
Abstract
Objective
The purpose of this review is to assess the efficacy and safety of laparo-endoscopic local resections for colorectal lesions not suitable for endoscopic resection.
Summary background data
The combined laparo-endoscopic approach has been proposed for large colorectal lesions unsuitable for endoscopic resection, in order to reduce morbidity of common laparoscopic resection. However, data on the efficacy and safety of laparo-endoscopic local resections are still controversial.
Methods
An Embase search of papers published during the period 1985–2014 was performed. Published studies that evaluated laparo-endoscopic resections for colorectal lesions were assessed using PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analyses) recommendations by two authors. Forest plots on primary (per-lesion rate of further surgery, including surgery for complications and surgery for oncologic radical treatment) and secondary outcomes were produced based on fixed and random effects models. Heterogeneity was assessed using the I2 statistic. Risk for within-study bias was ascertained with QUADAS (Quality Assessment of Diagnostic Accuracy Studies) system.
Results
A total of 11 studies provided data on 707 lesions treated with a combined laparo-endoscopic approach. A variety of techniques were reported. The overall per-lesion rate of further surgery was 9.5%, while per-lesion rate of further surgery for oncologic treatment was 7.9%, per-lesion rate of further surgery for complications treatment was 3.5%, incidence of adenocarcinoma was 10.5%, incidence of overall complications was 7.9%, incidence of conversion to open surgery 4.3% and incidence of recurrence was 5.4%.
Conclusions
Despite laparo-endoscopic approach ensures limited invasiveness, it is affected by a consistent rate of complications and oncologic inadequacy that often requires further surgical treatment.
Introduction
Colorectal cancer (CRC) has a precursor in colorectal adenomas, as identification and removal leads to a significant reduction in CRC incidence and mortality prevention. 1 This has increased CRC screening programmes. Nevertheless, the procedure to remove colorectal polyps represents a major cause of morbidity and mortality.2,3
It has been shown that large polyps >2 cm in diameter are found with a prevalence of 0.8–5.2% in patients undergoing colonoscopy. 4 However, large polyps or those that are difficult to access may require either piece-meal endoscopic mucosal resection (EMR) or endoscopic submucosal dissection (ESD), although these procedures are burdened by technical difficulty and risk of perforation.5–7 For this reason, there are studies reporting of a majority of patients with polyps >2 cm resected surgically, 8 although with the increased expertise in endoscopic techniques the rate of surgically removed polyps lowered till about 15% in more recent years. 9 Nevertheless, surgical treatment for colorectal lesions is associated with a substantial increase in morbidity and mortality when compared with endoscopy, 10 and this is not clinically warranted for benign lesions.
The combined laparo-endoscopic local resections of large colorectal polyps may represent an advantage for these instances. Endoscopy might provide additional safety for the surgeon by precise localisation of the lesion and endoluminal observation of resection and reconstruction and might reduce the invasiveness of the surgical approach. 11 However, most of these studies are retrospective and single-centre studies that included only a relatively small number of cases. When considering the relatively low frequency of recurrences or complications, such small sample sizes prevent reliable estimates of the efficacy and safety of the technique. This is even more burdened by the description of different laparo-endoscopic techniques which can be summarised as follows: (a) endoscopic polypectomy under laparoscopic assistance; (b) endoscopic-assisted laparoscopic wedge resection by mechanical staplers, and/or endoscopic-assisted transluminal resection, meaning a colotomy and polypectomy followed by laparoscopic suture of the colotomy; (c) endoscopic-assisted segmental resection minor than hemicolectomy.
The aim of this systematic review and meta-analysis was to assess the efficacy and safety of combined laparo-endoscopic local resections for colorectal lesions.
Methods
The methods used for the analysis and selection of inclusion criteria were based on PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analyses) recommendations. 12
All studies published between January 1985–December 2014, in which patients underwent laparoscopic-assisted endoscopic removal or endoscopic-assisted laparoscopic removal of colorectal lesions by local or limited excision were reviewed. Extended resections such as large segmental or hemicolectomies, case reports (<10 cases), non-human studies, review articles, position papers, editorials, commentaries and book chapters were excluded from the review. If there was any suspicion of cohort overlap between studies, only the most recent study was considered for inclusion.
A literature search was performed in January 2015. Relevant publications were identified by Embase and PubMed for the period 1985–2014, using the string ‘laparoscopy assisted' AND (‘endoscopy'/exp OR ‘endoscopy') AND (‘polypectomy'/exp OR ‘polypectomy') AND (‘colon'/exp OR ‘colon') OR ‘rectum'/exp OR ‘rectum' AND ((controlled clinical trial)/lim OR (randomized controlled trial)/lim) AND ((article)/lim OR (article in press)/lim OR (conference abstract)/lim) AND (humans)/lim AND (english)/lim AND (1985–2014)/py.
Potential studies were initially screened by two researchers (AA, MMi). Papers were first screened by title, then by abstract, and finally the full paper of all relevant studies was retrieved. The reference lists from identified papers were hand-searched to identify any additional studies.
Data extraction was independently performed by the two reviewers using pre-defined data extraction forms. A third investigator (MMo) arbitrated in the event of any lack of agreement.
QUADAS (Quality Assessment of Diagnostic Accuracy Studies) criteria were used to assess the methodological quality of the included studies and detect potential bias, the following details were noted: (a) whether the reference standard (histological verification) was available, (b) whether data on technical failure were provided and (c) whether data on oncological failure were provided. 13
The primary outcome of this systematic review was the per-lesion rate of further surgery (i.e. including surgery for complications and surgery for oncologic radical treatment). Secondary outcomes were:
incidence of adenocarcinomas per-lesion rate of further surgery for oncologic radical treatment per-patient rate of overall complications per-lesion rate of further surgery for complications treatment per-patient rate of conversion to open surgery per-lesion rate of recurrence.
Attempts were made to contact authors if data presentation was incomplete or if it was necessary to resolve an apparent conflict or inconsistency in the article. However, additional data were only sought regarding the primary outcome.
