
Abstract
Acute pancreatitis is a heterogeneous illness. Most patients experience a mild course of disease, but one third will develop local complications and/or organ failure associated with increased morbidity and risk of mortality. Diagnosis of acute pancreatitis is based on typical epigastric pain, elevation of serum lipase or amylase levels, and/or characteristic findings on imaging. Personalised management is needed in patients with acute pancreatitis. Currently, analgesia, Ringer’s lactate solution-based goal-directed fluid resuscitation and early oral refeeding providing enteral nutrition if not tolerated are the cornerstones for early management. Prophylactic antibiotics or endoscopic retrograde cholangiopancreatography in the absence of cholangitis are considered to be futile. Future clinical trials should address optimal fluid resuscitation, the early administration of anti-inflammatory drugs and the exact role of nutritional support in severe acute pancreatitis. Here, we present a patient case and review the diagnosis, treatment and prognosis of acute pancreatitis.
Keywords
Brief clinical case
A 45-year-old male patient presented to the emergency room with acute-onset epigastric pain and vomiting. The patient was an active smoker and consumed up to one unit of alcohol per day. The patient reported no chronic diseases or previous surgical interventions.
How to diagnose acute pancreatitis
According to the revised Atlanta classification (RAC), for the diagnosis of acute pancreatitis (AP), the patient should meet at least two of the following three criteria: 1 typical abdominal pain (acute onset of epigastric pain often radiating to the back), serum lipase or amylase at least three times the upper limit of normal (ULN) and characteristic findings of AP on imaging.
Symptoms
The cardinal symptom of AP is sudden-onset acute epigastric abdominal pain, often radiating to the back. Nausea and vomiting are very frequent.
Blood and urine tests
Serum amylase and/or lipase have been used to diagnose AP for more than seven decades. 2 The two major sources of serum amylase are the pancreas and the salivary glands; the specific isoforms of pancreatic amylase can be measured in the blood, and some laboratories only determine those isoforms to rule out the influence of salivary amylase. Its serum activity starts to rise within six hours after the onset of AP, peaks at 48 hours and normalises in five to seven days. 3 Lipase comes almost exclusively from the pancreas and so it is considered to be more specific for AP. 3 It rises after four to eight hours, peaks at 24 hours and remains at high levels longer than amylase (8–14 days). 3
Regarding urine markers, we can measure urinary amylase or perform the quick trypsinogen-2 dipstick test. 3 Both have a good sensitivity and specificity. However, the trysinogen-2 dipstick test has a limited availability. 4 Urine markers can be more useful when there is high diagnostic suspicion of AP and blood amylase or lipase normal levels, for example, in cases of hypertriglyceridaemia. 5 Interestingly, there is no evidence of an analytical test that is more accurate than other tests. 3 Repeated measures of pancreatic enzyme levels in blood or urine are not useful for predicting severity or monitoring the disease course.
Other causes of acute abdominal pain and inflammation are associated with increased amylasaemia or lipasaemia, including acute cholecystitis, cholangitis, perforation, acute mesenteric ischaemia or gynaecological problems. Inflammatory diarrhoea and diabetic ketoacidosis are other causes of acute increases of pancreatic enzymes in the blood and urine. These alternative diagnoses are usually associated with atypical signs or symptoms. In this scenario, imaging is needed.
Imaging
Imaging is needed for three purposes: (a) early in the course of disease for differential diagnosis in cases of atypical signs or symptoms, (b) to diagnose local complications of AP and (c) to determine the aetiology of AP.
Differential diagnosis
Imaging is not needed to diagnose AP in patients with typical features of AP and elevated amylase or lipase blood levels higher than three times the ULN. 1 In cases of atypical signs or symptoms (e.g. high-grade fever, chills, peritoneal signs, diarrhoea, pain in central or lower quadrants), a contrast-enhanced computed tomography scan (CECT) is particularly useful to confirm AP. However, abdominal ultrasonography has higher sensitivity and specificity for diagnosing acute cholecystitis compared to CECT. 6
Diagnosis of local complications
During admission, CECT and abdominal magnetic resonance imaging (MRI) are used to evaluate the severity of pancreatitis by detecting the presence of local complications. 7 These techniques should not be performed before the first 72 hours, as they may underestimate the severity of AP, 8 and should only be performed when local complications are suspected (predicted severe disease, persistent pain, persistent systemic inflammatory response syndrome (SIRS), inability to resume oral feeding or early satiety, presence of an abdominal mass, etc…).
