
Abstract
Background and aim
The safety of endoscopic resection of large colorectal lesions (LCLs) (≥20 mm) is clinically relevant. The aim of the present study was to assess the rate of post-resection adverse events (AEs) in a real-life setting.
Patients and methods
In a prospective, multicentre, observational study, data from consecutive resections of LCLs over a 6-month period were collected in 24 centres. Patients were followed up at 15 days from resection for AEs. The primary endpoint was intra-procedural bleeding according to lesion morphology. Secondary endpoints were delayed bleeding and perforation. Patient and polyp characteristics, and polypectomy techniques were analysed with respect to the bleeding events.
Results
In total, 1504 patients (female/male: 633/871, mean age, 66.1) with 1648 LCLs (29.1% pedunculated and 70.9% non-pedunculated lesions) were included. Overall, 168 (11.2%) patients had post-resection bleeding (8.5 and 2.0% immediate and delayed, respectively), while 15 (1.0%) cases of perforation occurred. Independent predictors of immediate bleeding for pedunculated lesions were bleeding prophylaxis (odds ratio (OR) 0.28, 95% confidence interval (CI) 0.13–0.62), simple polypectomy (versus endoscopic mucosal resection, OR 0.38, 95% CI 0.17–0.88) and inpatient setting (OR 2.21, 95% CI 1.07–5.08), while bleeding prophylaxis (OR 0.37, 95% CI 0.30–0.98), academic setting (OR 0.27, 95% CI 0.12–0.54) and size (OR 1.03, 95% CI 1.00–1.05) were predictors for those non-pedunculated. Indication for colonoscopy (screening versus diagnostic (OR 0.33, 95% CI 0.12–0.86)), antithrombotic therapy (OR 3.12, 95% CI 1.54–6.39) and size (OR 2.34, 95% CI 1.12–4.87) independently predicted delayed bleeding.
Conclusions
A low rate of post-resection AEs was observed in a real-life setting, reassuring as to the safety of endoscopic resection of ≥2 cm colorectal lesions. Bleeding prophylaxis reduced the intra-procedural bleeding risk, while antithrombotic therapy increased delayed bleeding.
CLINICALTRIAL: (NCT02694120).
Key summary
Established knowledge
Endoscopic resection of colonic superficial neoplastic lesions decreases the incidence and mortality from colorectal cancer (CRC). Data from referral centres have indicated excellent safety performance even for resection of large lesions.
Findings
The risk of intra-procedural and delayed bleeding, as well as of perforation, after resection of LCLs is low in a real-life setting. Safety performance of endoscopic resection of LCLs coming from referral centres appears reproducible in the real-life setting.
Introduction
Endoscopic resection of superficial neoplastic lesions of the colon decreases the incidence and mortality from CRC.1–3 Implementation of CRC screening programmes in several countries has increased the detection of large colorectal lesions (LCLs) suitable for endoscopic management, with a prevalence ranging from 1–5.5%.4,5
While resection of LCLs is the main driver of CRC incidence prevention, it has been associated with a clinically relevant risk of adverse events (AEs), i.e. bleeding and perforation, observed in 9.2% of endoscopic mucosal resections (EMRs) of laterally spreading tumours (LSTs), as reported in a recent systematic review and meta-analysis. 6 However, most of the available series come from tertiary centres and primarily focus on non-pedunculated lesions, leaving uncertainty on the generalizability of such data.7–12 In addition, the role of patient- and polyp-related risk factors in the risk stratification of LCL-related AEs has only been scantly addressed.
Recent clinical guidelines13,14 have provided specific guidance and recommendation for the management of LCLs in order to reduce the risk of post-resection AEs. Specifically, the use of bleeding prophylaxis has been recommended for pedunculated polyps with head ≥20 or stalk ≥10 mm, and is not recommended for sessile polyps except those with high risk, i.e. those receiving antithrombotic drugs.
The aim of this study was to assess the rate of AEs after endoscopic resection of LCLs in a real-life setting, and to evaluate predictors for immediate and delayed bleeding according to pedunculated or non-pedunculated morphology
Methods
Study design
Over a 6-month period, data on consecutive endoscopic resections of LCLs performed in adult subjects from 24 endoscopy practices with the participation of 71 endoscopists were prospectively collected by means of a web-based dedicated case report form (Study on ComplicAtions of Large Polypectomy [SCALP] study). During the study period, all patients who underwent a colonoscopy for any indication were asked to sign a specific consent form before the procedure. Subjects unable to provide informed consent, and those with a prior removal attempt or recurrent lesions were excluded.
A meeting was planned before the beginning of the enrollment, with the purpose of presenting and discussing the study protocol, in order to guarantee the standardization of terminology.
The study was approved by the Valduce Hospital ethical review board (number 2016/2, 2/29/2016). Written informed consent was obtained from each patient included in the study. The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a priori approval by the institution’s human research committee.
