
Abstract
Background
Biliary dilatation in the asymptomatic patient is a frequent incidental finding in the work-up for which there are no current guidelines.
Objectives
The purpose of this study was to determine the yield of magnetic resonance cholangiopancreatography (MRCP) in asymptomatic patients with an incidental finding of biliary duct dilatation.
Methods
The study included 68 consecutive patients for evaluation of biliary duct dilatation found incidentally on computed tomography (CT) or ultrasound (US). MRCP scans were reviewed, and data were retrospectively collected on demographics and laboratory work-up. Patients were divided by the presence of a significant or non-significant MRCP findings explaining the biliary duct dilatation and compared for normal or abnormal liver function.
Results
Liver function was normal in 47 patients and abnormal in 21 patients. MRCP identified the cause of the bile duct dilatation in 41 patients (60.3%). Rates of insignificant causes were 51% in the normal-liver-function group and 7% in the abnormal-function group. Corresponding rates of significant causes were 27.7% and 61.9% (p = 0.007).
Conclusions
MRCP is a valuable tool in the work-up of biliary duct dilatation. Although significantly more significant causes of bile dilatation are identified in patients with abnormal liver function, almost one-third of patients with normal liver function need further work-up. This has important implications for establishing criteria for the use of MRCP in asymptomatic patients with biliary dilatation.
Keywords
Introduction
Biliary dilatation is a frequent incidental finding in clinical practice. An individual approach is needed to distinguish significant pathological changes from benign anatomical variations, with consideration of the patient’s age and background, clinical symptoms, and results of laboratory tests and imaging studies.1–8 Endoscopic retrograde cholangiopancreatography (ERCP) is no longer considered the standard modality for the routine investigation of biliary duct dilatation owing to its potential complications. According to the guidelines of the American Society for Gastrointestinal Endoscopy (ASGE), ERCP should be reserved for patients at high risk for choledocholithiasis (elevated bilirubin and liver enzyme levels), with the application of other, noninvasive, techniques for patients at low-intermediate risk. Regarding other biliary and pancreatic diseases, the ASGE recommends that diagnostic ERCP be undertaken for the evaluation of pancreaticobiliary pain only in the presence of objective findings on other imaging modalities. However, the preferred modality has yet to be determined.9,10
There are no specific guidelines for the management of asymptomatic biliary duct dilatation. Previous research in patients with normal liver function tests and no biliary colic pain found a low yield for further examination by endoscopic ultrasound (EUS). 11
The present study was designed to evaluate the yield of magnetic resonance cholangiopancreatography (MRCP) for the investigation of biliary dilatation in asymptomatic patients. We focused on the likelihood of finding a significant pathology in this low-risk subgroup of patients and the clinical implications of this probability.
Materials and methods
The sample included consecutive patients who underwent MRCP at a tertiary medical center for an indication of biliary duct dilatation on a previous computed tomography (CT) or ultrasound scan (US) between May 2008–February 2011. Patients were identified by review of the hospital’s picture archiving and communications system (PACS). Inclusion criteria were age more than 18 years, no obvious cause of the biliary dilatation demonstrated on previous imaging, and available relevant imaging and biochemical data. The study was approved by the local institutional review board. The need for informed consent was waived owing to its retrospective design.
MRCP technique
All MRCPs were performed on a 1.5T magnetic resonance imaging (MRI) machine (Phillips Intera Release 2.6, Phillips Healthcare, Best, The Netherlands) using a torso phased array coil. No oral or contrast agents were administered. Twelve thick slabs (40 mm sections) equally angulated at the sagittal and coronal planes were obtained during breath hold. A fat-suppressed single shot turbo spin/echo (TSE) sequence was used. Scan parameters were repetition time/echo time (TR/TE) 8000/800 ms, field of view (FOV) 300 mm, and in-plane resolution (frequency × phase) 0.94 mm × 1.17 mm. In addition, a three-dimensional navigator respiratory-gated sequence was acquired using a half Fourier fat-suppressed TSE sequence, with a slice thickness of 3.0/–1.5 mm, TR/TE 1279/650 ms, turbo factor 126, and in-plane resolution 1.13 mm × 1.49 mm for a scan time of 1:13 min. Maximum intensity projection (MIP) images were reconstructed on the console and sent to the PACS. Single-shot TSE T2-weighted axial images of the liver were also included. Scan parameters were TE 80 ms, slice width/gap 7.0 mm/1 mm, and SENSE 2, with an in-plane resolution of 1.47 mm × 1.80 mm.
Data collection
Reports of the initial imaging examinations (US, CT, or both) and the MRCP examinations were collected from the institutional radiology information system (RIS). All MRCP scans were read by an abdominal imager with 15 years' experience in MRCP interpretation.
