with the Austrian consensus recommendations.21,22
Ascitic fluid analysis
Ascites fluid was collected at diagnostic or therapeutic paracentesis and analyzed at the Department of Laboratory Medicine, Medical University of Vienna, which runs a certified (International Organization for Standardization (ISO) 9001:2015) and accredited (ISO 15189:2012) quality management system. Briefly, ascitic fluid cellular components were quantified on Sysmex XE-5000 or XN-2000 hematology analyzers (Sysmex, Kōbe, Japan), which are equipped with a specific body fluid mode that gives total cell counts, leukocyte counts, as well as the shares of PMN and mononuclear (MN) cells. For samples with leukocyte counts >100 cells/µl, additional microscopic 100-cell differential counts were performed by biomedical technicians and/or laboratory physicians from cytospin-preparations stained according to a modified Wright protocol (Hema-Tek, Siemens Healthineers, Erlangen, Germany).
Subgroup analyses
Patients were divided into three subgroups in regard to ascitic fluid cell counts at index paracentesis: a group A-LEUK-low with < 250 cells/µl, A-LEUK-intermediate with 250–500 cells/µl and A-LEUK-SBP with > 500 cells/µl for ascitic fluid leukocytes (A-LEUK); and group A-PMN-low with < 125 cells/µl, A-PMN-intermediate with 125–250 cells/µl and A-PMN-SBP with > 250 cells/µl for A-PMN cells.
Statistical tests
Statistical analyses were performed with IBM SPSS Statistics 25 (IBM, Armonk, NY, USA) and GraphPad Prism 7 (GraphPad Software, La Jolla, CA, USA). Continuous variables are displayed as mean ± SD, or in case of nonparametric distribution, as median with low and high quartiles. Categorical variables are presented as number and proportion of patients. Group comparisons of continuous variables were performed with one-way analysis of variance, when applicable. Alternatively, Kruskal-Wallis test was used. Mann-Whitney U test with Shaffer procedure for multiple comparisons was chosen for post hoc analysis. Categorical variables were compared with chi-squared or Fisher exact test when applicable. Linear correlation between two variables was calculated using Pearson correlation coefficient.