AE definition
For the purpose of the study, lesion morphology was described according to the Paris Classification. 15 LSTs, defined as superficial lesions ≥10 mm in diameter that typically extend laterally rather than vertically along the colonic wall, were also classified according to the surface topography (granular or non-granular). AEs were categorized as early when occurring during the resection or before discharge from the endoscopy unit, and delayed when occurring after hospital discharge but within 15 days. Bleeding was intra-procedural if it occurred during the procedure and required endoscopic treatment, and delayed if occurring after discharge from the endoscopy centre and within 15 days, and resulted in admission to hospital, prolongation of an existing hospital stay or another intervention (endoscopic, radiological, surgical). Sidney Classification was used to define perforations. 16 No specific recommendations were given on either patient pre-procedure management (i.e. antithrombotic agent withdrawal) or technical aspects of the resection. No restrictions were provided regarding the endoscopy equipment given. All colonoscopies were carried out according to the common practice of each centre. Early AEs were recorded by the endoscopists, whereas delayed events were collected by searching hospital records and then double-checked by telephone at 15 days.
Study variables
These were patients’ demographics and settings (in- or outpatients), American Society of Anesthesiologists status, colonoscopy indication (screening, surveillance or diagnostic assessment), and the use of antithrombotics and their management before the procedure (interruption or not). For each resected lesion, location, size and morphology were recorded. Techniques for resection included standard polypectomy, EMR, underwater EMR (UEMR) and endoscopic submucosal dissection (ESD). Usage of prophylactic manoeuvres to prevent perforation (submucosal solution injection to lift the lesion) or bleeding, before or after polyp resection (submucosal epinephrine injection, argon plasma coagulation, clips or endo-loops, either alone or in combination), were specified, as well as intra-procedural and delayed AEs, and histology reports.