Determination of aetiology of AP
Aetiology.
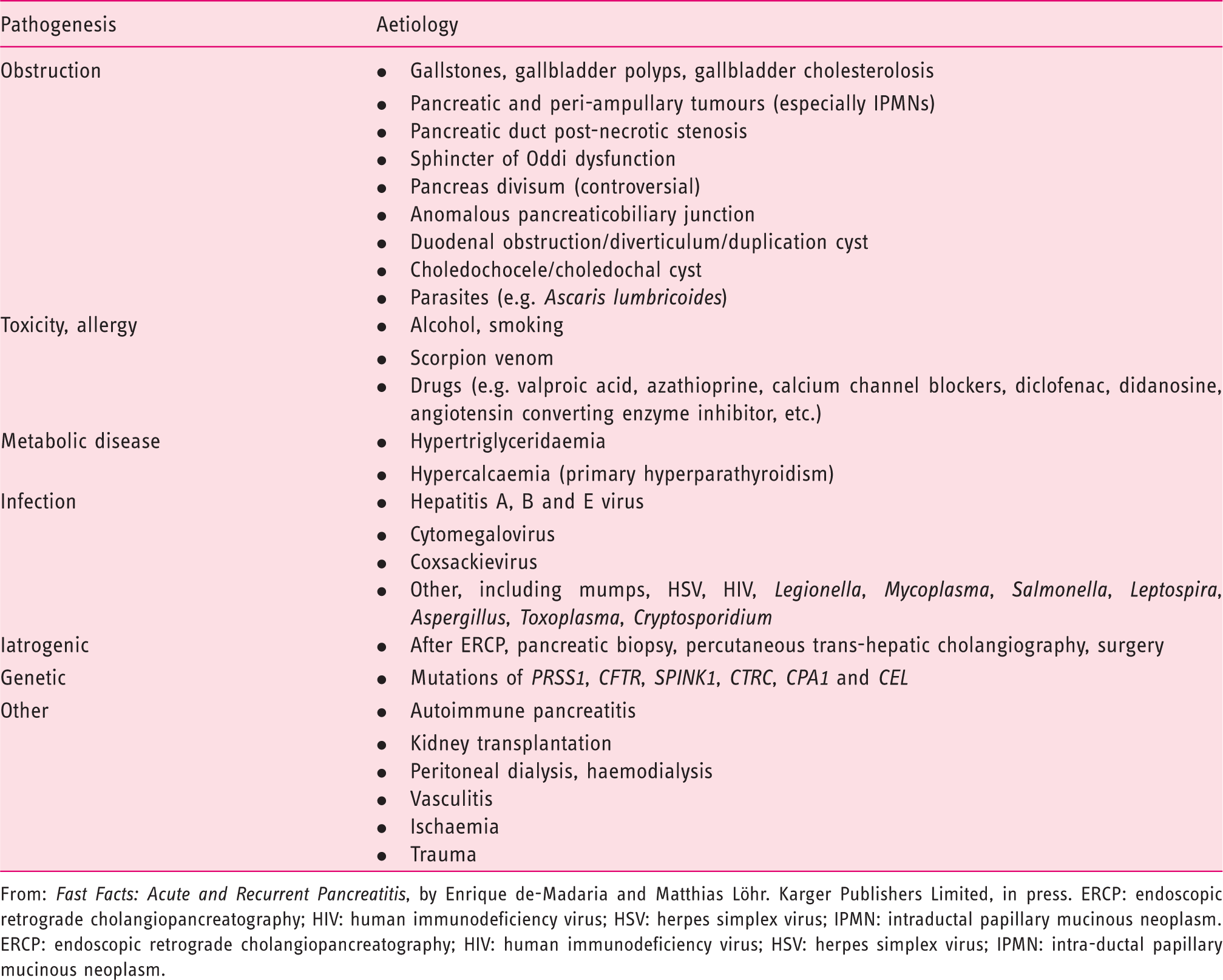
From: Fast Facts: Acute and Recurrent Pancreatitis, by Enrique de-Madaria and Matthias Löhr. Karger Publishers Limited, in press. ERCP: endoscopic retrograde cholangiopancreatography; HIV: human immunodeficiency virus; HSV: herpes simplex virus; IPMN: intraductal papillary mucinous neoplasm.
ERCP: endoscopic retrograde cholangiopancreatography; HIV: human immunodeficiency virus; HSV: herpes simplex virus; IPMN: intra-ductal papillary mucinous neoplasm.
