
Abstract
Background and objective
Post-endoscopic retrograde cholangiopancreatography (ERCP) pancreatitis (PEP) is the most prevalent complication after ERCP with an incidence of 3.5%. PEP severity is classified according to either the consensus criteria or the revised Atlanta criteria. In this international cohort study we investigated which classification is the strongest predictor of PEP-related mortality.
Methods
We reviewed 13,384 consecutive ERCPs performed between 2012 and 2017 in eight hospitals. We gathered data on all pancreatitis-related adverse events and compared the predictive capabilities of both classifications. Furthermore, we investigated the correlation between the two classifications and identified reasons underlying length of stay.
Results
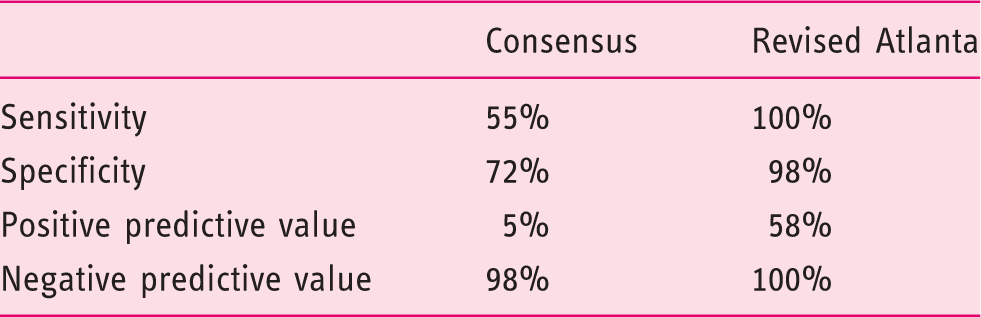
The total sample consisted of 387 patients. The revised Atlanta criteria have a higher sensitivity (100 vs. 55%), specificity (98 vs. 72%) and positive predictive value (58 vs. 5%). There is a significant difference (p < 0.001) between the two classifications. In 124 patients (32%), the length of stay was influenced by concomitant diseases.
Conclusion
The revised Atlanta classification is superior in predicting mortality and better reflects PEP severity. This has important implications for researchers, clinicians and patients. For the diagnosis of PEP pancreatitis, the consensus criteria remain the golden standard. However, the revised Atlanta criteria are preferable for defining PEP severity.
Keywords
Key summary
Established knowledge
Post-ERCP pancreatitis (PEP) is the most prevalent complication of ERCP, with an incidence rate of 3.5%. Adequate assessment of PEP severity is necessary for researchers and clinicians to predict prognosis and compare efficacy of prophylactic measures for PEP. Two classification systems for PEP severity exist: the consensus criteria and the revised Atlanta criteria.
New findings
Our study shows that the diagnostic performance of the revised Atlanta criteria for PEP-related mortality is better than the consensus criteria, because of its focus on necrosis and organ failure. In that way, use of the revised Atlanta criteria allows for a better and more objective evaluation of PEP prophylaxis efficacy. However, the consensus criteria, with its focus on length of hospital stay, could still be useful in light of patient-reported outcome measures and patient-centered care.
Introduction
Post-endoscopic retrograde cholangiopancreatography (ERCP) pancreatitis (PEP) is the most prevalent complication after ERCP with an overall incidence rate of 3.5%. 1 In high-risk patients, particularly those with sphincter of Oddi dysfunction, the PEP rate is 15%. 2 In up to 3% of patients, PEP is fatal. 1
Adequate assessment of PEP severity is important to predict prognosis. It enables researchers and clinicians to compare the efficacy of prophylactic measures that prevent PEP or reduce its severity. Currently, there are two classification systems to assess PEP severity: the consensus criteria and the revised Atlanta criteria.3,4 The consensus criteria stem from an expert meeting in 1991 that defined ERCP-related adverse events and discussed technical considerations as well as management. 3 The consensus criteria are widely used in ERCP guidelines,5,6 landmark trials on PEP prophylaxis7,8 and epidemiological studies,1,2 The revised Atlanta criteria from 2012 are an update of the 1992 Atlanta criteria for defining and treating acute pancreatitis, regardless of etiology. 4 Both classification systems distinguish three categories of disease severity: mild, moderate or severe PEP. The main difference between both criteria is that the consensus criteria use length of hospital stay as a discriminative element, while the revised Atlanta criteria focus on the development of local and systemic adverse events (online Supplementary Table 1).