The study protocol was approved by the local ethics committees and informed consent was obtained from all patients prior to colonoscopy. Only patients undergoing resection of LCLs were included in the analysis.
Statistical analysis
Analyses were performed using R software version 3.3.2 (R Development Core Team, Vienna, Austria, 2011). All p values are two-sided. All p values < 0.05 were considered statistically significant. Continuous variables were expressed as means ± standard deviations (SDs), and discrete data were expressed as numbers and percentages. For the analysis of AEs, we considered as endpoints AEs associated with polypectomy. First, the analysis included the calculation of the (by-patient) rates of colonic perforation, immediate (intra-procedural) and delayed bleeding, and the 95% confidence intervals (CIs). Second, a polyp-based multivariable logistic regression analysis was performed to identify independent risk factors for immediate (intra-procedural) bleeding. The predictors of intra-procedural bleeding were determined on the basis of univariate analysis (Supplemental material – Appendix 1). For the purpose of this analysis, certain variables were collapsed into binary categories. We ran separate models for each group of polyp morphology (i.e. pedunculated and semi-pedunculated versus non-pedunculated lesions). Data were expressed as the odds of being a polyp with immediate bleeding, either for a one-unit increase in the explanatory variable (for variables measured on a continuous scale, such as polyp size or patient age) or for each category relative to the odds of baseline category (for categorical explanatory variables, such as polyp colon location). The basic unit of this analysis was the polyp. Since a patient could have more than one polyp in the data, robust standard errors (using standard estimators of variance 17 ) were used for all regression analyses to account for some non-dependence of the data that came from the same patient.