Natural history
About two-thirds of AP patients have a mild course of disease with a quick recovery. However, one third experience disease progression, with the development of local complications and/or organ failure (OF). Two phases are apparent in moderate-to-severe AP: an early phase during the first week and a late phase thereafter. 1 In the early phase, the release of pro-inflammatory agents due to local pancreatic and peri-pancreatic tissue damage may result in the development of SIRS. Uncontrolled inflammation is associated with OF. The development of local complications (collections, necrosis) is linked to fluid sequestration during the early phase but, most importantly, has consequences in the late phase, in which those local complications can be associated with symptoms and infection.
Local complications
There are two types of AP: interstitial and necrotising AP. In interstitial AP, the pancreas is enlarged due to inflammatory oedema. Some patients with interstitial AP may develop acute peri-pancreatic fluid collections (APFC), which are early (<4 weeks) homogeneous collections (without necrotic debris) with no defined wall. Most APFC are reabsorbed; those persisting more than four weeks develop a defined wall and are called pseudocysts. 1
Necrotising AP is characterised by the presence of pancreatic or/and peri-pancreatic necrosis. In the first four weeks, these collections lack a defined wall and are called acute necrotic collections (ANC). ANC are heterogeneous due to the presence of fluid and necrotic debris inside. ANC persisting for more than four weeks develop a defined wall and are known then as walled-off necrosis. 1
All local complications increase morbidity in AP, but only an increase of mortality occurs if persistent OF is present. 9 The infection of pancreatic or peri-pancreatic necrosis is particularly associated with worse outcomes.
OF
OF is defined in AP, according to the RAC, by the modified Marshall scoring system.1,10 OF is present if the patient has two or more points in the modified Marshall score, namely: respiratory (PaO2/FiO2 ≤ 300); renal (serum creatinine ≥1.9 mg/dL) and/or cardiovascular (systolic blood pressure < 90 mmHg not responsive to fluid resuscitation).
OF can be transient (up to 48 hours) or persistent (lasting for more than 48 hours) and single or multiple (if more than one system is affected). Any OF increases morbidity and mortality, but the risk of mortality is greatly increased in persistent OF and/or multiple OF (approximately 50% mortality in both types of OF according to prospective data). 9
Classification of severity
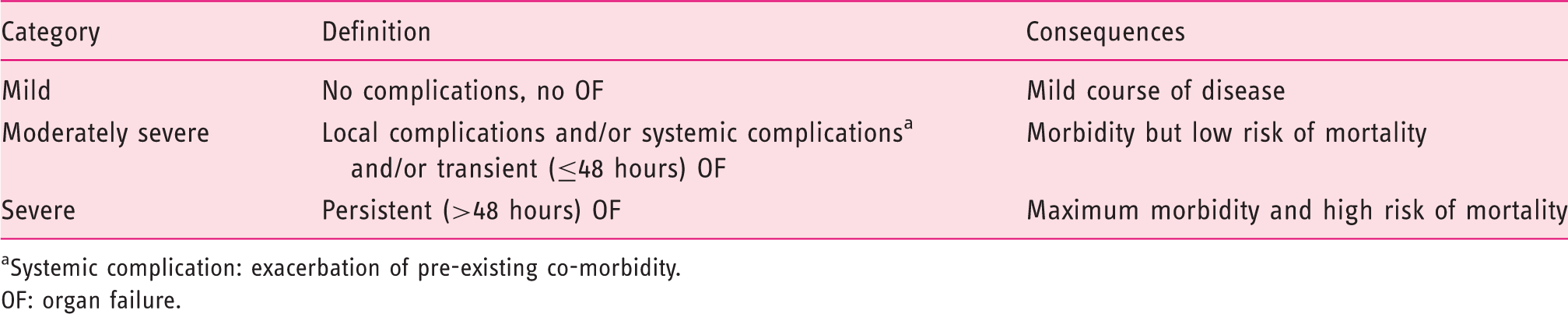
Systemic complication: exacerbation of pre-existing co-morbidity.
OF: organ failure.
Current early management of AP
The cornerstones of the early management of AP are shown in Figure 1.
