
Abstract
Introduction
After standard diagnostic work-up, the aetiology of acute pancreatitis remains unknown in 16–27% of cases, a condition referred to as idiopathic acute pancreatitis (IAP). Determining the aetiology of pancreatitis is essential, as it may direct treatment in the acute phase and guides interventions to prevent recurrent pancreatitis.
Methods
Between 2008 and 2015, patients with acute pancreatitis were registered prospectively in 19 Dutch hospitals. Patients who had a negative initial diagnostic work-up with regard to the underlying aetiology of their pancreatitis were labelled ‘presumed’ IAP. The aim of this study was to assess the use of diagnostic modalities and their yield to establish an aetiology in ‘presumed’ IAP, and to assess recurrence rates both with and without treatment.
Results
Out of the 1632 registered patients, 191 patients had a first episode of ‘presumed’ IAP, of whom 176 (92%) underwent additional diagnostic testing: CT (n = 124, diagnostic yield 8%), EUS (n = 62, yield 35%), MRI/MRCP (n = 56, yield 33%), repeat ultrasound (n = 97, yield 21%), IgG4 (n = 54, yield 9%) and ERCP (n = 15, yield 47%). In 64 of 176 patients (36%) an aetiological diagnosis was established, mostly biliary (n = 39). In 13 out of 176 of patients (7%) a neoplasm was diagnosed. If additional diagnostic workup revealed an aetiology, the recurrence rate was lower in the treated patients than in the patients without a definite aetiology (15% versus 43%, p = 0.014).
Conclusion
Additional diagnostic testing revealed an aetiology in one-third of ‘presumed’ IAP patients. The aetiology found was mostly biliary, but occasionally neoplasms were found. Identification of an aetiology with subsequent treatment reduced the rate of recurrence.
Keywords
Key summary
What is established knowledge on this subject?
The aetiology of acute pancreatitis remains unknown in 16 to 27% of cases. Acute pancreatitis can be wrongfully classified as IAP due to an incomplete diagnostic work-up. The yield of the diagnostic process and its effect on recurrence rates have not been previously described.
What are significant findings in this study?
Additional diagnostic work-up can identify an aetiology one-third of 'presumed' idiopathic pancreatitis patients. Diagnostic work-up is not performed according to current guidelines in most cases. The aetiology most found in 'presumed' idiopathic pancreatitis is occult biliary stones but pancreatic or ampullary tumours are not rare. Especially in patients with recurrent AP, treatment of underlying aetiologies prevents further recurrences.
Introduction
Acute pancreatitis has a wide range of causes; however, in 16–27% of patients the aetiology remains unexplained.1–4 The recommended minimal diagnostic work-up in the acute setting of a first episode of acute pancreatitis has been summarized in the IAP/APA evidence-based guidelines and should comprise at least five elements: (1) a detailed personal history; (2) a family history; (3) a physical examination; (4) laboratory tests (i.e. liver enzymes, calcium, triglycerides); and (5) a transabdominal ultrasound (TUS). 5 If the aetiology cannot be determined using this work-up, the acute pancreatitis is classified as ‘presumed’ idiopathic acute pancreatitis (IAP).
Several causes of acute pancreatitis cannot be reliably identified with this work-up. For instance, microlithiasis and biliary sludge are missed in up to 34% of patients on TUS. 6 Furthermore, rare causes with a major impact on patients, such as a small pancreatic carcinoma, are easily missed by TUS. If a second TUS remains inconclusive, an endoscopic ultrasound (EUS) is recommended as the next diagnostic step. A systematic review from 2015 showed that EUS may identify an aetiology in 61% of ‘presumed’ IAP patients, mainly microlithiasis or sludge. 7 Other recent studies also confirm the value of EUS in the determination of a biliary aetiology of IAP.6,8–10 In the case of a negative EUS, further diagnostic modalities, such as magnetic resonance cholangiopancreatography (MRCP) and computed tomography (CT), should be considered. 5
Some studies have reported on the value of MRCP and EUS in IAP, but studies addressing the efficacy of each step in the diagnostic process are lacking. Therefore, in this study, we evaluated the current diagnostic work-up of ‘presumed’ IAP and the recurrence rate in a multicentre prospective observational cohort. The primary aim of this study is to explore the use of additional diagnostic modalities and associated diagnostic yield to identify underlying aetiologies in ‘presumed’ IAP. The secondary aims are twofold: first, determine the recurrence rate of acute pancreatitis after a first attack of ‘presumed’ IAP, and second, the recurrence rate after treatment of underlying aetiological factors.
Methods
Study design
In this study, 19 hospitals, including five university hospitals and 14 large teaching hospitals, of the Dutch Pancreatitis Study Group (DPSG) collaborated. Between January 2008 and December 2015, nearly all acute pancreatitis patients admitted to these 19 hospitals were prospectively registered with the DPSG. The DPSG acute pancreatitis registration is part of four DPSG randomized controlled trials, i.e. PYTHON-trial (approved 4/3/2008), PONCHO-trail (approved 22/7/2010), TENSION-trial (approved 31/1/2011) and APEC-trial (approved 12/12/2012), and consists of all patients that did not participate in these trials.11–14 The ethical review board approved the protocol for all four trials including the DPSG acute pancreatitis registry. All patients gave written informed consent prior to inclusion. This study was conducted in accordance with the principles of the Declaration of Helsinki.
Study population
Acute pancreatitis was diagnosed according to the revised Atlanta criteria. 15 The patients included had undergone the minimal diagnostic work-up for a first episode of acute pancreatitis. 5 Any additional diagnostic work-up, i.e. repeat TUS, CT, magnetic resonance imaging (MRI)/MRCP, EUS, immunoglobulin G4 (IgG4) or endoscopic retrograde cholangiopancreatography (ERCP), was performed at the discretion of the treating clinician. This was also the case for the treatment strategy for the underlying aetiologies.
