
Abstract
Background
Acute pancreatitis is one of the most common causes of gastrointestinal-related hospitalization and the incidence is increasing. Endo- and exocrine pancreatic function can be compromised after acute pancreatitis.
Objective
The purpose of this study was to explore the long-term consequences of post-endoscopic retrograde cholangiopancreatography pancreatitis (PEP) on pancreatic function.
Methods
A follow-up study was carried out with prospective assessment of endo- and exocrine pancreatic function among cases with previous PEP and matched controls from a Danish cohort consisting of 772 patients undergoing first-time ERCP. Pancreatic function was evaluated by faecal-elastase-1 test, blood levels of haemoglobin A1c, C-peptide, vitamin B12, vitamin D and indirectly by changes in body weight.
Results
Twenty-nine cases and 49 controls participated in the study. Mean follow-up time (standard deviation) was 58 (21) months. Twelve (41%), eight (28%) and nine (31%) patients had mild, moderate and severe PEP, respectively. There was no difference between cases and controls with regard to pancreatic function parameters and PEP severity was not associated with pancreatic function. Factors associated with pancreatic function impairment included body mass index, alcohol consumption, age and smoking.
Conclusion
This study suggests that long-term pancreatic function following PEP is similar to the pancreatic function of other patients with comparable gallstone-related morbidity.
Keywords
Introduction
Acute pancreatitis (AP) is one of the most common causes of gastrointestinal-related hospitalization in the USA and the incidence is increasing. 1 Endo- and exocrine pancreatic function can be compromised after AP.2–7 Exocrine pancreatic insufficiency may lead to malabsorption and steatorrhoea, but can be treated with enzyme supplements, nutritional guidance, and smoking and alcohol cessation. 8 Endocrine pancreatic insufficiency causes diabetes mellitus (DM), which is associated with an increased risk of cardiovascular disease, renal insufficiency and neuropathy.9,10
Pancreatic function following an episode of AP has only been explored in uncontrolled studies or in studies using controls chosen from the general population. 11 A recent meta-analysis on the topic suggested a need for studies including a population with AP and matched AP-free controls to explore the impact of AP on pancreatic function, since current studies have yielded conflicting results with regards to pancreatic insufficiency following AP. 10 In general, studies have reported impairment of both endo- and exocrine pancreatic function following AP irrespective of AP severity.2–7 A meta-analysis found that more than one out of three patients with a first-time admittance for AP developed pre-diabetes or diabetes within five years. However, the severity of AP was not significantly associated with the risk of subsequently developing prediabetes and diabetes. 10
The two most common causes of AP are gallstones and alcohol consumption. The association is, however, confounded by negative lifestyle factors that also affect the risk of endo- and exocrine pancreatic insufficiency regardless of AP development.12–16 This emphasises the relevance of including a comparable control group to evaluate the long-term consequences of AP. Endoscopic retrograde cholangiopancreatography (ERCP) is considered the third most frequent cause of AP. 17 Post-endoscopic retrograde cholangiopancreatography pancreatitis (PEP) offers a unique possibility for studying AP because time of onset and the aetiology are well defined. Knowledge of the prevalence and risk factors for pancreatic dysfunction following AP might facilitate selection of patients to be followed up for the prevention of morbidity related to long-term consequences of AP.
The objective of this study was to determine the long-term impact of PEP on endo- and exocrine pancreatic function biomarkers. We hypothesised that development of PEP has long-term clinically important sequelae affecting both endo- and exocrine pancreatic function.
Methods and materials
Data from all ERCP procedures conducted at the Digestive Disease Center, Bispebjerg Hospital during a six-year period from 1 January 2009–31 December 2014 were prospectively registered in a local database. An ERCP cohort has previously been formed using this database, identifying 772 patients undergoing first-time ERCP. 18 Patients were excluded if they had: (a) pancreatitis or a serum amylase level of more than three times the upper limit of normal before ERCP; (b) a rendezvous ERCP procedure; (c) incomplete endoscopic access to the duodenum; or (d) fatal outcome within 24 h after the procedure. All patients in the cohort included after 1 January 2012 received prophylactic rectal administration of diclofenac sodium (100 mg) immediately after the ERCP.
The present study was a prospective follow-up study with matching performed at the exposure level including cases and controls from the ERCP cohort. Cases represent patients from the cohort who developed PEP. Each eligible case was matched with two controls without PEP according to sex, age ± 5 years, American Society of Anesthesiologists (ASA) physical status classification system (ASA 1 and 2 vs ASA 3 and 4) and indication for the ERCP procedure. Eligible cases and controls were invited by mail to participate in the study. Patients who did not respond were contacted by phone. Patients who were willing to participate but unable to visit the outpatient clinic were visited at their residence.