In acute pancreatitis the development of persistent organ failure is the main driver of mortality. 9 The question is whether length of hospital stay accurately reflects disease severity. Variables associated with length of hospital stay in acute pancreatitis are comorbidity, department, fasting period, diet reintroduction and diagnostics. 10 Furthermore, hospital stay is dependent on culture, practice styles and institutional policies. 11 For instance, in the US the length of hospital stay decreased 0.2% per year between 2003 and 2012. 12 Finally, competing diagnoses may increase the length of stay as well.
We created an international, multicenter, real-life cohort of PEP patients with all parameters to assess local and systemic adverse events of PEP, reasons underlying length of hospital stay and PEP-related mortality. This allowed us to compare both classification systems. Our aims were to determine: 1) which system (consensus or revised Atlanta) is the strongest predictor of PEP-related mortality; 2) the correlation between the consensus and revised Atlanta criteria in defining PEP severity; and 3) the effect of concomitant diseases or other factors on length of stay in PEP.
Materials and methods
In this study we adhered to the Strengthening The Reporting of Observational studies in Epidemiology (STROBE) guidelines. 13 As this study was an anonymous, retrospective evaluation of hospital charts, in which collected data could not be traced back to individual patients, it was not necessary to obtain written informed consent. The study was approved by the Medical Ethics Committee of the Radboud University Medical Center on December 1, 2016 (no. 2016-2974) and follows the declaration of Helsinki.
Study design and setting
We created a multicenter retrospective cohort of patients with PEP by reviewing all ERCPs that were performed between 2012 and 2017 from seven Dutch and one US hospital. The hospitals consisted of two university medical centers (one Dutch, one US) and six large teaching hospitals. We reviewed all hospital contacts up to 48 hours after ERCP in order to discover incident cases with PEP. In the participating centers, it is common practice that patients with symptoms suggestive for adverse events present to the same hospital in which they received their ERCP.
Participants
We included patients if they met the consensus or revised Atlanta criteria for acute pancreatitis (see online Supplementary Table 2). We included patients who fulfilled the revised Atlanta criteria for pancreatitis if they had a hospital stay of at least two additional nights. Their clinical course was comprehensively reviewed in order to assess pancreatitis-related adverse events up to discharge. In patients with necrotizing pancreatitis or organ failure during the initial admission, we checked hospital contacts up to one year after discharge to detect readmissions for the same disease process. Patients with acute pancreatitis prior to ERCP were excluded.
Endpoints
The primary endpoint of the study is PEP-related mortality. The secondary endpoint is PEP severity, defined according to the consensus criteria and the revised Atlanta criteria (see online Supplementary Table 1). We defined local adverse events as an acute peripancreatic fluid collection, pancreatic pseudocyst or necrotizing pancreatitis (parenchymal or peripancreatic).4,14 An intervention was defined as any drainage (percutaneous or endoscopic) or necrosectomy (surgical or endoscopic) for treating PEP. We defined organ failure as follows
15
:
– Pulmonary: PaO2 < 60 mm Hg, despite FiO2 of 0.30, or need for mechanical ventilation; – Circulatory: systolic blood pressure <90 mm Hg, despite adequate fluid resuscitation, or need for inotropic catecholamine support; or – Renal: creatinine >177 μmol/liter after rehydration or new need for hemofiltration or hemodialysis.
Multi-organ failure is defined as the failure of two organ systems at the same time. Persistent organ failure is defined as organ failure lasting >48 hours.
Other variables
Other variables we collected were age, gender, American Society of Anesthesiologists (ASA) score, ERCP indication (adopted from the American Society of Gastrointestinal Endoscopy (ASGE) 16 ), intensive care unit (ICU) admission, length of ICU stay and length of hospital stay. We calculated length of hospital stay in two ways. The total length of hospital stay was calculated as the number of days from ERCP to discharge, regardless of any concomitant disorders. Where possible, we separated this from the length of stay for PEP: the number of days from ERCP until PEP subsided. We defined this as minimal pain medication requirement (non-opioids) and normal diet tolerance. Doubts in the distinction between PEP and other reasons for hospital stay were discussed with the local investigator and, in case of disagreement, resolved after discussion with the lead investigator (EvG). Finally, we scored all concomitant diseases and other reasons for a (prolonged) hospital stay during the initial admission for PEP.