To classify a pancreatitis as ‘presumed’ idiopathic, signs of any known aetiological factor had to be absent in the initial diagnostic work-up. The following groups were excluded:
Patients with a biliary aetiology, defined as a serum alanine transferase (ALT) > 2 × upper limit of the normal value, a common bile duct (CBD) diameter of ≥8 mm for age ≤75 and ≥10 mm for age >75 years or gallstones and/or sludge in the gallbladder and/or CBD on the first TUS.16–18 Patients drinking either more than 3 units of alcohol each day, or more than 5 units in the 48 hours prior to the start of abdominal pain.19,20 Patients were also excluded when the medical records did not specify an amount of alcohol used, but treating clinician considered an alcoholic aetiology as likely. Patients with a recent ERCP, recent abdominal trauma, recent abdominal or vascular surgery or with cystic fibrosis or known autoimmune pancreatitis. Patients with a family history of hereditary pancreatitis, i.e. known relatives with chronic or recurrent acute pancreatitis, or with a genetic mutation associated with hereditary pancreatitis.
21
Patients with a serum triglycerides level of >1000 mg/dl or 11.2 mmol/l.
22
Patients with a serum calcium level corrected for the serum albumin level of >12 mg/dl or 3 mmol/l.
23
Patients with chronic pancreatitis according to the M-ANNHEIM criteria.
24
Patients with medication as a possible aetiology. Medication as an aetiology was considered when medication with a definite association with acute pancreatitis was used (see Supplementary Table 1 online) combined with a reasonable temporal sequence with either the start of the medication or dosage increase one month before the onset of the pancreatitis.
25
Additionally, when patients were using experimental medication (e.g. chemotherapy), and the treating clinicians considered this a likely aetiology of the pancreatitis. Patients with known altered anatomy of the pancreas, pancreatic or bile duct(s), i.e. after hepatopancreatobiliary surgery or a pancreas divisum.
In all the patients included in this study the above-mentioned work-up was performed, and was negative for any aetiological factor.
Criteria for the aetiologies found after additional diagnostic work-up were defined according to the above described criteria. Autoimmune pancreatitis was classified as possible aetiological factor when one cardinal feature of the International Consensus Diagnostic Criteria for Autoimmune Pancreatitis established by the International Association of Pancreatology was present. 26
Data collection
Patients were prospectively followed during the initial episode of pancreatitis by means of regular phone calls to the treating clinician to assess the patient's clinical status and treatment strategy. During follow-up, on-site data collection was performed including: data on the disease course, the physical examinations and laboratory values, imaging during follow-up, data on readmissions and on out-patient hospital visits. To potentially identify any aetiological factor, data from all imaging and other tests performed, for any given indication, were collected. If patients were transferred or referred to other hospitals, data from these admissions and/or visits were also collected. Outcome measures were assessed at a minimum of two years after the initial admission. Before analyses, all study data were verified by two independent researchers (NH, DU).
Outcomes
The primary outcome was the use and yield of additional diagnostic tests in patients in whom initial diagnostic work-up failed to determine an aetiology during a first episode of acute pancreatitis. The following tests were included: repeat TUS, CT, MRI/MRCP, EUS, ERCP and IgG4 testing. If multiple aetiological factors were found, the factor for which treatment was initiated was considered the main aetiology. Minimal diagnostic work-up was defined as, a family and personal history, laboratory tests and a TUS. Complete diagnostic work-up according to the IAP/APA guideline was defined as undergoing work-up until an aetiology has been established or until all possible diagnostic tests described in the guideline were performed. The secondary outcome was the recurrence rate of acute pancreatitis after a first attack of ‘presumed’ IAP.
Statistical analysis
All analyses were performed using IBM SPSS statistics for Macintosh version 20 (Armonk, NY: IBM Corp). We performed a subgroup analysis in the patients with a first episode of IAP after initial diagnostic work-up at admission. For every diagnostic modality, the percentage of utilization and the diagnostic yield was determined individually. Diagnostic yield was calculated for each test individually, by dividing the number of positive tests for aetiology by the total number of times this test was performed. The yield was calculated for all available diagnostic modalities with a two-sided 95% confidence interval (CI). Continuous variables are shown as means with SDs and, in the case of a skewed distribution, as medians with interquartile ranges (IQRs). Continuous data was analysed using the Student's t-test and Mann–Whitney test. Fisher's exact test of independence and the chi-square test were used, as appropriate, to compare proportions. A p-value < 0.05 was considered statistically significant.
