
Abstract
Background
Incomplete polyp resection during colorectal endoscopic mucosal resection (EMR) might contribute to the development of interval cancer.
Objective
This retrospective study aimed to determine the incidence of incomplete polyp resection during EMR of colorectal polyps located across a fold compared with that of colorectal polyps located between folds.
Methods
In total, 262 patients with 262 lesions that were ≥10 mm in diameter and treated with conventional EMR were enrolled. The main outcome was the incidence of incomplete polyp resections. Propensity score matching and inverse probability of treatment weighting (IPTW) were performed to reduce the effects of selection bias.
Results
Fifty-seven lesions (21.8%) were incompletely resected. After propensity score matching, the lesions located across a fold were at higher risk of incomplete resection than those between folds (26/68, 38.2% vs 7/68, 10.3%; odds ratio (OR): 3.71; 95% confidence interval (CI): 1.61–8.56; p < 0.01). These findings persisted after adjusting for the differences at baseline using the IPTW method (OR: 3.63; 95% CI: 1.72–7.63; p = 0.001).
Conclusions
There is an increased risk of an incomplete polyp resection for a colorectal polyp that is located across a fold compared with that for a polyp that is located between folds.
Keywords
Introduction
The endoscopic resection of colorectal polyps reduces the incidence of colorectal cancer and its associated mortality.1,2 Endoscopic mucosal resection (EMR) is widely acknowledged as a general treatment for colorectal polyps because of its technical simplicity and lower adverse event rate.3–5 However, incomplete polyp resection might play an important role in the development of interval cancer, and a higher frequency of local recurrence is associated with endoscopic piecemeal mucosal resections; therefore, complete en bloc resections are recommended.3,6–8
Semipedunculated and superficial polyps that may be carcinomas are good indications for EMR, particularly colorectal polyps that are ≥10 mm in diameter, of which 28.2% have been determined to be non-invasive high-grade and invasive neoplasia.9,10 While it is necessary to completely resect these polyps, those that are 10–20 mm in diameter are more likely to be incompletely resected compared with smaller polyps that are 5–9 mm wide. 11
Little is known about the predictive factors of incomplete polyp resection during colorectal EMR, but some factors have been described, including the polyp diameter, a sessile serrated histology and the endoscopist’s skill.11–13 However, these studies evaluated undefined biopsy specimens following EMR. The findings from one retrospective matched study showed that the polyp’s location and histology were associated with significant risks of positive resection margins. 14 However, previous studies have not evaluated concerns about the technical difficulties that may be encountered based on detailed preoperative findings, in particular, the polyp’s location with respect to the colonic folds, its relationship with a colonic flexure and its visibility. The presence of an underlying semilunar fold is an independent risk factor associated with the failure of an en bloc resection or a perforation during colorectal endoscopic submucosal dissection (ESD). 15 In addition, the findings from one of our previous studies showed that a colorectal polyp that was located across a fold was one of the risk factors associated with incomplete polyp resection during EMR. 16 Therefore, we conducted a comparative study of incomplete polyp resections during the EMR of colorectal polyps that were located across a fold or between folds, using propensity score analysis to explore our hypothesis that colorectal polyps located across a fold are more difficult to resect completely than those that are located between folds.
Materials and methods
Patients
This was a single-center retrospective observational study. Between January 2012 and December 2013, patients with colorectal polyps that were ≥10 mm in diameter who underwent conventional EMR were enrolled. All patients expected to undergo colorectal polyp resection en bloc were enrolled. Cases of planned endoscopic piecemeal resection were excluded because we use ESD to perform en bloc resection on lesions that are difficult to resect en bloc via conventional EMR. Pedunculated tumors were excluded. Sessile serrated polyps were not included. These might be classified as hyperplastic polyps because of insufficient diagnosis. All cases involved targeted en bloc resection and we excluded cases of planned endoscopic piecemeal resection based on the database.
The larger lesions were considered the target lesions in those patients in whom multiple synchronous lesions were treated. Propensity score matching and inverse probability of treatment weighting (IPTW) were performed to reduce the effects of selection biases associated with incomplete polyp resection during EMR and other possible confounding factors. 17
The study’s protocol was approved by Izumiotsu Municipal Hospital’s Institutional Review Board on 30 June 2016. Written informed consent was obtained from all of the patients who participated in this study. The study’s protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki, as reflected in a prior approval by the institution's human research committee.
Endoscopic mucosal resection procedure
Thirteen endoscopists conducted the endoscopic procedures. The indication of conventional EMR was colorectal polyps that were ≥10 mm in diameter, which was considered as difficult to resect en bloc with standard polypectomy technique because of the size or flat shape. 9 Polyp diameter was measured using the size of the snare catheter. Bowel preparation using a polyethylene glycol solution was performed before the procedure. A single-channel lower gastrointestinal endoscope and a standard electrosurgical generator (ICC 200 or VIO300D; ERBE Elektromedizin GmbH, Tübingen, Germany) with a 13-mm or 26-mm Dragonare™ bipolar snare (BSDS-217; Zeon Medical Inc., Tokyo, Japan) were used. Normal saline was injected into the submucosal layer of the lesion, and electrosurgically resected using a snare and the ‘Auto cut’ mode. If the lesion was not resected en bloc, we performed an endoscopic piecemeal mucosal resection on the residual polyp.