Finally, a per-patient multinomial regression analysis was performed to explain delayed bleeding versus intra-procedural bleeding versus non-bleeding patients. Where patients had two or more lesions resected in one procedure, one lesion was selected at random for analysis. If the patient developed bleeding and two or more lesions had been resected, the non-bleeding lesion was removed from analysis.
A number of polyp and patient characteristics investigated here may be dependent on each other, such as the modality for polyp removal and polyp size. Strong correlations among variables, described as multicollinearity, may generate misleading results in multivariable regression analyses. We used Pearson’s correlation to identify the degree of correlation between all pairs of the study predictors; it has been observed that correlation coefficients in absolute values >0.90 signify harmful multicollinearity between two variables. Multicollinearity was also checked by using the variance inflation factor (VIF); multicollinearity does not have adverse consequences if VIFs for all predictors are <3. 18
Results
Study population
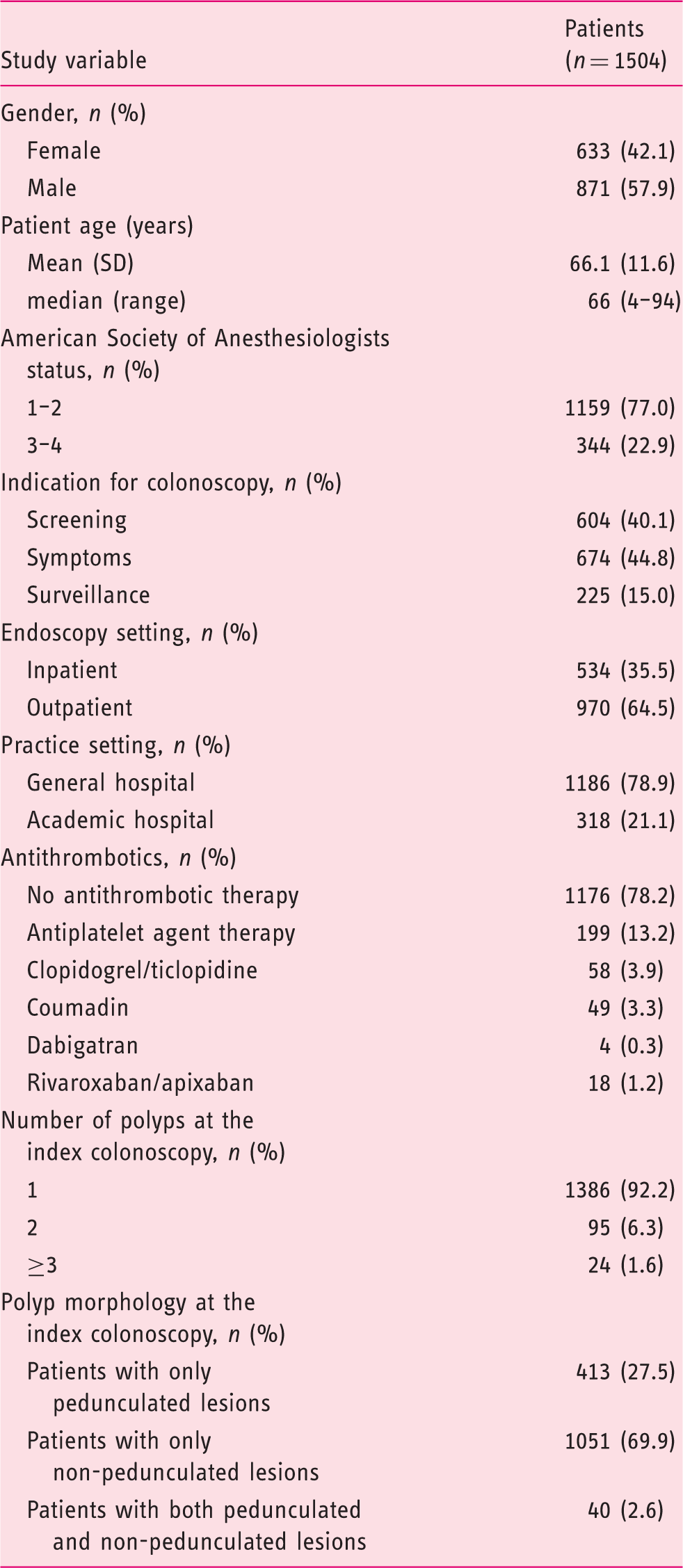
Overall, 1504 (females: 633, 42.1%; mean age: 66.1 ± 11.6 years) patients with a diagnosis of LCLs were included in the 24 study centres, accounting for a total of 1648 LCLs. The average number of ≥2 cm lesions per patient was 1.1 (median = 1, range: 1–4). Of the 1648 lesions, 479 (29.1%) were pedunculated and 1169 (70.9%) non-pedunculated, including 437 (37.4%) sessile lesions and 732 (62.6%) LSTs.
Patient-related factors
Patient characteristics.
Polyp-related factors
Characteristics of polyps at the baseline colonoscopy stratified by polyp morphology (pedunculated versus non-pedunculated, including sessile and laterally spreading tumour morphology).
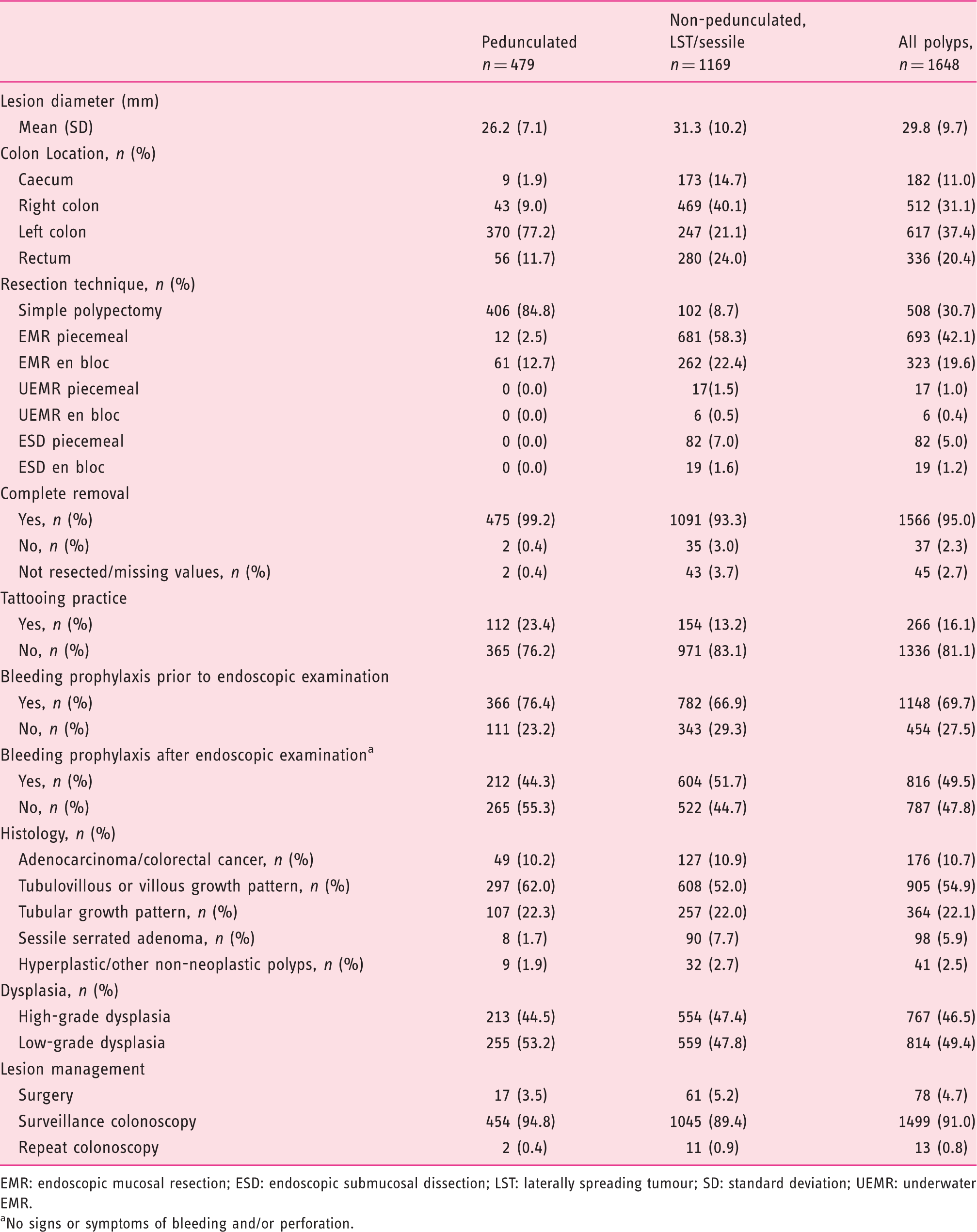
EMR: endoscopic mucosal resection; ESD: endoscopic submucosal dissection; LST: laterally spreading tumour; SD: standard deviation; UEMR: underwater EMR.
No signs or symptoms of bleeding and/or perforation.
Procedure-related factors