Results
Baseline characteristics
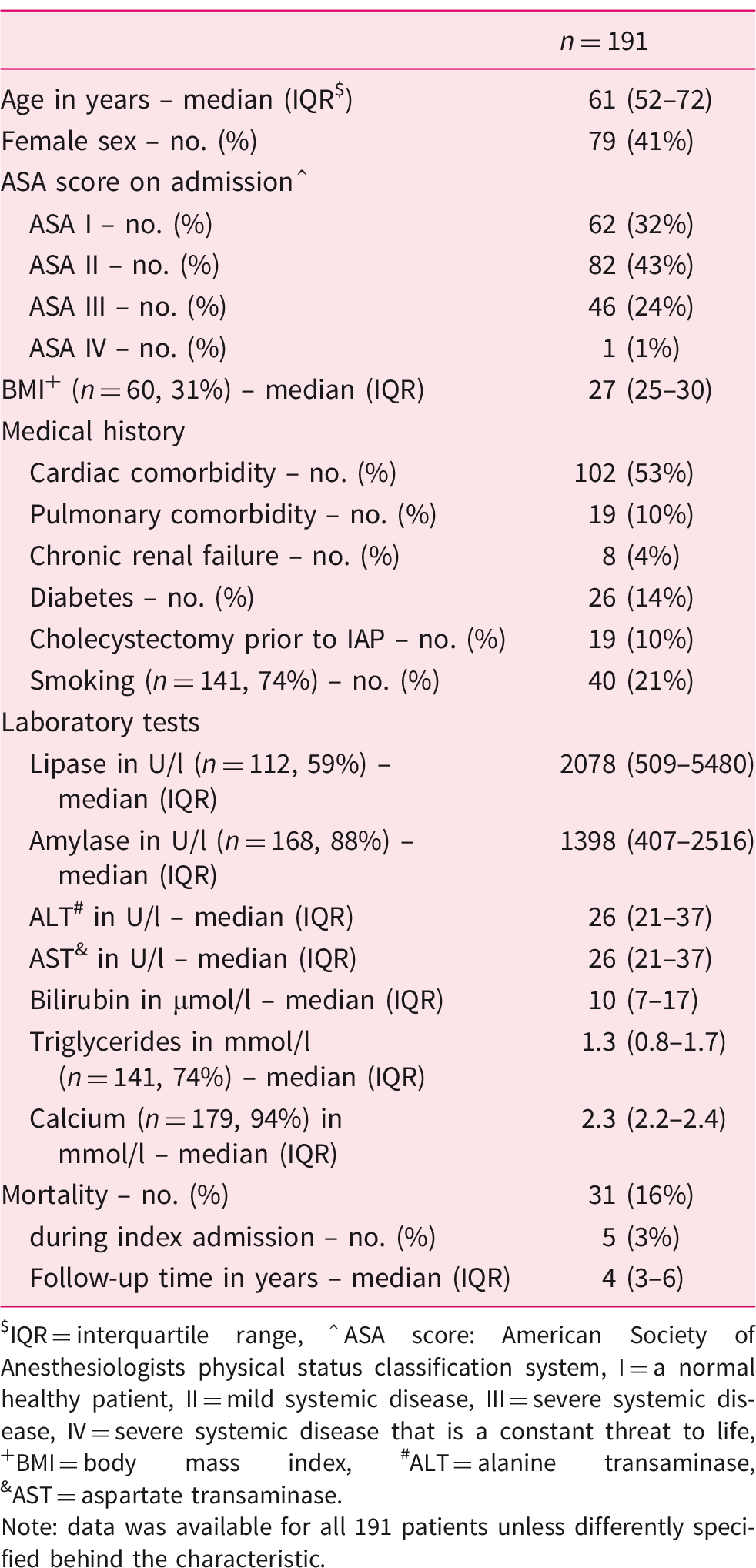
Of the 1632 patients registered between 2008 and 2015, 1615 patients had undergone not more than the minimal standard diagnostic work-up on admission. Seventeen patients who did not have a TUS on admission were excluded. Of these 1615 patients, a total of 191 (12%) were diagnosed with a first episode of ‘presumed’ IAP (Figure 1). Baseline characteristics are shown in Table 1. Seventy-nine of the patients were female (41%), the median age was 61 years. In total, 31 patients died during follow-up, 5 of whom during the initial admission. Significantly more patients with severe systemic disease (ASA class > 2) died compared to more healthy patients and those with mild systemic disease (p < 0.001). None of the patients died during a recurrent pancreatitis episode.
Flow chart of patient selection. Baseline characteristics of patients with first episode of ‘presumed’ idiopathic pancreatitis. IQR = interquartile range, hat;ASA score: American Society of Anesthesiologists physical status classification system, I = a normal healthy patient, II = mild