Per-lesion rate of further surgery was defined as the ratio between the absolute number of laparo-endoscopic resections and the overall number of patients who required further surgery for any reason, including surgery for complications and surgery for oncologic radical treatment. The same methodology was applied to all the secondary outcomes.
Following a conservative approach, all outcomes were analysed by a random-effects model, where the proportions of single studies were used to calculate an overall proportion. This model incorporates heterogeneity among studies and takes into account differences in sample size by which proportions were measured in each study; this within-study variation was accounted for by using the exact binomial distribution. Individual and pooled estimates of these proportions together with 95% confidence intervals (CIs) were presented in the forest plots.
Publication bias was assessed by generating a funnel plot and performing the rank correlation test of funnel plot asymmetry. Heterogeneity was assessed by the I2 measure of inconsistency, statistically significant if I2 > 50%. Potential sources of heterogeneity were explored by two sensitivity analyses: checking the results of cumulative (sequentially including studies by date of publication) and influence analyses (calculating pooled estimates by omitting one study at a time). All analyses were performed using R 3.1.0 package meta (R Foundation for Statistical Computing, Vienna, Austria). 14
Results
Study selection
A flow diagram of this systematic review, with the number of papers retrieved, included and excluded, as well as the reasons for exclusion, is shown in Figure 1. In summary, 3275 studies were identified by the Embase and Pubmed searches and one by searching the reference list of selected papers. After removing non-pertinent papers, 55 abstracts were selected and 11 published papers were included in the systematic review.11,15–24 The reasons for exclusion are given in Figure 1.
Flow-chart of the literature search in this systematic review.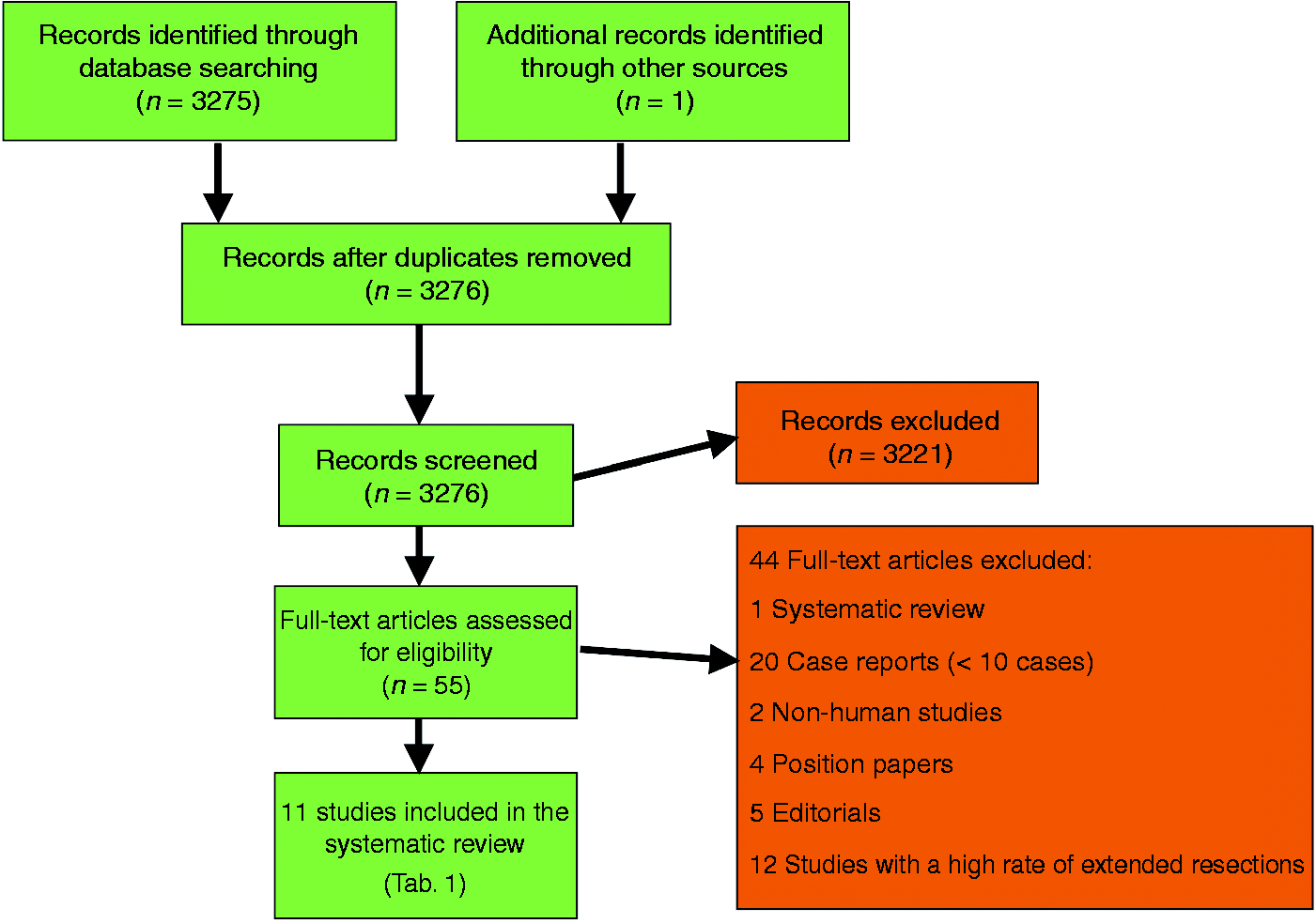
Characteristics of the included studies
Characteristics of the included studies
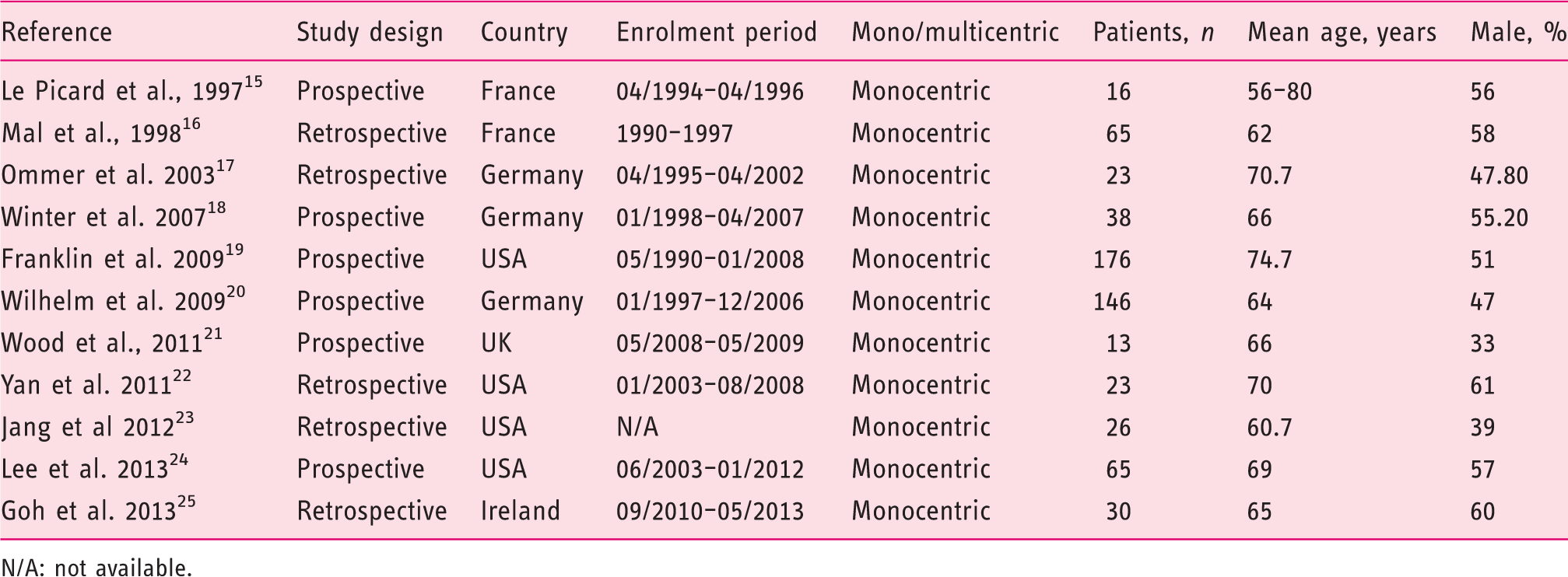
N/A: not available.
A total of 621 patients were enrolled in the selected studies. The number of patients enrolled in each study ranged from 13–176, with a median of 30. The median of the mean ages across the included studies was 66 years (range 62–75 years). The median proportion of male patients was 55% (33–61%).
The clinical indication for laparo-endoscopic resection was benign polyps not removable by an experienced endoscopist in six studies, benign polyps with large size/difficult location/failed polypectomy/recurrence in two studies and both in one study, while in two studies indications were not specified (Table 2). The most represented location was caecum and right colon, with a median of mean rates of 57.8% (26.6–87.5%).