The institutional RIS also served as the source for patient demographic and clinical data, as follows: age, sex, and clinical history relevant to the hepatic, biliary and pancreatic organs preceding or following the MRCP examination. The latter included surgical, histopathological and imaging (ERCP, EUS) reports, hospitalization letters, and laboratory markers of malignancy (Carcinoembryonic Antigen, Cancer Antigen 19-9 tumor marker).
Biochemical data were collected from the medical records. liver function tests included aspartate aminotransferase (AST), alanine aminotransferase (ALT), gamma-glutamyltransferase (GGT), alkaline phosphatase (ALP), total bilirubin, and direct bilirubin.
Classification of MRCP results
MRCP findings that explained biliary dilatation were classified as significant or insignificant in terms of warranting further workup. Findings were considered significant if they prompted further investigation (e.g. additional imaging or biopsy of a suspected space-occupying lesion) or treatment (e.g. stone removal on ERCP), and insignificant if they indicated a benign pathology that did not require further management (e.g. periampullary diverticulum slightly compressing the distal common bile duct).
Confirmation of MRCP diagnosis
In cases in which MCRP failed to indicate a cause for the biliary dilatation or the findings were considered insignificant, the diagnosis was confirmed by the absence of evidence of malignancy in the liver, bile ducts, or pancreas during the follow-up period in addition to at least one of the following:
Follow-up US, CT, or MRCP scan demonstrating normal width of the bile ducts. Normal liver function test results on follow-up. Normal findings on EUS or ERCP (performed for various reasons in some patients, although not indicated by the MRCP findings).
When MRCP indicated a cause for the biliary dilatation or the findings were considered significant, the diagnosis was confirmed, as follows:
Choledocholithiasis: by ERCP. Space-occupying lesion: by ERCP or EUS or surgery and justified tissue biopsy or brush cytology (regardless of whether the result was positive, negative or unknown) or diagnosis of malignancy made in another institute. Cholecystitis and/or cholangitis: by cholecystostomy (PTC). Biliary congenital cyst: by surgery and histopathological study. Ischemia and cirrhosis: by later imaging studies showing stable disease while awaiting liver transplantation.
When the classification or confirmation of the MRCP results was unclear, a discussion was held among all four authors (two gastroenterologists and two radiologists), and a consensus was reached.
MRCP as diagnostic tool for biliary dilatation
The study patients were divided into two groups by the presence of a significant (requiring further evaluation/treatment) or insignificant (not requiring further evaluation/treatment) finding on MRCP and compared for normal or abnormal liver function, defined respectively as a value less or more than 1.5 times the upper normal limit for any relevant biochemical parameter. This range was selected to avoid borderline elevations.
Statistical analysis
Data were analyzed with the SPSS version 21 (SSPS Inc., Chicago, Illinois, USA). Continuous variables are presented as mean ± standard deviation (SD) and categorical values as percentages. Categorical variables were compared between groups with chi-squared test. Pathological findings were compared between groups with Fisher’s exact test or t-test. Results were considered statistically significant at p < 0.05.
Results
Study cohort
During the study period, 83 MRCPs were performed in 81 patients for the evaluation of dilated bile ducts. Thirteen patients were excluded from the study: three because the initial imaging findings already suggested a cause of the biliary dilatation, and MRCP was performed only to confirm the diagnosis, and 10 because their available data were limited. In the two patients who underwent MRCP twice, only the findings on the first examination were included in the analysis (Figure 1).