Analyses and statistics
In the primary analysis we investigated the predictive capabilities of both severity definitions for PEP-related mortality. First, we dichotomized both classification systems into mild/moderate or severe PEP. We expressed diagnostic performance in terms of sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV). In the secondary analysis we investigated the correlation between the consensus and revised Atlanta criteria. To that end, we tested their correlation using the chi-square test. Finally, we investigated the effect of concomitant diseases or other reasons on the length of hospital stay. We checked if the PEP disease course could be separated from other reasons for hospital stay.
All analyses were performed by using IBM SPSS version 25. A two-sided P-value below 0.05 will be regarded as significant.
Results
Flow chart
The eight participating centers performed a total of 13,384 ERCPs during the inclusion period (see Figure 1). The inclusion criteria were met in 396 patients (3%). After excluding nine patients who had acute pancreatitis prior to ERCP, the final study population consisted of 387 PEP cases. No patients were lost to follow-up.
Flow chart.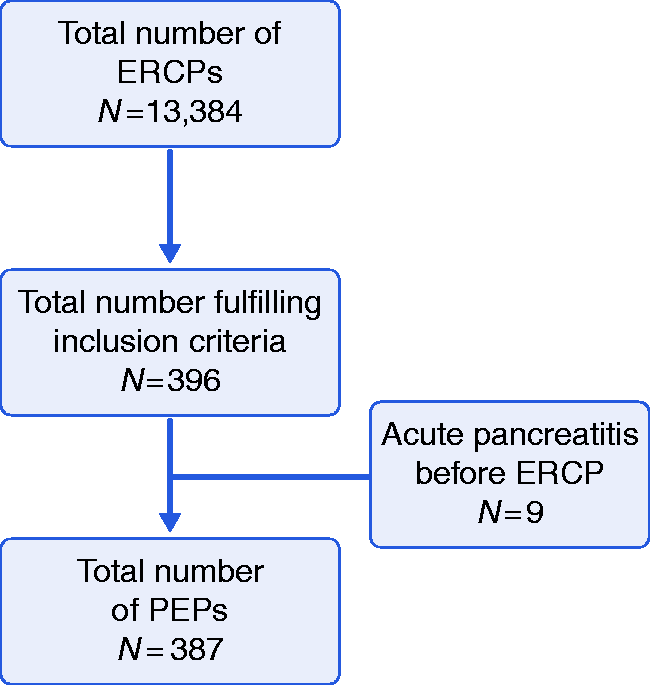
Baseline characteristics
Baseline characteristics.
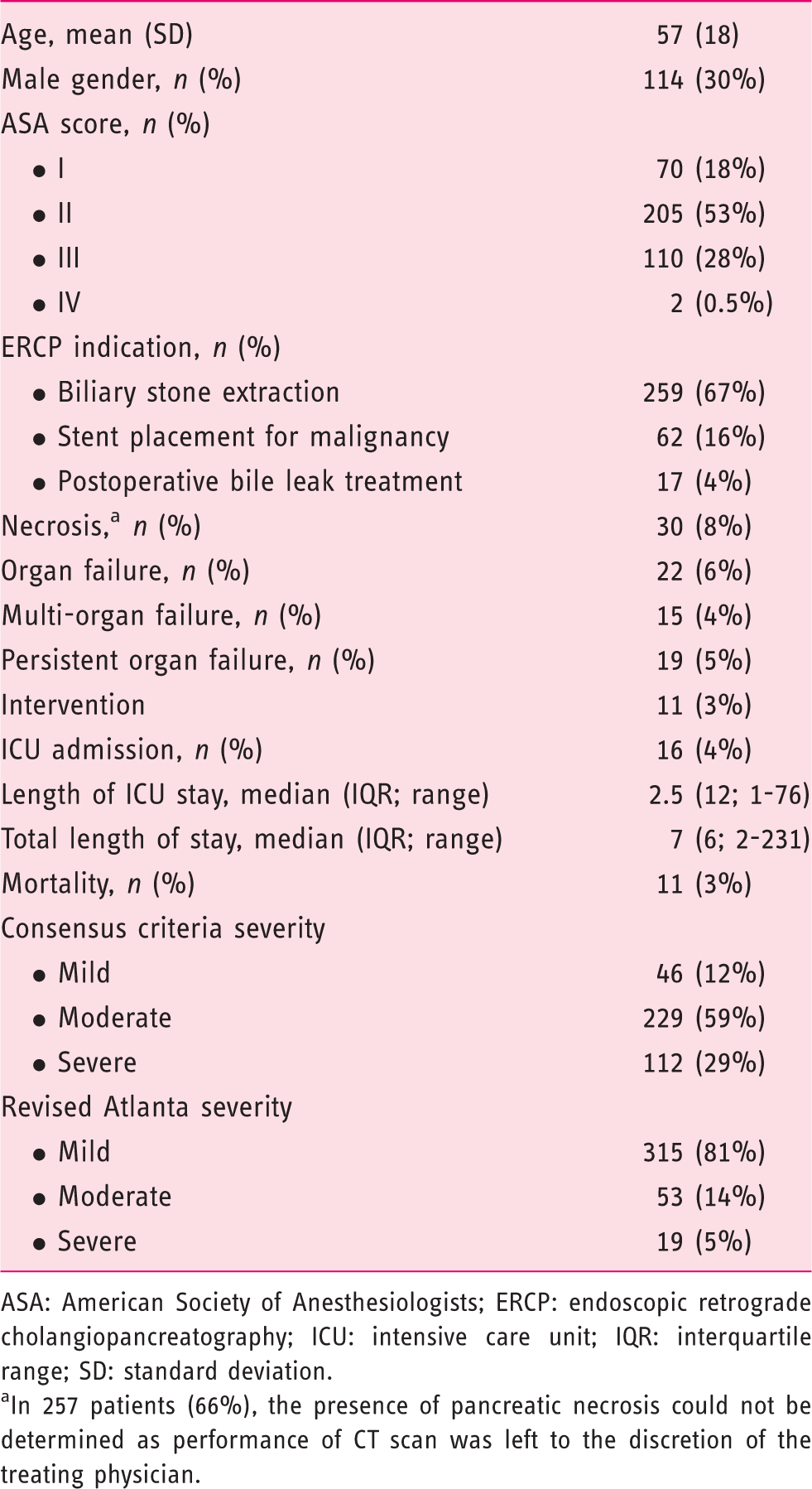
ASA: American Society of Anesthesiologists; ERCP: endoscopic retrograde cholangiopancreatography; ICU: intensive care unit; IQR: interquartile range; SD: standard deviation.
In 257 patients (66%), the presence of pancreatic necrosis could not be determined as performance of CT scan was left to the discretion of the treating physician.
Prediction of PEP-related mortality
Prediction of mortality.
Correlation between the consensus and revised Atlanta criteria
The correlation between the consensus and revised Atlanta criteria is displayed in Figure 2. There is a significant difference between the two classifications (p < 0.001).
