
Abstract
Background
Dysplasia assessment of Barrett’s esophagus biopsies is associated with low observer agreement; guidelines advise expert review. We have developed a web-based review panel for dysplastic Barrett’s esophagus biopsies.
Objective
The purpose of this study was to test if 10 gastrointestinal pathologists working at Dutch Barrett’s esophagus expert centres met pre-set benchmark scores for quality criteria.
Methods
Ten gastrointestinal pathologists twice assessed 60 digitalized Barrett’s esophagus cases, enriched for dysplasia; then randomised (7520 assessments). We tested predefined benchmark quality criteria: (a) percentage of ‘indefinite for dysplasia’ diagnoses, benchmark score ≤14% for all cases, ≤16% for dysplastic subset, (b) intra-observer agreement; benchmark score ≥0.66/≥0.39, (c) percentage agreement with ‘gold standard diagnosis’; benchmark score ≥82%/≥73%, (d) proportion of cases with high-grade dysplasia underdiagnosed as non-dysplastic Barrett’s esophagus; benchmark score ≤1/78 (≤1.28%) assessments for dysplastic subset.
Results
Gastrointestinal pathologists had seven years’ Barrett’s esophagus-experience, handling seven Barrett’s esophagus-cases weekly. Three met stringent benchmark scores; all cases and dysplastic subset, three met extended benchmark scores. Four pathologists lacked one quality criterion to meet benchmark scores.
Conclusion
Predefined benchmark scores for expert assessment of Barrett’s esophagus dysplasia biopsies are stringent and met by some gastrointestinal pathologists. The majority of assessors however, only showed limited deviation from benchmark scores. We expect further training with group discussions will lead to adherence of all participating gastrointestinal pathologists to quality criteria, and therefore eligible to join the review panel.
Keywords
Key summary
Barrett’s esophagus (BE) with dysplasia is a proven risk factor for the development of esophageal adenocarcinoma. Observer agreement for the diagnosis of low-grade dysplasia in BE is low, prompting guidelines to advise expert review. This study shows that expert review can be objectified by using pre-defined benchmark quality criteria for histological assessment of BE biopsies. This study establishes that expertise according to benchmark criteria can be acquired and maintained using digital pathology training. This study implies that constant output quality within a digital pathology review panel can be maintained when expanding the number of pathologists.
Introduction
In Barrett’s esophagus (BE), the normal stratified squamous epithelium of the distal esophagus has been replaced by columnar epithelium with or without goblet cells. Patients with BE have a risk of developing esophageal adenocarcinoma (EAC) and malignant transformation follows the metaplasia – dysplasia – carcinoma sequence. 1 BE patients therefore undergo endoscopic surveillance. Low-grade dysplasia (LGD) in biopsies obtained during endoscopic surveillance is an accepted risk factor for progression, but diagnosis can be difficult and interobserver agreement is low.2,3 Therefore, guidelines advise review of all dysplastic cases by a second, preferably expert, pathologist.4–11
In The Netherlands we have initiated a national digital review panel for dysplastic BE, consisting of five core pathologists considered ‘experts’ in the field of BE. These five expert BE pathologists have been dedicated to the field of BE for a minimum of 10 years, have a minimum caseload of five BE cases per week of which ≥25% is dysplastic, have participated in multiple training programs (www.best-academia.eu), and have co-authored on >5 peer reviewed publications in this field. Moreover, it is the only BE expert pathologist group of individuals worldwide that have validated their BE diagnostic assessments in prospective clinical studies.12–15 To optimize the throughput time of the Dutch digital review panel, to divide the workload and to gain nationwide coverage, we aim to expand the panel with 10 gastrointestinal (GI) pathologists from the eight BE expert centres in The Netherlands. To maintain panel diagnostic quality we need to confirm that these pathologists’ assessments correspond with the assessment standards of the current five core pathologists. In an earlier study, we defined benchmark quality criteria, based on the assessment of the core pathologists of a study set of 60 whole-endoscopy cases. 16 The aim of this study was to evaluate if the assessment scores of 10 dedicated GI pathologists, reviewing the same study set of 60 whole-endoscopy cases, fall within the predefined range for these benchmark quality criteria.