systemic disease, III = severe systemic disease, IV = severe systemic disease that is a constant threat to life, +BMI = body mass index, #ALT = alanine transaminase, &AST = aspartate transaminase. Note: data was available for all 191 patients unless differently specified behind the characteristic.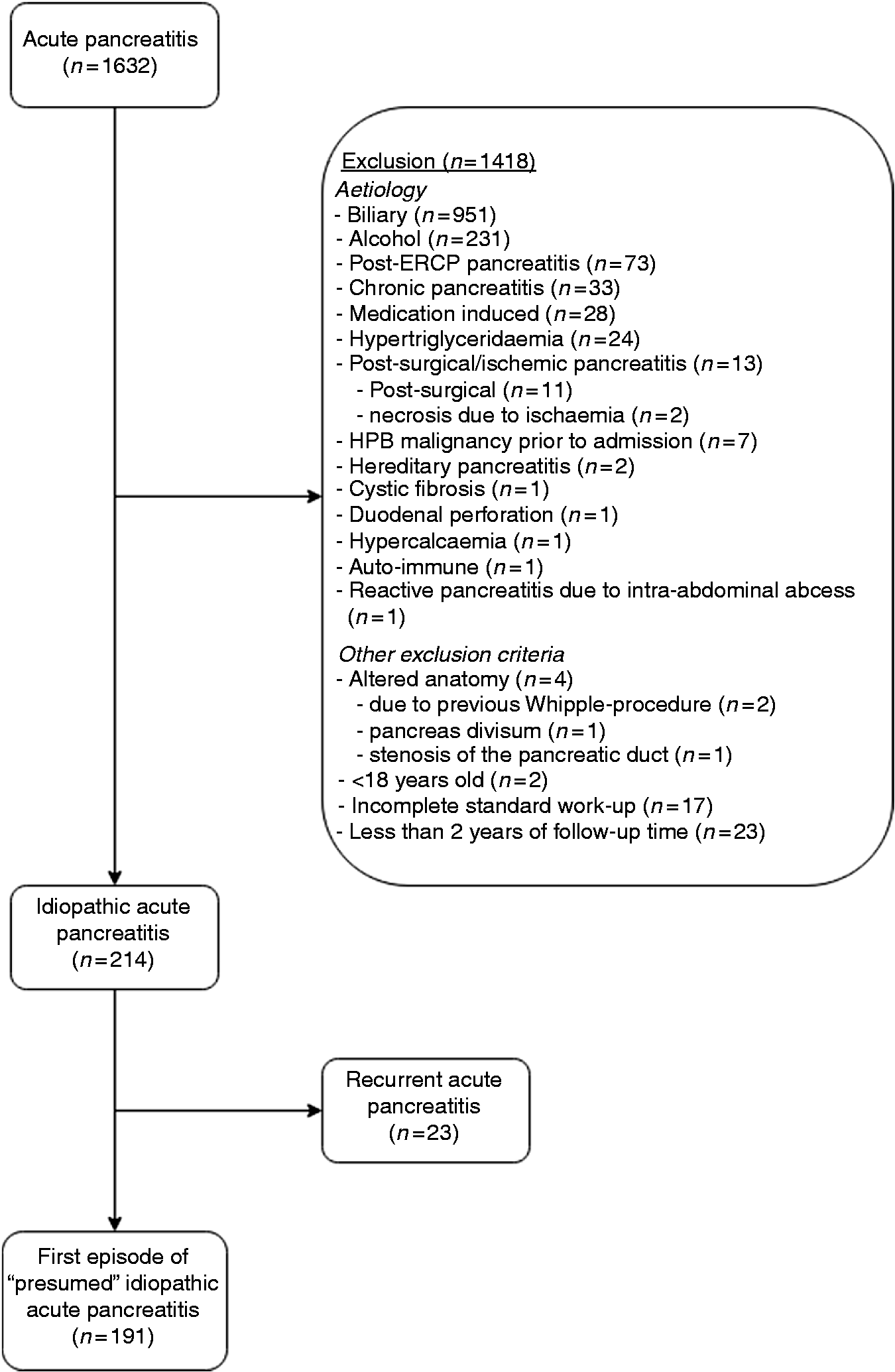
Diagnostic tests
Out of 191 patients with a first episode of ‘presumed’ IAP after minimal diagnostic work-up, 176 (92%) underwent one or more additional diagnostic tests. Fifty-two patients underwent one additional diagnostic test; the remaining 124 underwent more than one test. Forty-one patients (22%) had a complete initial diagnostic work-up according to the IAP/APA guidelines. 5
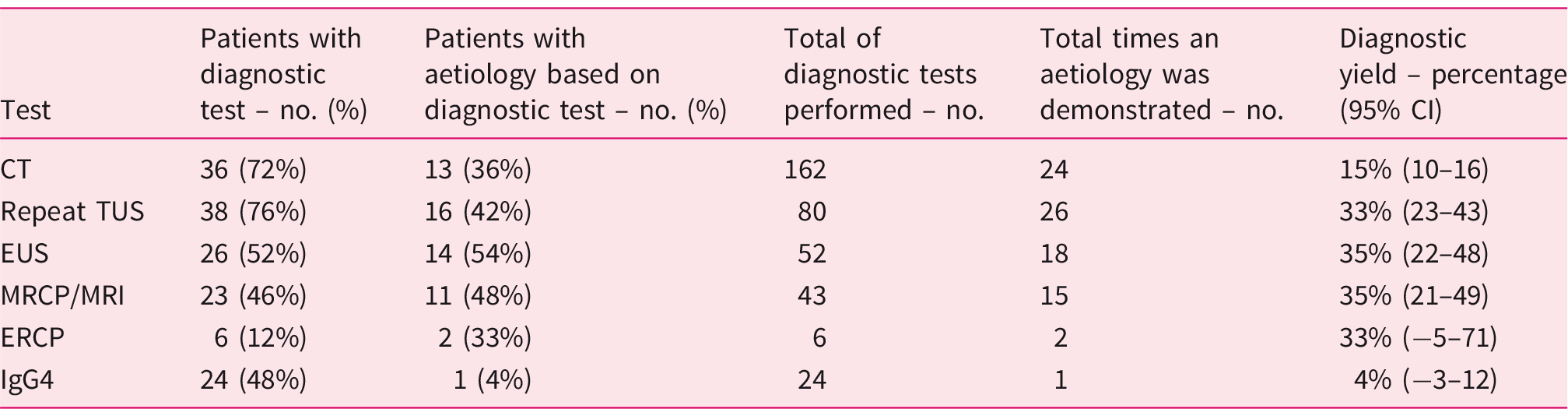
Overview of number and yield of diagnostic tests in all patients (n = 191).
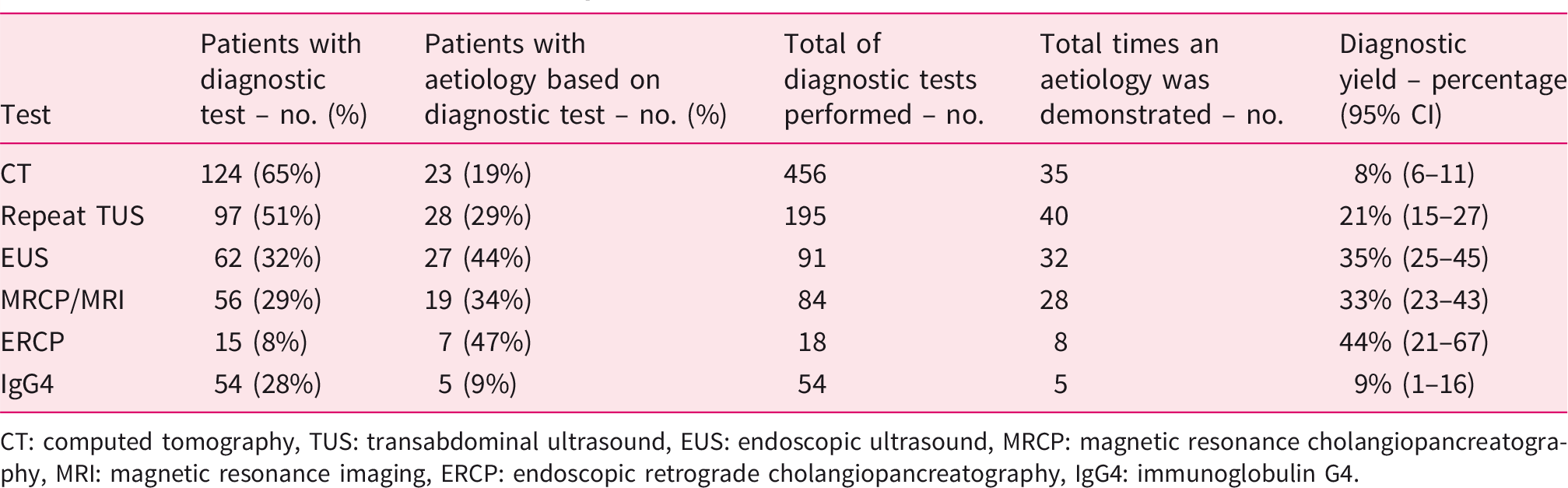
CT: computed tomography, TUS: transabdominal ultrasound, EUS: endoscopic ultrasound, MRCP: magnetic resonance cholangiopancreatography, MRI: magnetic resonance imaging, ERCP: endoscopic retrograde cholangiopancreatography, IgG4: immunoglobulin G4.