Correlation between consensus and revised Atlanta criteria for PEP severity. Values depict number of cases (percentage of total sample). P < 0.001 (Pearson χ2).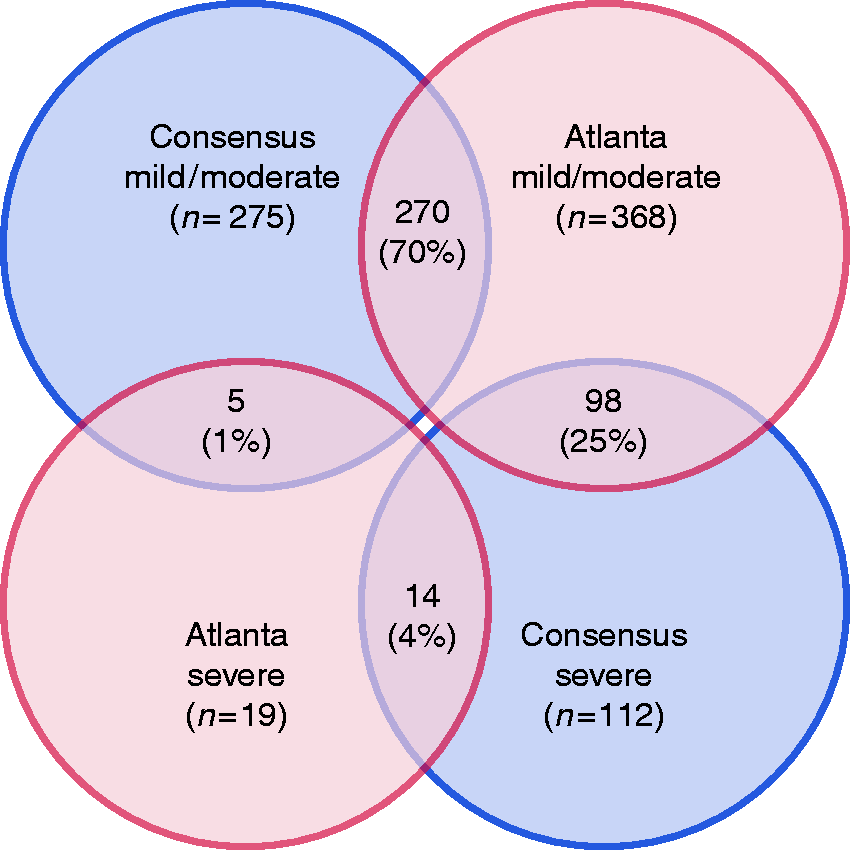
The consensus criteria labelled five cases (1%) as mild or moderate, while the revised Atlanta criteria labelled them as severe. All five patients had fatal persistent organ failure. None of them met the severe consensus criteria because PEP was fatal within 10 days, necrosis was not yet visible on computed tomography (CT) scan and none of them had an intervention.
Furthermore, 98 patients (25%) had a severe course according to the consensus criteria, but a mild or moderate course according to the revised Atlanta criteria. In 76 of those patients (78%), the only reason for a severe consensus label was a hospital stay exceeding 10 days. In the remaining 22 patients (22%), reasons for assigning a severe consensus label were the development of necrosis (in all cases) or an intervention (in six cases). None of these 98 patients had persistent organ failure or died.
Hospitalization and concomitant diseases
We identified the reasons for the length of stay in our cohort (Figure 3). In 263 of the 387 patients (68%), the length of hospital stay was explained solely by PEP. In the remaining 124 patients (32%), the length of stay was influenced by concomitant diseases in 86 patients (69%). In 51 patients (59%), the PEP course could not be distinguished from concomitant disorders. The most prevalent concomitant diseases were cholangitis (n = 33; 38%) and perforation (n = 15; 17%). In 38 patients (31%), prolonged stay was due to other reasons, mainly waitlisted for cholecystectomy (n = 22; 58%) or diagnostic procedures (n = 12; 32%).
Reasons for length of hospital stay in cohort.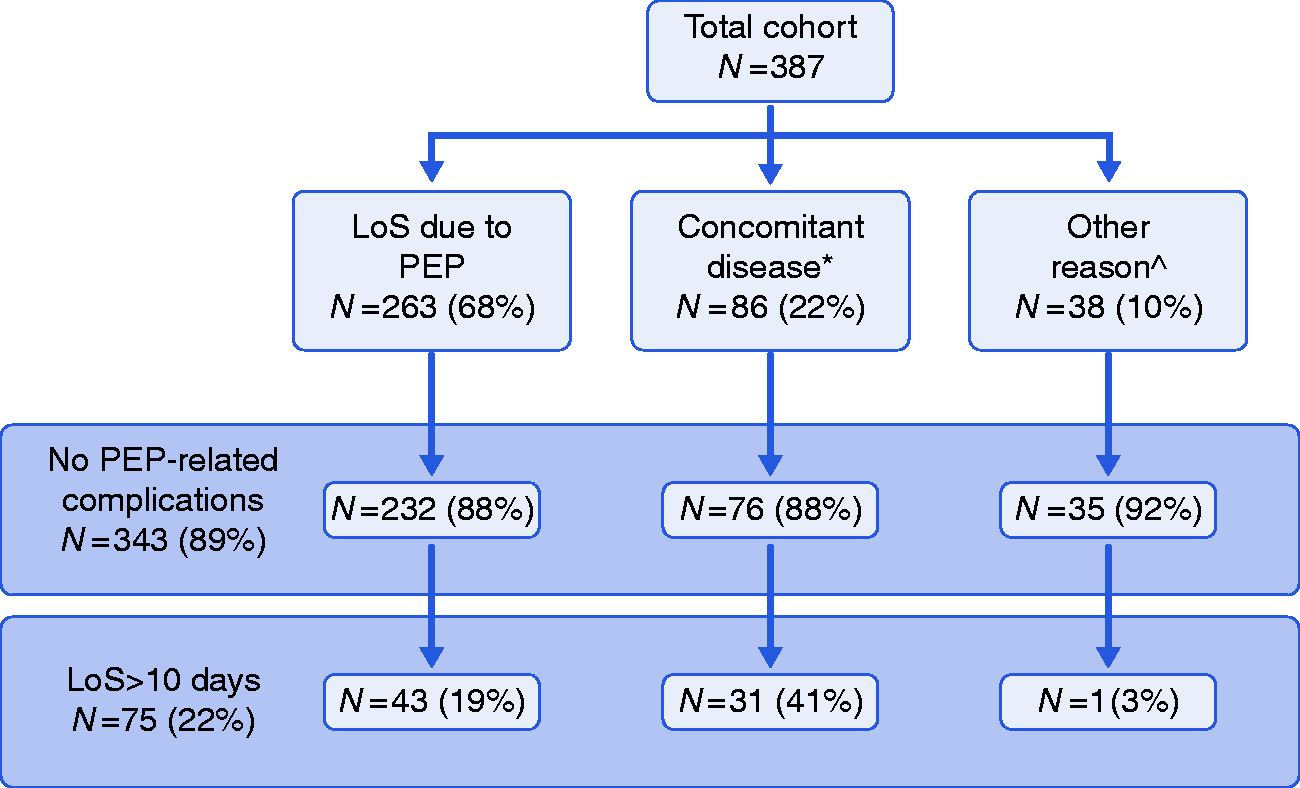
