
Abstract
Background
Underwater endoscopic mucosal resection without submucosal injection has been described for removing large flat colorectal lesions.
Objective
We aim to evaluate the reproducibility of this technique in terms of ease of implementation, safety and efficacy.
Methods
A prospective observational study of consecutive underwater endoscopic mucosal resection in a community hospital was performed.
Results
From September 2014 to April 2015, 25 flat or sessile colorectal lesions (median size 22.8 mm, range 10–50 mm; 18 placed in the right colon) were removed in 25 patients. Two of the lesions were adenomatous recurrences on scar of prior resection and one was a recurrence on a surgical anastomosis. The resection was performed en bloc in 76% of the cases. At the pathological examination, 14 lesions (56%) had advanced histology and seven (28%) were sessile serrated adenomas (two with high-grade dysplasia). Complete resection was observed in all the lesions removed en bloc. Intra-procedural bleeding was observed in two cases; both were managed endoscopically and were uneventful. No major adverse events occurred.
Conclusion
Underwater endoscopic mucosal resection appears to be an easy, safe and effective technique in a community setting. Further studies evaluating the efficacy of the technique (early and late recurrence), as well as comparing it with traditional mucosal resection, are warranted.
Keywords
Introduction
Underwater endoscopic mucosal resection (UEMR) is a technique described by Dr Kenneth Binmoeller in 2012 for removing flat colorectal lesions. 1 In contrast to conventional endoscopic mucosal resection (EMR), the bowel lumen is filled with water rather than air and submucosal injection of the lesion is not required.
Since the publication of the original paper in which the authors described 62 cases of large sessile colorectal polyps removed by the UEMR technique, other case series have been published,2–4 and authors have found UEMR to be easy to learn, safe and effective.
The aim of this series was to evaluate the reproducibility of UEMR in terms of ease of implementation, safety, and efficacy in a community setting.
Patients and methods
All procedures were performed in a community hospital by two operators (AA and FR). AA performed 23 out of 25 procedures and FR performed the two other UEMR. Before starting, AA had the opportunity to observe about five procedures performed by Dr Binmoeller, the ‘father’ of the technique. FR observed some videos and a few procedures conducted by AA. The colonoscopies were performed using the water-assisted technique in patients under conscious sedation (2.5 mg/5 mg midazolam and 25 mg/50 mg pethidine), with a standard colonoscope (CF-H180AI; Olympus, Tokyo, Japan). The snares used for the resection were the Captivator II (Boston Scientific, Natick, Massachusetts, USA), the Acusnare (Cook, Bloomington, Indiana, USA) or the Optimizer (Conmed, Utica, New York State, USA), with variable size. The size of the snares used ranged from 15–32 mm. The smaller ones were preferred for polyps less than 15 mm or in cases of piecemeal resection.
The electrosurgical system used was the ICC200 (ERBE Elektromedizin, Tübingen, Germany), with endocut setting effect 3 (120 W).
After identifying the lesion for removal, UEMR was begun by marking the perimeter of the adenoma by argon plasma coagulation. Next, the air, along with residual faecal material, was removed and the bowel lumen was filled with at least 500 ml of water at room temperature with a water pump (OFP-2; Olympus). Snare resection was then performed with the aim of achieving an en bloc removal of the specimen. Gentle suction while closing the snare was applied to produce a slow collapse of the lumen and to increase the capturable surface area (Figure 1).