Flow diagram describing study population.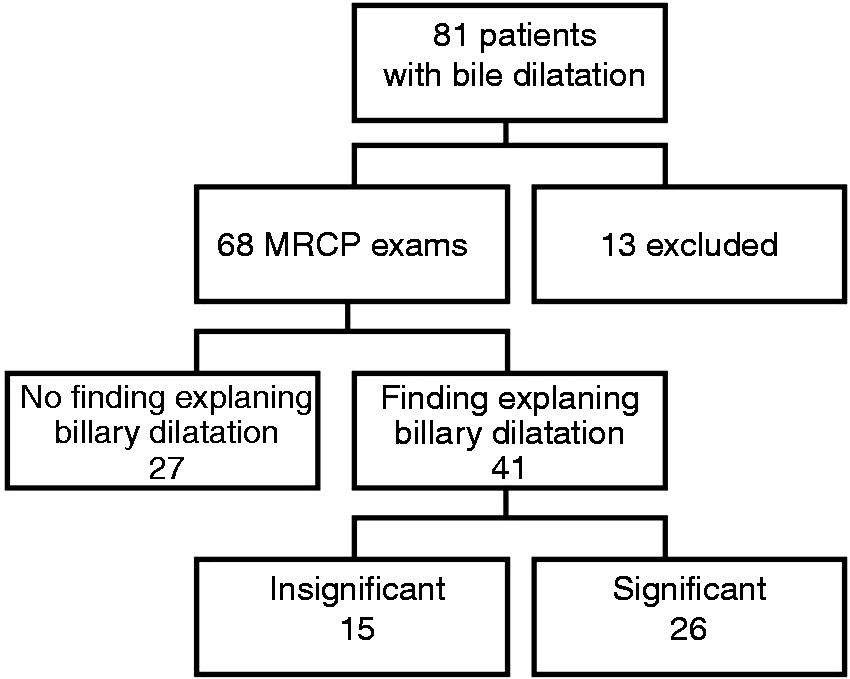
Thus, the final study sample consisted of 68 patients, 53 female and 15 male, of mean age 65 ± 15 years (range 25–98). Twenty-eight patients had initially undergone CT, 26 US, and 14 both CT and US. Liver function was normal (<1.5 times the upper normal limit for any biochemical parameter) in 47 patients (69.1%), considered to be at low clinical risk for biliary pathology and elevated in 21 patients (30.9%), considered to be at intermediate-high clinical risk for biliary pathology.
MRCP findings
Biliary duct dilatation was demonstrated in 53 of 68 MRCP examinations: extrahepatic in 10, intrahepatic in eight, and both intrahepatic and extrahepatic in 35. The remaining 15 MRCP scans (21.2% of patients with normal liver function, 23.8% of patients with abnormal liver function) showed no dilatation, but the patients were not excluded from the study, as it was designed to investigate all patients with unexplained biliary dilatation seen on US or CT. In seven of these 15 patients, a pathology that could have caused intermittent obstruction of varying degrees was identified, possibly explaining the biliary dilatation found by the previous imaging modality (US/CT). Three of the pathologies were significant (distal filling defect of the common bile duct (CBD), cholecystitis mildly compressing the CBD, and Mirizzi syndrome due to a stone in a cystic duct stump), and four were insignificant (proximal CBD stricture, hepatic artery compressing the CBD, tiny filling defect in distal CBD, diameter discrepancy in a biliary anastomosis of a transplanted liver). No finding that could explain the biliary duct dilatation was found in the remaining eight cases.
Pathological findings on 41 magnetic resonance cholangiopancreatographies (MRCPs) defined according to significance. a
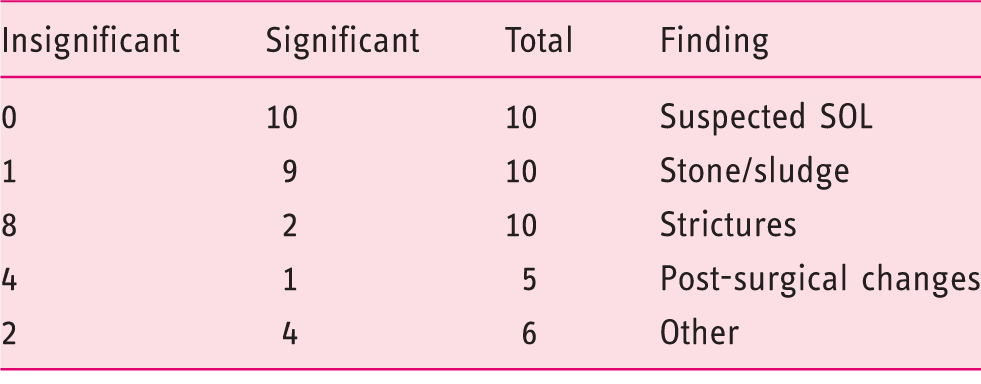
SOL: space-occupying lesion.
Requiring further evaluation (significant) or not (insignificant).
Clinical follow-up
The follow-up period for patients with no (n = 27) or insignificant (n = 15) biliary pathology ranged from 26–56 months (mean = 40). None had evidence of hepatobiliary or pancreatic malignancy or other significant biliary pathologies at any point during follow-up. Of the 26 patients with significant pathology, the diagnosis was confirmed in 23 (88.5%) according to the criteria described in the Methods section. Two of the remaining patients were lost to follow-up and one was misdiagnosed by MRCP with dilatation of the CBD and main pancreatic duct, the “double duct sign” indicative of a space-occupying lesion. Nevertheless, there was no documentation of further workup over a 48-month follow-up period, at the end of which the patient was alive with no evidence of malignancy and normal liver function. Retrospective revision of his MRCP scan revealed a duodenal diverticulum compressing the CBD. Overall, in the whole cohort, the MRCP findings were verified in 65 of the 68 patients (95.5%).