Exposure and outcome measurements
The main explorative variables were PEP and severity level of PEP according to the revised Atlanta consensus definition. 19 PEP was defined as the presence of at least two of the following three features 24 h after ERCP procedure: (a) upper abdominal pain consistent with AP; (b) serum amylase level exceeding the upper level of normal at least three times; or (c) diagnostic imaging findings consistent with AP. The severity level of PEP was defined as: (a) mild: no organ failure or local or systemic complications; (b) moderate: presence of transient organ failure and/or local complications (peripancreatic fluid collections, pancreatic and peripancreatic necrosis, pseudocyst and walled-off necrosis determined by contrast-enhanced computed tomography); and (c) severe: persistent organ failure (>48 h).
The main outcomes were levels of biomarkers on pancreatic function. Exocrine pancreatic function was determined by concentrations of faecal elastases (FEs) in stool samples from all cases and controls using an enzyme-linked immunosorbent assay (ScheBo, Biotech AG, Giessen, Germany). A FE level <200 µg/g was considered abnormal. Patients who had borderline values (FE=150–200 µg) or a watery stool were retested to enhance sensitivity. 20 If they presented with FE<200 on re-test they were considered abnormal. Pancreatic exocrine deficiency-associated malnutrition was evaluated by levels of vitamins B12 (reference level ≤ 200 pmol/l and vitamin D (reference level ≤ 50 nmol/l) in venous plasma as well as change in measured body weight from inclusion to follow-up. Endocrine pancreatic function was indirectly evaluated by means of fasting plasma