Histological assessment
All of the specimens were assessed microscopically to evaluate their histological type, the depth of invasion, and the vertical and horizontal margins using the Japanese classification of cancers of the colon and rectum. 18 Hence, an early colorectal carcinoma was defined as a lesion that was confined to the mucosa or submucosa, regardless of the presence of lymph node metastases. A complete polyp resection was defined histologically as an en bloc resection with confirmed adenomatous component-free vertical and horizontal margins. 14 An incomplete polyp resection was identified if a piecemeal resection had been performed, or if the vertical and/or horizontal margins were positive or indeterminate for an adenomatous component.
Outcome measures
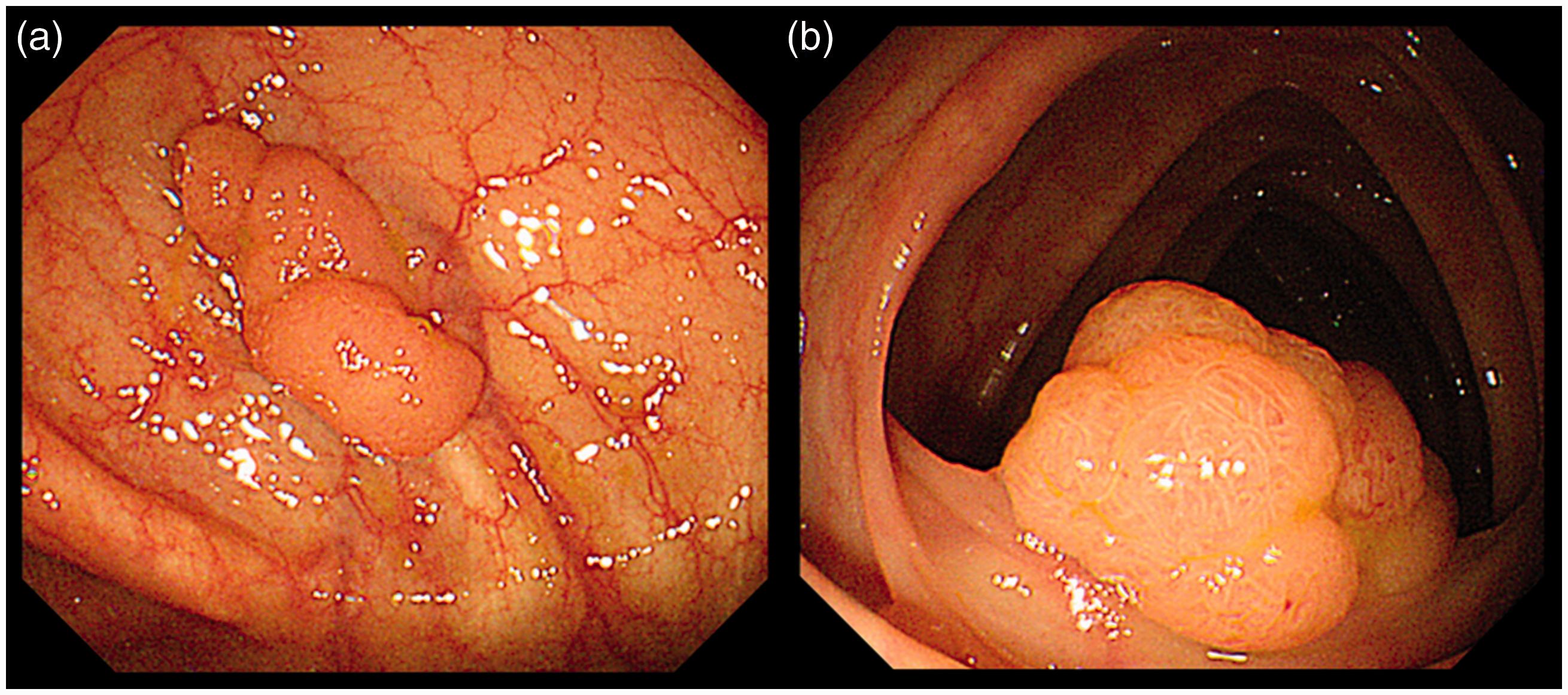
The main outcome was the incidence of incomplete polyp resections following the EMR between colorectal polyps that were located across a fold and those that were located between folds. Colorectal polyps that were located across a fold identified if the lesion margin at the oral side and/or the anal side passed through a fold completely. To evaluate this outcome, we assessed the risk factors associated with incomplete polyp resection during EMR, including age, gender, the polyp diameter, the polyp’s location, where the right side was defined as being proximal to the splenic flexure, the histological polyp type (namely, an adenoma or a carcinoma), the depth of polyp invasion, the endoscopic appearance of the polyp (sessile or slightly elevated), the presence of a lateral spreading tumor (LST), the polyp’s location with respect to a colonic fold (that is, located across a fold or between folds) (Figure 1(a) and (b)), the polyp’s relationship with a colonic flexure, the vertical or tangential visibility of the lesion (Figure 2(a) and (b)), and the endoscopist’s experience (more or less than 300 cases of EMR).