Materials and methods
Case selection and slide scanning
For 60 patients who had had an endoscopy for BE surveillance, we selected all formalin fixed, paraffin embedded tissue blocks and/or slides of the biopsies obtained during the endoscopy. The case set consisted of 39 cases with an original diagnosis of LGD (n = 20) or high-grade dysplasia (HGD; n = 19) that had been sent to our centre for consultation, between 2012 and 2014. These 39 dysplastic cases were supplemented with 21 consecutive non-dysplastic BE (NDBE) cases from a community hospital in the Amsterdam region.
The five core expert BE pathologists had assessed this case set twice individually at an earlier stage followed by consensus meetings to create a gold standard diagnosis for all cases. 16 Their scores were used to create benchmark values for the quality criteria.
Assessors
The assessors were 10 dedicated GI pathologists working in the eight BE expert centres in The Netherlands. In accordance with Dutch guidelines, work-up and treatment of dysplastic BE is centralized in these specialized centers. All pathologists had been dedicated to the field of BE for a median of seven years (range 5–30 years) and had a median case load of seven BE cases per week (range 5–17), of which ≥25% were dysplastic. All were actively practicing pathologists, considered experts by their peers, and had already participated in a joint training programme consisting of evaluating and discussing 60 single-slide BE cases (35 dysplastic), of which the results were published separately. 17
Histological assessment of samples
For the current study, the pathologists independently assessed all 60 cases twice in random order, with a wash-out time of at least one month, scoring them according to the modified Vienna criteria for GI neoplasms.2,18 The p53 immunohistochemistry (IHC) was used as a diagnostic adjunct and scored according to the p53 decision rule developed earlier. 17 The pathologists individually logged onto the virtual slide system to assess the cases and record the highest diagnostic grade per case. After two assessment rounds, all cases that did not have a majority diagnosis were discussed in a face-to-face group discussion with all participants, for educational purposes.
Definition of benchmark values for quality criteria
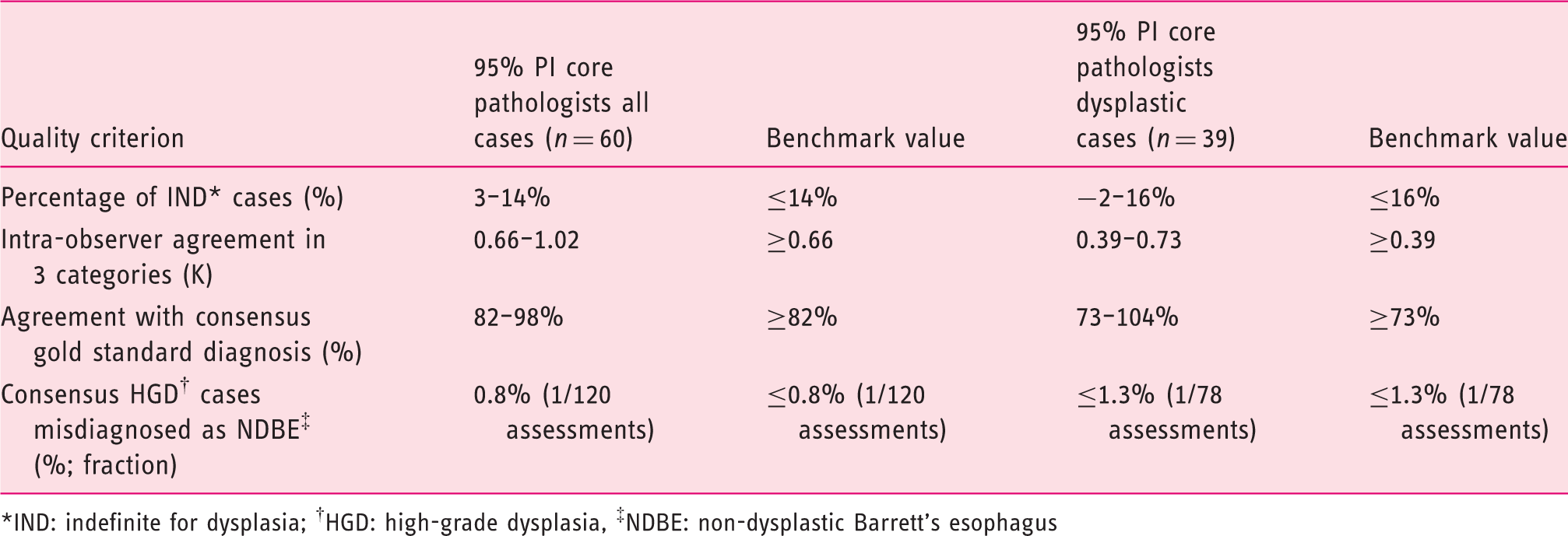
For each of the four quality criteria, a benchmark range had been calculated based on the scores of the five core pathologists in the aforementioned earlier study (see Table 1).