proinsulin C-peptide (reference level > 700 pmol/l), haemoglobin A1c (HbA1c) (reference level ≥ 48 mmol/mol) and mean glucose (reference level ≥ 7.7 mmol/l) in the blood. The individual case and its matched controls were tested within a two-week range in order to avoid fluctuations in vitamin D levels due to seasonal changes. All analyses were performed at the Department of Clinical Biochemistry, Bispebjerg Hospital, University of Copenhagen, Denmark.
Statistics
Linear regression was performed for continuous variables and statistical significance was defined as a p < 0.05. Normal distribution of variables in the models was defined as a linear fit of standardised residuals in normal Q-Q plots at visual inspection. Plots of residuals over fitted values were inspected for deviations from zero, and for not being randomly distributed. Models were controlled by an exclusion of outliers followed by an inspection of plots and estimates. All of the models had satisfactory linear fits and residuals did not deviate from zero. Exclusion of outliers did not change estimates significantly. Multivariable models were adjusted for age, sex and variables with possible association to both exposure and outcome. Follow-up time was included in order to adjust for possible time-dependent changes of pancreatic insufficiency following PEP. Cholecystectomy during the observation period was adjusted for, due to the possible metabolic changes associated with this procedure. 21 Diabetes was defined as using antidiabetic medication. In order to explore which baseline variables determined pancreatic function at follow-up, post-hoc analyses were performed on multivariable models with backward elimination of variables with no significant association.