15
These findings were assessed by a review of endoscopic images by an experienced gastrointestinal endoscopist (H.M.). We defined LSTs as lesions that were ≥10 mm in diameter with low vertical axes that extended laterally along the interior wall of the lumen.
19
Location with respect to colonic fold. (a) Located across a fold and (b) located between folds. Visibility of a lesion. (a) Vertically and (b) tangentially.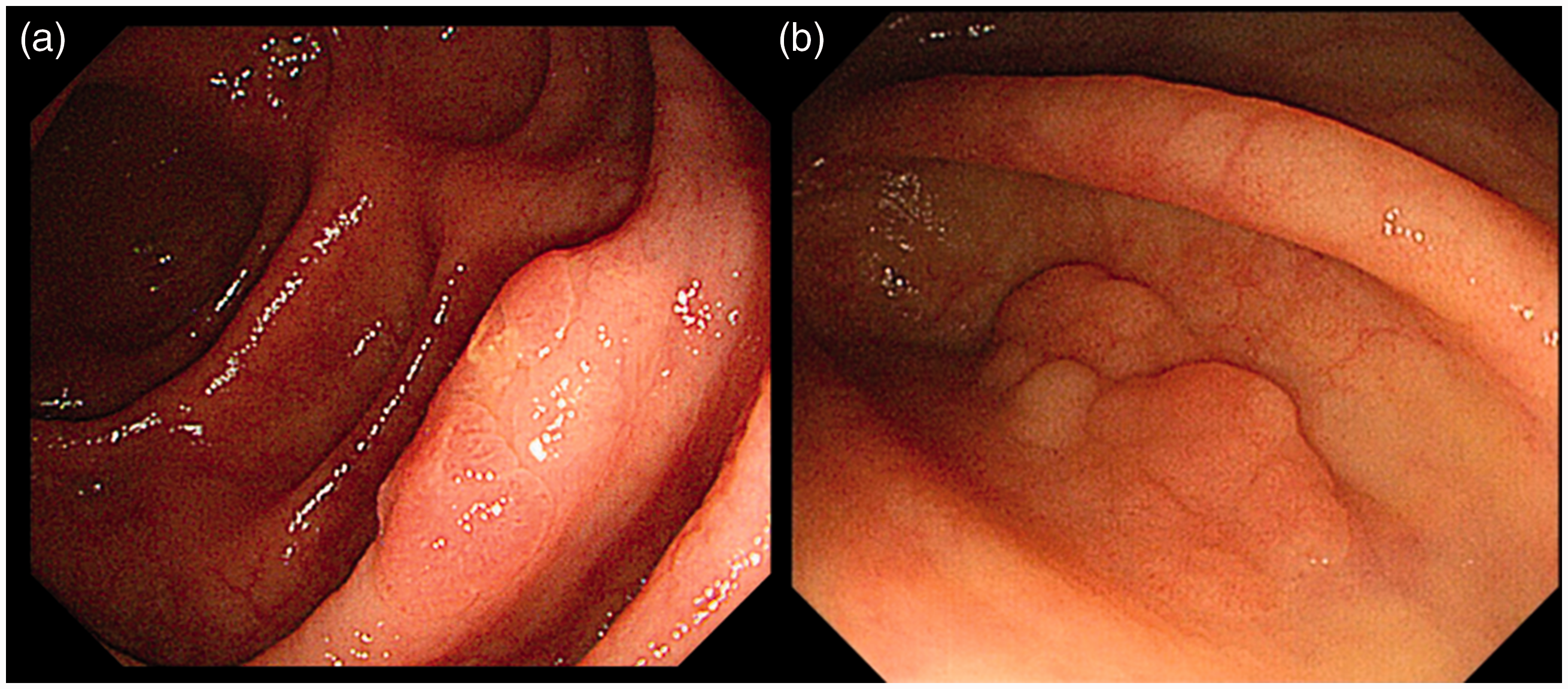
Statistical analyses
Baseline characteristics before and after propensity score matching.