The majority of patients in our PEP cohort had no adverse events related to PEP (necrosis, organ failure or death) (n = 343; 89%). However, 75 (22%) were labelled as severe according to the consensus criteria because the length of stay exceeded 10 days. In the cohort of patients who did not have another diagnosis apart from PEP, the prolonged stay was due to persistent pain, failure to thrive and problems with oral refeeding.
Discussion
Our analysis establishes that the predictive capabilities of the revised Atlanta criteria for PEP-related mortality is better than the consensus criteria in terms of sensitivity, specificity and PPV. The NPV was similar, although three patients with mild PEP according to the consensus criteria died. There is a statistically significant difference between both classifications.
This study identifies three reservations that come with the use of the consensus criteria to define PEP severity. First, these criteria do not capture the patient category with early persistent organ failure, known to have an especially high mortality rate up to 36%.17,18 In our cohort, five of the 11 deceased patients (45%) developed such a disease course. Second, length of hospital stay is problematic as a parameter of disease severity. On the one hand, it was influenced by reasons other than PEP (e.g. concomitant diseases) in 124 patients (32%). This results in a biased assessment of PEP severity. On the other hand, in the majority of patients (n = 343; 89%), length hospital of stay was dictated by persistent pain, failure to thrive or problems with oral refeeding, not by severe morbidity prognosticating mortality. Third, from a methodological point of view, length of hospital stay is subjective and dependent on the treating physician. This could lead to important bias in unblinded studies.19,20