Interventions
A total of 707 lesions were resected by the different laparo-endoscopic techniques (see Supplementary Material, Table 2) which can be summarised as follows: (a) endoscopic polypectomy under laparoscopic assistance; (b) endoscopic-assisted laparoscopic wedge resection by mechanical staplers, and/or endoscopic-assisted transluminal resection, meaning a colotomy and polypectomy followed by laparoscopic suture of the colotomy; (c) endoscopic-assisted segmental resection minor than hemicolectomy.
Outcomes
Conversion to open surgery for technical difficulty or intraoperative complications is reported in only four studies16,18,20,23 in a range of 3.0–7.7% of cases. Postoperative bleeding was reported in only three studies15,20,24 or in six patients only (0.8%). Overall postoperative complications are reported in seven of the 11 studies,15,18–21,23,24 ranging between 4.4–25%. Indeed, complications required surgery in only eight patients, as reported in two studies. The median of the mean lengths of hospital stays reported was 3.0 days (1–8) (see Supplementary Material, Table 3).
Histology demonstrated an adenoma in the vast majority of cases. The median rate of adenomas was 87.5% (76–100%), whereas of carcinomas 11.0% of cases (0–20.0%). Surgery to achieve an oncologic radical treatment was reported in a median of 7.5% of cases (0–17.7%) (see Supplementary Material, Table 4).
Risk of bias assessed in individual studies
Potential risk of bias in individual studies was assessed according to the QUADAS score (see Supplementary Material, Table 5). All but two studies clearly reported the selection criteria.17,18 The spectrum of patients was always representative of the patients’ population in daily practice. The index test (completion of the laparo-endoscopic procedure) and the execution of the reference standard (further surgery) were described in all but three studies which was considered sufficient to permit the analysis.16,18,19 All other items were extensively reported.
Primary outcome
The primary outcome of this systematic review was the per-lesion rate of further surgery, including surgery for complications and surgery for oncologic radical treatment. The per-lesion rate of further surgery estimate was 9.5% (95% CI 6.9–12.9%), showing a low heterogeneity (I2 = 11.2%) and no publication bias (p = 0.183) (Figure 2). Performing a cumulative analysis (adding one study at a time by publication date), the rate estimate varied from 6–13% in the time frame 1997–2007, but was quite stable around 9% after 2009; performing an influential analysis (by omitting one study in turn), the rate estimate was not influenced by any trial.