Results
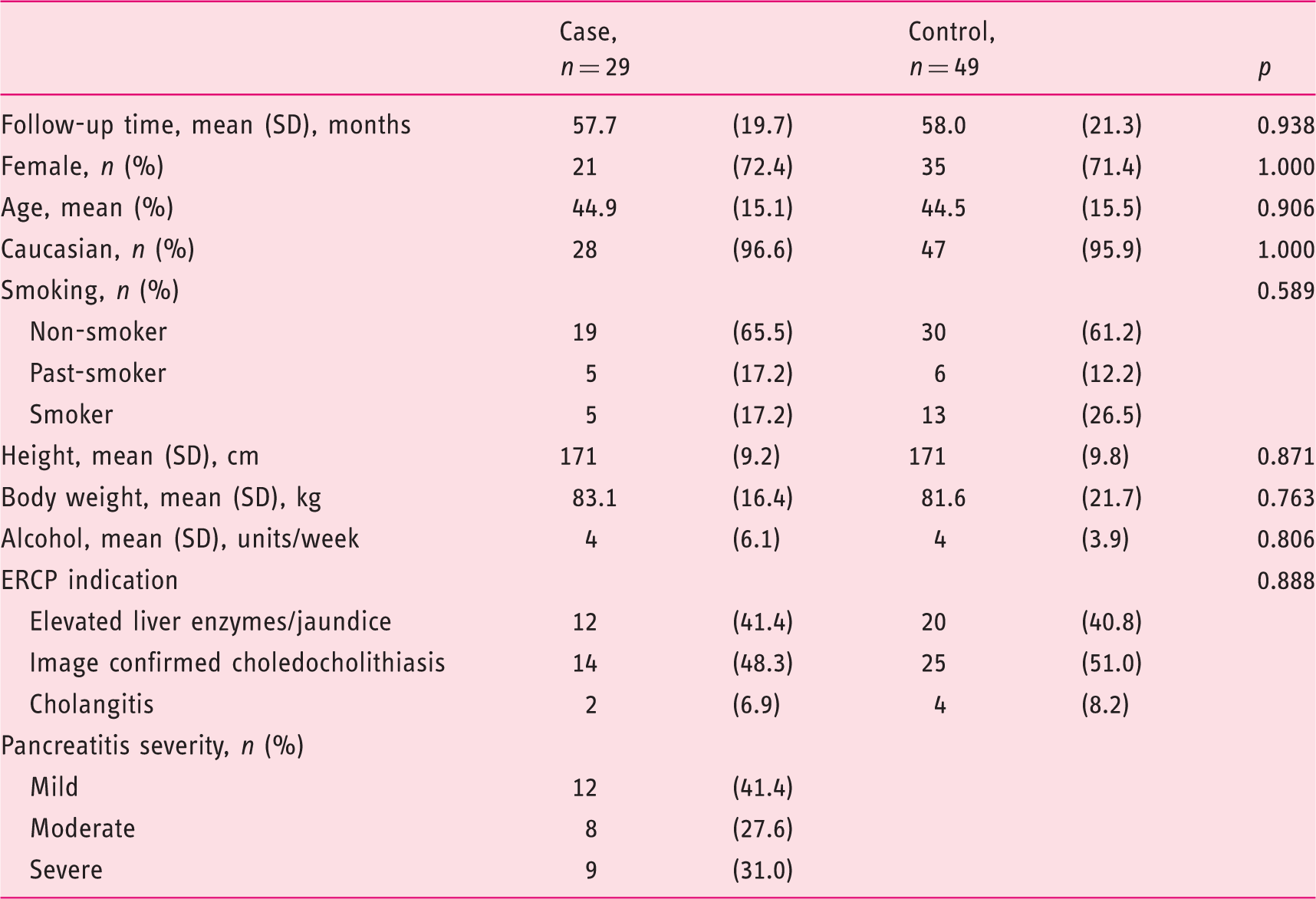
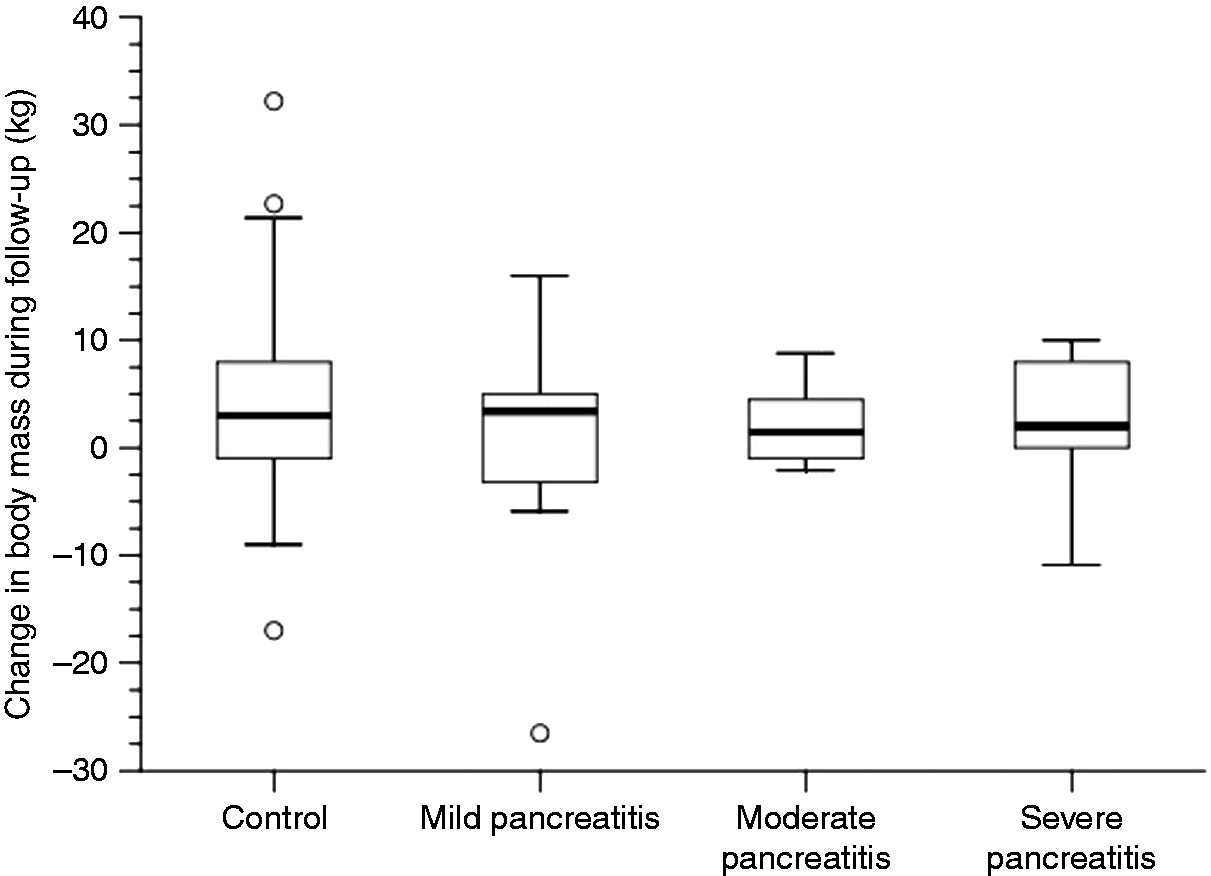
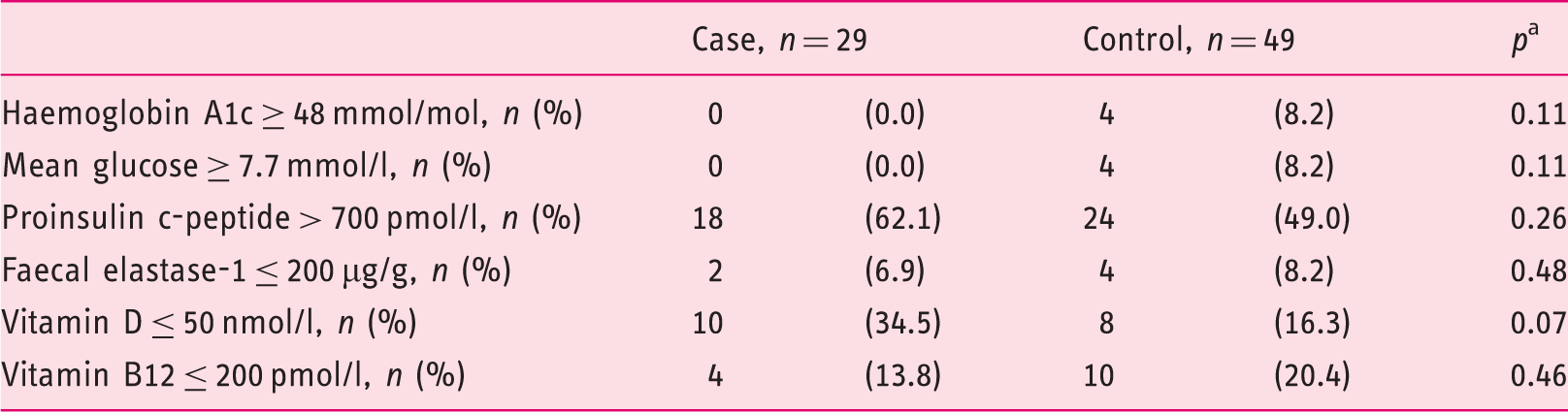
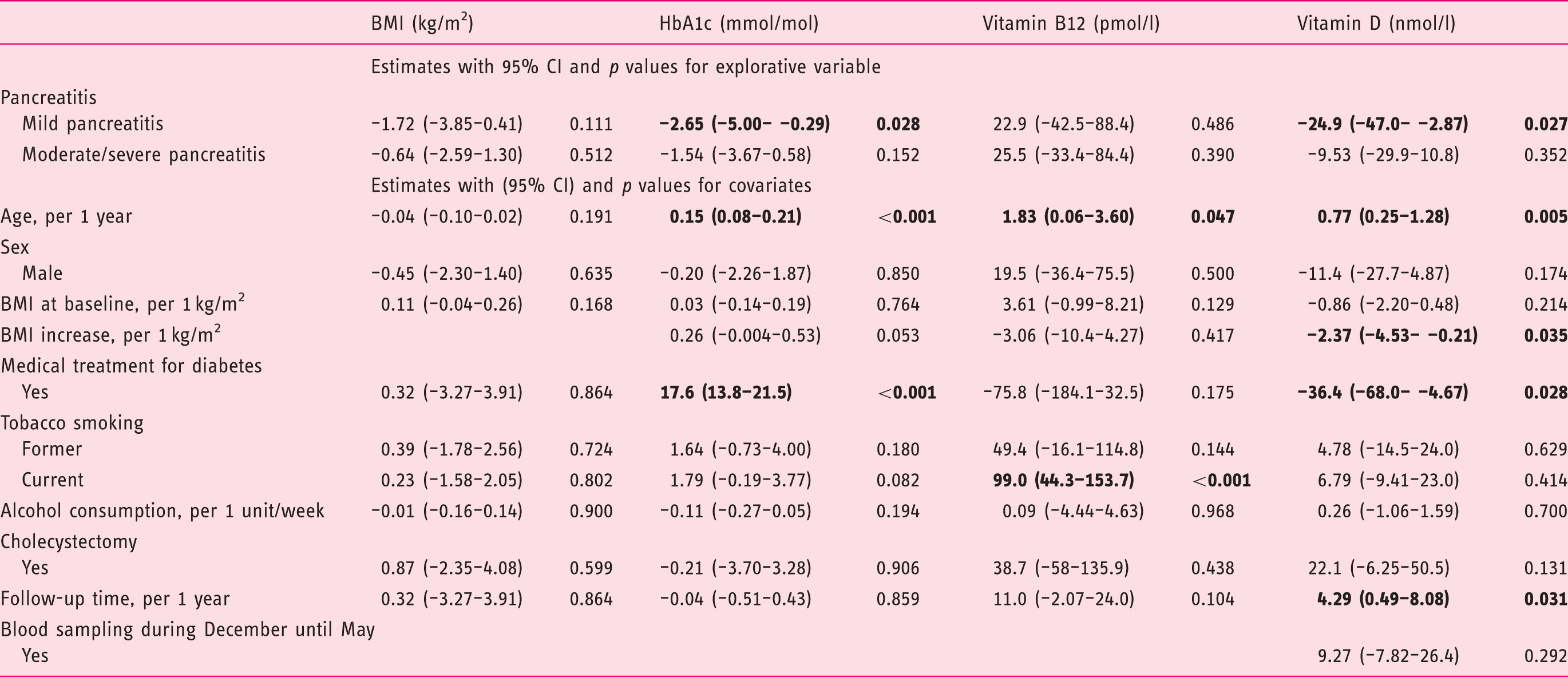
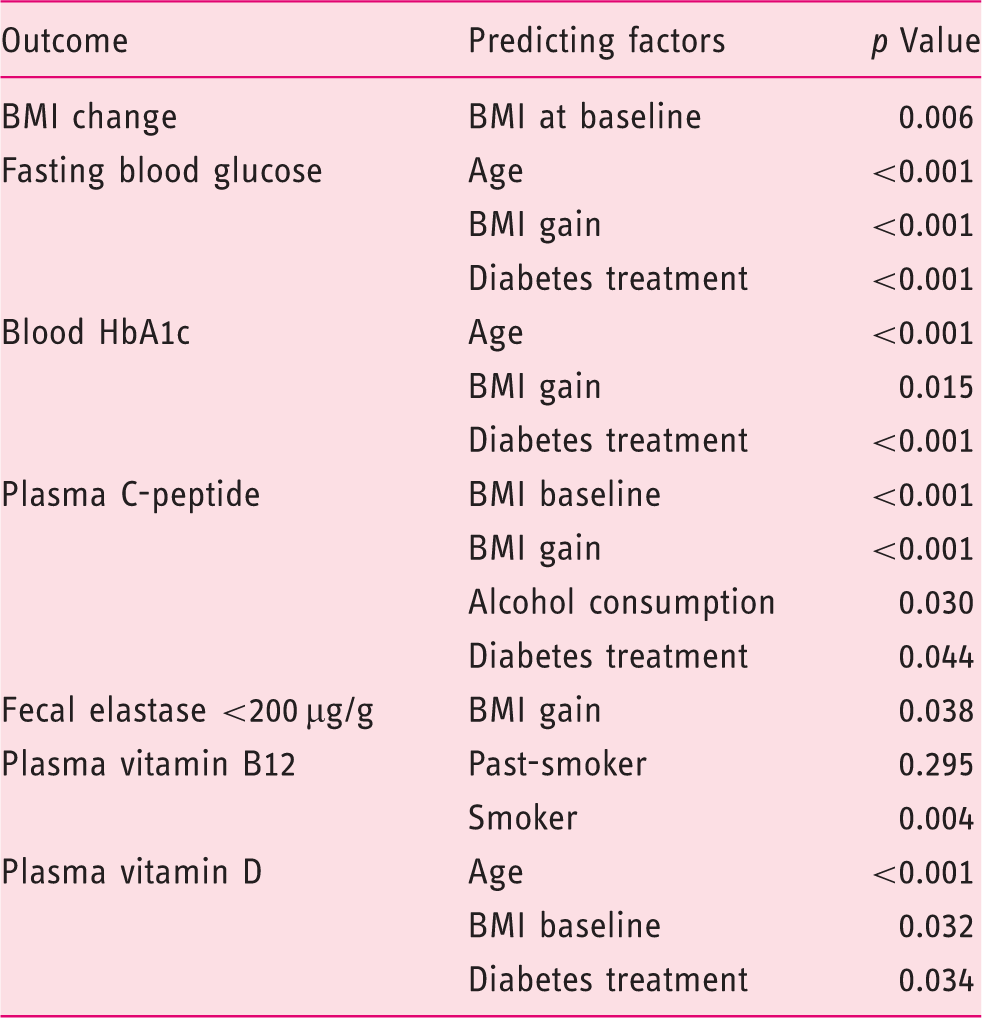
A total of 77 cases (10%) of PEP were identified of which 29 were available for further analysis. For comparison 49 matched controls were included in this study (Figure 1). Twelve (41%), eight (28%) and nine (31%) patients had mild, moderate or severe AP according to the Atlanta classification of severity. The baseline characteristics were consistent across cases and controls, and there were no differences between the groups with regard to risk factors for compromised pancreatic function or indication for ERCP (Table 1). Mean follow-up time was 58 (standard deviation (SD) 21) months. The 78 cases and controls had a 3.4 (8.6) kg mean weight gain during follow-up with no significant difference between the groups, p = 0.19 (Figure 2). Elevated levels of HbA1C in blood was present in none of the 29 cases and in four of the 49 controls (8%), p = 0.11 (Table 2). Impaired exocrine pancreatic function indicated by low FE was present in two of 29 cases (7%) and in four of 49 controls (8%), p = 0.48 (Table 2). There was no significant difference between cases and controls in terms of measurements of malabsorption (Table 2). There was no significant association between the severity level of AP and succeeding parameters of exocrine pancreatic function including FE, vitamin D and vitamin B12 measurements. In multivariable linear regression analyses, moderate to severe PEP was not associated with impaired