Underwater endoscopic mucosal resection of a polyp (Paris IIa + IIc) of the ascending colon. (a) polyp view in colon filled with air, (b) underwater polyp view and (c) UEMR.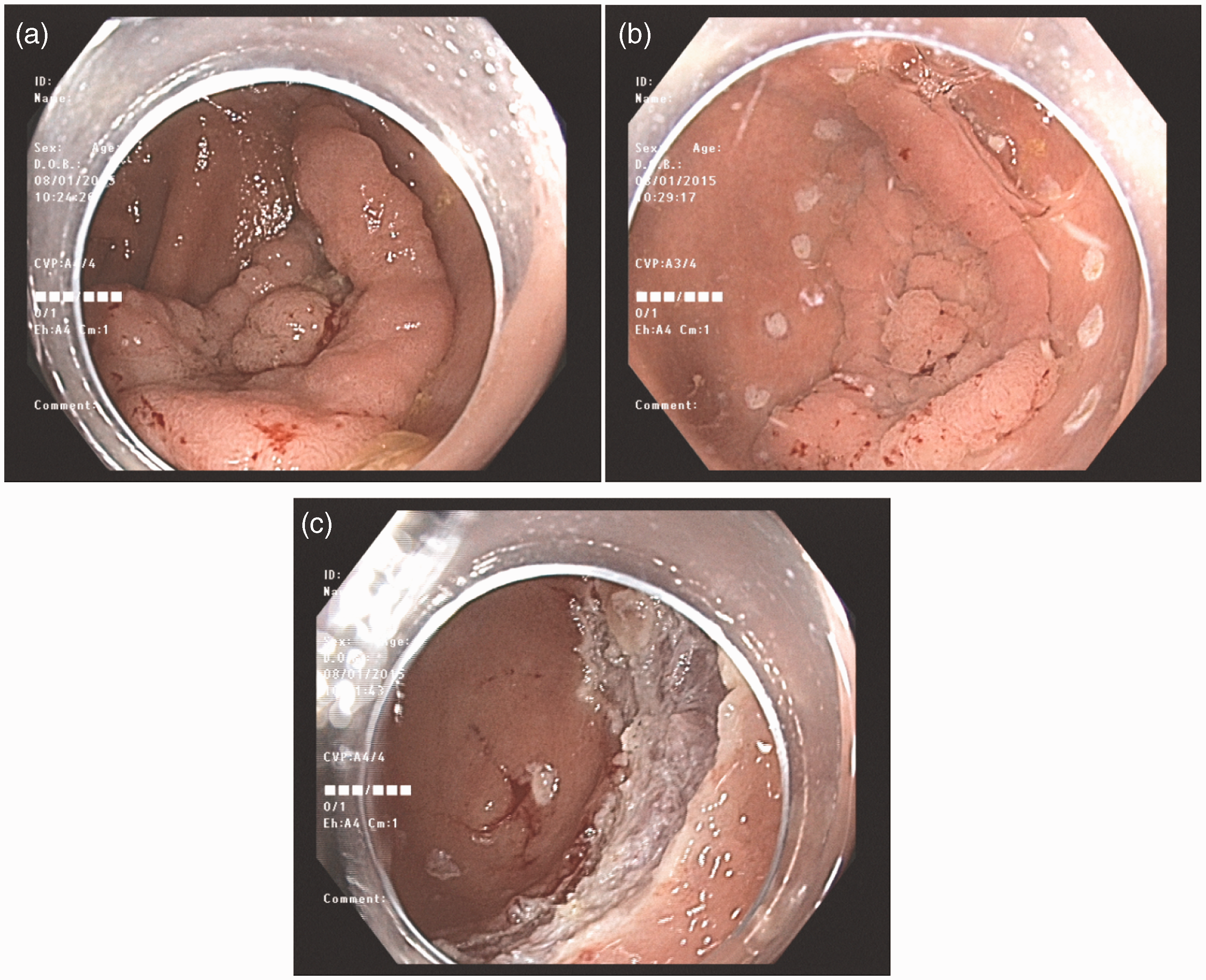
After complete removal of the lesion was achieved, the colonic resection margins were assessed by white light and Narrow Band Imaging application in order to evaluate the endoscopic efficacy of the resection. The main outcomes evaluated were en bloc resection rate, R0 resection rate, and adverse events.
Results
From September 2014 to June 2015, 25 flat colorectal lesions were removed using the UEMR technique in 25 patients (10 men and 15 women). The median age was 62.2 years (range 40–86 years). Of 25 polyps, 22 were diagnosed and simultaneously removed during the same procedure. The median size was 24.6 mm (range 10–50 mm). The remaining three lesions consisted of two adenomatous recurrences on scars of previous polypectomies and one recurrence at an anastomosis site; all were around 10 mm in size.
The majority of the lesions (18/25, 72%) were located in the right colon, four were in the left colon and three in the rectum. In all the cases in which an en bloc resection was not successful, piecemeal resection was performed. Complete resection with endoscopic negative margins at visual assessment (white light and Narrow Band Imaging) was obtained in all the lesions. Fourteen lesions (56%) had advanced histology and seven (28%) were sessile serrated adenomas (two with high-grade dysplasia).