16
The flow chart of the study can be seen in Figure 1.
Flowchart of study set-up. Values for benchmark quality criteria based on 95% prediction interval (PI) of five core pathologists.
16
*IND: indefinite for dysplasia; †HGD: high-grade dysplasia, ‡NDBE: non-dysplastic Barrett's esophagus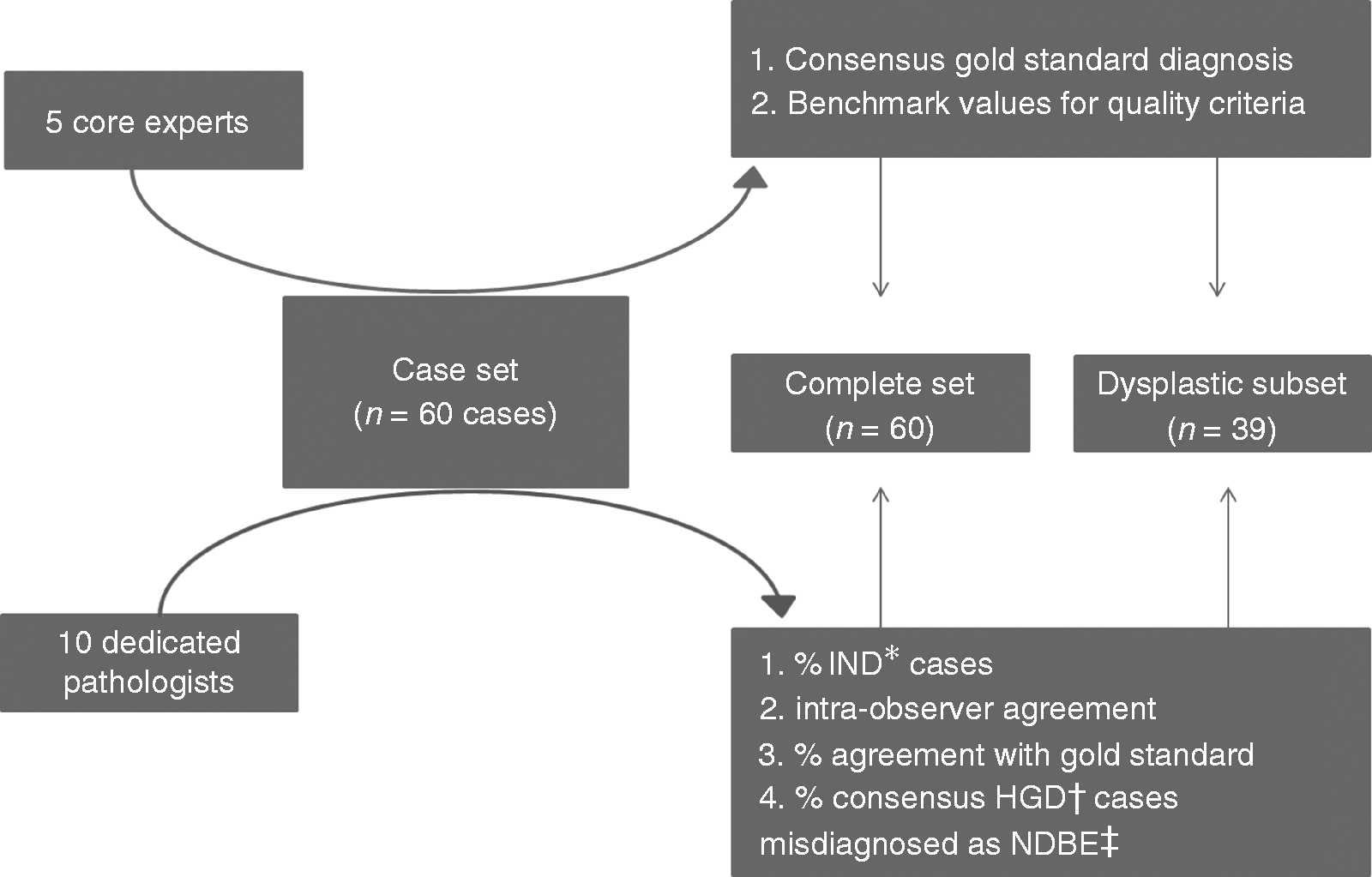
Outcome measurements
Per pathologist, we established whether the scores met all benchmark quality criteria, for the complete case set as well as for the dysplastic subset (Figure 2). The different outcome measurements were calculated as per our previous study.
