
Abstract
Patients with diabetes have distinct risks during precolonoscopy bowel preparation, caused by change of diet, change of antihyperglycemic medication regimens and diabetes-related complications and comorbidities. These risks include hypoglycemia, water and electrolyte imbalance, acute renal failure, lactic acidosis, ketoacidosis and low quality of bowel preparation. Here we review the existing literature and present recommendations from a subcommittee of the Israeli National Diabetes Council for primary care physicians and gastroenterologists. The instructions include general suggestions on diet and glucose monitoring and specific recommendations on timing of modification or cessation of each of the antihyperglycemic medication types to ensure patient safety during bowel preparation.
Introduction
Colonoscopy is a common procedure in adults older than age 50 years, more than 10% of whom have diabetes. 1 Diabetes patients have a higher risk for complications during colonoscopy preparation caused by change of diet, concomitant presence of diabetes complications and comorbidities and untimely continuation or cessation of antihyperglycemic agents (AHAs). Neither American nor European diabetes and gastroenterology organizations have addressed the special concerns and needs of diabetes patients undergoing colonoscopy.
The only official guideline on this matter is a section on colonoscopy in the 2012 Australian Diabetes Society perioperative diabetes management guidelines. 2 These recommendations suggest stopping oral AHAs during the clear-fluid preparation phase, adding glucose as needed to clear fluids, and reducing the dose or replacing insulin injections. An elaborate and somewhat complicated insulin replacement regimen is suggested, with a comment that patients who have unstable glycemic control should be hospitalized during bowel preparation. These guidelines do not address the different AHAs.
Unfortunately, there are no studies on the safety and preferred regimen of AHAs (including almost all insulin types) prior to and during colonoscopy. Nevertheless, physicians and patients alike need practical and clear instructions, even if based only on expert opinion and the known pharmacokinetic and safety profiles of the different AHAs.
During the first quarter of 2018, a subcommittee of the Israeli National Diabetes Council including endocrinologists, gastroenterologists, diabetes nurses and dietitians convened to create a position statement clarifying diabetes-specific issues and changes to AHAs during precolonoscopy bowel preparation. The position statement was written as a short handout for primary care physicians and gastroenterology clinics. The recommendations were endorsed by the Israeli National Diabetes Council, the Israeli National Gastroenterology Council, the Israeli Gastroenterology Association and the Israeli Medical Association.
Here we review the limited literature on colonoscopy in diabetic patients and present the Israeli position statement recommendations on precolonoscopy bowel preparation in diabetic patients.
Risk of AHA-associated complications during colonoscopy preparation in patients with diabetes