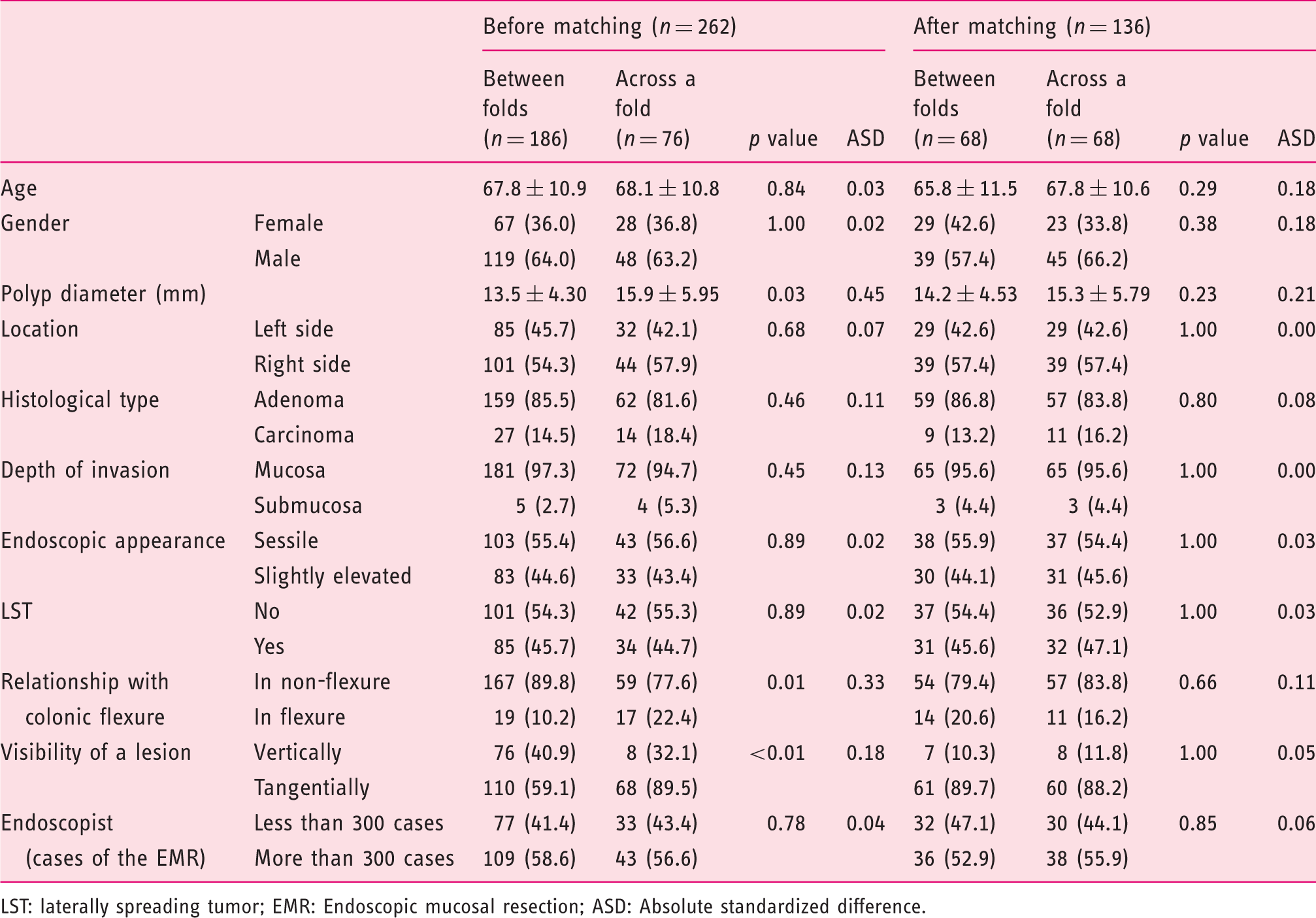
LST: laterally spreading tumor; EMR: Endoscopic mucosal resection; ASD: Absolute standardized difference.
In addition, the IPTW method based on the propensity score was applied to the risk factors associated with incomplete polyp resection, which enabled us to adjust for confounding factors between binary groups, can evaluate causal effects without reducing the sample size by using the estimated propensity scores to construct weights for the data.23,24
The statistical analyses were performed using IBM® SPSS® software, version 23.0 for Windows (IBM Corporation, Armonk, NY, USA) and the R statistical package, version 3.0.2 (The R Foundation for Statistical Computing Vienna, Austria; http://www.R-project.org/). All of the statistical tests were two-sided, and a value of p < 0.05 was considered statistically significant.
Results
Clinicopathological characteristics of the study subjects
A total of 321 patients with 455 colorectal polyps that were ≥10 mm in diameter were treated using conventional EMR (Figure 3). Of those, 59 with 84 pedunculated tumors were excluded. The larger lesions were the target lesions in 109 patients who underwent treatment for multiple synchronous lesions. Consequently, 262 patients with 262 lesions were enrolled.