Recurrence rate of acute pancreatitis
During a median follow-up of 4 years (IQR 3–6), 50 out of 191 patients (26%) had at least one recurrence, 26 of whom had more than one recurrent episode. In the recurrent pancreatitis group, there were 101 recurrences with a median of two per patient (IQR 1–2).
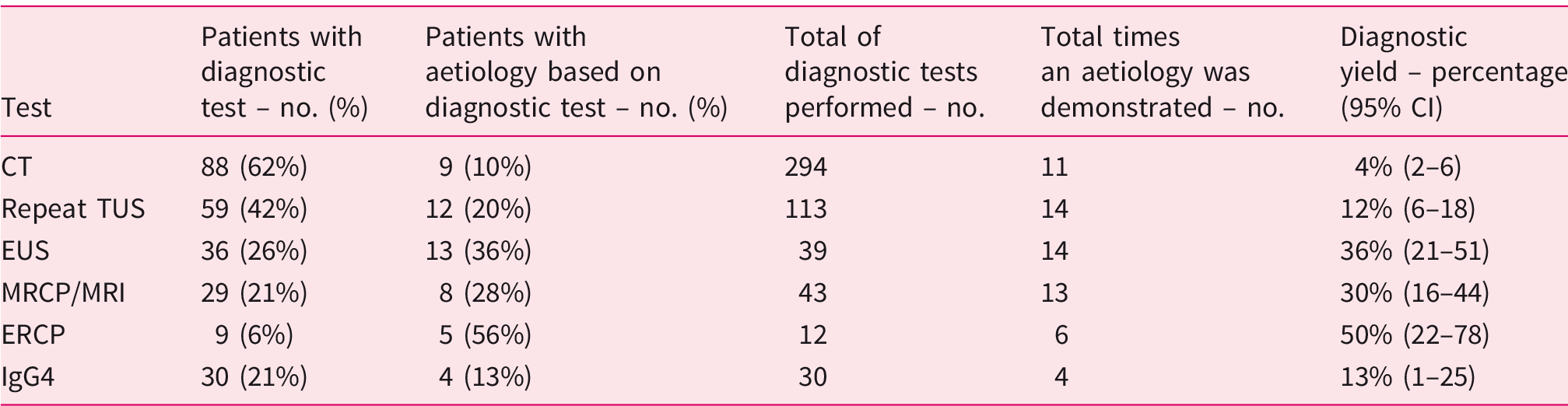
Out of 141 patients with a single episode of ‘presumed’ IAP, 128 patients underwent additional diagnostic testing. In 35 cases (27%), an aetiology was found.