Transplant-free survival (TFS) is presented by Kaplan-Meier diagrams. Differences between groups were compared using log-rank test. The influence of changes in ascitic fluid relative to PMN cell count between two paracenteses on transplant-free mortality was assessed using Cox regression hazard models. TFS was computed as the time from the day of the first paracentesis within the study (index paracentesis) until the last day of follow-up, death, or liver transplantation. For mortality analyses, death was considered as an event. In case of liver transplantation, patients were censored at the day of surgery, otherwise at the day of the last follow-up. Variables with p < 0.1 at univariate analysis and established prognostic factors were included as covariates for multivariate analysis. To further investigate the impact of prognostic group on mortality, we used a Fine and Gray competing risk regression model (cmprsk: Subdistribution Analysis of Competing Risks; https://CRAN.R-project.org/package=cmprsk). 23 Orthotopic liver transplantation was considered as a competing risk.
A p value ≤ 0.05 was considered statistically significant in all statistical tests.
Ethics
This study was conducted in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments and approved by the local ethics committee of the Medical University of Vienna (No. 1786/2017). Patients consented to the paracentesis performed. The need for a dedicated informed consent for these retrospective analyses was waived by the ethics committee of the Medical University of Vienna, since all procedures and tests were performed in clinical routine and only anonymized data are reported.
Results
Patient characteristics
A total of 178 patients with cirrhosis and ascites were included. According to an A-LEUK count > 500/µl or an A-PMN cell count > 250/µl, 21.3% (38/178) and 17.5% (31/177) had a history of SBP, diagnosed at paracentesis performed prior to study entry. One patient had an A-LEUK count > 500/µl (but no A-PMN cell counts were assessed) during follow-up, which led to immediate initiation of antibiotic treatment; thus, the patient was excluded from follow-up because of missing A-PMN counts (Tables 1 and 2, Figure 1).