endo- and exocrine pancreatic function. Mild pancreatitis was significantly associated with a lower level of HbA1c and vitamin D (Table 3). Body mass index (BMI), diabetes, alcohol consumption, tobacco smoking, and age remained statistically significant in post-hoc backward elimination analyses of variables associated with impaired pancreatic function (Table 4).
Consort diagram. ERCP: endoscopic retrograde cholangiopancreatography; PEP: post-endoscopic retrograde cholangiopancreatography pancreatitis. Characteristics of cases and controls. ERCP: endoscopic retrograde cholangiopancreatography; SD: standard deviation. Patient body-mass change during follow-up according to disease severity. Abnormal endo- and exocrine pancreatic function according to case/control status and evaluated by clinical limits. Fishers exact test. Multivariable linear regression analyses on predicting change in outcome parameters from index endoscopic retrograde cholangiopancreatography (ERCP) to follow-up. CI: confidence interval; BMI: body mass index; HbA1c: haemoglobin A1c Significant findings (p<0.05) are in bold. Post-hoc backward elimination analyses of variables associated with measurements of impaired pancreatic function. BMI: body mass index; HbA1c: haemoglobin A1c. All models included age and sex.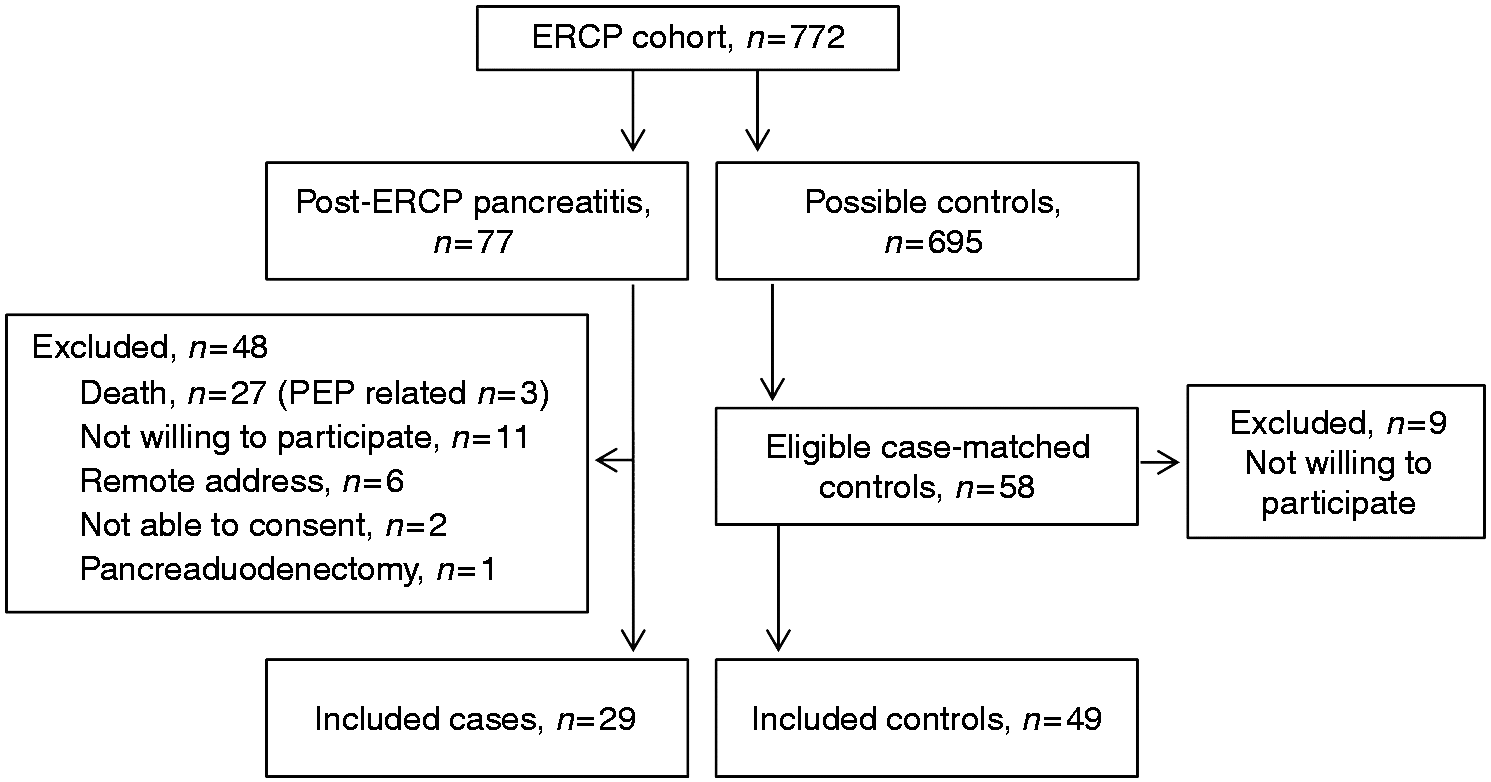
Discussion
In this controlled cohort study previous PEP was not found associated with development of endo- or exocrine pancreatic insufficiency as compared to matched controls. In contrast to this study most previous studies on the long-term consequences of AP mainly included patients with different aetiologies of AP, a severe course of AP, and were non-controlled. Moreover, they did not apply the revised Atlanta classification of AP severity11,19 making it difficult to compare results on the long-term consequences of disease severity.