Potential effects and adverse reaction of AHAs on colonoscopy preparation.
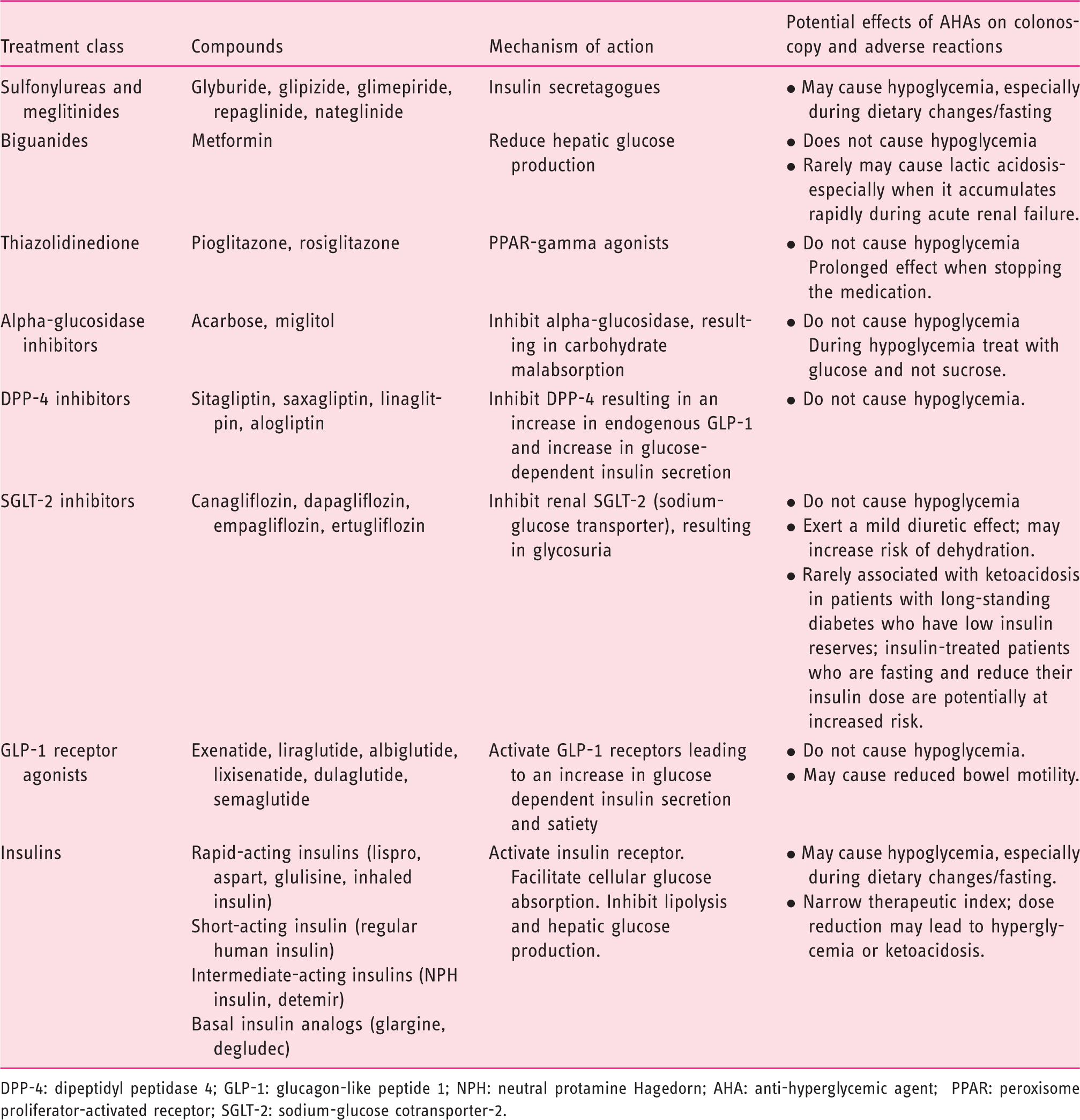
DPP-4: dipeptidyl peptidase 4; GLP-1: glucagon-like peptide 1; NPH: neutral protamine Hagedorn; AHA: anti-hyperglycemic agent; PPAR: peroxisome proliferator-activated receptor; SGLT-2: sodium-glucose cotransporter-2.
Hypoglycemia
In the low-fiber diet phase, patients are instructed to consume refined carbohydrates. Patients who are accustomed to avoiding refined carbohydrates because of their high glycemic index may significantly reduce their carbohydrate intake without a concomitant adjustment of their AHAs, thus increasing the risk for hypoglycemia. The clear-liquid diet phase is generally hypocaloric even when sugary juice and tea are consumed, and patients who continue their habitual avoidance of sugar-sweetened beverages will consume no carbohydrates. Insulin secretagogues are likely to cause hypoglycemia in the liquid diet and cathartic day prior to colonoscopy or the day of the procedure and should be discontinued. Sulfonylurea preparations with a very long half-life can cause hypoglycemia even when taken more than 24 hours before the test and should be discontinued from the morning of the day prior to the test. Likewise, insulin dose (long-acting basal preparations as well as short-acting insulin) should be adjusted.
The clear-liquid diet before colonoscopy has not been shown to lead to superior bowel cleansing compared with a low-fiber diet, 4 and there is sufficient evidence to strongly recommend a low-fiber diet the day before a colonoscopy, avoiding the liquid-diet phase. This recommendation has been incorporated into the international guidelines3,5 and to the recommendations from the United States Multi-Society Task Force on Colorectal Cancer. 6 Those recommendations were made with moderate-quality evidence at the time of publication of those guidelines, but the evidence has grown stronger in the following years. The recommendation, especially for diabetic patients, should be to avoid a liquid diet and consume a low-fiber diet the day before the colonoscopy including the morning of an afternoon or evening colonoscopy. Avoiding fasting and a hypocaloric liquid diet as much as possible is the key to avoiding complications during bowel preparation in diabetic patients.
Dehydration, electrolyte imbalance and acute renal failure
The cathartic phase leads to significant diarrhea and in some patients, nausea and vomiting, which together may result in dehydration and electrolyte imbalance. In susceptible individuals with preexisting diabetic nephropathy and renal dysfunction, this may result in acute kidney injury and worsening renal function.7,8 The incidence of acute kidney injury is much higher after use of oral sodium phosphate solutions compared with oral sulfate solutions. 8 Hyponatremia is more common with sodium picosulfate preparations in older adults, 9 and polyethylene glycol (PEG) is the cathartic of choice in patients with renal failure.3,8 Use of PEG preparations should be considered in all patients with diabetes because of their increased risk for developing kidney injury and electrolyte imbalances.