Forest plot for per-lesion rate of further surgery, including surgery for complications and surgery for oncologic radical treatment.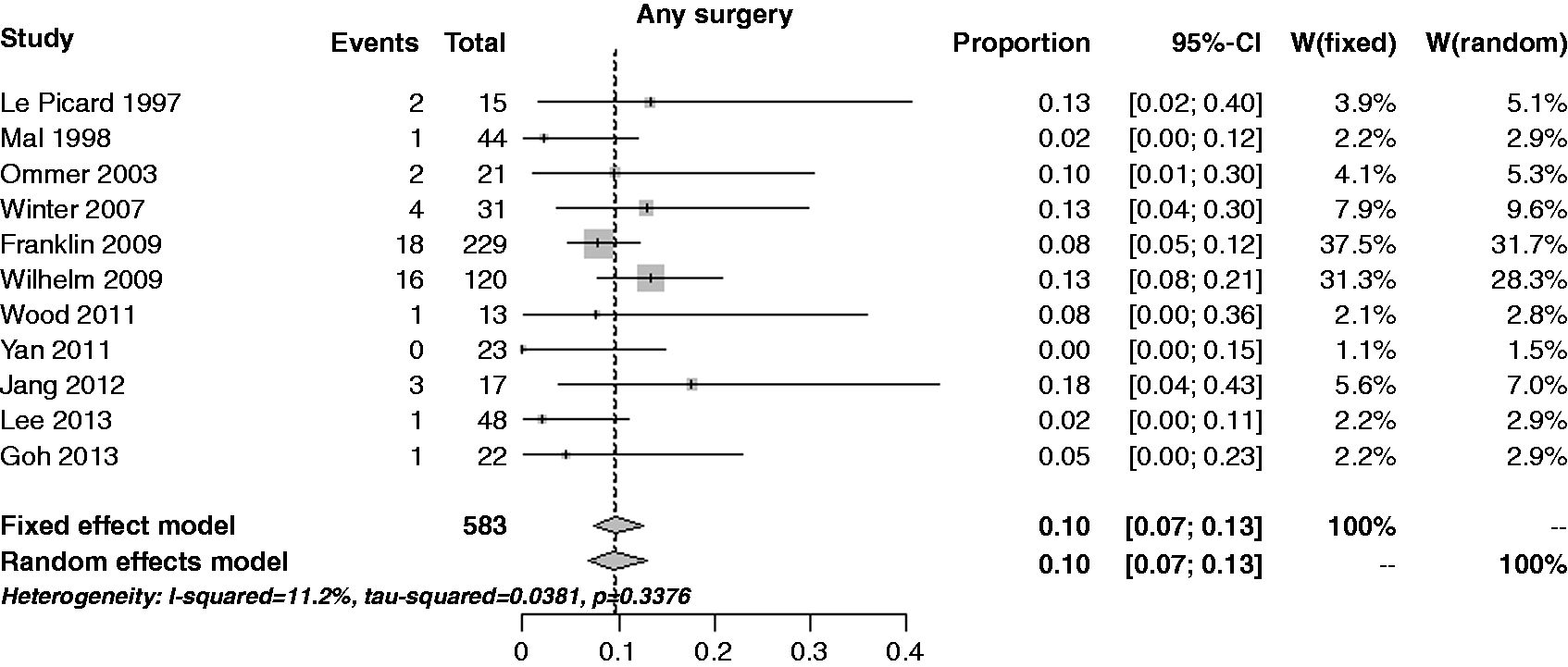
Secondary outcomes
The estimate of the incidence of adenocarcinomas was 10.5% (95% CI 7.3–14.9%), with a moderate heterogeneity (I2 = 42.9%) and no publication bias (p = 0.374) (see Figure 3). Performing a cumulative analysis, the rate estimate decreased on time course: from 12–18% in the time frame 1997–2007, but quite stable around 10–11% after 2009; performing an influential analysis, the rate estimate was reported as constant.
Forest plot for incidence of adenocarcinomas.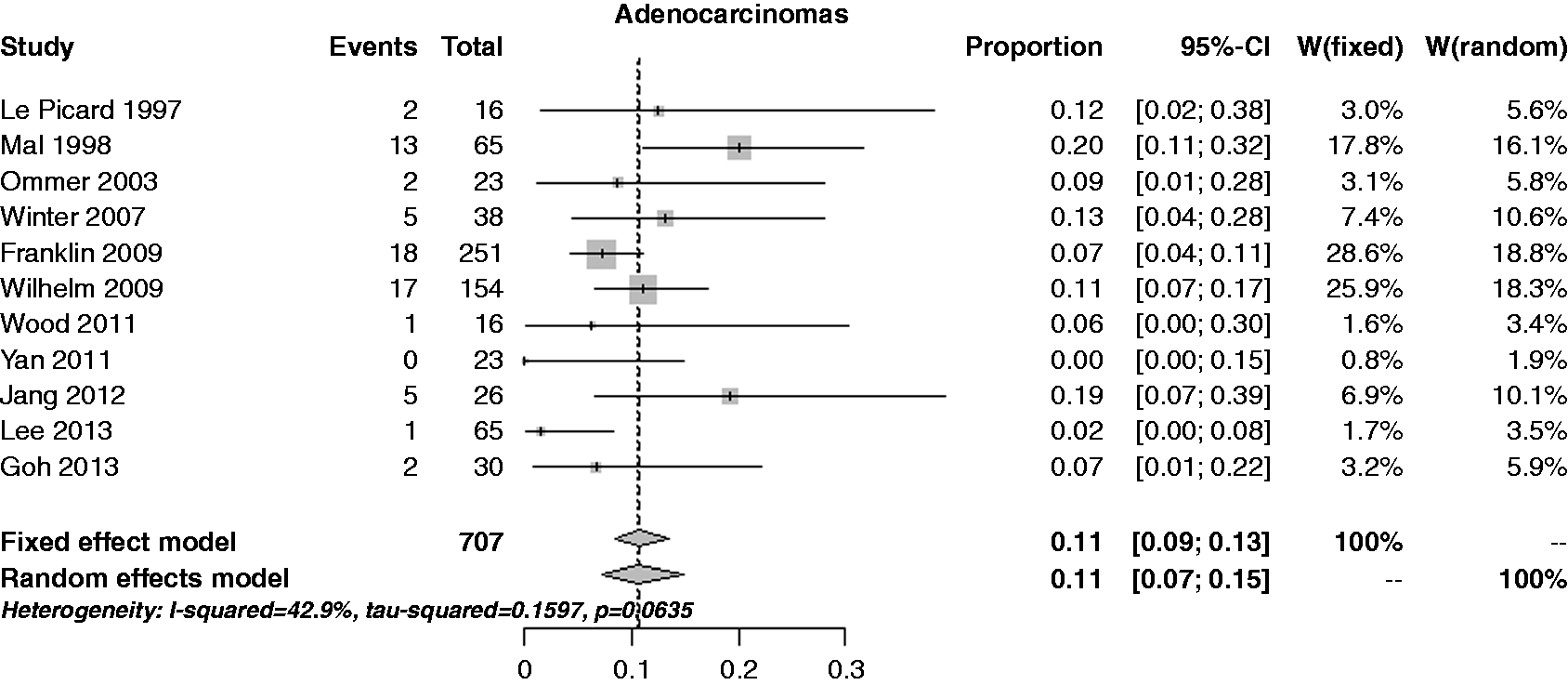
The estimate of the per-lesion rate of further surgery for oncologic radical treatment was 7.9% (95% CI 5.8–10.5%), with no heterogeneity (I2 = 0%) and no publication bias (p = 0.356) (Figure 4). Performing a cumulative analysis, except for the Le Picard et al. trial (13%),15 the rate estimate was stable around 8%; performing an influential analysis, the rate estimate was constant.