Diagnostic yield of additional diagnostic work-up in the single episode group (n = 141).
Diagnostic yield of additional diagnostic work-up in the recurrent pancreatitis group (n = 50).
Aetiological factors
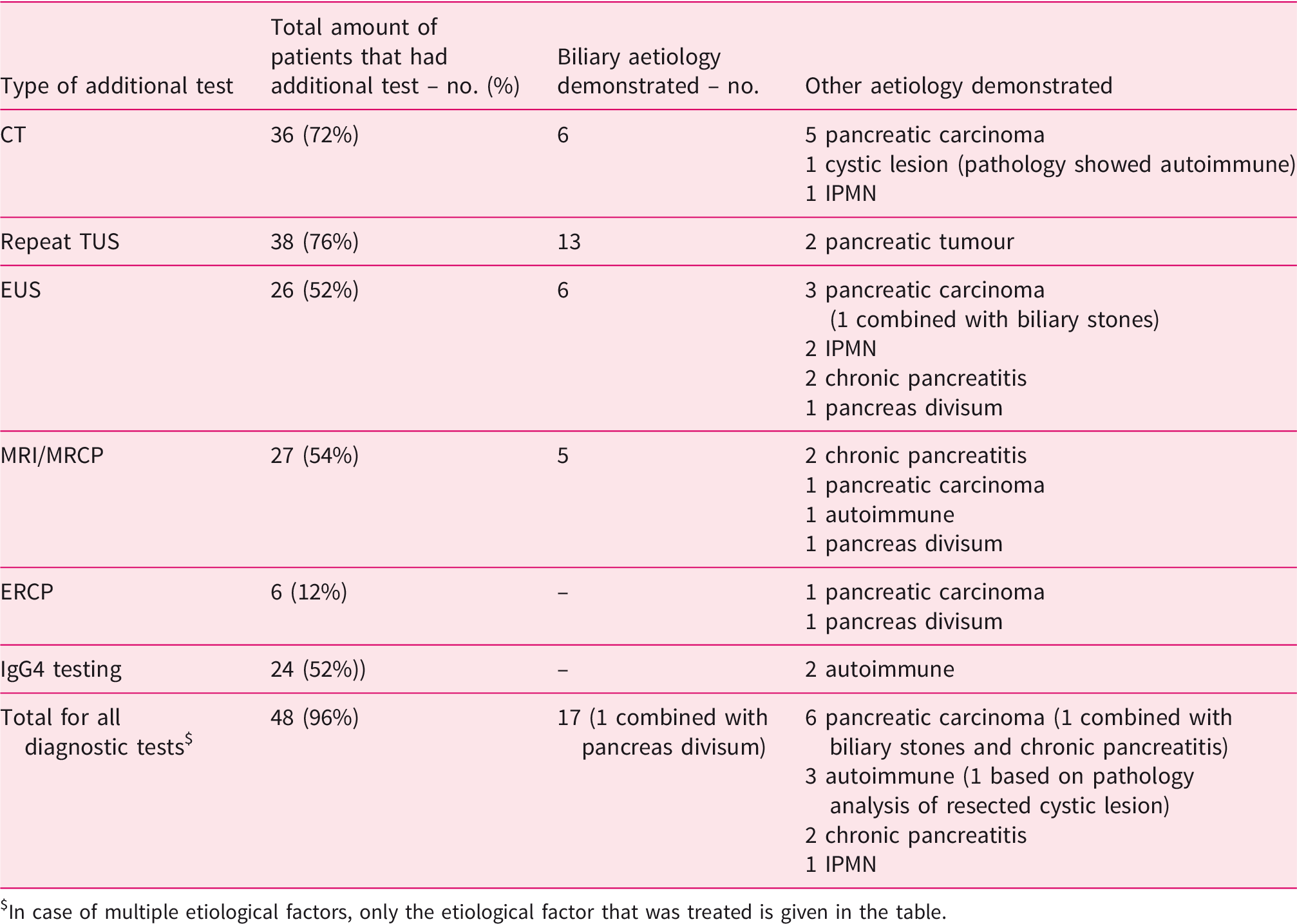
Diagnostic work-up in patients with a single episode of idiopathic acute pancreatitis (n = 141).
In case of multiple etiological factors, only the etiological factor that was treated is given in the table.
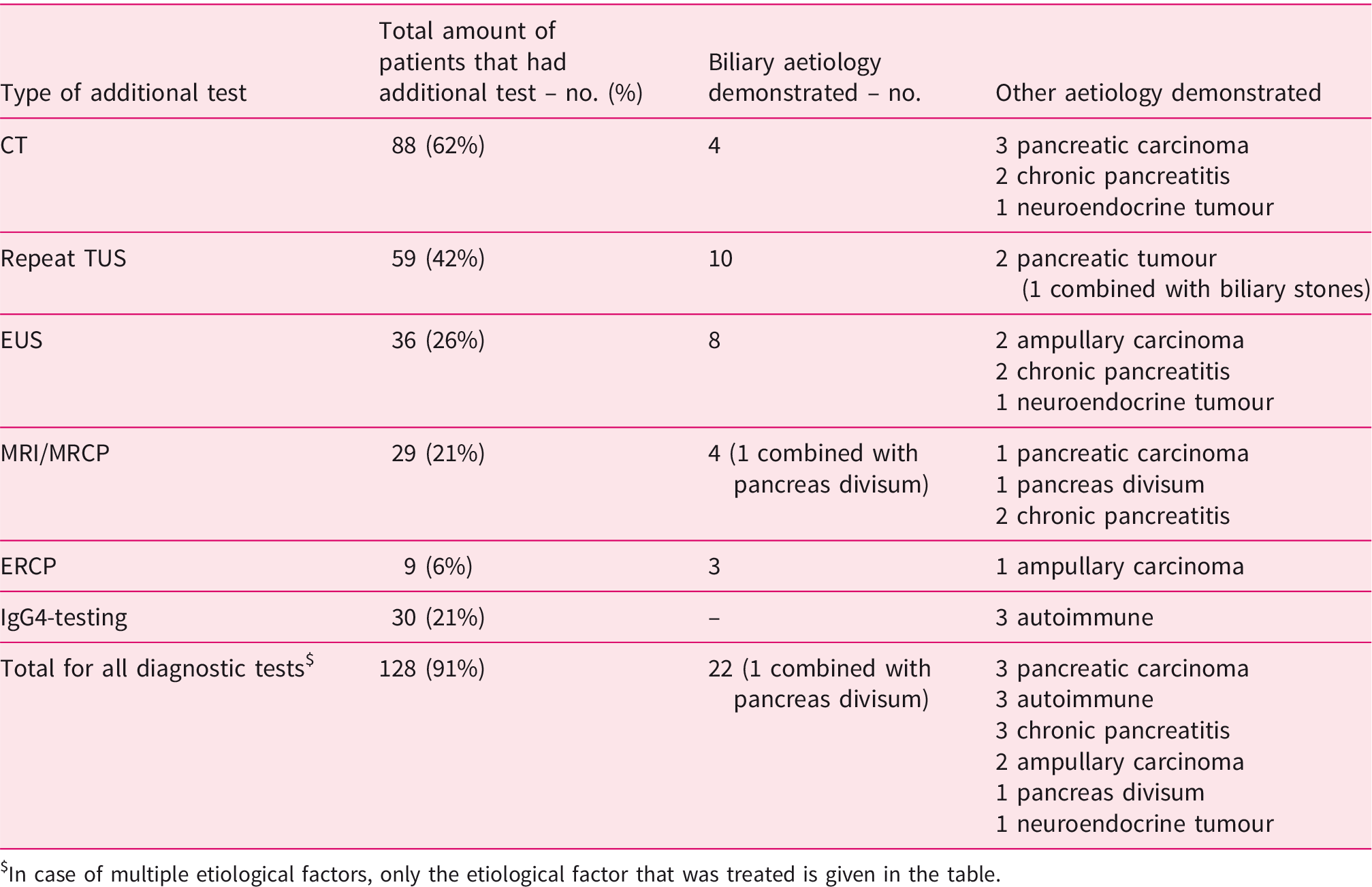
Diagnostic work-up in patients with recurrent acute pancreatitis (n = 50).