16
Figure 2 illustrates the spectrum of diagnostic agreement, over- and underdiagnoses.
Example of 4 × 4 cross table of pathologist against consensus gold standard diagnosis, showing the position of agreement, overdiagnosis and underdiagnosis. IND: indefinite for dysplasia; LGD: low-grade dysplasia.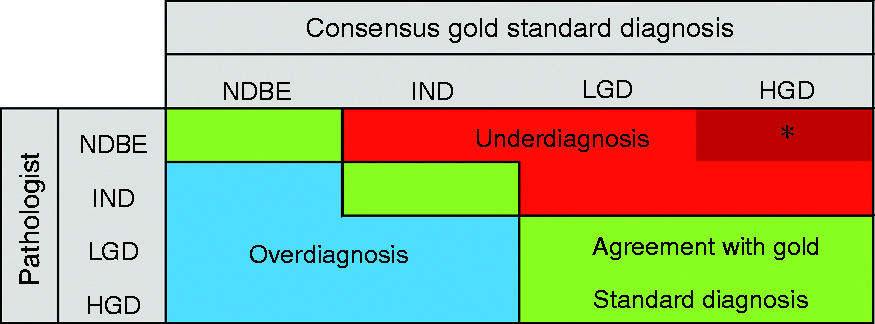
Results
Baseline characteristics of samples in case set
The median age of patients at diagnosis was 66 years (interquartile range (IQR) 13) and 73% were male. Cases contained a total of 151 sets of quadrant biopsies with a median of five slides (IQR 3–9), from a median of two levels (IQR 1–4) with four biopsies per level (IQR 3–4.5), with a total of 376 slides to be assessed.
Performance of 10 pathologists for the complete case series (n = 60)
The pathologists generated a total of 1200 case diagnoses over 7520 assessed slides. For the percentage of indefinite for dysplasia (IND) cases, eight out of 10 pathologists met the benchmark value (see Figure 3(a)). For the intra-observer agreement, nine out of 10 pathologists fell within the benchmark value (see Figure 3(b)). For the percentage agreement with the consensus gold standard diagnosis, five out of 10 pathologists fell within the benchmark value (see Figure 3(c)). For the consensus HGD cases misdiagnosed as NDBE, eight pathologists fell within the benchmark value (see Figure 3(d)). In Supplementary Material Table 1, these results are visualised in cross tables per pathologist compared to the consensus gold standard diagnosis. For the complete case set, five out of 10 pathologists met the benchmark values for all four criteria.