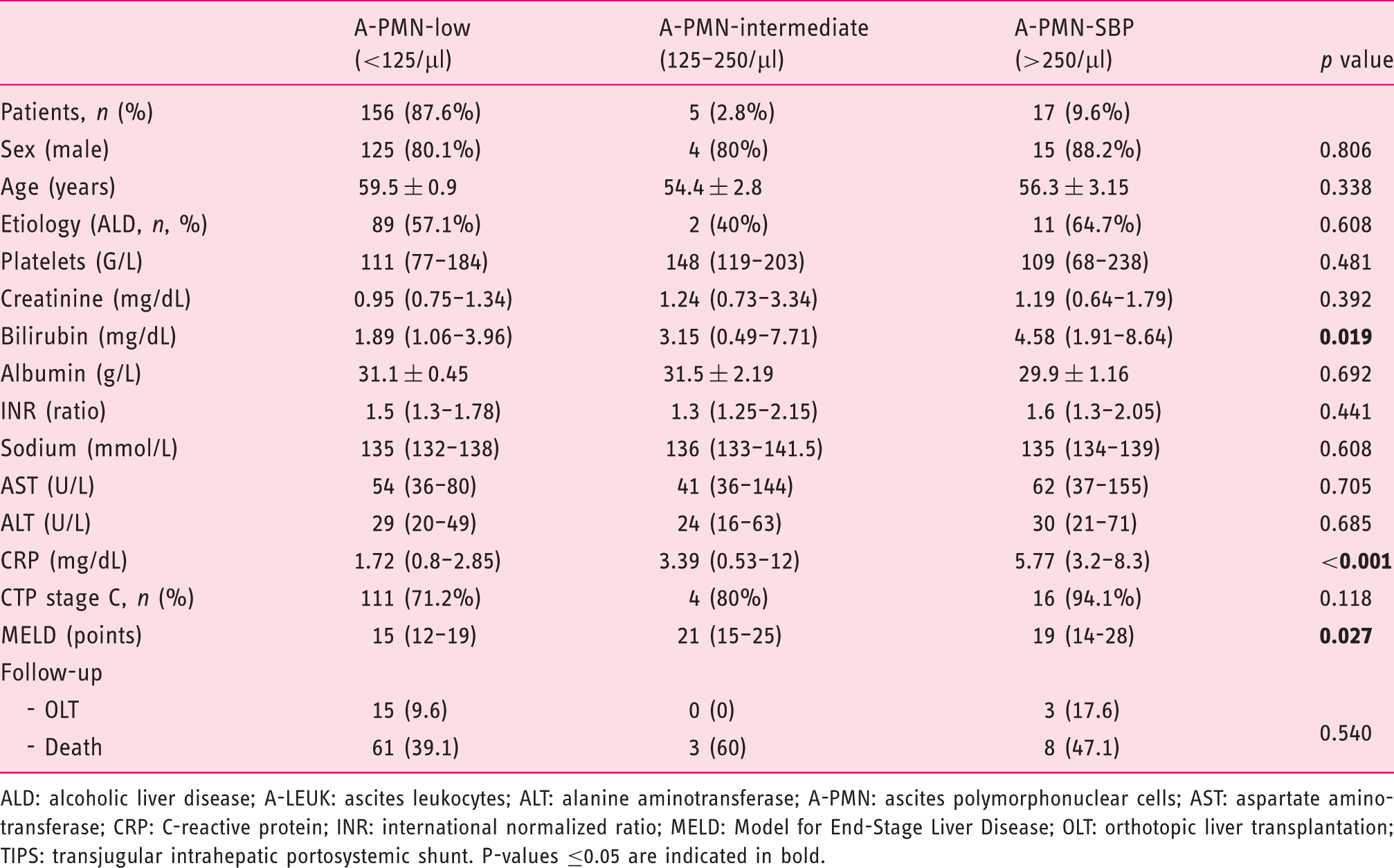
The prognostic value of (a) subclinical ascitic fluid leukocyte and (b) PMN cell counts for subsequent SBP and death. Patient characteristics (overall cohort) and comparison between patients with ascitic fluid leukocytes <250/µl, 250–500/µl and >500/µl. Normally distributed parameters are displayed as mean ± SD, others as median with quartiles. ALD: alcoholic liver disease; A-LEUK: ascites leukocytes; ALT: alanine aminotransferase; A-PMN: ascites polymorphonuclear cells; AST: aspartate aminotransferase; CRP: C-reactive protein; INR: international normalized ratio; MELD: Model for End-Stage Liver Disease; OLT: orthotopic liver transplantation; TIPS: transjugular intrahepatic portosystemic shunt. P-values ≤0.05 are indicated in bold. Patient characteristics (overall cohort) and comparison between patients with ascitic fluid polymorphonuclear cells <125/µl, 125–250/µl and >250/µl. Normally distributed parameters are displayed as mean ± SD, others as median with quartiles. ALD: alcoholic liver disease; A-LEUK: ascites leukocytes; ALT: alanine aminotransferase; A-PMN: ascites polymorphonuclear cells; AST: aspartate aminotransferase; CRP: C-reactive protein; INR: international normalized ratio; MELD: Model for End-Stage Liver Disease; OLT: orthotopic liver transplantation; TIPS: transjugular intrahepatic portosystemic shunt. P-values ≤0.05 are indicated in bold.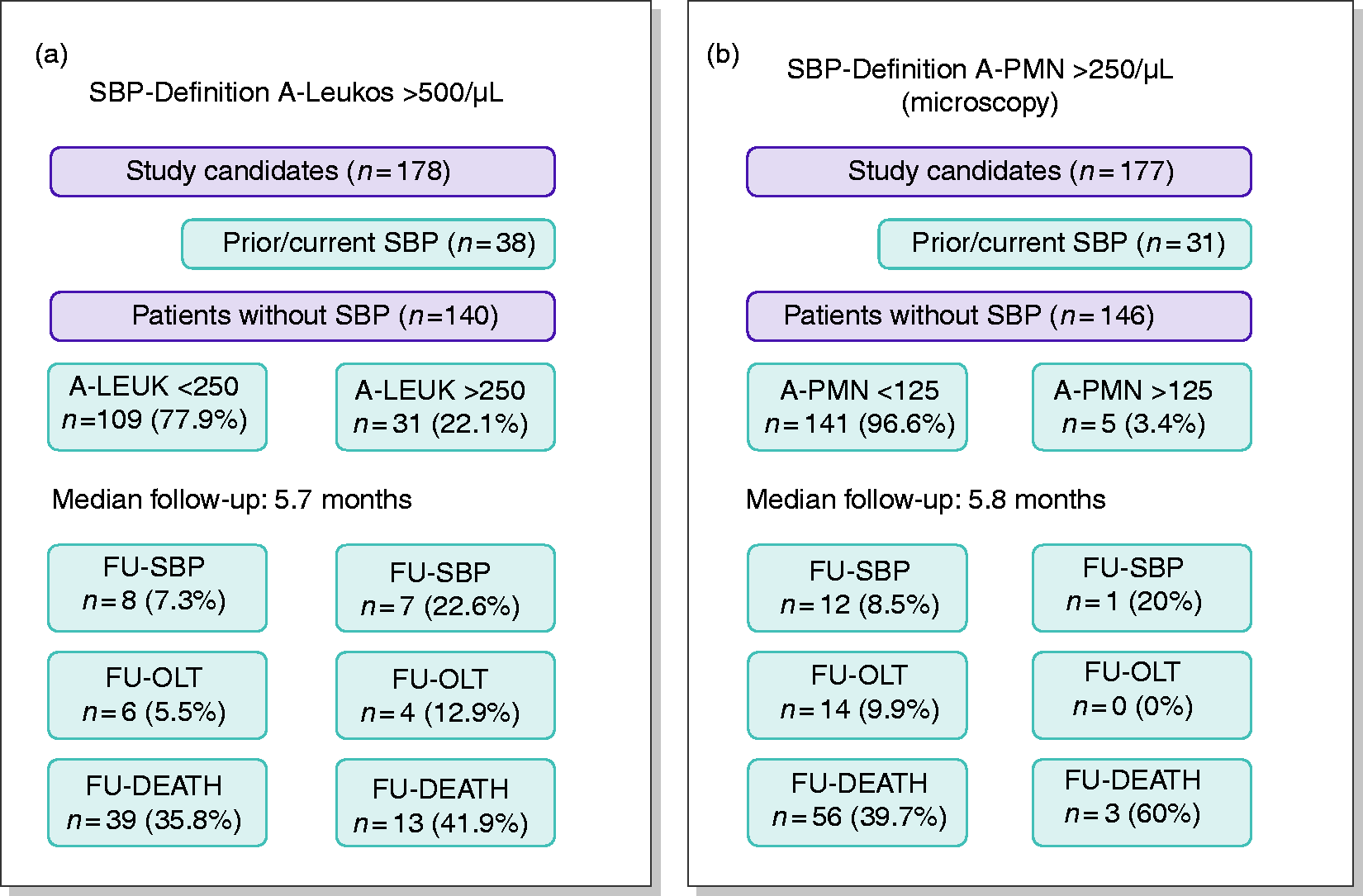
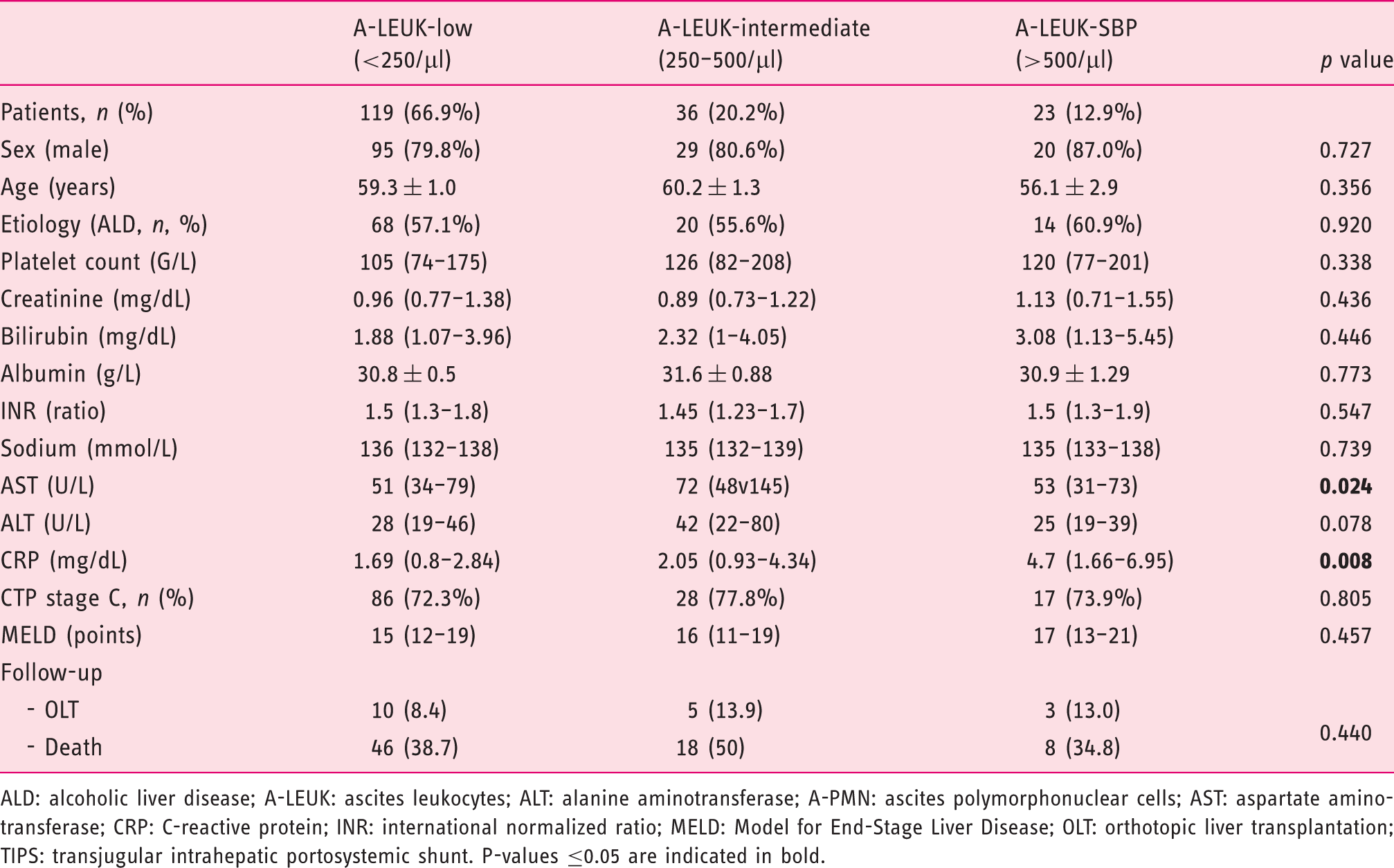
Comparison of patient characteristics at baseline in regard to A-LEUK groups (group A-LEUK-low with 119 (66.9%), A-LEUK-intermediate with 36 (20.2%) and A-LEUK-SBP with 23 (12.9%) patients, respectively) showed comparable characteristics except for a significant difference in median AST (median 51 (34–79), 72 (48–145) and 53 (31–73) U/l, respectively; p = 0.024; low vs intermediate: p = 0.021, low vs SBP: p = 0.788, intermediate vs SBP: p = 0.038) and median CRP levels (1.69 (0.8–2.84), 2.05 (0.93–4.34) and 4.7 (1.66–6.95) mg/dl, respectively; p = 0.008; low vs intermediate: p = 0.145, low vs. SBP: p = 0.009, intermediate vs SBP: p = 0.04).