Early management of acute pancreatitis.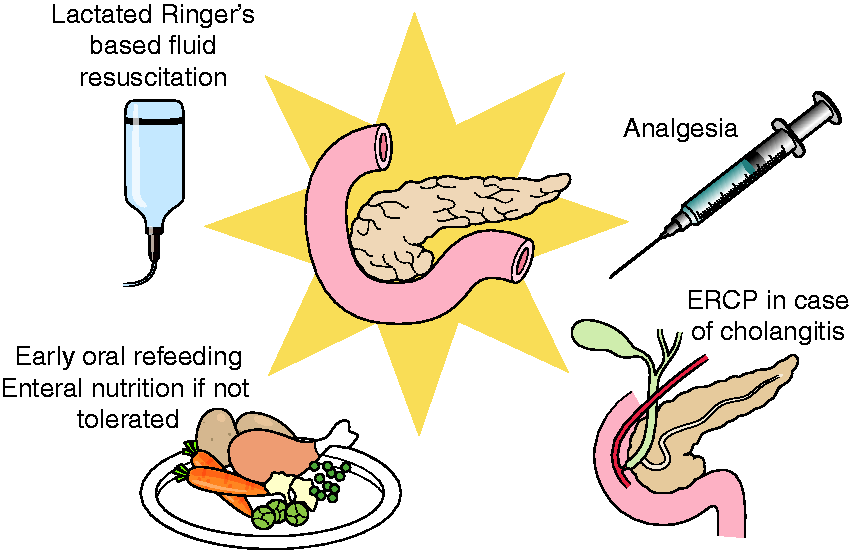
Fluid resuscitation
Hypovolaemia is frequent in AP for several reasons. First, AP is associated with increased vascular permeability with extravasation of fluids into tissues (vascular leak syndrome), which together with local complications and paralytic ileus produces fluid sequestration. In addition, there is an increase in fluid loss due to vomiting, sweating (due to increased body temperature), tachypnoea associated with SIRS, and decreased oral intake of liquids. Severe hypovolaemia may result in decreased organ perfusion that can be countered with adequate fluid resuscitation. However, aggressive fluid resuscitation in patients without hypovolaemia may result in pulmonary oedema and increased intra-abdominal pressure, resulting in abdominal compartment syndrome.
Volume
The optimal volume rate in AP is controversial, and the few available trials have provided conflicting results. In 2009 14 and 2010, 15 two randomised clinical trials (RCTs) on severe AP from the same group showed that patients assigned to aggressive fluid therapy presented worse outcomes (higher morbidity and mortality). These were open-label single-centre trials with some flaws. A recent RCT focused on patients with predicted mild AP compared to aggressive versus moderate fluid resuscitation based on Ringer’s lactate (RL) solution. 16 The primary outcome was ‘clinical improvement within 36 hours’ that required a decrease in haematocrit, blood urea nitrogen and creatinine levels, decreased pain, and tolerance to oral diet. Patients under aggressive fluid resuscitation showed a higher rate of that primary outcome. The definition of ‘clinical improvement’ has been criticised for relying too much on haemodilution, which is not a direct marker of a good disease course, and it is clear that patients receiving aggressive fluid resuscitation will have quicker haemodilution. 17 Well-designed RCTs are needed. Thus, the evidence of recommendations in the guidelines is weak. International Association of Pancreatology/American Pancreatic Association (IPA/APA) 8 and recent American Gastroenterological Association guidelines 18 recommend goal-directed therapy for fluid resuscitation in AP with low-quality evidence.
Type of fluid
RL solution is recommended for fluid resuscitation in AP, since it is associated with decreased inflammation. In an open-label 19 and in a triple-blind RCT 20 with 40 patients each, RL solution decreased the rate of SIRS and C-reactive protein (CRP) blood levels compared to normal saline. Therefore, IAP/APA 8 and American College of Gastroenterology guidelines 21 recommend RL solution as resuscitation fluid in AP. However, SIRS and CRP are surrogate markers of severity, and new RCTs are required that focus on more important clinical outcomes such as OF, local complications or mortality. 18
Oral refeeding and nutritional support
Intra-pancreatic-activated trypsin is a key step in the pathophysiology of AP. Because food stimulates the secretion of trypsinogen, the inactive precursor of trypsin, it was previously believed that ‘pancreatic rest’ improved outcomes (patients were nil by mouth until complete recovery, with or without parenteral feeding). However, several studies have subsequently challenged that belief.