The difficulties with defining PEP severity according to the consensus criteria were also highlighted by three other studies.21–23 The first study 21 reported a smaller discrepancy between the two definitions. According to the consensus criteria, 64 cases were mild, 11 moderate and three severe. When assessed by the revised Atlanta, 76 cases were mild and two were severe. However, the incidence of mild PEP in that cohort is probably overestimated, because the study defined PEP as pancreatic pain and hyperamylasemia (>3 × upper limit of normal), without including the criterion of prolongation of hospitalization (>2 days). Furthermore, because our larger sample size allowed us to identify more patients with a severe disease course, we believe our study was better equipped to point out the differences between the definitions. The second study 22 found a large discrepancy between the consensus criteria and the Ranson score, which is a severity prediction score. In a cohort of 25 PEP cases, 11 had a mild PEP and 14 had a moderate PEP by following the consensus criteria, whereas all episodes were mild by applying the Ranson score. Our results are comparable because we also showed that the consensus criteria have low predictive properties. However, our study also identified the reasons behind the low prognostic accuracy and, more importantly, how this relates to the worth of the consensus criteria as a definition. Finally, in a cohort of 86 PEP cases, the agreement between the consensus and revised Atlanta criteria was tested by Cohen’s K statistic. A value of 0.285 was found, indicating fair agreement between the definitions. 23
Our findings are important from several perspectives. First of all, from a scientific point of view it is necessary to adopt objective definitions that are related to clinically important outcomes. In that way, a reported reduction in PEP severity parallels a reduction in morbidity and mortality. With this study we showed that the revised Atlanta criteria are capable of meeting these requirements better than the consensus criteria. A further advantage would be that PEP severity can be more easily compared to acute pancreatitis of other etiology, which is reported according to the revised Atlanta criteria.