When comparing the A-PMN count strata, serum CRP (p < 0.001; low vs intermediate: p = 1.000, low vs SBP: p < 0.001, intermediate vs SBP: p = 0.295) and bilirubin levels (p = 0.019; low vs intermediate: p = 1.000, low vs SBP: p = 0.015, intermediate vs SBP: p = 0.471) were elevated in SBP patients. MELD score was significantly different among A-PMN groups (p = 0.027; low vs intermediate: p = 0.122, low vs SBP: p = 0.068, intermediate vs SBP: p = 1.000). Furthermore, A-PMN cell counts at index paracentesis showed a statistically significant correlation of moderate strength with serum CRP levels (Pearson r = 0.446, 95% confidence interval (CI) 0.319–0.557; p < 0.001; Supplementary Figure 1).
Ascitic fluid cultures were positive in only eight (4.5%) patients, including four patients with SBP and four patients with BA (A-PMN count < 250/µl). Streptococcus and Staphylococcus species were isolated from patients with BA, and E coli, Staphylococcus, and Klebsiella species were isolated from patients with culture-positive SBP, respectively.
Ascitic fluid cell counts across MELD strata and CTP stages
Ascitic cell counts were divided into subgroups according to MELD score (<16, 16–22, > 22) and CTP stages (B and C). Ascitic fluid cell counts, i.e. A-LEUK counts and A-PMN cell counts, were similar between CTP stage B vs C (A-LEUK: p = 0.509; A-PMN: p = 0.382). When considering MELD strata <16 vs 16–22 vs > 22, patients with MELD score between 16 and 22 had significantly higher A-PMN counts at index paracentesis as compared with patients with MELD score below 16; however, this was not found for A-LEUK levels (A-LEUK: p = 0.322; A-PMN: p = 0.019, post hoc < 16 vs 16–22 p = 0.036) (Figure 2).
Ascitic fluid leukocyte and PMN cell counts at inclusion in regard to Child-Turcotte-Pugh and MELD score.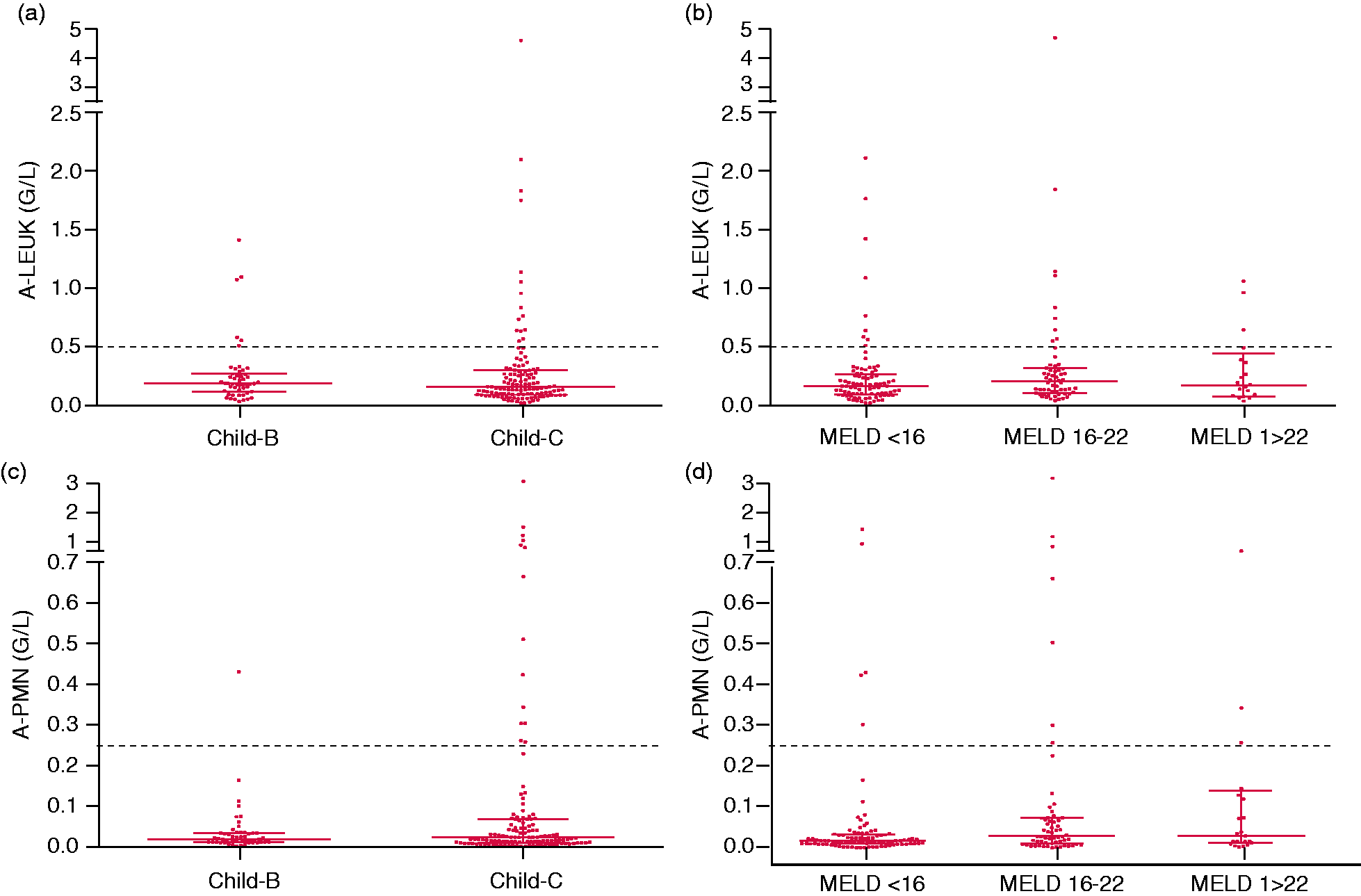
The rather similar distribution of ascitic fluid cell counts underlines that SBP may occur across all MELD strata and CTP stages. This is further supported by plotting the cell count results of all paracenteses (including multiple paracenteses of the included study participants, Supplementary Figure 2).