Study enrollment.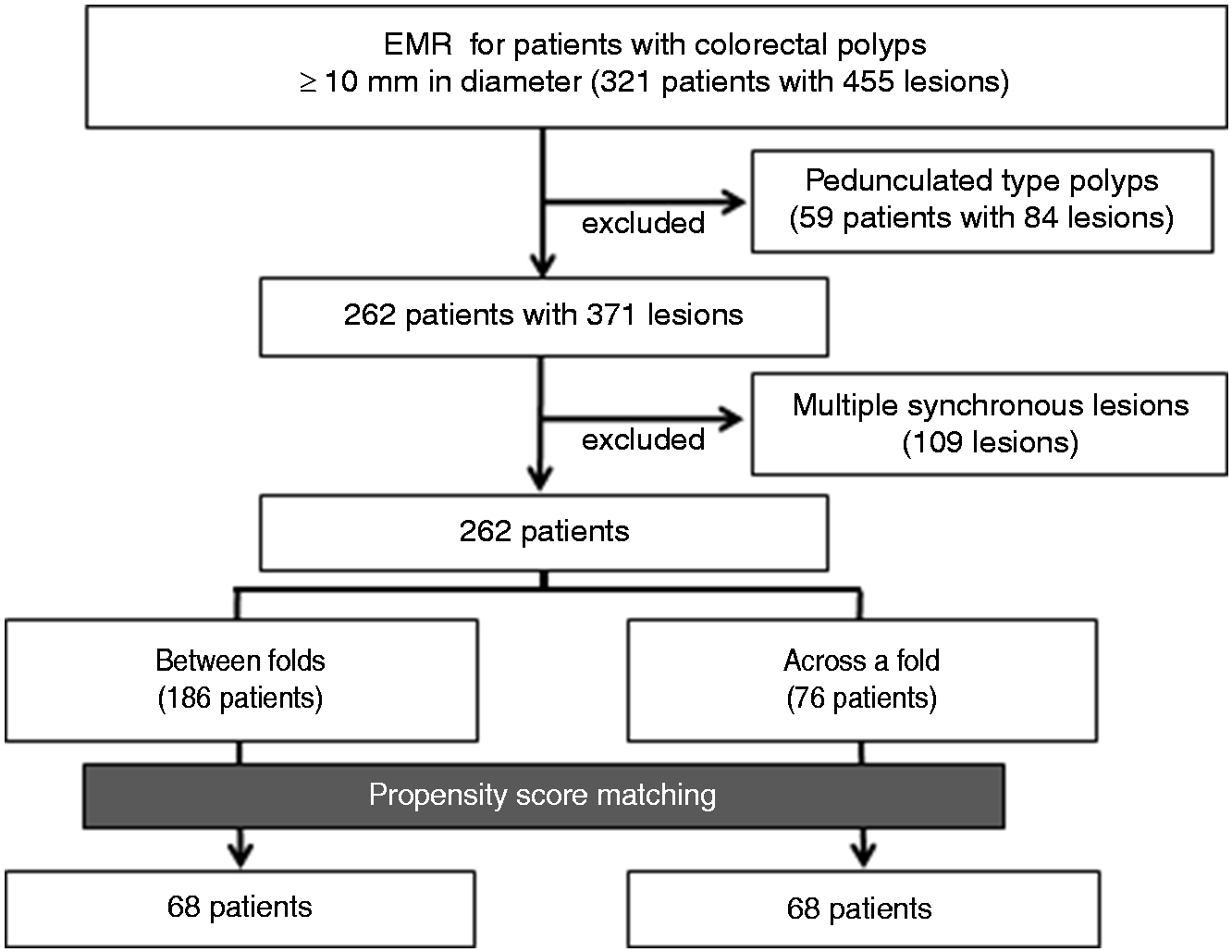
The range of polyp diameter was 10–40 mm in diameter. Adenocarcinoma was diagnosed in 15.6% of cases. There were no adverse events such as perforation. Compared with the colorectal polyps that were located between folds, those that were located across a fold had a significantly larger diameter, were more frequently located in a colonic flexure and were more visible tangentially before matching. After propensity score matching, there were 68 matched pairs of colorectal polyps that were located across a fold or between folds. The baseline characteristics of the two groups were comparable (Table 1).
Effect of a lesion located across a fold on incomplete resection
Risk factors of incomplete polyp resection by crude logistic regression before and after propensity score matching.