Nutrition in mild AP
RCTs have shown that in mild AP, early oral refeeding is safe and results in a shorter hospital stay.22,23 Furthermore, starting with clear liquids with a step-up progression to solid diet is not necessary, and initiation of refeeding with a fully solid diet is well tolerated and also results in a shorter hospital stay. 22
Nutrition in moderate to severe AP
In a multi-centre RCT, in patients with predicted severe AP, early naso-jejunal feeding within 24 hours did not show better outcomes compared to on-demand enteral nutrition (used only in patients without tolerance to oral diet on day 4). 24 Therefore, in moderate to severe AP, an attempt at oral refeeding can be done, reserving tube feeding if oral diet is not tolerated after three to four days. In patients who cannot tolerate oral feeding, nutritional support with enteral nutrition is clearly superior to total parenteral nutrition (TPN). RCTs and meta-analysis have demonstrated a decrease in infection complications, the need for operative interventions, OF and mortality with enteral nutrition compared to TPN. 25 Hence, in this setting, guidelines for AP strongly recommend enteral nutrition.8,18,21 Regarding the route of enteral feeding, three RCTs and two meta-analyses (although with some methodological flaws) compared naso-jejunal versus nasogastric tube feeding, and showed no differences in mortality, need for surgery or abdominal pain. 26 However, in the presence of gastric outlet obstruction, a naso-jejunal tube is preferred.
Antibiotics
Antibiotic treatment is not recommended in AP unless pancreatic necrosis infection or other infection is present or highly suspected. Early open-label RCTs showed a benefit of prophylactic antibiotics for the prevention of pancreatic necrosis infection. Nevertheless, these studies had methodological flaws. More recent better-designed double-blind RCTs and meta-analysis of RCTs did not demonstrate a reduction in pancreatic necrosis infection or mortality with prophylactic antibiotics. 18 Consequently, the current AP guidelines do not recommend the use of prophylaxis antibiotics in AP.8,18,21
Early endoscopic retrograde cholangiopancreatography
A meta-analysis of RCTs comparing early endoscopic retrograde cholangiopancreatography (ERCP) versus conservative management in AP showed no benefits for early ERCP in the absence of acute cholangitis. 27 The latter is the only widely accepted indication for urgent exploration of the biliary tree. 18
Similar to the case of prophylactic antibiotics, earlier studies suggested the reduction of complications, biliary sepsis and hospital stay with ERCP within 24–72 hours. However, these benefits were not confirmed in later well-designed RCTs. A recent RCT from the Dutch pancreatitis study group addressing this scenario is expected to be published soon. The preliminary analysis published as an abstract in the United European Gastroenterology Journal also suggests that early ERCP is not associated with better outcomes. 28
Analgesia
Although some RCTs have compared different analgesics in AP, most of them only included a few patients and had low methodological quality. 29 Therefore, there is no firm consensus on which drug and which route of administration are preferable in AP. A systematic review concluded that opioids might reduce the need for supplementary analgesics without increasing the adverse effects. 30 Classic non-steroidal anti-inflammatory drugs (NSAIDs) and metamizole can be used to treat AP pain, although their adverse effects (gastrointestinal damage and renal impairment with NSAIDs and neutropenia with metamizole) must be considered. Epidural analgesia may be an alternative in patients with intense pain due to AP.
Final outcome and areas of uncertainty
The patient had SIRS at presentation. Blood tests showed increased blood amylase levels of 3500 IU/L (ULN 100 IU/L) and haematocrit of 51%. The patient needed aggressive fluid resuscitation to maintain an adequate urine output (>0.5 mL/kg/h), but oral feeding was effectively started on day 3. An abdominal ultrasonography showed cholelithiasis. A CT scan was performed on day 4 showing an acute peri-pancreatic fluid collection. A follow-up outpatient ultrasonography showed reabsorption of the collection, and so cholecystectomy was performed on day 30.
While several RCTs have clarified the treatment of late complications,31,32 many questions regarding the early management of AP remain. Future studies should address specific drugs aimed at improving inflammation at an early stage, and identifying the optimal volume and type of fluid resuscitation, role of nutritional support (routes, different composition of nutritional supplements), new ways to prevent pancreatic necrosis infection (selective gut decontamination) and optimal analgesic drugs.
Footnotes
Acknowledgements
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Enrique de-Madaria reports receiving consulting fees from Takeda Pharmaceutical Company Limited, fees for serving on a data and safety monitoring board from Kowa Research Institute, and travel support and lecture fees from Abbott and Mylan.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: G.G.-R. was supported by a grant from the Instituto de Salud Carlos III and the Instituto de Investigación Sanitaria (IIS) Aragón (Río Hortega grant CM17/00145).
Ethics approval
Not applicable.
Informed consent
Not applicable.