Subclinical ascitic fluid leukocyte counts
After excluding patients with SBP prior to or at index paracentesis, 109 (77.9%) patients had an A-LEUK cell count < 250/µl, and 31 (22.1%) patients 250-500/µl. In summary, patients in group A-LEUK-low developed SBP less often during follow-up (7.3% vs 22.6%), required less often liver transplantation (OLT: 5.5% vs 12.9%) and showed lower mortality (35.8% vs 41.9%) during follow-up than patients in group A-LEUK-intermediate.
Subclinical ascitic fluid PMN cell counts
If SBP was defined only by an A-PMN count of > 250/µl, 146 patients (82.5%) had no history of SBP at study inclusion. Of these, 141 (96.6%) patients had an A-PMN count < 125/µl and five (3.4%) patients between 125 and 250/µl.
Twelve of 141 (8.5%) in group A-PMN-low and one of five (20%) patients in group A-PMN-intermediate developed SBP during follow-up. Fifty-six (39.7%) and three (60%) patients in groups A-PMN-low and A-PMN-intermediate died during the follow-up period, respectively.
Subclinical ascitic fluid cell counts and risk for subsequent SBP
We observed a significantly increased incidence of SBP during the follow-up period (27.3% in group A-LEUK-intermediate vs 8.7% in group A-PMN-low; log-rank p = 0.019) in patients with intermediate—but subclinical—A-LEUK counts. Similarly, patients in group A-PMN-intermediate showed a nonsignificantly higher risk of subsequent SBP development, as compared with patients with low A-PMN counts (33.3% in group A-PMN-intermediate vs 9.8% in group A-PMN-low, p = 0.174) (Figure 3).
Time-to-SBP according to ascitic fluid (a) leukocyte and (b) PMN cell counts at inclusion.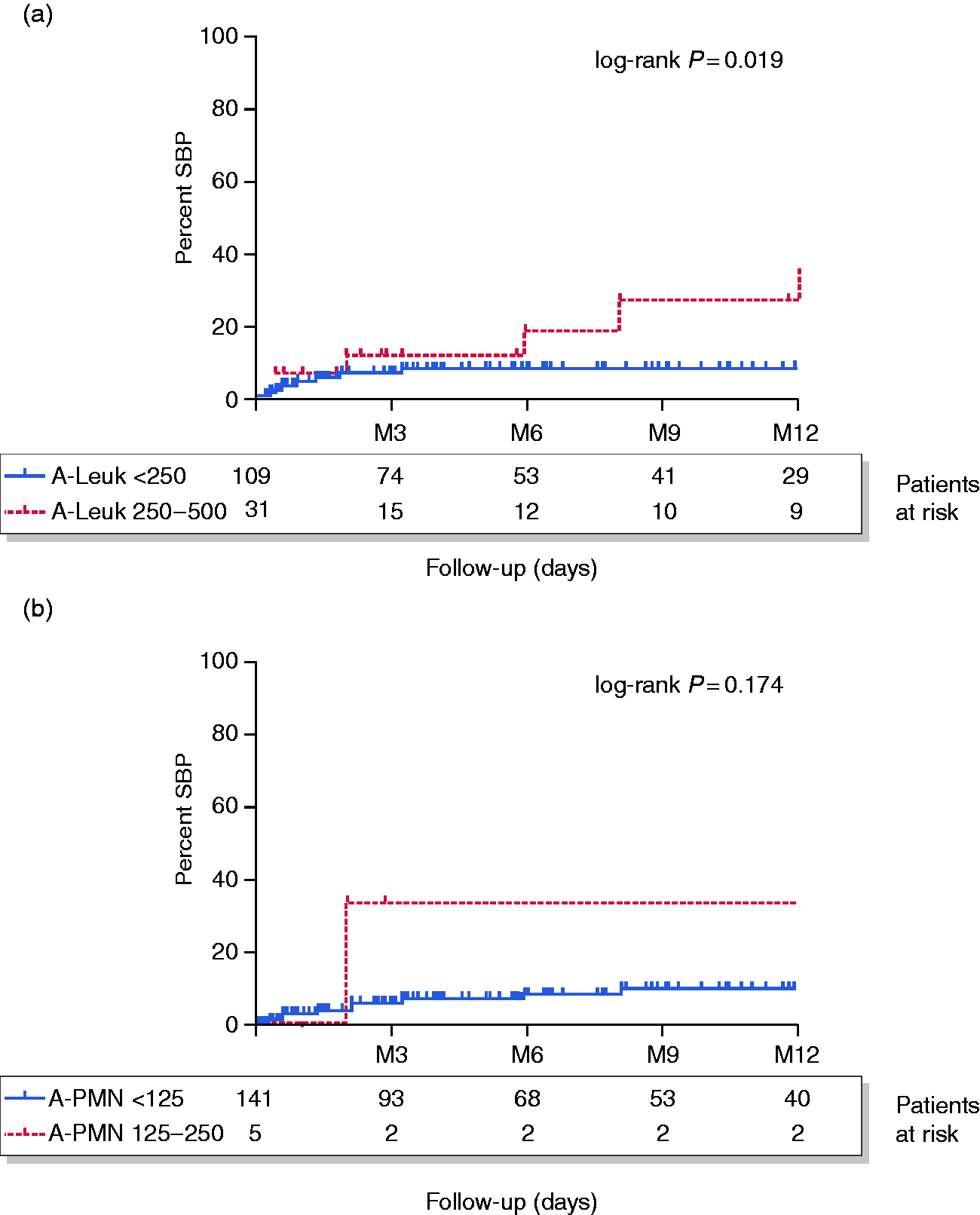
Survival according to ascitic fluid leukocyte count strata
Additionally, one-year transplant-free mortality was assessed in regard to A-LEUK counts. Here we considered A-LEUK counts > 500/µl as the definition of SBP. However, one-year mortality of patients in group A-LEUK-SBP was not significantly different in this analysis as compared with patients with subclinical cell counts (53.9% for A-LEUK-SBP vs 34.5% for A-LEUK-low and 43.5% for A-LEUK-intermediate, p = 0.547) (Figure 4(a)).