(a)–(d) Performance of 10 gastrointestinal pathologists relative to benchmark criteria, for the complete case set. (e)–(h) Performance of 10 gastrointestinal pathologists relative to benchmark criteria, for the dysplastic subset.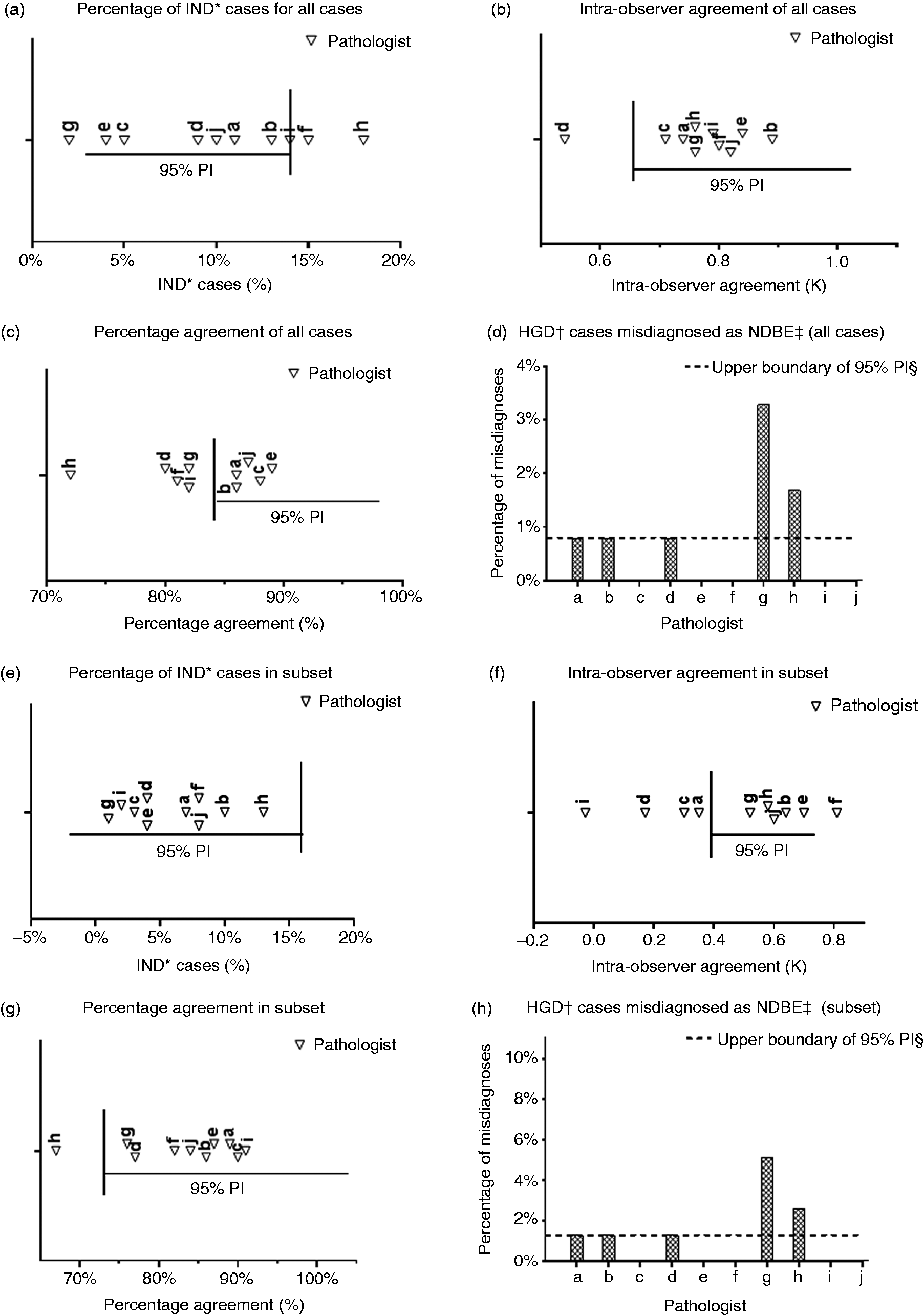
Performance of 10 pathologists for subset of dysplastic cases (n = 39)
For the percentage of IND cases, all pathologists fell within the benchmark value (see Figure 3(e)). For the intra-observer agreement, six out of 10 pathologists fell within the benchmark value (see Figure 3(f)). For the percentage agreement with the consensus gold standard diagnosis, nine out of 10 pathologists fell within the benchmark value (see Figure 3(g)). For the consensus HGD cases misdiagnosed as NDBE, eight out of 10 pathologists fell within the benchmark value (see Figure 3(h)). In Supplementary Material Table 2 these results are visualised in cross tables per pathologist compared to the consensus gold standard diagnosis. For the dysplastic subset, six out of 10 pathologists met the benchmark values for all four criteria.
Performance of pathologists relative to benchmark scores
Overall, three out of 10 pathologists met all benchmark values for the complete case set as well as for the dysplastic subset. When we extended our benchmark quality criteria by using a wider range, the 99% prediction interval (PI) scores of the five core pathologists, an extra three pathologists met the benchmark range (results not shown). Four pathologists did not meet the 99% PI benchmark range on one quality criterion, namely the intra-observer agreement of the dysplastic subset, or the percentage of HGD gold standard cases misdiagnosed as NDBE.