Features of the polyps removed.
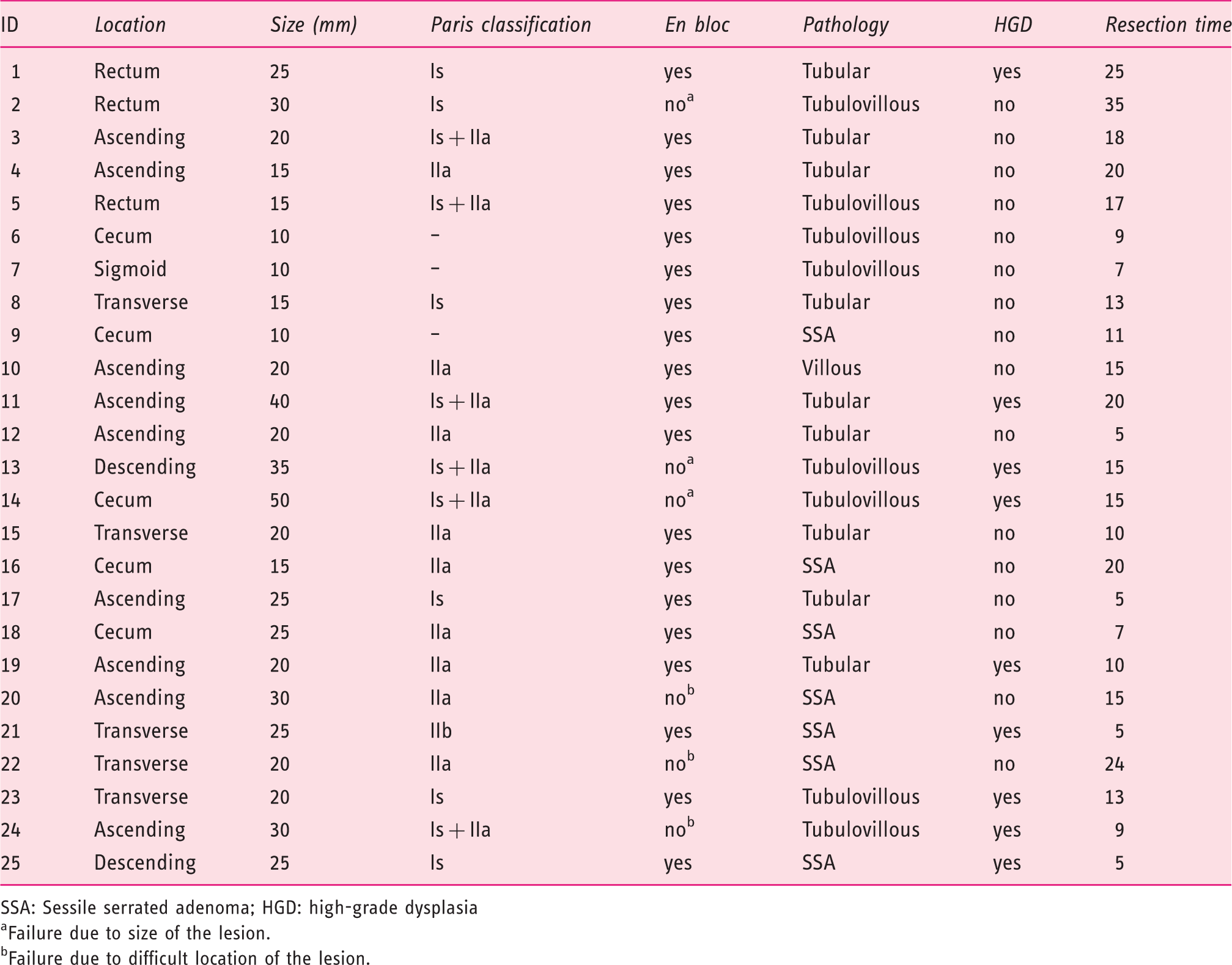
SSA: Sessile serrated adenoma; HGD: high-grade dysplasia
Failure due to size of the lesion.
Failure due to difficult location of the lesion.
Intra-procedural bleeding occurred in two patients and was managed by endo-clip application. These events occurred in the first two procedures performed, and both in lesions located in the rectum. Neither perforations nor major bleeding (early or delayed) were observed (complication rate 0%).