Kaplan-Meier survival analysis of patients in regard to ascitic fluid (a) leukocyte and (b) PMN cell counts.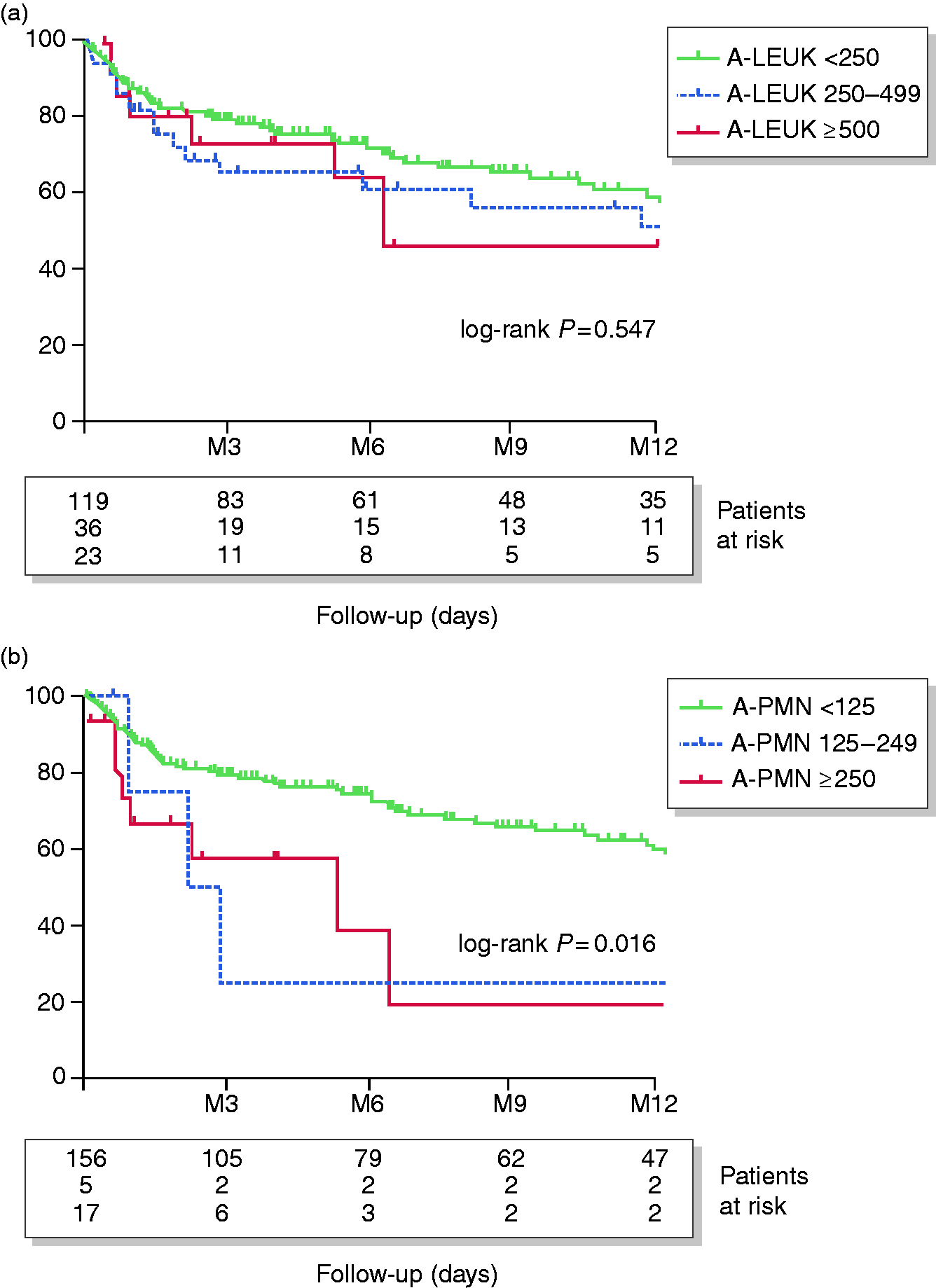
Survival according to ascitic fluid PMN cell count strata
There was a trend toward higher mortality among patients with elevated subclinical A-PMN values; however, this finding did not achieve statistical significance (40.5% in group A-PMN-low vs 75% in group A-PMN-intermediate, p = 0.123). In contrast, one-year mortality was significantly higher in patients with subclinical A-PMN cell counts > 125/µL (80.9% in group A-PMN-SBP vs 40.5% and 75% in groups A-PMN-low and A-PMN-intermediate, respectively; p = 0.016) (Figure 4(b)).