Comparison between groups
Magnetic resonance cholangiopancreatography (MRCP) findings in patients with biliary duct dilatation and normal or abnormal liver function. a
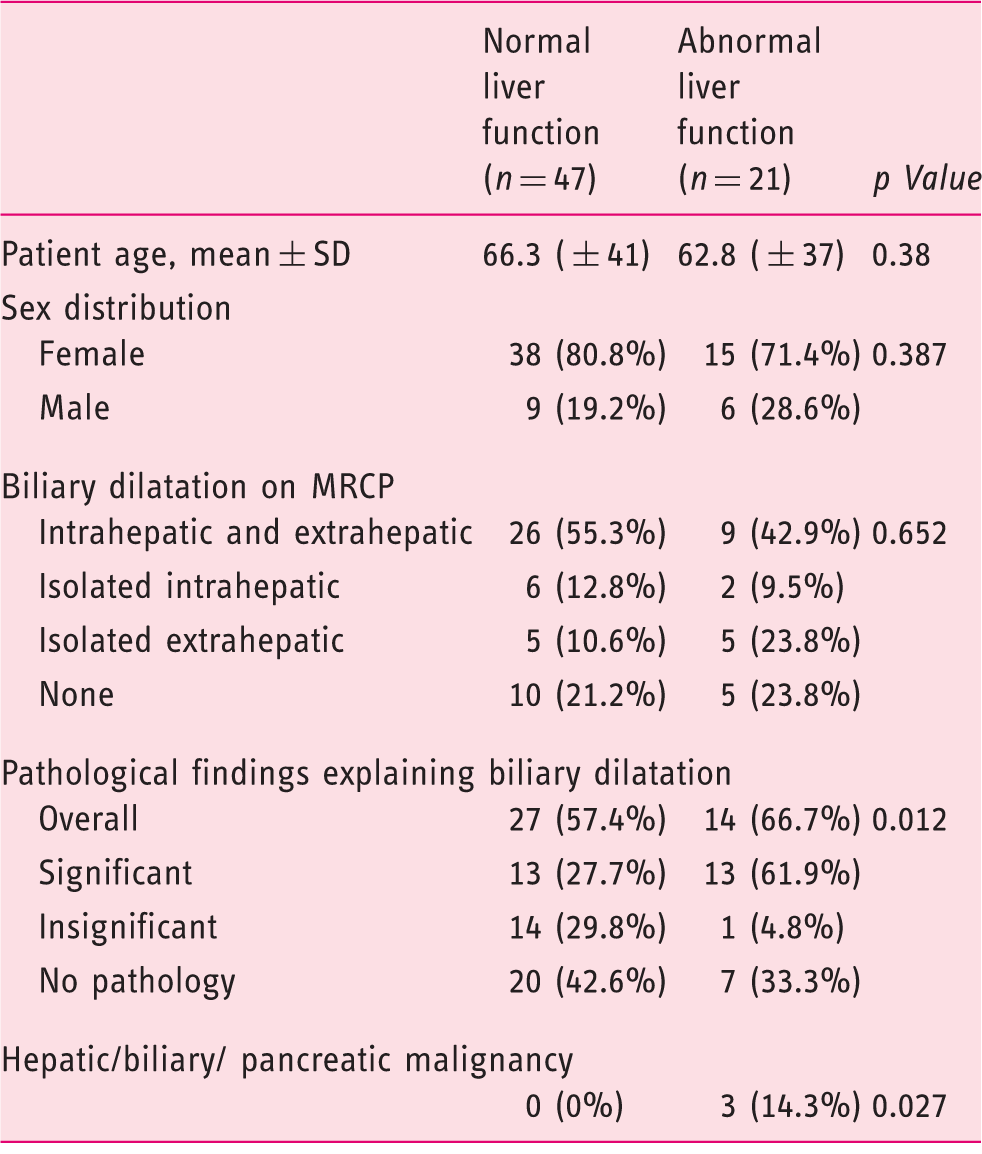
SD: standard deviation.
All values are n (%) unless otherwise indicated.
Defined respectively as a value less or more than 1.5 times the upper normal limit for any relevant biochemical parameter.