Forest plot for per-lesion rate of further surgery for oncologic radical treatment.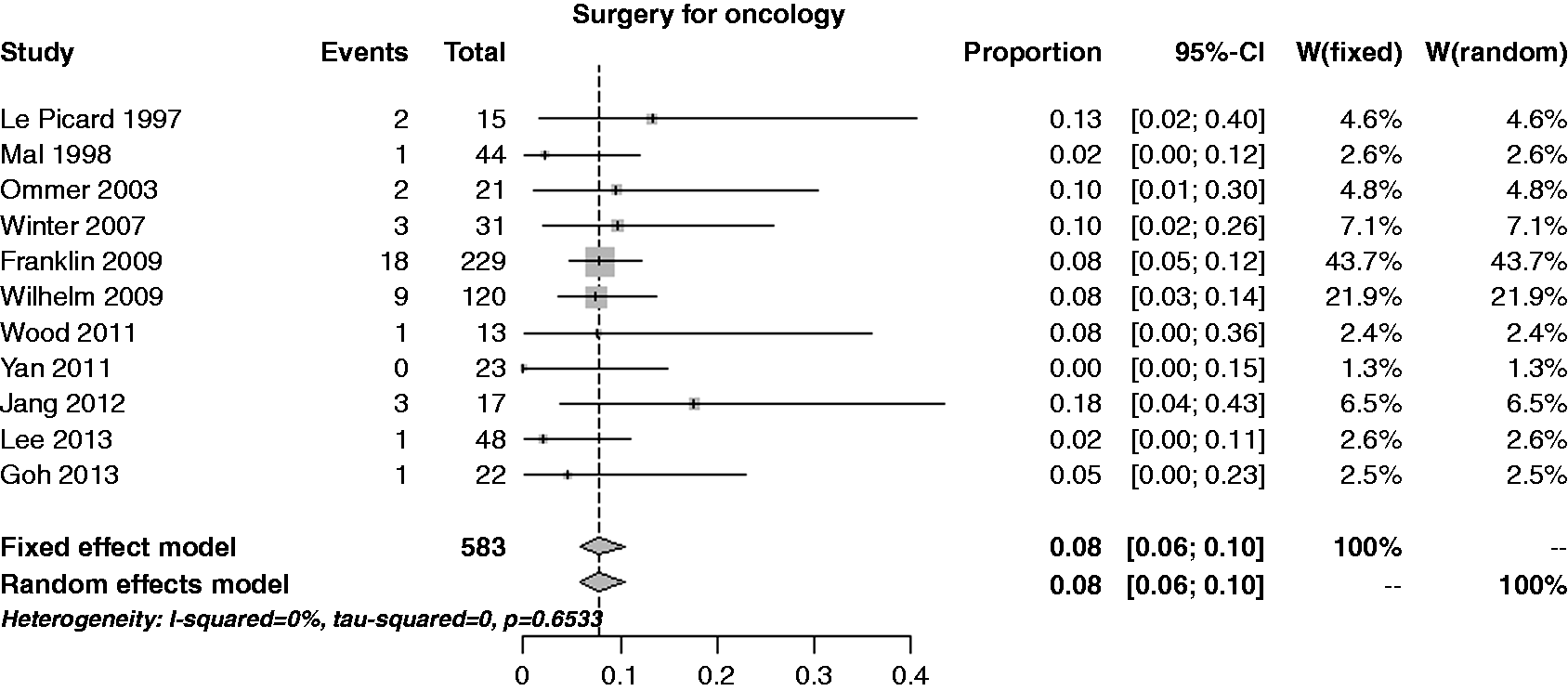
The estimate of the per-lesion rate of overall complications was 7.9% (95% CI 4.2–14.4%), with severe heterogeneity (I2 = 71,5%) and a notable publication bias (p = 0.007) (Figure 5). Performing a cumulative analysis, except for the Le Picard et al. trial (12.5%),15 the rate estimate ranged from 4–9%; performing an influential analysis, the rate estimate was constant.