In case of multiple etiological factors, only the etiological factor that was treated is given in the table.
In 13 out of 191 of patients (7%), additional testing revealed an ampullary or pancreatic neoplasm. With seven out of 141 patients in the single episode group (5%) versus six out of 50 in the recurrent acute pancreatitis group (12%), neoplasms were significantly more common in the recurrent acute pancreatitis group (p = 0.043). Five patients were shown to have chronic pancreatitis. Serum IgG4 testing was performed in 54 patients (28%), five of whom had levels of 2 times the upper limit of normal (ULN) or higher. Two patients were treated with prednisone with good clinical response, one of which had characteristic findings of autoimmune pancreatitis on MRI. The other three patients had no signs of autoimmune pancreatitis on imaging and did not receive treatment. One of these patients did have a history of ulcerative colitis and had one recurrent episode; the other patient did not have any recurrences. In one patient autoimmune pancreatitis was diagnosed, after six recurrences, in the pathology sample of a pancreatic mass. No serum IgG4 levels of this patient were available. None of the patients were diagnosed with IgG4-negative autoimmune pancreatitis.
Treatment of aetiological factors
Underlying aetiological factors were treated in 34 out of 64 patients in whom an aetiology was found. The other 30 patients did not receive any treatment for underlying aetiologies.
In the treated group, the treatments performed for underlying aetiological factors were the following: cholecystectomy with/without ERCP with sphincterotomy (n = 22), only ERCP with sphincterotomy (n = 3), prednisone treatment (n = 2), pylorus preserving pancreatoduodectomy (n = 4), pancreatic tail resection (n = 1), distal pancreatectomy and splenectomy (n = 1) and a pancreatic duct stent placement (n = 1).
In 21 of 34 patients (62%), the treatment was started after the initial IAP episode, whereas the other 13 patients (38%) had recurrent acute pancreatitis episodes before the start of treatment. After treatment 29 patients out of 34 patients (85%) were free of recurrences. In the group of patients where additional diagnostic workup revealed an aetiology, the risk of recurrence after treatment was 0.34 (95% CI: 0.137–0.841) compared to the risk of recurrence without treatment. In the subgroup of 50 patients with recurrent acute pancreatitis, the recurrence rate after treatment was 31% versus 97% in patients without treatment (p < 0.001), the accompanying relative risk of recurrence in the group without treatment 23.4 (95% CI: 3.296-–165.778), compared to the group with treatment.
Discussion
The aetiology of acute pancreatitis remains unknown 16-26% of cases. In our cohort of 1632 acute pancreatitis patients, 12% was idiopathic which is lower compared to other studies such as the Hungarian Pancreatic Study Group cohort that showed a rate of 16.3%.1–4 Possibly, the strict criteria to define ‘presumed’ IAP in our cohort, especially in regard to absence of a possible biliary aetiology explains this lower rate. For acute pancreatitis, current guidelines advise the diagnostic work-up to comprise at least a thorough personal and family history taking, laboratory tests and a TUS. As a next step, a repeat TUS can be performed to re-assess a potential biliary aetiology. In our cohort half of the patients underwent a repeat TUS with a yield of 21%. Even though current guidelines advise a repeat TUS, few studies have investigated its diagnostic yield in IAP. Signoretti et al. retrospectively investigated the sensitivity, specificity and accuracy for detecting a biliary origin on repeat TUS in a group of 155 acute pancreatitis patients, of whom 85 underwent a repeat US within 1 week after admission. They found a sensitivity of 82%, a specificity of 75% and an overall accuracy of 78% to detect a biliary aetiology. 27 However, they investigated all acute pancreatitis patients and not specifically IAP patients, including those with a first positive TUS giving ample explanation of why their performance was higher compared to our study. Overall, the diagnostic yield of 21% found in this study, combined with the low costs, safety, and widespread availability of TUS, underscore the diagnostic worth of performing a repeat TUS.
In our study the yield of EUS was 36%, which is low compared to other studies. Wan et al. found a diagnostic yield for the aetiology of IAP of 64% for EUS in a meta-analysis of 2,338 patients with IAP, with the most common finding being choledocholithiasis and/or cholecystolithiasis (33%). 6 In a recent systematic review a similar diagnostic yield of 62% with 37% biliary aetiology was found. 10 This difference is likely explained by the fact that most studies in this meta-analysis included patients with high serum ALT levels and/or CBD dilatation prior to EUS resulting in a higher a priori chance of finding biliary stones, thereby increasing the diagnostic yield of EUS. In our study, a biliary aetiology was established using additional work-up in 20% of patients with ‘presumed’ IAP. However, in order to exclude patients with a high likelihood of having a biliary aetiology, the criteria we used to define ‘presumed’ IAP were stricter. Both patients with CBD dilatation and patients with serum ALT levels > 2 × ULN were excluded. Multiple studies have shown that the likelihood of a biliary aetiology is very high in these patients.16–18 Despite these strict inclusion and exclusion criteria in the current study, we found a sizable portion of ‘presumed’ IAP patients that turned out to have occult biliary disease, underlining the importance and need for an additional and detailed work-up in these patients.
The yield of MRI/MRCP (33%) was similar to other studies. The meta-analyses by Wan et al. showed a yield of 34% for MRI. 6 Previous studies have shown that the yield of finding microlithiasis and sludge is higher in EUS than in MRI/MRCP.6,28 Especially in the IAP population, where microlithiasis is considered an important aetiological factor, many clinicians consider EUS the preferred second diagnostic step after TUS.