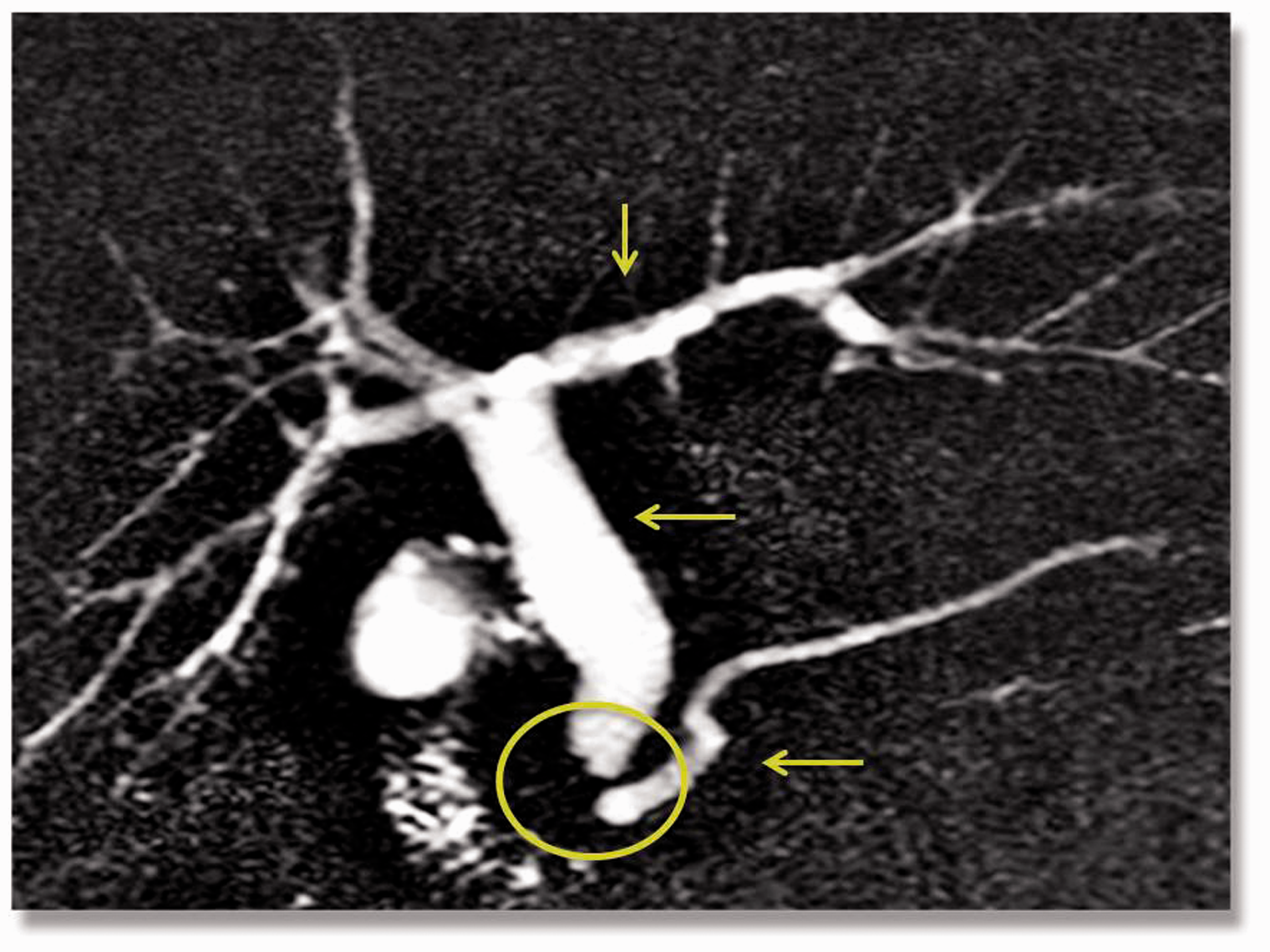
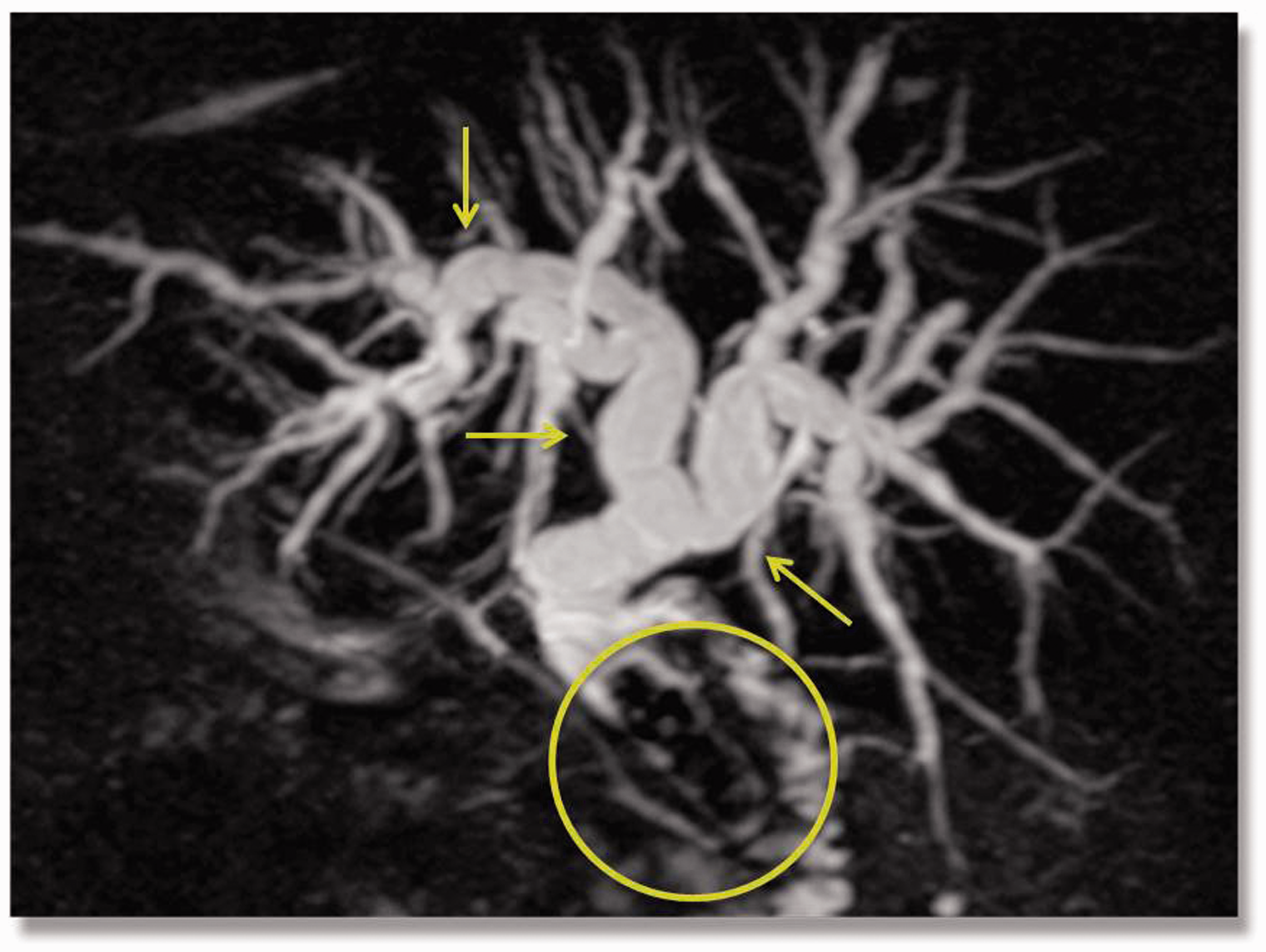
The rate of findings explaining the biliary dilatation was similar in the two groups (57.4% and 66.7%, respectively, p = 0.473). The rate of significant findings was significantly higher in the patients with abnormal liver function than in the patients with normal liver function (13/21, 61.9% vs 13/47, 27.7%, p = 0.007). Representative significant imaging findings in the patients with normal liver function are shown in Figures 2–4. The three patients ultimately diagnosed with a malignancy (all of pancreatic origin) had elevated liver function values (p = 0.027).
Significant finding in a 61-year-old man with normal liver function. Magnetic resonance cholangiopancreatography (MRCP)-3D reconstruction demonstrates severe dilatation of the intrahepatic bile ducts in the left lobe with a filling defect at the level of the hepatic bifurcation, possibly indicative of a space-occupying lesion or stone. The patient underwent surgery where a mass of stones and fibrosis was found in this