Interestingly, the median (interquartile range) A-PMN count of patients taking prophylactic antibiotics (28.2% in A-PMN-low, 20% in A-PMN-intermediate, 17.6% in A-PMN-SBP; p = 0.646) was significantly lower in the overall cohort at index paracentesis: 14 (20) cells/µl vs 24 (57) cells/µl; p = 0.016. However, survival analysis did not indicate that antibiotic prophylaxis or rifaximin affected TFS (log-rank p = 0.949).
Predictive value of increase of relative PMN cell counts for transplant-free mortality
Predictive value of ΔA-PMN cell counts for transplant-free mortality.
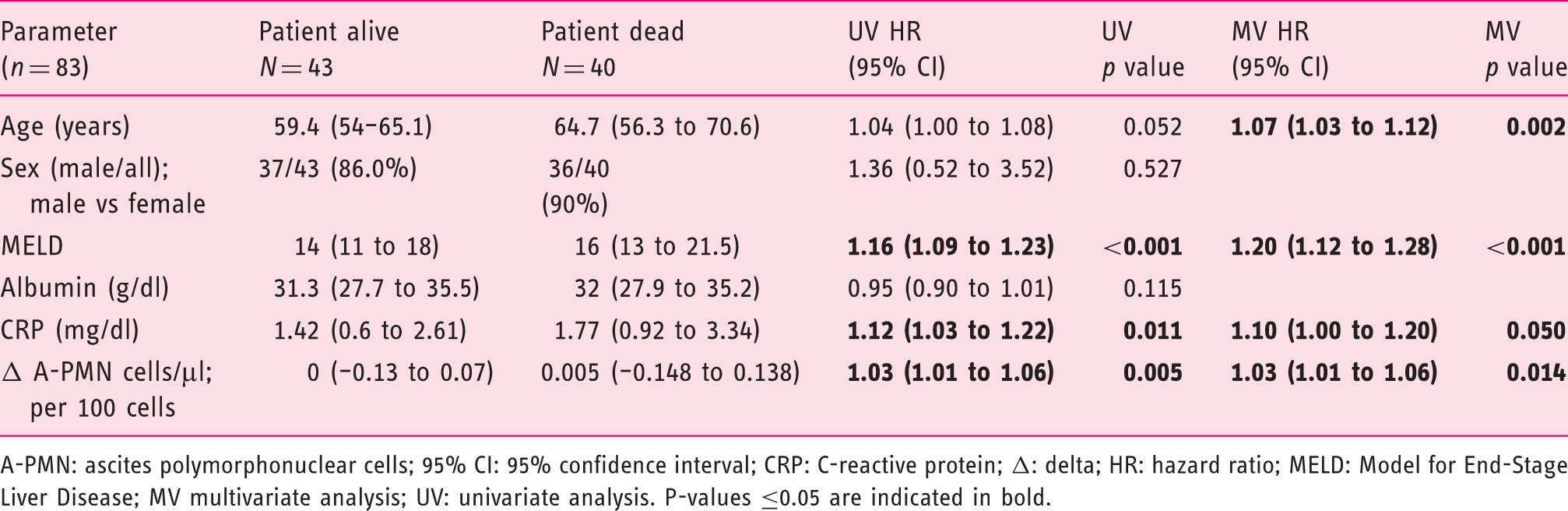
A-PMN: ascites polymorphonuclear cells; 95% CI: 95% confidence interval; CRP: C-reactive protein; Δ: delta; HR: hazard ratio; MELD: Model for End-Stage Liver Disease; MV multivariate analysis; UV: univariate analysis. P-values ≤0.05 are indicated in bold.
Interestingly, an increase in relative A-PMN cell count was associated with univariate analysis (hazard ratio (HR) 1.15 (95% CI 1.06–1.26); p = 0.001), while the increase of absolute A-PMN cells was independently associated with transplant-free mortality (per 100 cells/μl increase: HR: 1.03 (95% CI 1.01–1.06); p = 0.014). The increase of absolute A-PMN cell count remained an independent predictor of mortality in competing risk analysis: HR 1.03 (95% CI 1.02–1.04); p < 0.001 (Supplementary Table 1).
Ultimately, age (per year; HR: 1.07 (95% CI: 1.03–1.12); p = 0.002), MELD (per point; HR: 1.20 (95% CI 1.12–1.28); p < 0.001) and CRP (per mg/dl; HR: 1.10 (95% CI 1.00–1.20); p = 0.050) emerged as independent predictors of transplant-free mortality.
Discussion
In this study, we investigated the prognostic value of subclinical ascitic fluid cell counts for SBP development and mortality. According to current guidelines, an ascitic fluid PMN count >250 cells/µl defines SBP.22,24 However, these cut-off values were empirically determined years ago by international consensus.13,14 Considering the detrimental impact of SBP on the clinical course of patients with decompensated cirrhosis,9,11 better and evidence-based models for SBP prediction are needed to guide primary prophylaxis and optimize individual patient management. We confirmed that SBP may occur at any MELD—which is in line with a recent study stating that MELD was not associated with risk of SBP development. 25
It has recently been suggested that automatic assessment of A-PMN cell counts with flow cytometry represents a more reliable technique for the diagnosis of SBP than traditional manual counting. 16 More importantly, standard hematology analyzers capable of performing differential blood counts—which are permanently available at most hospitals—are reliable alternatives to manual counting to assess A-PMN counts.26,27 We deem this relevant because in clinical routine, and especially in nontertiary centers, SBP diagnosis and treatment are often exclusively based on an A-LEUK count > 500 cells/µl. Furthermore, manual counting is often not available outside routine working hours on work days and on weekends. In this study, we formed groups of A-LEUK counts at study inclusion, i.e. < 250/µl, 250–500/µl and >500/μl, and found no differences in survival. In contrast, when comparing groups in regard to subclinical A-PMN cell counts of <125/µl and 125-250/µl, we observed increased mortality already in patients with A-PMN cell counts > 125/µl. As a consequence, it seems warranted to facilitate the assessment of A-PMN cell counts in clinical routine.