In the group of pedunculated lesions, simple standard polypectomy was used in 406/479 (84.6%) polyps and EMR (either en bloc or piecemeal) in 73/479 (15.0%) cases (i.e. semi-pedunculated lesions). Non-pedunculated lesions were resected by standard polypectomy in 102/1169 (8.7%), EMR/UEMR (either en bloc or piecemeal) in 966/1169 (82.7%) and ESD in 101/1169 (8.6%) cases. For pedunculated lesions, pre- or post-resection bleeding prophylaxis was applied in 366/479 (76.4%) and 212/479 (44.3%) cases, respectively; corresponding values for those non-pedunculated were 782/1169 (66.9%) and 604/1169 (51.7%).
Intra-procedural bleeding
Percentage of polyps with intra-procedural bleeding according to study variables and odds ratios (95% confidence intervals). Cluster robust 95% confidence intervals and p values were used for all regression models to account for clustering (i.e. multiple polyps within a patient). Continuous variables were centred around their means.
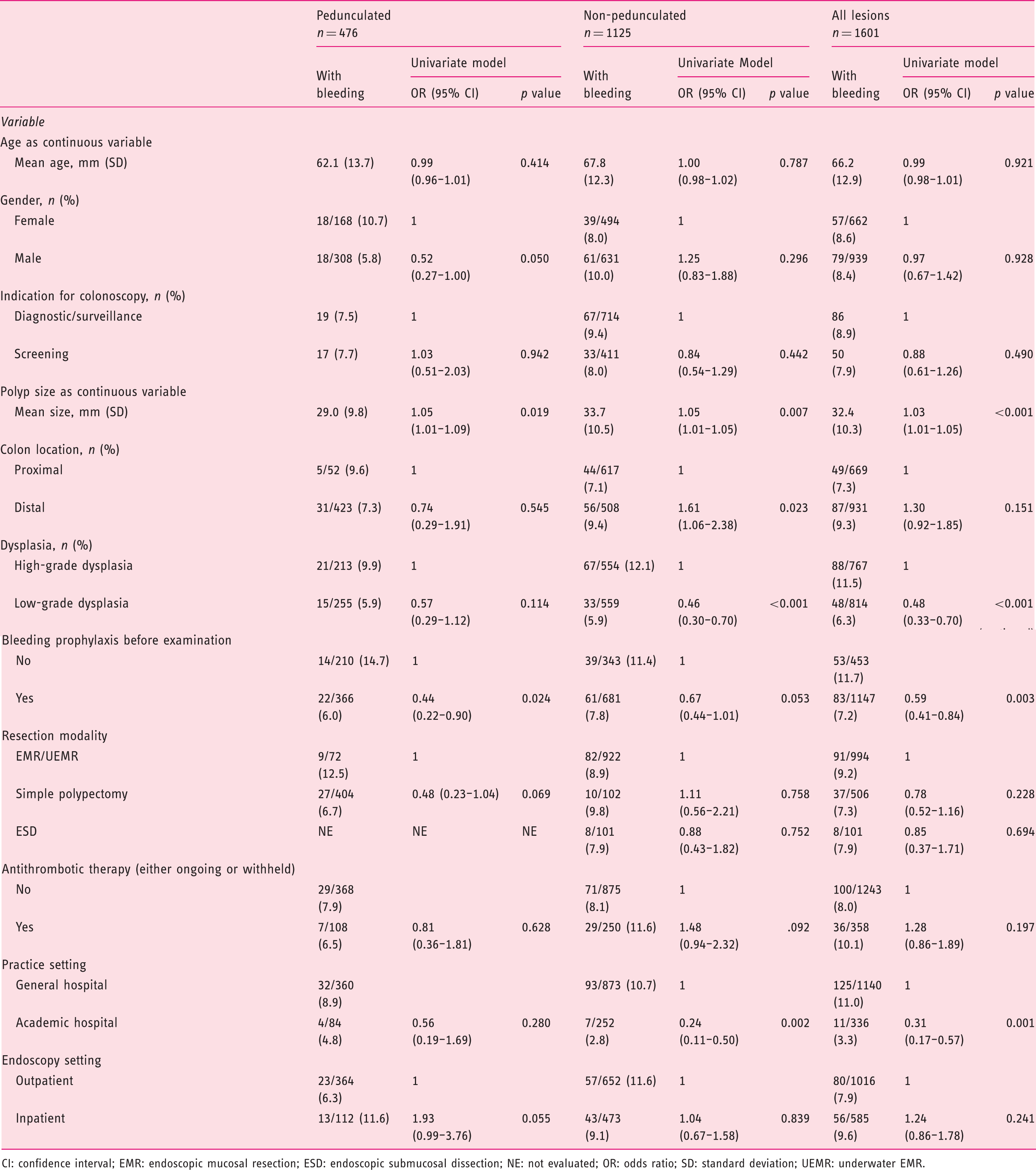
CI: confidence interval; EMR: endoscopic mucosal resection; ESD: endoscopic submucosal dissection; NE: not evaluated; OR: odds ratio; SD: standard deviation; UEMR: underwater EMR.
Pedunculated lesions
Univariate analysis showed significant associations with intra-procedural bleeding for polyp size (odds ratio (OR) 1.05, 95% CI 1.01–1.09) and bleeding prophylaxis before polypectomy (yes versus no: OR 0.44, 95% CI 0.22–0.90). Gender (male versus female: OR 0.52, 95% CI 0.27–1.00), resection mode (standard polypectomy versus EMR: OR 0.48, 95% CI 0.23–1.04) and endoscopy setting (inpatient versus outpatient: OR 1.93, 95% CI 0.99–3.76) were found to be marginally significant (p < 0.100).
Multivariable analysis for intra-procedural bleeding. Separate analyses were performed for pedunculated and non-pedunculated polyps (including sessile and laterally spreading tumours). Cluster robust 95% confidence intervals and p values were used for all regression models to account for clustering (i.e. multiple polyps within a patient). Continuous variables were centred around their means.
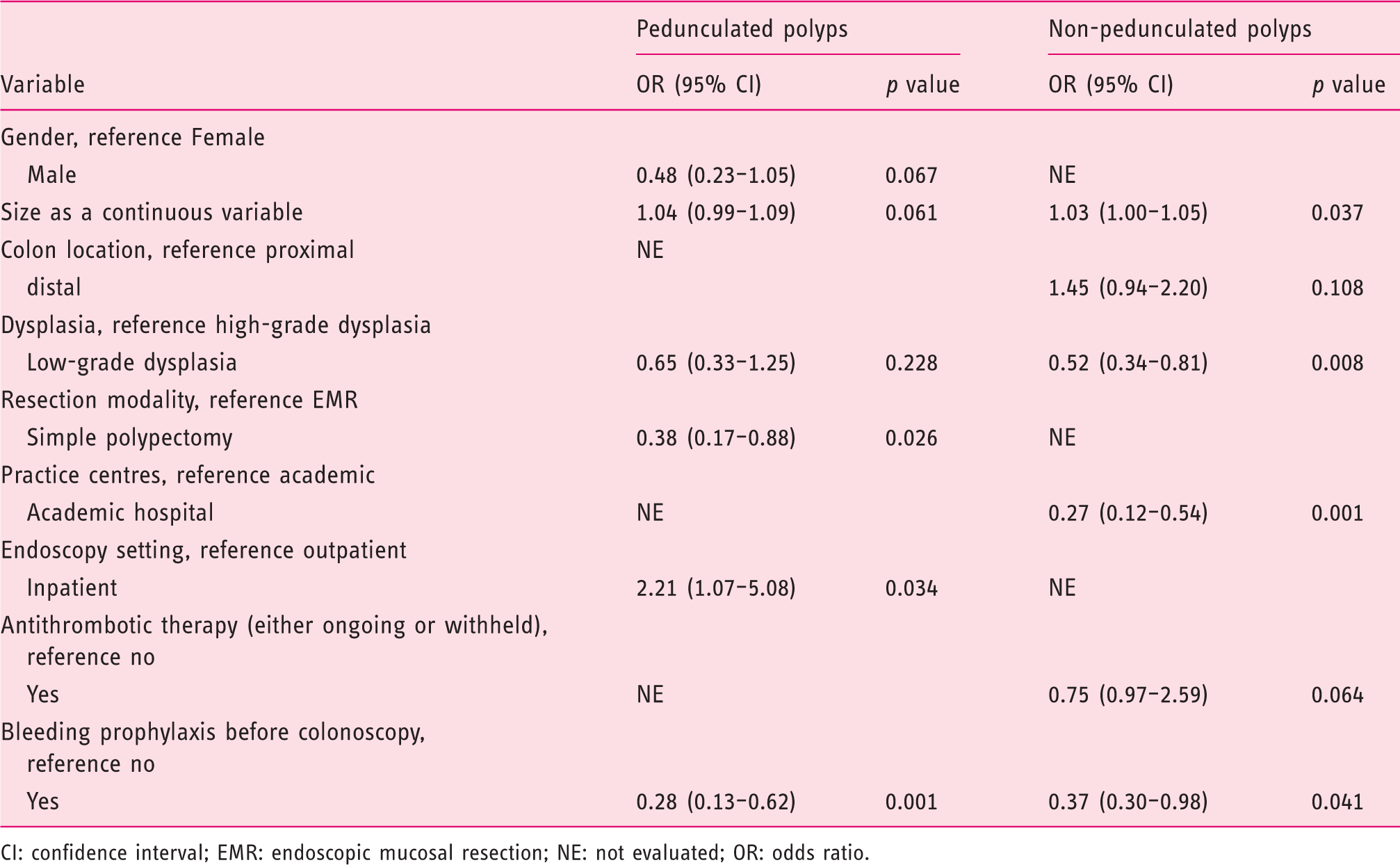
CI: confidence interval; EMR: endoscopic mucosal resection; NE: not evaluated; OR: odds ratio.