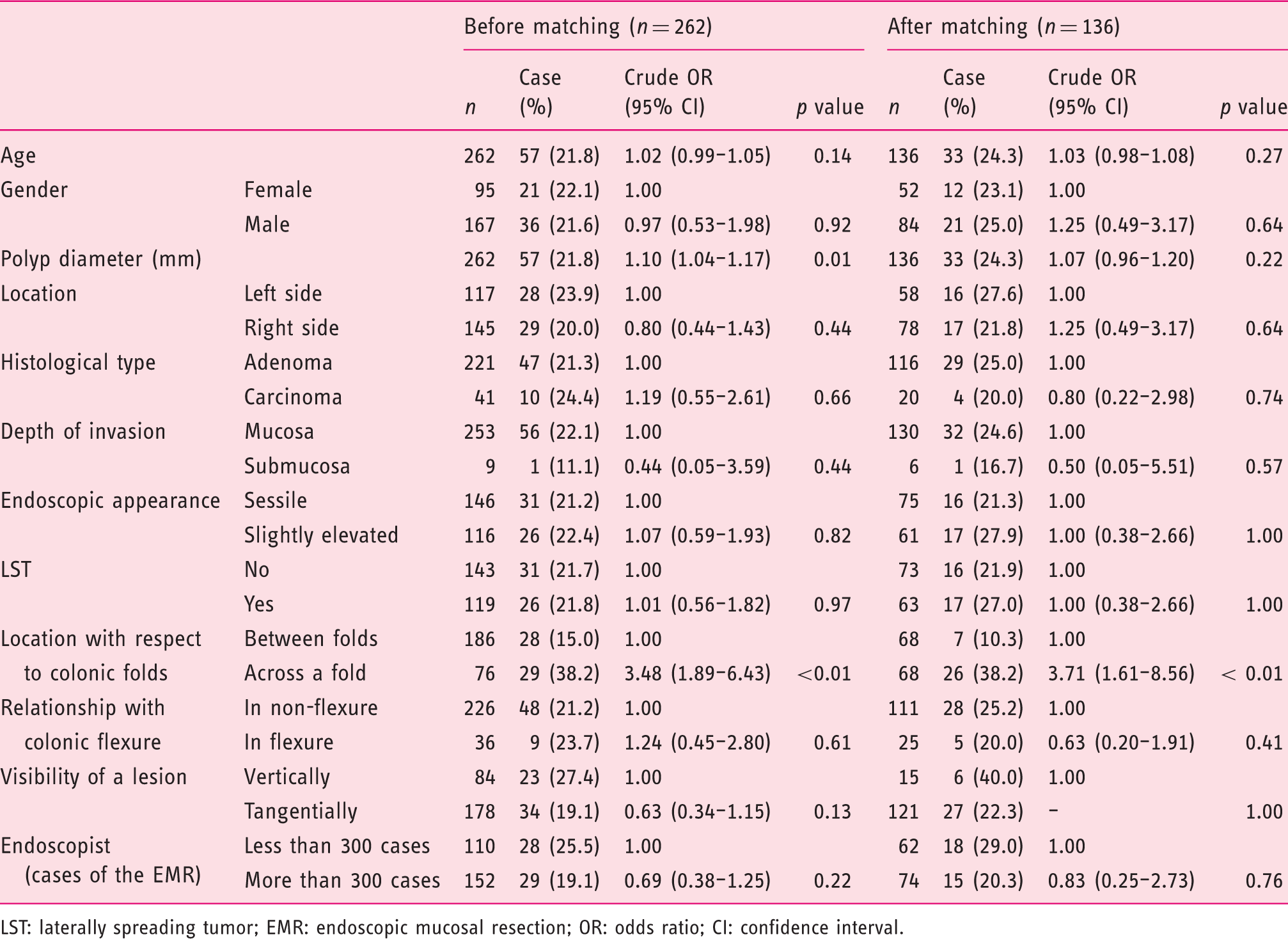
LST: laterally spreading tumor; EMR: endoscopic mucosal resection; OR: odds ratio; CI: confidence interval.
Risk of incomplete polyp resection by multivariate logistic regression after propensity score matching.
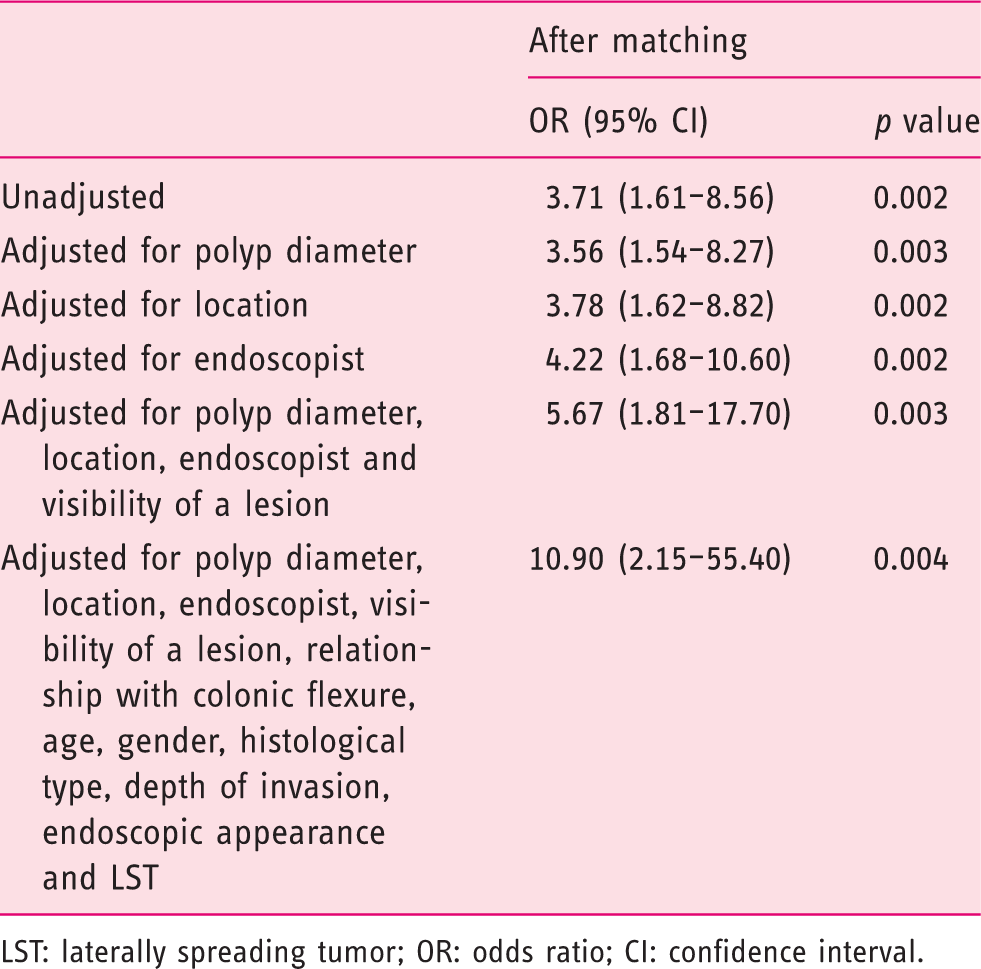
LST: laterally spreading tumor; OR: odds ratio; CI: confidence interval.