In line with previous conducted case-series, we found a limited effect of AP severity on subsequent endocrine or exocrine pancreatic function. 11 There was a significant association between certain lifestyle related parameters and subsequently increased HbA1C, mean glucose and proinsulin levels at follow-up. Altogether, these results suggest that follow-up after AP might not be best planned according to the severity level of AP, as individual patient characteristics and presence of pancreatic necrosis are more predictive of compromised pancreatic function.5,22,23 The low incidence of pancreatic dysfunction in our study is probably related to the fact that only one patient developed necrotising AP, since that is a known risk factor for subsequent pancreatic dysfunction.22,23 Pancreatogenic diabetes is in concordance with the definition by Ewald and Bretzal, 24 related to the presence of pancreatic exocrine insufficiency measured by FE; the present study only revealed a FE below the lower level of normal in two cases, neither of which were treated with antidiabetics, and which showed no evidence of prediabetes or diabetes in the obtained tests. The question is whether only patients with necrotising pancreatitis and subsequent chronic pancreatitis develop a significant loss of β-cell function and thus T3cDM (type 3c diabetes mellitus). This is in line with another study where 79% of the patients developing new-onset diabetes during index hospitalization had pancreatic necrosis and 64% of patients that required pancreatic enzymes supplements following AP had pancreatic necrosis. 25