Discussion
This series is the first to report the use of the UEMR technique in a community setting. The en bloc resection rate was 76%, with an R0 resection in all en bloc specimens. No adverse events were observed; two intra-procedural bleeding events occurred, and both were managed endoscopically with no consequences.
The ‘father’ of the UEMR technique developed this idea having observed that, during endoscopic ultrasound, in a bowel lumen filled with water, the muscularis propria does not change its circular configuration and does not follow the changes of the mucosa and sub-mucosa, even during peristaltic contractions. In this particular condition, lesions appear to float into the lumen, moving away from the muscularis propria.
When using the conventional EMR approach gas insufflation, needed for visualization, distends the lumen and thereby thins the bowel wall, theoretically increasing the risk of perforation and transmural burn. As a result, submucosal injection has been adopted for the purpose of increasing the bowel wall thickness in order to facilitate safe snare capture of the lesion. However, submucosal injection can sometimes make resection more difficult. For example, after injection, the snare can slip off the plane during closure as a result of the spread of solution, which can raise both the lesion as well as normal mucosa. In addition, submucosal injection can sometimes increase risk in EMR. For example, the injection may reach the inter-connective tissue between the circular and longitudinal muscle layers, resulting in accidental snare capture of the muscle layer itself. Further, when the injection is spread outside the bowel wall, it can result in post-polypectomy syndrome.
In contrast to its behaviour under air insufflation, a flat lesion tends to contract in water and appears more raised, possibly due to the high fat content of the sub-mucosa. Indeed, water immersion results in less distension of the bowel lumen compared with gas insufflation, allowing the capture of a larger mucosal surface area in the opened snare.
Some technical aspects deserve to be highlighted. For one, it appears to be important to fill the lumen with a large amount of water, at least 500–1000 ml. In our first two cases we did not use enough water and observed bleeding in both cases, probably due to poor ‘floatation’ of the polyp, as the lumen was not adequately filled. After modifying this error we no longer observed post-resection haemorrhage. Secondly, attention must be paid to closing the snare during a peristaltic contraction, thus allowing the capture the greatest surface area possible. This is especially important for larger lesions. Finally, the use of a stiff snare, to press firmly against the bowel wall, can help to capture the entire ‘floating’ lesion.
The main drawback of the UEMR technique is related to poor visualization due to suboptimal bowel preparation; however, vigorous irrigation and suction or, as an alternative, water-exchange colonoscopy, may help solve this problem.
The UEMR technique has already been shown to be easy, effective, and safe in referral centres, with a technical success rate in polyps that had not undergone a prior resection attempt of 99.7%, an adverse event rate of 3.4% and a recurrence rate of 3%.
The main limitation of the present study is the small sample size. In spite of this, our series further confirms that UEMR is an easy, safe, and effective technique for the removal of flat and sessile colorectal polyps.
Another limitation is the lack of follow-up in 14 out of 25 patients; these patients have a follow-up endoscopy scheduled in the coming months. At 6-month colonoscopy, we found the presence of residual adenomas in 1 out of 11 (9%) subjects.
It is well known that en bloc removal should be the goal of any polypectomy, since it is the only technique able to provide adequate evaluation of the margins of the resected lesion. Moreover, en bloc resection has been shown to decrease the risk of adenoma recurrence related to the incomplete removal that is frequently associated with piecemeal resection. 5 For this reason, endoscopic submucosal dissection (ESD) has been proposed in recent years. This technique has the ability to obtain an en bloc resection of large lesions, but it is complex, technically demanding, and time consuming. In addition, ESD is associated with high risk of perforation and has a long learning curve.
The UEMR technique could increase the rate of en bloc resection when compared with traditional EMR. 6 In addition, it may make resection easier, especially in more complex situations, such as in lesions scarred from prior resection attempts or in lesions located on an anastomosis.
The ease of learning and lower risk of adverse events may ultimately lead to UEMR providing a ‘third way’ of resection, in between traditional EMR and ESD, for the removal of large lesions. Further studies on the efficacy of UEMR in terms of early and late recurrence, as well as comparing UEMR with traditional EMR, are needed.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.
Acknowledgements
We would like to thank Steve Kane BS (Paul May & Frank Stein Interventional Endoscopy Center, California Pacific Medical Center, San Francisco, USA), for a critical review of the manuscript.