Propensity score matched and weighted odds ratios for risk of incomplete polyp resection.
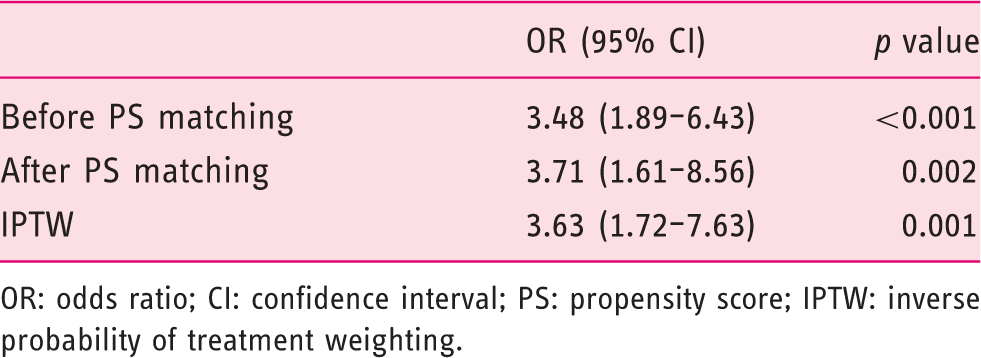
OR: odds ratio; CI: confidence interval; PS: propensity score; IPTW: inverse probability of treatment weighting.
Subgroup analysis
We performed subgroup analysis according to two polyp-diameter groups. In the 10–19-mm diameter group, the lesions located across a fold were more frequently resected incompletely (15/48, 31.2%) than those located between folds (21/152, 13.8%; p = 0.01). In the ≥20-mm diameter group, the lesions located across a fold were also more frequently resected incompletely (14/28, 50.0%) than those located between folds (7/34, 20.6%; p = 0.02).
Evaluation of the propensity score model
The propensity score model was well calibrated (Hosmer–Lemeshow test: p = 0.751), and it had a high level of discrimination between the colorectal polyps located between folds and those located across a fold (c-statistic: 0.750). Therefore, it appeared that the most likely possible confounders had been identified in this study. However, after matching, the median ASD was 0.06 (interquartile range: 0.03–0.18). Therefore, the ASD values indicated that the propensity score matching could not completely remove the imbalance of the variables.
Discussion
The present study indicates that there is an increased risk of an incomplete polyp resection for a colorectal polyp that is located across a fold compared with those that are located between folds. In other words, a colorectal polyp that is located across a fold is harder to resect en bloc.
Although the reasons underlying the association between colorectal polyps that are located across a fold and incomplete resection remain unclear, we regularly manage such cases and offer three explanations. First, since the polyp’s margin on the oral side is difficult to identify in the straight view, the resection margin attained using a snare may be incorrect. Second, an inaccurate submucosal injection may cause the lesion to turn more towards the oral side, thereby making it more difficult to identify the lesion’s margin on that side. Third, even if the snare can squeeze the lesion properly, it may be slippery because of the presence of a semilunar fold.
This study has three important strengths. First, this was the first attempt to evaluate the technical difficulties associated with colorectal EMR based on detailed preoperative findings, especially the polyp’s location with respect to a colonic fold, the polyp’s relationship with a colonic flexure and the visibility of a lesion during the procedure. Although some predictive factors associated with incomplete polyp resection have been described, including the polyp diameter, a sessile serrated histology, the polyp’s location and the skill of the endoscopist, these do not necessarily help with respect to evaluations before a polyp is resected. A polyp’s location with respect to a colonic fold was previously reported to have no association with incomplete polyp resection. 11 However, the study in question included several small (5–9 mm) polyps. In addition, their evaluation of an incomplete resection that involved using biopsies to identify the polyp margins was inexact and a major limitation. Conversely, our study only targeted colorectal polyps that were ≥10 mm in diameter, 10 and we evaluated the margins of the resected specimens microscopically. Furthermore, our study reduced the selection bias associated with a polyp’s location with respect to a colonic fold and we confirmed the results using multivariate analysis.