Metformin-induced lactic acidosis
In acute renal failure, metformin—the essential first-line AHA in type 2 diabetes—may accumulate rapidly and result in life-threatening lactic acidosis. 10 Several cases of metformin-induced lactic acidosis have been reported in patients with acute renal failure who continued their metformin treatment during the aggressive cathartic phase.11–13
Hyperglycemia
Owing to concerns about hypoglycemia, some primary care physicians or gastroenterologists recommend halting or reducing the dose of antihyperglycemic therapy for several days. A prolonged interruption of treatment can lead to hyperglycemia-induced osmotic diuresis, which may worsen dehydration. Therefore, optimal timing for each medication should be aimed at halting or reducing the dose. 14
Fasting and insulin-deficiency–induced ketoacidosis
The combination of a hypocaloric diet followed by fasting, accompanied by a discontinuation or significant reduction of insulin treatment, may result in ketosis and an increased risk of ketoacidosis. The risk is greater in patients with type 1 diabetes who are completely dependent on exogenous administration of insulin,15,16 but may also occur in insulinopenic patients with type 2 diabetes who rely on exogenous insulin in addition to other AHAs.
Sodium-glucose cotransporter 2 inhibitor (SGLT-2i)-induced ketoacidosis
SGLT-2i are a new group of AHAs rapidly gaining popularity because of their cardio- and renoprotective effects. 10 SGLT-2i therapy has been associated with an increased risk of diabetic ketoacidosis (DKA), sometimes presenting without significant hyperglycemia both in type 1 and type 2 diabetes patients. Many of the reported cases of SGLT-2i–associated DKA events have been provoked by stressful physical and medical conditions, including prolonged fasting. While there have been no reports of SGLT-2i–induced ketoacidosis during precolonoscopy preparation, considering the combination of the low-calorie diet, fasting and increased risk of dehydration, this is a real concern. These medications should therefore be suspended the day before the procedure. 17
Risk of poor bowel preparation in patients with diabetes
Multiple studies have demonstrated that patients with diabetes have worse bowel preparation, frequently requiring a repeat colonoscopy.18,19 The higher risk for inadequate preparation does not depend on age, glycemic control or a prior diagnosis of diabetic neuropathy. 20 Possible mechanisms for this phenomenon may include colon dysmotility secondary to diabetic neuropathy, 21 reduced physical exercise because of comorbidities, and medications that slow bowel motility and cause constipation such as antihypertensive medications. Whereas glucagon-like peptide 1 (GLP-1) agonists slow bowel motility 22 and could potentially increase the risk of poor bowel preparation, a single study found no evidence of worse bowel preparation when comparing diabetic patients treated with GLP-1 agonists or other medications. 23 Despite these observations, current guidelines do not advocate different preparation regimens for diabetic patients.3,22
A potentially beneficial intervention is meticulously detailing each meal and snack during the precolonoscopy preparation, restricting the clear-liquid diet to eight hours before the colonoscopy, and allowing breakfast the day of an afternoon colonoscopy. This has been shown to reduce inadequate bowel preparation from 20 % to 7 %. 24
A single-center retrospective analysis of colonoscopy results in more than 1000 diabetes patients found that a change of scheduling of screening colonoscopy from early morning (7:30–9:30 a.m.) to mid-morning (after 9:30 a.m.) in patients with diabetes without end-organ complications decreased the frequency of inadequate bowel preparation from 7.7% to 3.2% in a logistic regression model that adjusted for the independent effects of age and gender afterward. 25 This improvement can probably be attributed to the increased likelihood of completing the second cathartic dose the morning of the colonoscopy, which in mid-morning procedures was recommended the morning of colonoscopy. 25
Summary and practical recommendations
To prevent the risk of hypoglycemia, hyperglycemia and ketoacidosis lactic acidosis, and to improve bowel preparation in people with diabetes, clear guidelines should be provided regarding diet, medication timing and glucose monitoring:
Diet
To reduce the risk of hypoglycemia and hyperglycemia, patients should be instructed to avoid significant changes in carbohydrate consumption while eating a low-fiber diet, and to include a combination of a carbohydrate and protein in each meal (i.e. egg/chicken/fish with white bread/peeled potato/white rice). Providing detailed dietary instructions is recommended. As for all patients undergoing colonoscopy, it is important to emphasize that the clear-liquid phase should include not only water but also liquids containing electrolytes such as broth and clear juice.
The current guidelines were approved by the Israeli Diabetes and Gastroenterology councils. A recommendation for a liquid diet remained in the Israeli colonoscopy preparation guidelines. Owing to emerging evidence, however, the authors of this manuscript strongly recommend avoiding a liquid diet in patients with diabetes the day before the colonoscopy and allowing a low-fiber breakfast the morning of an afternoon colonoscopy.