Forest plot for per-patient rate of overall complications.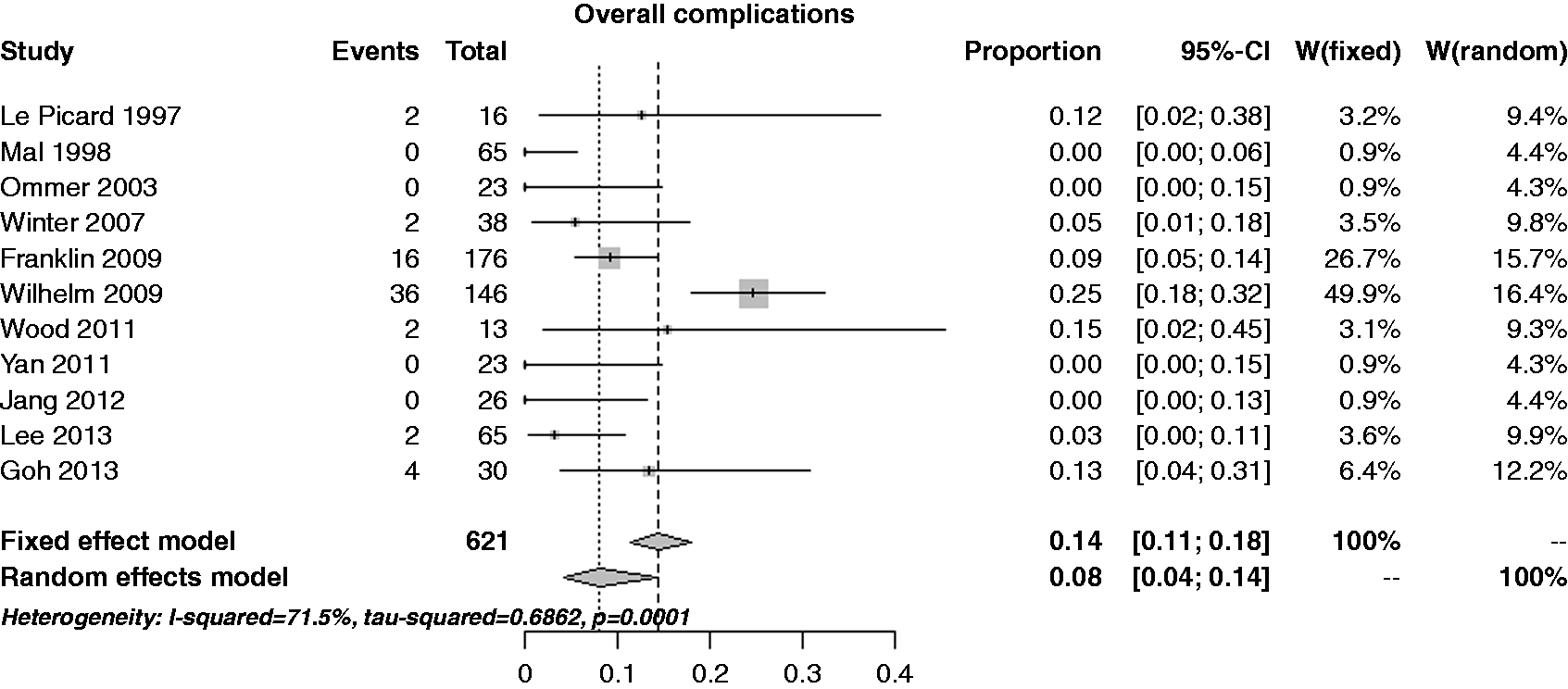
The estimate of the per-lesion rate of further surgery for complications treatment was 3.5% (95% CI 2.0–6.0%), with no heterogeneity (I2 = 0%) but with an extreme publication bias (p = 0.006) (see Figure 6). Performing a cumulative analysis, the rate estimate was stable around 3%; the same happened performing an influential analysis.
Forest plot for per-lesion rate of further surgery for complications treatment.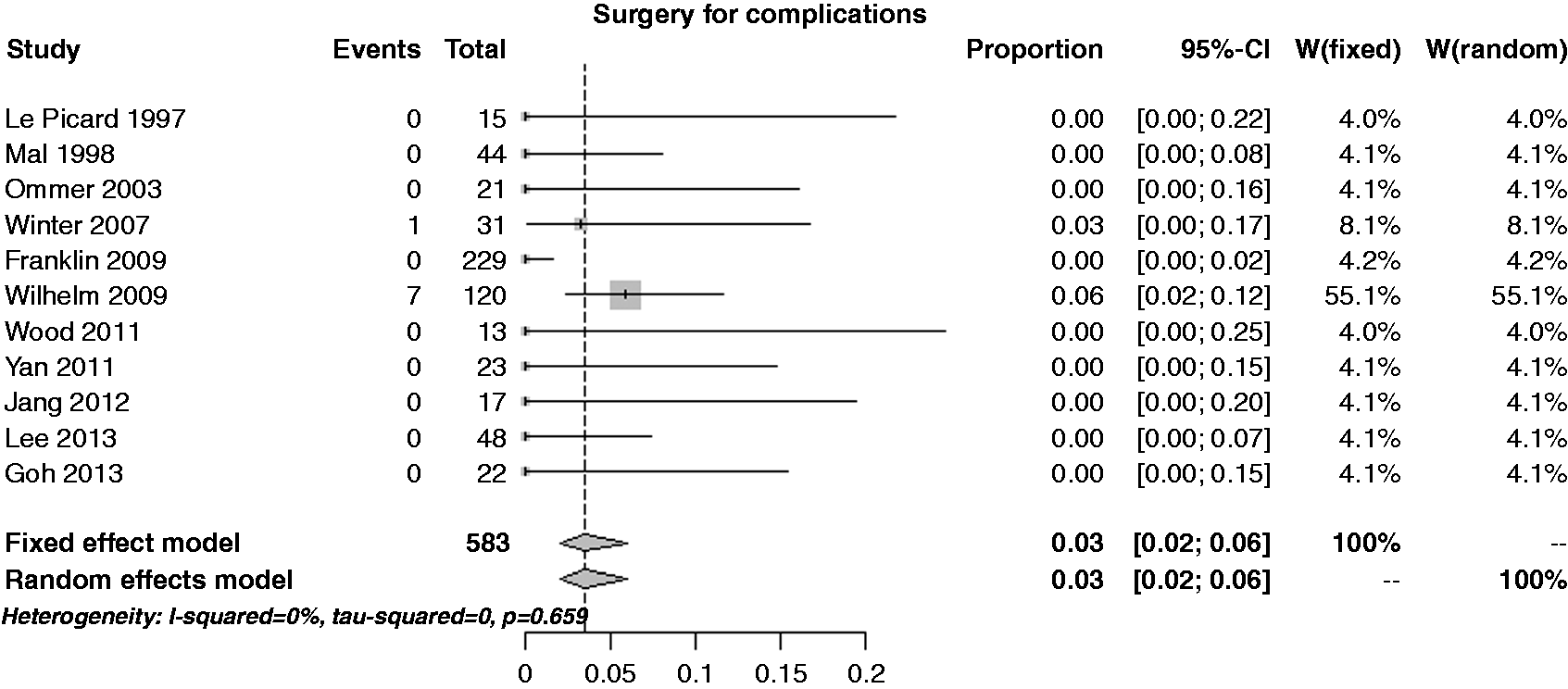
The estimate of the per-lesion rate of conversion to open surgery was 4.3% (95% CI 2.8–6.6%), with no heterogeneity (I2 = 0%) but with an extreme publication bias (p = 0.010) (see Figure 7). Performing a cumulative analysis, the rate estimate was stable around 4% only from 2009; performing an influential analysis, the rate estimate was constant.