Nevertheless, adopting the revised Atlanta criteria will have a profound influence on the feasibility of PEP studies, because severe PEP will then be an even rarer occurrence: in our PEP cohort, only 19 patients (5%) had severe PEP according to revised Atlanta, against 112 (29%) if the consensus criteria are used. Therefore, it will be exceedingly difficult for studies to detect a difference in PEP severity with sufficient statistical power. This calls for alternative methods such as individual patient data meta-analyses or composite endpoints.
Second, from a clinical perspective our results shed light on how to value PEP prophylaxis efficacy. Major PEP trials report relative risk reductions in moderate–severe PEP of up to 50%.7,8 Because they adopted the consensus criteria, this mainly translates to a reduction in hospital stays from ≥4 days to <4 days, not necessarily in a reduction of clinically important outcomes such as (persistent) organ failure. 24 This is important when assessing the cost–benefit ratio of conducting an ERCP and in the informed consent procedure for patients undergoing ERCP.
Despite the issues raised here, it must be stressed that the consensus criteria are valuable from a patient and societal perspective, since longer hospital stays lead to reductions in quality of life and higher costs and odds of mortality.25–27 Additionally, although problems like oral refeeding are clearly distinct from adverse events like organ failure, they probably carry significant meaning from a patient’s view. That is important in light of patient-reported outcome measures and patient-centered care.28,29 Because of that, there is perhaps a role for both systems in defining PEP severity. At the very least, the issues raised by this study justify reporting both classifications.
Some limitations might be important for the interpretation of our results. First, our study is retrospective. However, data collection was complete and there were no losses to follow-up. We may have missed patients with subclinical pancreatic necrosis as it is common clinical practice to only perform a CT scan in case of clinical deterioration. This could lead to an underestimation of necrotizing PEP in our cohort and result in a lower incidence of severe PEP according to the consensus criteria. On the other hand, this would have increased the discrepancy between the two definitions. A second limitation is our relatively limited sample size (i.e. only 11 deaths). However, our cohort is one of the largest reported and is well equipped to point out the main differences between the two definitions.
In conclusion, the revised Atlanta classification is the preferable system to define a PEP disease course and is superior in predicting PEP-related mortality. This has important implications for researchers, clinicians and patients. For the diagnosis of PEP pancreatitis, the consensus criteria remain the golden standard.
Declaration of conflicting interests
None declared.
Ethics approval
The study was approved by the Medical Ethics Committee of the Radboud University Medical Center on December 1st 2016 (nr. 2016-2974) and follows the declaration of Helsinki.
Funding
This work was supported by The Netherlands Organisation for Health Research and Development (grant number 837001506).
Informed consent
As this study was an anonymous, retrospective evaluation of hospital charts, in which collected data could not be traced back to individual patients, it was not necessary to obtain written informed consent.
Supplemental Material
Supplemental material for The revised Atlanta criteria more accurately reflect severity of post-ERCP pancreatitis compared to the consensus criteria
Supplemental Material for The revised Atlanta criteria more accurately reflect severity of post-ERCP pancreatitis compared to the consensus criteria by XJNM Smeets, N Bouhouch, J Buxbaum, H Zhang, J Cho, RC Verdonk, TEH Römkens, NG Venneman, I Kats, JM Vrolijk, GJM Hemmink, A Otten, ACITL Tan, BJ Elmunzer, PB Cotton, JPH Drenth and EJM van Geenen in United European Gastroenterology Journal
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.