location. Significant finding in an 83-year-old woman with normal liver function. Magnetic resonance cholangiopancreatography (MRCP)-maximum intensity projection (MIP) reconstruction demonstrates severe dilatation of the common bile duct (CBD) with a distal irregular cut-off and minimal dilatation of the main pancreatic duct, possibly indicative of a space-occupying lesion. Endoscopic ultrasound (EUS) revealed asymmetric thickening of the distal CBD. No malignancy was found on endoscopic retrograde cholangiopancreatography (ERCP) papillotomy and biopsy. Significant finding in a 71-year-old woman with normal liver function. Magnetic resonance cholangiopancreatography (MRCP)-maximum intensity projection (MIP) reconstruction demonstrates severe dilatation of the intrahepatic and extrahepatic bile ducts with a large filling defect in the distal common bile duct (CBD) consistent with a large obstructing stone. The diagnosis was confirmed by endoscopic retrograde cholangiopancreatography (ERCP).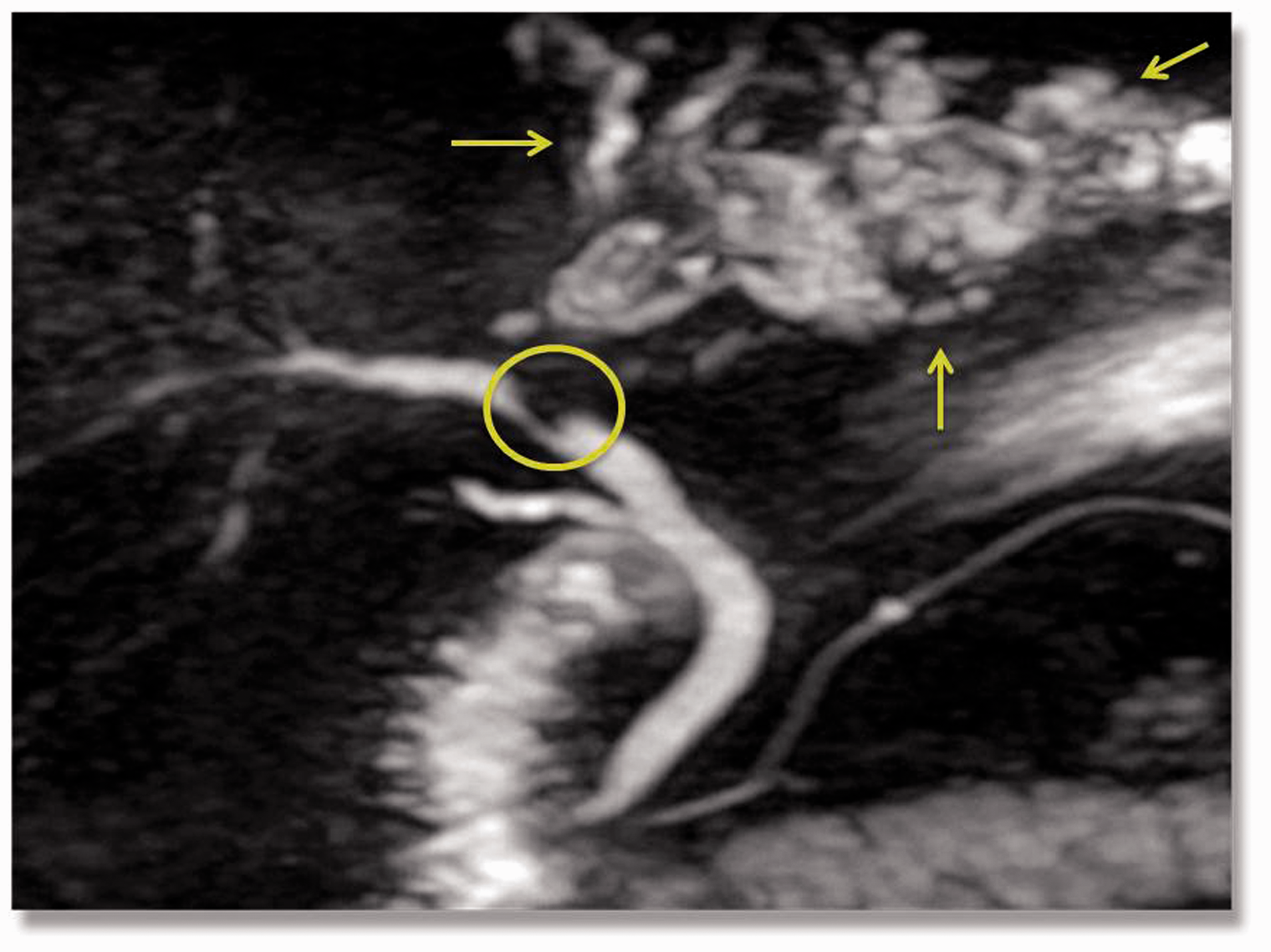
The rate of insignificant findings explaining the biliary dilatation was considerably higher in the patients with normal liver function than in the patients with abnormal liver function (14/21, 51% vs 1/47, 7%). The sole patient with abnormal liver function and an insignificant MRCP finding had previously undergone a Whipple procedure. His MRCP scan showed an irregularity in the choledochojejunostomy which was interpreted as a benign post-surgical change, and no further work-up was recommended.
Validation of findings
To validate the findings, we repeated the analysis with a new definition of abnormal liver function as a value 1.2 times the upper normal limit for any biochemical parameter. This increased the abnormal-liver-function group to 28 patients and decreased the normal-liver-function group to 40 patients. The rate of clinically significant findings explaining the biliary duct dilatation was considerably higher in the patients with abnormal liver function (57.1% vs 25.0%, p = 0.004). All three patients ultimately diagnosed with a malignancy were still included in the abnormal-elevated-liver-function group.