Discussion
The aim of this study was to test if 10 GI pathologists working at the eight BE expert centres in The Netherlands met pre-set benchmark scores of pre-defined quality criteria for evaluating BE biopsies (see Table 1), by assessing a case set of 60 BE cases consisting of 376 slides. To our knowledge, this is the first time that histopathological expertise has been quantified in the assessment of dysplastic BE biopsies. These criteria and benchmark values were established in an earlier study by using the assessments of five core expert BE pathologists as reference. These five pathologists are considered experts in BE diagnostics according to previously defined criteria: they have been dedicated to the field of BE for at least 15 years (range 15–45 years); have a median case load of seven cases per week (range 5–15), of which ≥25% are dysplastic; they participated in the Dutch Barrett advisory committee for 5–13 years12,19,20 and have co-authored more than 10 peer-reviewed publications in this field.12–17,19,21–30 To create a consensus gold standard diagnosis for this case set, these five core pathologists assessed the same dataset as used in this study, twice independently, followed by group discussions.
In the current study, the boundaries of the 95% PI and 99% PI of their individual scores were used as benchmark ranges to assess the performance of 10 dedicated GI pathologists working at the eight Dutch BE expert centers. These 10 pathologists have been dedicated to the field of BE with varying levels of experience (median of seven years (range 5–30), minimum case load of seven BE biopsies per week (range 5–17) of which ≥25% are dysplastic), however they did not have the intensive collaboration that the five core pathologists had. When comparing their assessments to the benchmark scores, we found that three out of 10 GI pathologists met all pre-set benchmark ranges for the quality criteria, for the complete case set as well as for the subset of dysplastic cases. Performance according to the benchmark range of the dysplastic subset is of key importance, since this subset is the main patient population for review requests by the national digital review panel. Their adherence to the benchmark ranges implies that these three pathologists perform similarly to the five core members in their diagnostic assessment. Expanding the digital revision panel with these three pathologists would therefore not compromise the current assessment homogeneity.
The results of our study need to be interpreted with caution. First of all, we have used intra-observer agreement (weighted kappa) as an indirect measure of expertise, because it underscores the individual reproducibility of the pathologist. However, calculating a kappa score can be less reliable when marginal totals are skewed, leading to a high chance of agreement and therefore a low kappa score. This is of particular relevance for the subanalysis of the dysplastic cases (where it is amplified by the low numbers in the subanalysis). Taking these aspects of the kappa calculation into account, we feel that the intra-observer agreement of the subanalysis is less reliable as a benchmark score than measuring diversions from the consensus gold standard diagnoses, i.e. the percentage agreement per pathologist. The percentage agreement of nine out of 10 pathologists falls within the 95% PI benchmark range for this criterion. This outcome signifies correct detection of dysplastic cases (Figure 3(g)). If we did not take the intra-observer agreement into account, one additional pathologist meets the predefined benchmark values. Second, the 95% PI benchmark range of percentage of cases ‘indefinite for dysplasia’ is inflated compared to clinical practice. This is explained by the fact that our case set was strongly enriched for difficult dysplastic cases, as encountered in a review panel setting, and by the fact that we used a p53 decision rule in the interpretation of p53 IHC as a diagnostic adjunct. 17 Moreover, the current study is part of a structured training programme and after the individual assessments presented here, the 10 GI pathologists participated in face-to-face plenary group meetings, discussing cases that were discrepant with the consensus gold standard diagnosis. Importantly, after completion of this study set, all pathologists have assessed a case set of 62 endoscopic resection cases, and are currently reviewing 40 cases sent to the national digital review panel. These assessments were again combined with face-to-face plenary group meetings, to discuss difficult and discrepant cases. This will further improve the experience and homogeneity of panel members. We aim to reevaluate their performance in the near future, and consequently expect more pathologists to meet the benchmark quality criteria presented here.
This study has some limitations. The benchmark quality criteria used in this study depend on the distribution of diagnoses in this dataset and the individual scores of the five core pathologists. The benchmark scores only apply to this specific digital study set and the number and scores of the core pathologists. However, because there is no standardized way to define expertise in BE diagnostics, we feel that these benchmark quality criteria are currently the best choice to quantify expertise when diagnosing BE dysplasia in biopsy samples in The Netherlands.