Forest plot for per-patient rate of conversion to open surgery.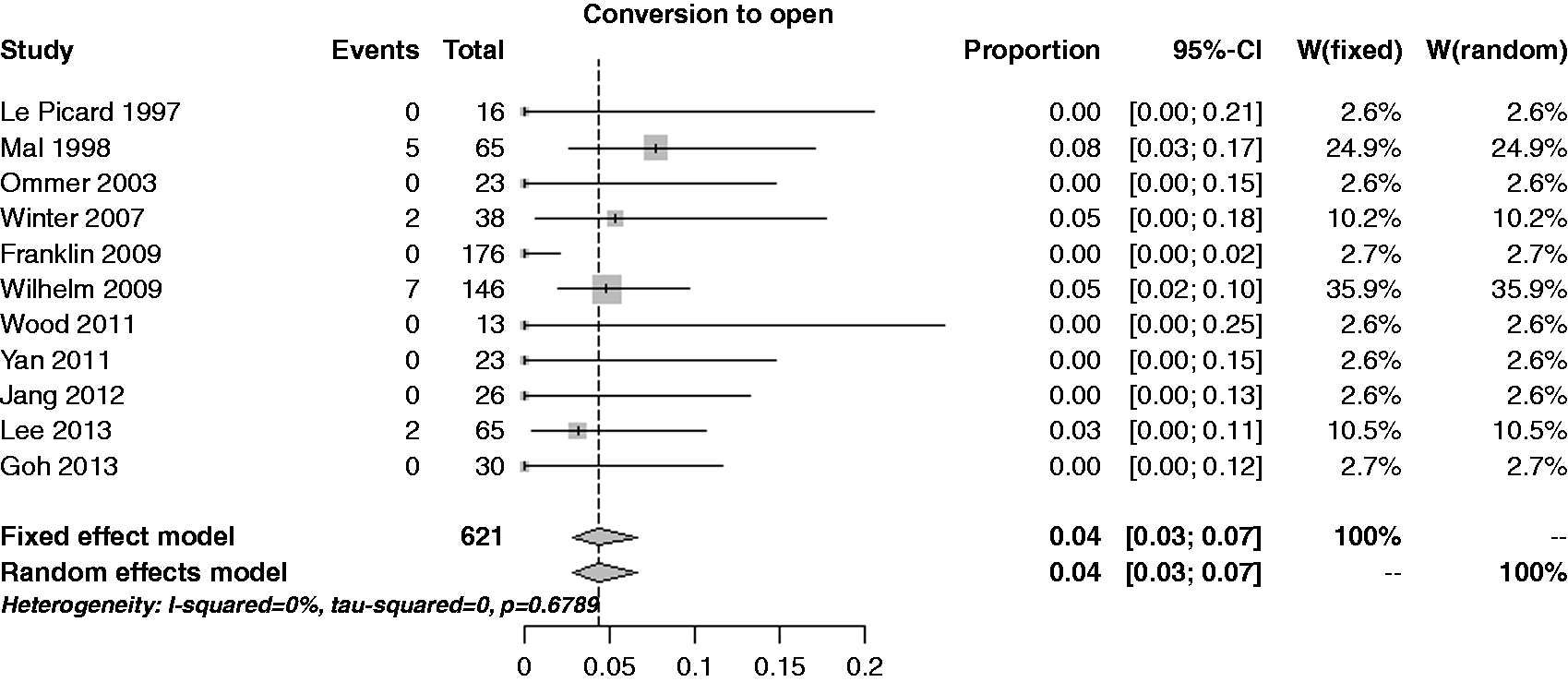
Post-procedural follow-up
Overall, eight studies including 652 resections provided information on post-procedural follow-up. Median follow-up across the series was 35.5 months (range 12–67). The median recurrence rate was 3.4% (0.0–15.0%), corresponding to a pooled risk of 5.4% (95% CI 2.4–11.7%) (see Figure 8).
Forest plot for per lesion rate of recurrence.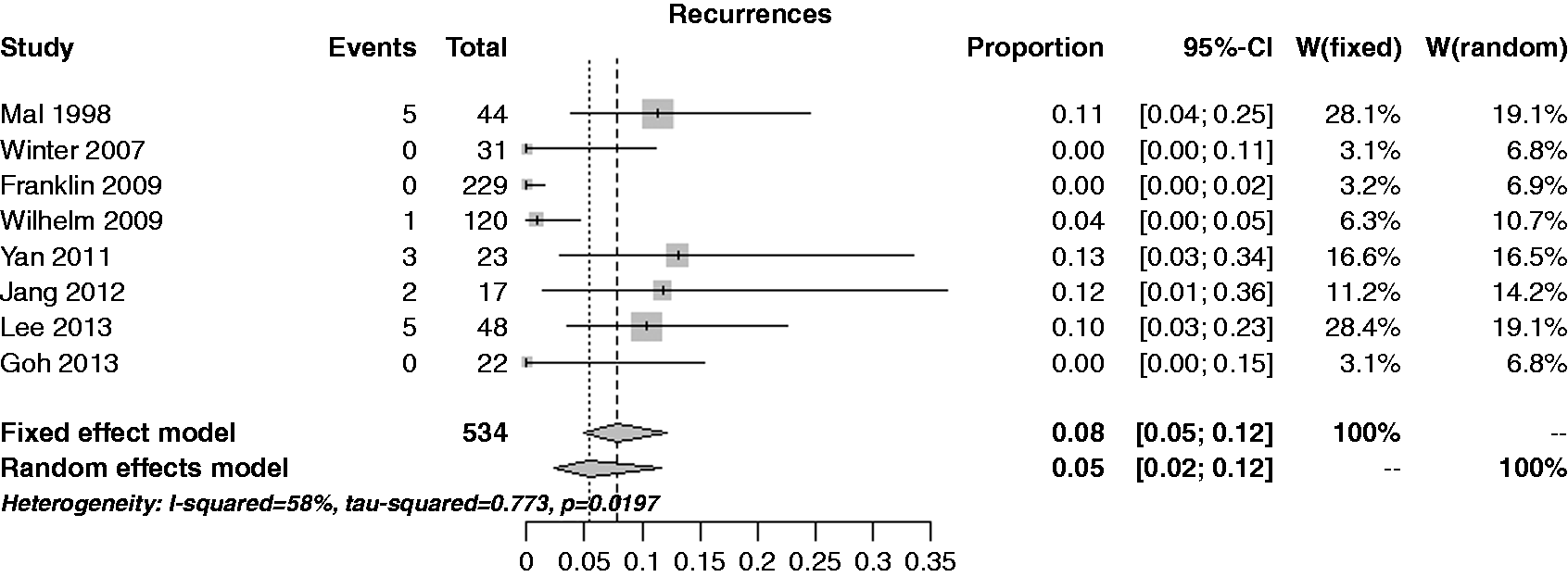
Discussion
The use of combined laparo-endoscopic resection of the large bowel is still controversial. With the exception of three studies,12,17,24 the vast majority of lesions for which a combined technique was indicated, were located in the right colon and caecum. This underlines a technical difficulty in manoeuvring the flexible endoscope in the right colon.