Non-pedunculated lesions
At univariate analysis, larger non-pedunculated polyps (ORs 1.03, 95% CI 1.02–1.05) and those located distally (versus proximally: OR 1.61, 95% CI 1.06–2.45) were associated with a greater risk of intra-procedural bleeding, while non-pedunculated lesions showing low-grade dysplasia (versus high-grade dysplasia: OR 0.46, 95% CI 0.30–0.70) and those removed at academic centres (versus general hospitals: OR 0.24, 95% CI 0.11–0.50) were associated with a lower bleeding risk. Bleeding prophylaxis (yes versus no: OR 0.67, 95% CI 0.44–1.01, p = 0.053) and antithrombotic therapy (yes versus no: OR 1.48, 95% CI 0.94–2.32, p = 0.092) tended to be associated with bleeding.
At multivariate analysis (Table 4), academic setting (OR 0.27, 95% CI 0.12–0.54, p = 0.001), polyp size (OR 1.03, 95% CI 1.00–1.05, p = 0.037) and bleeding prophylaxis (OR 0.37, 95% CI 0.30–0.98, p = 0.041) were independent predictors for bleeding. A trend approaching significance was found for antithrombotic therapy (p = 0.064). There was no evidence of multicollinearity; VIFs for all predictors were <2.0 (see Supplemental Figure A2/Table A1).
Delayed bleeding
Overall, 31 patients presented with delayed bleeding (23 non-pedunculated and 8 pedunculated). Of them, 11 were on APAs and six on anticoagulants, accounting for bleeding rates of 4.2 and 8.5% in these patient subgroups, respectively. Results from the univariate regression analysis for the total data set of patients (n = 1485) and for the subgroup of patients with LST/sessile lesions (n = 1049) are given in Supplemental Table A3. Patient age (p = 0.088), indication for colonoscopy (p = 0.008), the use of antithrombotic therapy (p < 0.001) and polyp size (p = 0.017) were associated with delayed bleeding.
A patient-level multinomial logistic regression of factors associated with delayed bleeding (reference group) versus non-bleeding patients and versus immediate bleeding. Results from multivariable analysis.
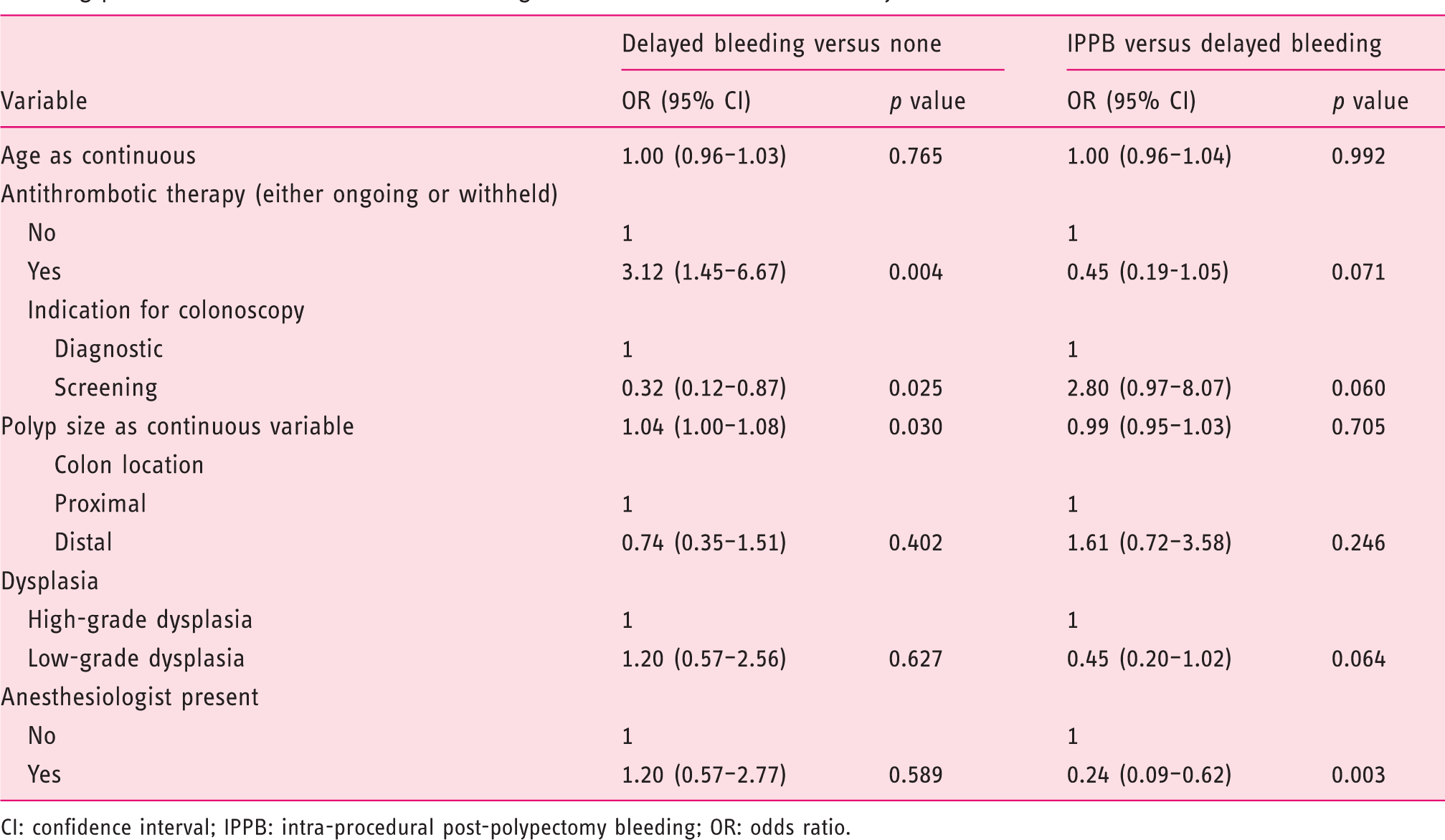
CI: confidence interval; IPPB: intra-procedural post-polypectomy bleeding; OR: odds ratio.
Perforation
Perforation occurred in 15 (1.0%) patients and was diagnosed before discharge in all cases. Overall, 13/15 (86.6%) cases were treated endoscopically (endoclips), whereas 2 (0.13%) needed surgery. In 7/15 cases, the polyp size was ≥50 mm in size. Perforation complicated resection of 1/487 (0.2%) pedunculated lesion, 2/481 (0.4%) sessile ones and 12/682 (1.8) LSTs. As concerns the modality of resection, perforation occurred after standard polypectomy in 1 case (0.2%), EMR in 6 (0.6%) and ESD in 8 (8%) cases.