High BMI, abdominal adiposity and hypertriglyceridaemia are known risk factors for AP26–28 and a large prospective cohort found a 50% increased risk of AP in type 2 diabetics. 29 We found comparable elevated levels of proinsulin c-peptide in more than 50% of cases and controls at follow-up and respectively 21% and 26% were considered obese (BMI ≥ 30 kg/m2) prior to the index ERCP procedure. This supports the idea that some of the reported long-term parameters might be related to pre-existing conditions, life-style factors and perhaps metabolic syndrome – rather than consequences of AP. 30
The results of the current study support the concept that restitution of pancreatic function occurs in most patients after an episode of PEP and that this favourable process is limited by negative lifestyle factors. Alcohol abuse, smoking and pancreatic necrosis are associated with a higher risk of both recurrent and chronic pancreatitis, and it has been suggested that only the presence of recurrent AP or low grade chronic inflammation of the pancreas are driving mechanism(s) for fibrogenesis and the associated risk of pancreatic insufficiency.31–33
In conclusion, the available data suggest that reduced intake or abstinence from alcohol consumption, smoking cessation, weight loss in the obese and cholecystectomy in patients with cholelithiasis,34,35 are recommended to reduce risk of developing endo- and exocrine pancreatic dysfunction following AP. The effect of lifestyle-interventions after AP on subsequent pancreatic function should be explored in a randomised controlled trial.