Timing of the procedure
Although early-morning colonoscopy shortens the period of fasting and AHA change and could potentially reduce the occurrence of hypoglycemia and hyperglycemia, there is no evidence supporting early-morning scheduling. There is evidence that mid-morning scheduling (after 9:30 a.m.) improves bowel preparation in patients with diabetes as it facilitates the adherence to a split-dosing of the laxative. An afternoon scheduling of the colonoscopy is also possible if diabetic patients are allowed to eat a low-fiber breakfast.
Antihyperglycemic medications
Suggested instructions for antihyperglycemic medication precolonoscopy.
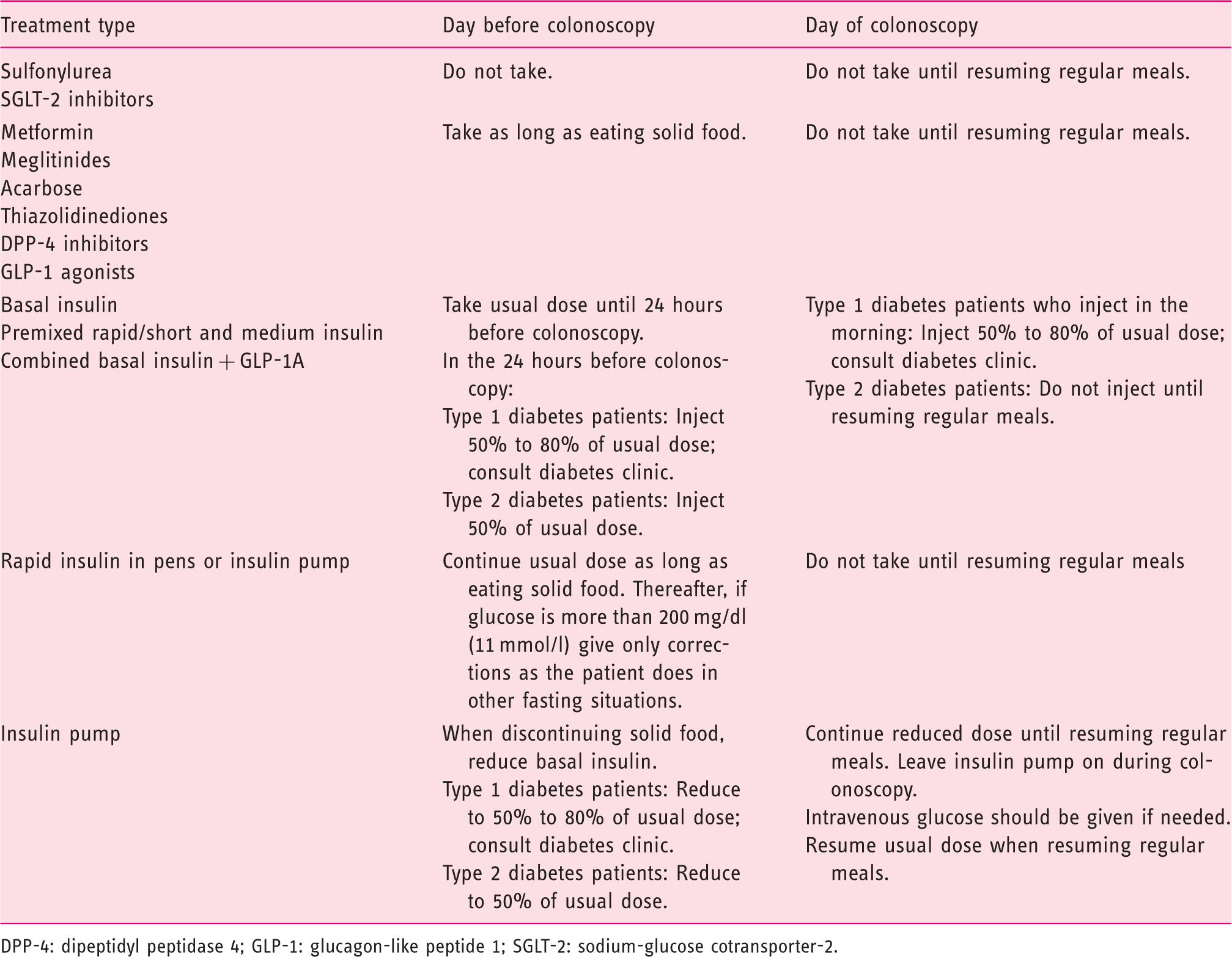
DPP-4: dipeptidyl peptidase 4; GLP-1: glucagon-like peptide 1; SGLT-2: sodium-glucose cotransporter-2.
Glucose monitoring
The day before the colonoscopy and the day of the procedure, patients should frequently monitor their glucose levels. Insulin-treated patients should monitor their glucose at least every four hours from the last solid meal until resuming eating after the colonoscopy.
Footnotes
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.