The second strength was associated with the use of propensity score analysis. Only one prospective study, but no randomized controlled trial (RCT), has investigated incomplete colorectal polyp resections. 11 While an RCT is the most robust study design for the generation of scientific evidence that may support causal associations, it is often difficult to conduct RCTs because of budgetary and time constraints, or ethical concerns.21,22 Non-randomized studies are associated with a potential selection bias, for example, a polyp’s size and location. Indeed, polyp size was a predictive factor in the present study before matching. Propensity score matching resolves the issues relating to bias in observational studies, and studies that use this technique are often considered to be pseudo-randomized. Furthermore, an IPTW method that was based on the propensity score was employed without reducing the sample size. IPTW was used to assess the sensitivity of the results, and it indicated that the results were qualitatively similar to those from the propensity score matching analysis.23–25
The third strength is associated with the use of the general endoscopic procedure, namely, ‘colorectal EMR’, by many of the endoscopists, including trainee endoscopists, at general hospitals. Recently, ESD has been developed for the curative resection of colorectal polyps, because of its higher en bloc resection and curability rates.12,19,26 However, ESD is associated with a higher perforation rate and has a longer procedure time than EMR.12,27,28,29 Therefore, conventional EMR remains the most widely recognized general treatment for colorectal polyps because of its technical simplicity and lower adverse event rate.3–5 Most studies have been conducted at high-volume specialist institutions, and some publications have cited the inexperience of endoscopists associated with incomplete resection.14,15 Conversely, our study involved an adjustment for the experience of the endoscopist. Therefore, our study’s data are more generalizable compared with previous studies.
This study’s findings give rise to the following questions: what therapeutic strategy should be selected for colorectal polyps that are located across a fold and should we select ESD for all of these cases? The presence of an underlying semilunar fold is associated with the risk of failure of an en bloc resection or perforation during ESD. 15 A variety of methods have been devised to prevent incomplete polyp resections, including EMR with a circumferential incision and EMR-precutting, which is technically simple and safe compared with ESD.27,30 Furthermore, a submucosal injection of hyaluronic acid may reduce the frequency of incomplete polyp resections due to maintaining mucosal elevations during EMR. 31 An appropriate therapeutic strategy should be investigated in a large prospective study.
The present study has some limitations. First, the study’s retrospective nature and the use of propensity score analysis led to some inherent limitations, including the choice of finite covariates, which implies that relevant covariates may have been omitted. We appreciate that it is difficult to adjust for potential confounders using propensity score analysis. We also did not consider other factors such as bowel preparation, indigocarmine use and the judgement of each endoscopist to allow piecemeal resection to avoid perforation, which might be associated with incomplete polyp resection. Second, the sample size declined after the propensity score matching, and the smaller sample size was associated with a reduction in the statistical power. However, since this study’s results appeared to be highly reliable, which was indicated by the statistical significance of the results, the study’s sample size may have been adequate. Moreover, we confirmed the results using IPTW that did not involve a sample size reduction. Third, in the present study, an incomplete polyp resection was identified if a piecemeal resection had been performed, or if the vertical and/or horizontal margins were positive or indeterminate for an adenomatous component. A recent study showed the local recurrence rate of an en bloc-lateral margin indeterminate group (2.2%) was significantly lower than that of a piecemeal-lateral margin indeterminate group (15.2%). 32 In addition, the present study demonstrated that not only piecemeal resection, but also resections with positive margins (R1 resection) excluding piecemeal resections, increased in a colorectal polyp located across a fold compared with those located between folds. Furthermore, we performed subgroup analysis on only two groups according to polyp diameter because of the small sample size. Polyp diameter was previously reported to be a risk factor for incomplete polyp resection 11 and was used as our before-matching outcome. However, colorectal polyps that were located across folds were larger in diameter than those located between folds (Table 1). Therefore, propensity score matching was used to reduce selection bias. Our outcomes prove that the risk of incomplete polyp resection for a colorectal polyp that is located across a fold is high regardless of polyp diameter. In addition, we performed multivariate regression analysis including the polyp diameter (Table 3) as well as IPTW analysis (Table 4), which is well known to reduce confounding and selection biases, to confirm this outcome. Moreover, incomplete polyp resection for a colorectal polyp that is located across a fold is higher in each diameter-based group in the subgroup analysis. Finally, we did not record surveillance after the resection. We should conduct histological analysis of the margins and recurrence. The lack of follow-up data is a limitation of this study.
In conclusion, the present study’s findings suggest that there is an increased risk of an incomplete polyp resection for a colorectal polyp that is located across a fold. To resect these polyps completely and prevent the development of interval cancer, another therapeutic method, for example, a submucosal injection of hyaluronic acid, may be needed.
Footnotes
Acknowledgements
Declaration of conflicting interests
TW, TT and YF are Faculty members of a course sponsored by EA pharma Co., Ltd. YF received research grants from Ono. All other authors declare that they have no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Informed consent
Written informed consent was obtained from all of the patients who participated in this study.
Ethics approval
The study's protocol was approved by Izumiotsu Municipal Hospital's Institutional Review Board.