Certain limitations of this study should be considered. Firstly, a large number of patients were excluded, mainly due to cancer-related death. Secondly, a relatively low incidence of both endo- and exocrine dysfunction was found compared to other studies. Selection bias may have caused inclusion of the healthiest patients, even though almost one-third of the included patients had severe AP and despite the fact that we had comparable participation rates among the invited cases and controls (Figure 1). Thirdly, exocrine pancreatic function was evaluated using the pancreatic elastase 1 stool test which is considered less reliable compared to the gold standard secretin-cerulein test (SCT). 20 However, the FE1 test has both a specificity and sensitivity of up to 93% and is easily applicable compared to the burdensome assessment of fat absorption (coefficient of fat absorption (CFA)) and the more invasive SCT.36–38 The sensitivity is considered high in the diagnostics of moderate and severe exocrine insufficiency, but considerably lower in mild disease and in patients with watery stools. 20
Three participants had borderline values of FE and were re-tested; all with similar results to the first FE1 test. We speculate that they might have suffered from pre-exocrine pancreatic insufficiency that could have been diagnosed robustly with the CFA test. However, a validated definition with associated cut-off levels for CFA does not exist for pre-exocrine pancreatic insufficiency.36,37
Previous studies have found that malabsorption of vitamin B12 is associated with pancreatic insufficiency, but results have been conflicting and many hypotheses have been generated on the possible mechanics of vitamin B12 deficiency and pancreatic insufficiency.39,40 We also evaluated pancreatic insufficiency by means of vitamin B12 and found no difference in cases and controls.
Strengths of the current study include the use of a well-described and characterised cohort with long follow-up and prospective outcome measurements. To our knowledge, our study is the first to include a relevant control group making it possible to account for other factors possibly related to pancreatic dysfunction. We applied the revised Atlanta criteria and adopted a clinically relevant definition of endo- and exocrine dysfunction.
Conclusion
This study suggests that long-term pancreatic function following PEP is similar to the pancreatic function of other patients with comparable gallstone-related morbidity who have previously undergone ERCP. Factors associated with impaired pancreatic function were high BMI, alcohol consumption, tobacco smoking and advanced age.
Established knowledge on this subject
Pancreatic function can be compromised following acute pancreatitis (AP). Impaired pancreatic function following AP is not limited to severe cases. The risk of endo- and exocrine pancreatic impairment is modified by negative lifestyle factors.
What are the significant and/or new findings of this study?
AP was not found associated with development of endo- or exocrine pancreatic insufficiency when compared to matched controls. Factors associated with pancreatic function impairment included body mass index (BMI), alcohol consumption, age and smoking.
Footnotes
Acknowledgements
The authors would like to acknowledge the contribution of the research staff at The Digestive Disease Center, Bispebjerg Hospital, for assistance in patient inclusion. Author contributions were as follows: Bonna Leerhøy: study concept and design; acquisition of data; analysis and interpretation of data; drafting of the manuscript; critical revision of the manuscript for important intellectual content; statistical analysis; obtained funding; final approval and accountable for all aspects of the work. Daniel M Shabanzadeh: critical revision of the manuscript for important intellectual content; statistical analysis; final approval and accountable for all aspects of the work. Andreas Nordholm-Carstensen: study concept and design; critical revision of the manuscript for important intellectual content; statistical analysis; final approval and accountable for all aspects of the work. Srdan Novovic: study concept and design; analysis and interpretation of data; drafting of the manuscript; critical revision of the manuscript for important intellectual content; final approval and accountable for all aspects of the work. Mark B Hansen: study concept and design; critical revision of the manuscript for important intellectual content; final approval and accountable for all aspects of the work. Lars N Jørgensen: study concept and design; analysis and interpretation of data; drafting of the manuscript; critical revision of the manuscript for important intellectual content; final approval and accountable for all aspects of the work.
Declaration of conflicting interests
Mark B Hansen declares that this was an academic study with no association to Zealand Pharma. The other authors declare that there are no disclosures to make.
Ethics approval
This study was conducted after approval by the Regional Scientific Ethical Committee of the Capital Region of Denmark, 9 March 2016 (protocol number: H-15017822).
Funding
This research was funded by Overlæge Johan Boserup og Lise Boserups Legat.
Informed consent
Both oral and written informed consent were obtained from all cases and controls in compliance with the Declaration of Helsinki V.