Discussion
The low risk of intra-procedural and delayed bleeding, as well as of perforation, after resection of ≥2 cm colorectal lesions in a real-life setting reassures regarding its favourable benefit/risk ratio, strengthening its role as first-choice treatment for the management of these lesions. Only 1 out of 10 patients will present with intra-procedural bleeding, while delayed bleeding and perforation are limited to ∼1 out of 50 and 1 out of 100, respectively. In addition, we showed a high efficacy of bleeding prophylaxis for both pedunculated and non-pedunculated LCLs, while confirming the contributing risk of antithrombotic therapy for delayed bleeding.
These data are in line with similar estimates from tertiary centres.7–11 Our 9% risk of post-resection bleeding for non-pedunculated lesions confirms the previous estimate of 11% observed in an Australian prospective multicentre study, 9 which included >1100 patients with large non-pedunculated lesions, and is also comparable with the 5–7% range described in other EMR series.10–12 In addition, most of the patient-/polyp-/procedure-related factors shown to be independent predictors of post-resection bleeding in our study at uni- or multivariate analysis confirm similar outcomes of previous analyses. In particular, the roles of increasing lesion size, antithrombotic use and high-grade dysplasia (univariate) in our study demonstrate the generalizability of these risk factors in previous analyses, supporting the integration of these variables in the risk stratification process in clinical practice.9–12 On the other hand, the 2.0% risk of delayed bleeding observed in our series is markedly lower than the 6% previously reported for non-pedunculated lesions.19–22 However, this may be partly related to a substantial use of bleeding prophylaxis in our series, accounting for >50% of the non-pedunculated cases. Our study also confirmed the very low rate of perforation associated with LCL resection, and especially how most of these AEs are amenable to endoscopic closure. Indeed, the risk of perforation-related surgery in our series was equal to 1 in every 769 resections.
The main technical results of our multivariate analysis were, on one hand, the efficacy of prophylaxis manoeuvres for the prevention of post-resection bleeding, and, on the other hand, the contribution of antithrombotic agents to such risk.