This study is unique because of a number of features. First, it is part of a structured approach to guarantee quality and uniformity of histological diagnosis of BE biopsies in The Netherlands. Over the past five years, our group has set up a national digital review panel for BE after conducting five preliminary studies.16,17,30 This is the first time worldwide that an expert pathology review panel has been set up conducting such quantifiable preliminary work in such a meticulous way. Second, the case set used for this study consisted of all slides from all biopsy levels of a single endoscopy (376 slides in total), was fully digitalized and only contained review cases from clinical practice. There were two assessment rounds with an adequate wash-out time. In order to improve homogeneity of the group the pathologists held a group discussion afterwards to discuss cases that did not have a majority diagnosis. This digital case set of dysplastic BE cases will be made available to allow pathologists in and outside The Netherlands to evaluate if they meet the aforementioned benchmark ranges for quality criteria.
Our goal for the future remains to improve the knowledge of BE-related diagnostic pathology among GI pathologists in The Netherlands; and to include all GI pathologists working at the BE expert centers in The Netherlands in our review panel. For this, we first need to ensure quality and homogeneity of the panel as outlined above. Subsequently, we need a prediction model that allows us to efficiently select the number of pathologists needed for reviewing cases and to divide the workload equally among panel members. We aim to improve and expand training in BE pathology both nationally as well as internationally by constructing a freely available, accredited training module incorporating the information gathered from all study sets and group discussions thus far.16,17,30 In this way, pathologists with an interest in BE can train themselves and reflect on their performance relative to the benchmark scores of the training set.
Supplemental Material
Supplemental material for Adherence to pre-set benchmark quality criteria to qualify as expert assessor of dysplasia in Barrett’s esophagus biopsies – towards digital review of Barrett’s esophagus
Supplemental Material for Adherence to pre-set benchmark quality criteria to qualify as expert assessor of dysplasia in Barrett’s esophagus biopsies – towards digital review of Barrett’s esophagus by MJ van der Wel, E Klaver, LC Duits, RE Pouw, CA Seldenrijk, GJA Offerhaus, M Visser, FJW ten Kate, K Biermann, LAA Brosens, M Doukas, C Huysentruyt, A Karrenbeld, G Kats-Ugurlu, JS van der Laan, G van Lijnschoten, FCP Moll, AHAG Ooms, JG Tijssen, JJGHM Bergman and SL Meijer in United European Gastroenterology Journal
V2 etc. research data Withdrawn
Research Data for Adherence to pre-set benchmark quality criteria to qualify as expert assessor of dysplasia in Barrett’s esophagus biopsies – towards digital review of Barrett’s esophagus
Research Data for Adherence to pre-set benchmark quality criteria to qualify as expert assessor of dysplasia in Barrett’s esophagus biopsies – towards digital review of Barrett’s esophagus by MJ van der Wel, E Klaver, LC Duits, RE Pouw, CA Seldenrijk, GJA Offerhaus, M Visser, FJW ten Kate, K Biermann, LAA Brosens, M Doukas, C Huysentruyt, A Karrenbeld, G Kats-Ugurlu, JS van der Laan, G van Lijnschoten, FCP Moll, AHAG Ooms, JG Tijssen, JJGHM Bergman and SL Meijer in United European Gastroenterology Journal
Footnotes
Acknowledgements
The following author contributions were made: study concept and design: MJW, EK, SLM, JJGHMB. Acquisition of data: MJW, CAS, GJAO, MV, FJWK, KB, LAAB, MD, CH, AK, GKU, JSL, GL, FCPM, AHAGO, SLM. Analysis and interpretation of data: MJW, EK, JGT, JJGHMB, SLM. Drafting of the manuscript: MJW, EK, LCD, REP, JGT, JJGHMB, SLM. Critical revision for important intellectual content and final approval of the manuscript: all authors. Study supervision: SLM, JJGHMB.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Ethical approval
Since the materials used in this study were anonymized, the medical ethical committee of the AMC waived the need for approval.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Informed consent
Since the materials used in this study were anonymized, the medical ethical committee of the AMC waived the need for obtaining informed consent.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.