In current practice, ERCP is not routinely performed for diagnostic purposes due to its associated procedural risks compared to other diagnostic modalities. 29 In the current study, 8% of patients did undergo an ERCP, which was mostly performed for reasons of a high clinical suspicion of biliary stones (i.e. jaundice, progressive cholestasis during admission) or because of a suspected anomaly of the papilla on EUS. In these cases with a high clinical suspicion for pathology, the diagnostic yield of ERCP was high (44%). Nevertheless, this was mostly after presumptive diagnosis was already made with another investigational modality which in fact constituted the indication to perform ERCP. On that note, one might argue that ERCP was negative in the majority of patients (56%) in whom this invasive procedure might have been prevented if, for example, a diagnostic EUS was performed prior to ERCP.
Even though current guidelines do not advise IgG4 testing as part of the diagnostic work-up of ‘presumed’ IAP after a first episode, surprisingly, in almost one-third of patients (28%) in this study serum IgG4 levels were measured. In 9% of those patients the serum IgG4 levels were elevated (i.e. 2x ULN or higher), and two of these patients were treated with prednisone with good response. The International Association of Pancreatology published a consensus guideline on diagnostic criteria for autoimmune pancreatitis stating that elevation in serological markers alone is not deemed sufficient for the diagnosis. 26 The work-up for autoimmune pancreatitis in patients included in this study was not uniformly performed according to guidelines.
In this study genetic counselling or genetic testing was not performed. This might be due to patient selection prior to inclusion, as patients with a family history of hereditary pancreatitis, know genetic mutations or younger patients with non-alcoholic calcifying pancreatitis in whom testing already revealed a genetic cause were excluded from this cohort. Omitting genetic counselling might lead to misclassification of patients with hereditary pancreatitis as idiopathic. Therefore, in accordance with the IAP/APA guideline clinicians should consider genetic counselling in recurrent IAP. 5
Additional work-up revealed a neoplasm in 13 (7%) ‘presumed’ IAP patients. Acute pancreatitis patients are known to have an increased risk of harbouring pancreatic malignancy. 30 A Danish population-based study, perform found that the pancreatic cancer risk was high in patients with IAP, with an adjusted Hazard ratio of 2.52 (95% CI: 1.83–3.47) at 5-years of follow-up. 31 A previous DPSG study confirmed this finding. In that study, a pancreatic cancer rate of 0.7% was found in 731 patients with a first episode of acute pancreatitis, and the risk was 2% in the subgroup of patients with an unknown aetiology. 32 In both aforementioned studies however, the definition of IAP or ‘unknown aetiology’ was not specified.
Most patients in our study had a single attack of ‘presumed’ IAP with a mild disease course. One-fourth of patients had one or more recurrences, which is comparable to previous studies. 33 In a similar Dutch cohort of 669 patients with acute pancreatitis, researchers found a recurrence rate of 17% overall and of 25% in the 108 included IAP patients. 34 However, in that study the definition of IAP was not as clearly described as in the current study, making it difficult to compare results. As expected, we found that treatment of an underlying aetiology reduced recurrence rates.
Strengths and limitations
The current study comprises a large cohort of patients with a first episode of ‘presumed’ IAP, all of whom were prospectively followed for more than 2 years, thus making sure that late complications, aetiological diagnoses and recurrences could be identified. The criteria we used to define patients with ‘presumed’ IAP after an initial work-up was in accordance with the latest literature consensus. Furthermore, the criteria used to exclude patients with a high likelihood of having biliary pancreatitis, alcohol-related pancreatitis or chronic pancreatitis were more strict compared to most other studies investigating the diagnostic work-up of IAP.
There are also limitations to our study. First, serum triglycerides and calcium levels were not available in all patients. Although hypertriglyceridemia and hypercalcemia are considered rare causes of pancreatitis, in this subgroup of patients with unexplained aetiology the proportion might be higher than in the total acute pancreatitis population. Therefore, omitting these tests might have led to an under-diagnosis of these aetiologies. Second, some caution is advised when interpreting the diagnostic yield of additional imaging. We evaluated all diagnostic tests that were performed, not only tests solely performed with the purpose of establishing an aetiology for the (recurrent) pancreatitis. Furthermore, the finding of an aetiological factor using a test is not definite proof that this factor is the definite cause of the acute pancreatitis.
Conclusion
Our study shows that additional diagnostic work-up can identify an aetiology in one-third of patients with ‘presumed’ IAP. The aetiology most commonly found was biliary. However, in a substantial portion of patients an underlying malignancy was detected. Furthermore, we show that the diagnostic work-up after a first attack of ‘presumed’ IAP is performed according to current guidelines in less than one-fourth of patients. This is worrisome, as identification of an aetiology with subsequent treatment reduces the risk of recurrences. In light of this observation, better guideline adherence is advised, i.e. a repeat TUS, if necessary followed by either EUS or MRCP in all patients after a first unexplained acute pancreatitis attack.
Supplemental Material
UEG890462 Supplemetal Material - Supplemental material for The diagnostic work-up and outcomes of ‘presumed’ idiopathic acute pancreatitis: A post-hoc analysis of a multicentre observational cohort
Supplemental material, UEG890462 Supplemetal Material for The diagnostic work-up and outcomes of ‘presumed’ idiopathic acute pancreatitis: A post-hoc analysis of a multicentre observational cohort by Nora D Hallensleben, Devica S Umans, Stefan AW Bouwense, Robert C Verdonk, Tessa EH Romkens, Ben J Witteman, Matthijs P Schwartz, Marcel B Spanier, Robert Laheij, Hjalmar C van Santvoort, Marc G Besselink, Jeanin E van Hooft, Marco J Bruno and for the Dutch Pancreatitis Study Group: the Saint-Antoine IBD network in United European Gastroenterology Journal
Footnotes
Declaration of conflicting interests
None declared.
Ethics approval
This study complies with the Declaration of Helsinki on research ethics, and the protocol was approved by all participating hospitals.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Informed consent
All participants in this study provided informed consent.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.