Regarding the former, our data on pedunculated lesions further strengthen the official recommendations to use specific manoeuvres when dealing with large lesions. Of note, in our analysis the efficacy of prophylactic manoeuvres also emerged for non-pedunculated lesions, being statistically significant for intra-procedural bleeding and with a suggestive trend for delayed bleeding. These data confirm the efficacy of coagulation or prophylactic clipping of the resection sites after EMR of large polyps in reducing the risk of post-resection bleeding in a retrospective series, 23 while in disagreement with another study where routine prophylactic endoscopic coagulation of non-bleeding vessels did not decrease the incidence of delayed bleeding. 22 Furthermore, the effectiveness of clipping, even for non-pedunculated lesions, has recently been demonstrated in a randomized controlled trial, especially in the proximal colon. 24 Of note, a recent study 25 showed the possibility of stratifying the risk of post-EMR bleeding according to the presence of visible vessels within the post-resection mucosal defect, opening the door for endoscopic stratification of the bleeding risk in order to orientate the need for prophylactic clipping closure of the EMR defect.
Regarding the latter, the use of antithrombotic therapy was independently associated with the risk of delayed but not intra-procedural bleeding. This risk was substantial, albeit comparable to that reported in other studies,26–28 despite the fact that most patients were managed according to guidelines recommended for peri-endoscopic management of antithrombotics. 29 This indirectly supports the conclusions of a cost-effectiveness study showing that, for polyps >10 mm in size, prophylactic endoscopic clipping was cost-effective for patients receiving APAS or anticoagulant agents. 30
It could be argued that by mixing lesions removed by different techniques (polypectomy, EMR, UEMR and ESD), the types of interventions performed for colorectal polyps become heterogeneous, as each of these procedures has a different bleeding and perforation risk profile (particularly ESD). However, while we are aware of the great differences between resection techniques, this study did not aim to evaluate the safety of one technique over another; instead, we wanted to assess whether the excellent performance of endoscopic resection of the LCLs coming from the referral centres was reproducible in the real-life setting and we think we have been able to prove it. The tertiary centres remain the most suitable places for the treatment of these lesions, but when this is not possible, due to health policy issues or local situations, endoscopic resection appears to also be safe in a community setting if carried out by adequately skilled individuals. Thus, training of skilled operators outside of tertiary centres is mandatory.
Moreover, another criticism that can be made of the study is that it does not bring anything new to the debate on the endoscopic resection of large polyps of the colon. Conversely, we think our study contributes to the understanding of another important issue. It is common experience that over recent years, thanks to the development of skills and techniques, the safety of endoscopic resection even of large lesions in the colon has improved.
Intra-procedural bleeding can be practically removed from the list of AEs, and perforation, which has always been feared and in most cases leads to a need for surgery, has almost always become an endoscopically manageable event. Although it has already been demonstrated in the literature by large studies coming from referral centres, our study demonstrates for the first time the reproducibility of this important result in the real-life setting. Again, due to improvements in safety, another paradigm of the past can be changed, which is the need to admit the patient to be subjected to endoscopic resection. Indeed, our study shows that the setting of resection (inpatients versus outpatients) did not correlate with delayed bleeding for any type of lesion. Thus, this evidence, together with the low risk of delayed bleeding, supports the possibility of avoid hospitalization for the performance of endoscopic resection of large lesions.
Moreover, we think that this issue is relevant to the debate about the correct management of LCLs. In the past, surgical resection was the standard of care for LCL management, but more recently it has been shown that endoscopic removal of LCLs in comparison with surgical resection is associated with higher efficacy31,32 and reduced incidence of complications,33,34 so that guidelines now recommend endoscopic resection of LCLs in the majority of cases. However, surgical colonic resection for non-malignant polyps continues to be performed, even more frequently than in the past, 35 despite the fact that it has been demonstrated that it is associated with a non-negligible major post-operative AE rate, high rates of rehospitalization, second surgery and colostomy, and a still-present risk of mortality. 34 In this context, while data from referral centre have shown that endoscopic resection of LCLs is a safer, cheaper and more resilient alternative to surgery, this large cooperative, nationwide study has the strength to demonstrate that excellent outcomes can be obtained, regardless of the strategies of resection, even outside of tertiary referral centres.
In conclusion, our study confirms the favourable safety profile of endoscopic resection of LCLs in the real-life setting, as well as the prominent role of clinical and technical factors in stratifying or marginalizing risk.
Supplemental Material
UEG874176 Supplemental material - Supplemental material for Intra-procedural and delayed bleeding after resection of large colorectal lesions: The SCALP study
Supplemental material, UEG874176 Supplemental material for Intra-procedural and delayed bleeding after resection of large colorectal lesions: The SCALP study by Arnaldo Amato, Franco Radaelli, Loredana Correale, Emilio Di Giulio, Andrea Buda, Vincenzo Cennamo, Lorenzo Fuccio, Massimo Devani, Ottaviano Tarantino, Giancarla Fiori, Germana De Nucci, Mario De Bellis, Cesare Hassan, Alessandro Repici and on behalf of the Bowell Group in United European Gastroenterology Journal
Footnotes
Acknowledgements
Author contributions: AA, FR, LC, EDG, AB, VC, LF, MD, OT, GF, GDN, MDB, CH and AR: study concept and design, interpretation of results and drafting of the manuscript; AA and LC: acquisition of data and statistical analysis; and all authors: acquisition of data, critical revision of the article for important intellectual content and final approval of the article.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Ethics approval
The study protocol was approved by the local ethics committees of each involved center.
Informed consent
Written, informed consent was obtained from each patient included in the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.