Discussion
MRCP is an important tool in for the investigation of biliary dilatation. It is noninvasive, does not utilize ionizing radiation, and visualizes the bile ducts proximal to the obstruction as well as the extrabiliary structures. Its disadvantages include a lack of functional information, technical artifacts, and relatively low resolution. 12 According to a recent meta-analysis, MRCP has a 95% sensitivity and 97% specificity for the detection of biliary dilatation, 13 comparable to ERCP and EUS and surpassing CT and transabdominal US.14–20 In the presence of a dilated CBD, MRCP has 90–95% compatibility with ERCP in diagnosing stones larger than 4 mm.21–23 Like ERCP, it identifies the location and degree of extrahepatic biliary stenosis with a sensitivity of 91–100%.23,24 MRCP has been found to have a positive predictive value (PPV) of 93% and a negative predictive value (NPV) of 94% for malignant causes of biliary obstruction, and a PPV and NPV of 86% and 98%, respectively, for benign causes.16,17,19
The present retrospective study was designed to evaluate the yield of MRCP in the investigation of biliary duct dilatation in asymptomatic patients. MRCP provided an explanation for the dilatation in 57.4% of cases. Importantly, it identified a significant cause that required further evaluation and/or treatment in 27.7%. No cases of malignancy were found in patients with normal liver function as opposed to three cases among 21 patients with elevated liver parameters (0% vs. 14.3%, p = 0.027).
Malik et al. 11 reported a low yield of EUS for the evaluation of biliary duct dilatation in patients with normal enzyme levels in whom the incidence of clinically significant pathologies was 6% compared to 53% for patients with elevated levels. In the present study, the rate was also lower in the patients with normal than with abnormal liver function (27.7% vs 61.9%), but the disparity was smaller. This difference between the studies is mostly attributable to the higher incidence of significant pathologies in our normal-liver-function group, at least partly owing to our inclusion also of patients with isolated intrahepatic dilatation whereas Malik et al. 11 limited their population to patients with CBD dilatation. We found that the rate of significant findings was higher in the subgroup of patients with isolated intrahepatic dilatation and normal liver function (3/6, 50%) than in the total patients with normal liver function (13/47, 27.7%), thereby raising the overall incidence of significant pathology in the normal-liver-function group.
In our study, 15 patients had pathologies that explained the biliary dilatation, but they were considered insignificant because they did not mandate further evaluation or treatment. This subgroup included eight patients with apparently benign mild to moderate strictures and three patients after liver transplantation with a kink, stricture, or diameter discrepancy at the biliary anastomoses. None had evidence of malignancy or other significant hepatobiliary pathology during follow-up.
MCRP failed to identify a cause for the biliary dilatation in 42.6% of the patients with normal liver function. No malignancy or other biliary pathology was detected in this subgroup during follow-up. A partial explanation for this finding may be the average patient age (66.3 years) and rate of status/post-cholecystectomy (27.7%), both higher than in the general population.
In 15 patients, the biliary dilatation seen on CT or US scan was not seen on subsequent MRCP. The rate of this discrepancy was similar in the normal- and abnormal-liver-function groups (21.2% and 23.8%, respectively; p = 0.652). Interobserver variance (in the definition of normal CBD width and in location of the measurement) and intermodality variance (in biliary width) may explain the between-modality difference in cases of mild dilatation. Change over time may explain some of the other cases, such as an impacting stone that passes through the ampulla during the interval from US/CT to MRCP or an anatomic variant (hepatic artery crossing the CBD, periampullary duodenal diverticula) that causes slight, intermittent compression on the CBD.
According to our predefined study criteria, there were no false-negative results. Patients who did not have a significant pathology on MRCP were followed from 26–56 months, and none had evidence of malignancy or other hepatobiliary or pancreatic disease. There was only one false-positive. These findings are compatible with the reports of high sensitivity and specificity of MRCP in the diagnosis of obstructing pathologies, including stones, benign strictures, and malignant strictures.16,17,23,24
This study has several limitations. The single-center, retrospective design may have harbored an inherent bias. Furthermore, the interval between the laboratory tests and imaging study was varied, and the laboratory tests were done in various institutions. Partial standardization was achieved by recording the results as a percentage from the upper normal limit set by the laboratory in which the particular tests were done.
In conclusion, MRCP successfully detects significant causes of biliary duct dilatation in a higher-than-expected number of patients with normal liver function tests. Although twice as many significant causes are identified in patients with abnormal liver function, almost one-third of patients with normal liver function are also at risk. This has important implications for the establishment of appropriate criteria for the use of MRCP in asymptomatic patients with biliary duct dilatation. The findings should be further verified in prospective studies.
Footnotes
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.