Our finding of increased mortality among patients with an A-PMN cell count of 125–250/µl (in contrast to patients with A-PMN cell counts < 125/µl) may imply that the threshold for antimicrobial treatment should be reconsidered and “early” antimicrobial treatment should be evaluated in clinical trials. This is also supported by the finding that one-year survival of patients with SBP defined by an A-PMN count > 250 cells/µl was similar to patients with A-PMN cell counts of 125–250/µl.
However, multiple results of this study indicate that patients with A-PMN counts between 125 and 250 cells/µl have an increased risk of SBP and mortality. Some of these trends for a worse outcome did not attain statistical significance, most likely because of the small sample size of this particular subgroup. Thus, further prospective studies are needed including a larger number of patients to assess the prognostic value of “subclinical” PMN cell counts of 125–250/μl in ascitic fluid of patients.
A previous study showed that primary prophylaxis of SBP among patients with particular risk factors effectively reduces SBP incidence, development of hepatorenal syndrome and mortality. 28 Further studies on primary prophylaxis also displayed reduced risk of SBP development,29–31 although TFS was not consistently improved. 31 Interestingly, we found a significantly lower A-PMN count at index paracentesis in patients taking prophylactic antibiotics, which may indicate an effective reduction of bacterial translocation.
However, the use of antibiotic prophylaxis should be critically discussed in regard to the emergence of multiresistant bacteria but may provide important benefits in selected risk groups. 32 For example, in contrast to current guidelines, it was recently found that low ascitic fluid protein level is not suited to predict SBP. 33 However, the consideration of pathophysiology-oriented biomarkers may represent a promising approach; for example, it was demonstrated that von Willebrand factor antigen correlates with bacterial translocation and bacterial infections, including SBP. 34
Furthermore, a recent study by Lutz et al. 19 suggested that the relative A-PMN count has a predictive role for SBP development, possibly as a marker of subclinical infection/inflammation as a consequence of bacterial translocation into the ascitic fluid. In addition, an absolute PMN count ≥100 cells/µl has previously been associated with a significantly increased risk for SBP development. 12 Moreover, it was recently shown that the absolute A-PMN cell count may also serve as a predictor for progression of BA to SBP. 35 In addition, Oey and colleagues made the observation that patients with BA had comparable hepatic dysfunction and similarly poor prognosis as patients with SBP. 36 These findings support that BA should be treated similarly to SBP, and indicate the need for a paradigm shift toward more individualized treatment strategies in case of bacterial translocation into ascitic fluid.
Our results indicate that a longitudinal increase in absolute and relative A-PMN cell count is associated with mortality; however, only absolute A-PMN cell counts, age, MELD and CRP remained as independent predictors of mortality on multivariate analysis. Important limitations of our study include the retrospective design, lack of an external validation cohort and the limited number of patients in some subgroup analyses.
In summary, A-PMN cell counts hold considerable information on the risk of SBP development and mortality in patients with cirrhosis. If a worse prognosis of patients with “subclinical” A-PMN counts of 125–250/µL is confirmed by further studies, the use of similar treatments as for SBP should be investigated in this subgroup. Moreover, increased A-PMN counts may also be applied within clinical studies to identify patients who might benefit from antibiotic prophylaxis, since some currently used markers for risk stratification (i.e. ascitic fluid protein concentration28,37 are suboptimal. 33 The prognostic value of changes in absolute and relative A-PMN cell counts should be evaluated in future studies.
Supplemental Material
Supplemental material for Ascitic fluid polymorphic nuclear cell count impacts on outcome of cirrhotic patients with ascites
Supplemental Material for Ascitic fluid polymorphic nuclear cell count impacts on outcome of cirrhotic patients with ascites by Benedikt Simbrunner, Annika Röthenbacher, Helmuth Haslacher, David Bauer, David Chromy, Theresa Bucsics, Philipp Schwabl, Rafael Paternostro, Bernhard Scheiner, Michael Trauner, Mattias Mandorfer, Ilse Schwarzinger and Thomas Reiberger in United European Gastroenterology Journal
Footnotes
Declaration of conflicting interests
BS, AR, HH, DB, DC, TB, PS, RP and BS have nothing to declare. MT has served as a speaker and/or consultant and/or advisory board member for Albireo, Bristol-Myers Squibb, Dr. Falk Pharma, Gilead, Intercept, MSD, Novartis, and Phenex Pharmaceuticals, and has received research funding from Albireo, Dr. Falk Pharma, Gilead, Intercept, MSD, and Takeda. MM has served as a speaker and/or consultant and/or advisory board member for AbbVie, Bristol-Myers Squibb, Gilead, W.L. Gore & Associates, and Janssen. IS declares no conflict of interest. TR has served as a speaker and/or consultant and/or advisory board member for AbbVie, Bayer, Boehringer Ingelheim, Gilead, W.L. Gore & Associates, and MSD, and has received research funding from AbbVie, Boehringer Ingelheim, Gilead, MSD, Phenex Pharmaceuticals, and Philips.
Ethics approval
This study was conducted in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments and approved by the local ethics committee of the Medical University of Vienna (No. 1786/2017). Patients consented to the paracentesis performed.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Informed consent
The need for a dedicated informed consent for these retrospective analyses was waived by the ethics committee of the Medical University of Vienna, since all procedures and tests were performed in clinical routine and only anonymized data are reported.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.