The per-lesion rate of further surgery (i.e. including surgery for complications and surgery for oncologic radical treatment) was chosen as primary outcome of this systematic review for several reasons. First, a robust and independent reference standard is required to minimise the potential risk of publication or recall bias. Second, when passing from a pure endoscopic procedure to a combined laparo-endoscopic technique a lower risk of complications is expected due to the intrinsic double check on the bowel wall integrity. However, according to our analysis, we reported a cumulative risk of 7% between bleeding and perforation requiring further surgery for complication management in about half of these cases, which is quite a high rate compared to standard endoscopic related complications. This underlines the fact that cases included in the studies are likely to remain difficult to treat despite the help of the combined techniques, but it could also suggest that the combination of the two techniques does not necessarily make things easier. In any case, the management of these complications requires secondary surgery in 3% of the cases, which is also slightly more than the incidence of further surgery after standard endoscopic polypectomy 25 and comparable to the results of laparoscopic standard resections. 10 In fact, laparoscopic right and left colectomy are burdened by about 8% overall complication rate, 26 which requires further surgery in about 2% of cases, 27 which is slightly lower than the results from the present meta-analysis.
Recent technological and technical advancements together with the increase in expertise in the field of endoscopic resection of large colorectal superficial lesions are destined to overcome the current need to resort to surgery. A recent Japanese multicentre trial of ESD for colorectal neoplasia in 1111 cases demonstrated an en bloc resection rate of 88%, 28 which lowered to 74% 29 when only lesions >2 cm were taken into consideration, as they should be, for ESD. Considering that as many as 19% of patients at histology revealed an adenocarcinoma, and consequently required surgery, the main oncological advantage of ESD over EMR was realised in only about 10% of all patients. These patients were affected by a well-differentiated, superficial submucosal invasive adenocarcinoma with no lymphovascular invasion.
This limited clinical benefit should be considered together with the technical difficulties. ESD should be primarily limited to lesions with an increased probability of early submucosal invasion while in all other cases at an earlier stage a standard piece-meal EMR would be sufficient. It seems reasonable that EMR should be most probably the treatment of choice of any large (>2 cm) colonic sessile and flat lesions. In all cases in which adenocarcinoma tissue are found and not confined to the mucosal layer, radical surgery should be advised. It is assumed that an infiltrated margin in case of dysplasia is never an indication for radical surgery, but for a repeated endoscopy. On the other hand, this is mandatory if the lesion reveals malignant tissue. For this reason the occasional finding of carcinomas in about 11% of cases treated by laparo-endoscopic technique, despite the fact that the vast majority of studies only included lesions preoperatively assessed as benign relying on endoscopic biopsies, must be taken into serious concern. Indeed, about 8% of the overall cases needed a second surgical procedure to achieve a radical oncologic treatment as indicated. This means that the global incidence of second surgical procedures is as high as 10%, which is considerable especially if compared to the 2% of patients who required further surgery after standard laparoscopic colonic resection, as reported above. 26 To be exact, in the largest studies here represented, 19 this second surgical procedure was performed under the same general anaesthesia, as the specimen was examined on frozen sections during surgery. This is a practice achieving some appreciation in the USA, but not at all common in Europe nor in Asia. A critical issue in the application of laparo-endoscopic techniques is patient selection, in order to guarantee adequate oncologic treatment. In order to optimise this, the widespread adoption of more accurate endoscopic diagnostic techniques such as chromoendoscopy, magnification and fluorescence will play a crucial role in the near future.
As a counterpart of the high incidence of secondary surgery the recurrence rate is relatively low, being set at 5.4% which is lower that standard polypectomy, 25 although still consistent.
There are limitations to the present analysis. A moderate/high degree of heterogeneity was present in the estimates, mainly due to the variety of the techniques. Regarding study design, not only were most of the publications retrospective, but they also embraced very long enrolment periods, so that a different mix of learning curve and post-training experience was likely to occur in the different series. The individual studies did not separately report data on efficacy according to the histological subtype (low and high grade adenoma, submucosal cancer). Therefore, we cannot exclude lower rates of R0 resection in more advanced histological lesions that are potentially more difficult to treat. Moreover, the different techniques have not yet been standardised so that appropriate technical guidelines may be needed. Finally, the majority of the included studies did not report the results obtained related to various outcomes in a separate way for each technique used, making it not possible to compare specific results of the different techniques.
In conclusion, the findings of this systematic review have to be taken with reasonable caution, as the studies selected describing laparo-endoscopic procedures were extremely variable in techniques adopted. Nevertheless, the general impression is that the gain in terms of reduced invasiveness is quite limited, and difficult to justify in the presence of a consistent rate of complications and oncologic inadequacy that require further surgery. A meticulous case by case analysis is therefore recommended.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.