
Abstract
Background
Indications for endoscopic retrograde cholangiopancreatography (ERCP) in children differ from adults. Paucity of data and concerns about potential lower effectiveness and more side effects limit its use even in high volume centers. We retrospectively analyzed indications, success rates, limitations, and side effects of ERCPs in children <18 years.
Methods
From January 2012 to March 2015, 54 ERCPs were performed in 31 children (median age 11 (0–17) years; median weight 22 (3.3–142.7) kg) with suspected choledocholithiasis (n = 13 interventions in 9 patients), post-transplantation anastomotic stenosis (10/4), malignancy (10/5), chronic pancreatitis (7/1), biliary atresia (6/6), anomaly (2/2), leak (4/3), or primary sclerosing cholangitis (PSC) (2/1). All patients were followed up as inpatients.
Results
Thirty-six therapeutic and 18 diagnostic procedures were performed by adult ERCP expert endoscopists. Successful intervention was achieved in 90.7% of cases. Failed cannulation (n = 4) was associated with lower body weight (p = 0.023). In children younger than 1 year, ERCP was significantly more often diagnostic than in patients >1 year (p < 0.001). In three of six infants with suspected atresia, surgical exploration was avoided. Five complications were recorded (9.3%), and included four episodes of mild pancreatitis (7.4% post-ERCP pancreatitis (PEP) rate) and one cholangitis in PSC. A trend towards a protective effect of pancreatic stents on PEP was observed. All complications were managed conservatively. No complications were attributed to mechanical stress on the gastrointestinal tract.
Conclusions
ERCP in newborns, infants, and adolescents can be safely performed with high technical and clinical success. Endoscopists must be aware of differing spectrum of pediatric diseases. Failed cannulation was associated with lower body weight of young children. Complications were similar to rates reported in adults.
Keywords
Introduction
Endoscopic retrograde cholangiopancreatography (ERCP) is an advanced endoscopic technique that is well established for diagnosis and treatment in biliary and pancreatic disorders in adults but is associated with a relatively high adverse event rate. 1 It is increasingly, but not commonly, used in the workup of pediatric biliopancreatic disorders. Its conservative use in children is a result of the paucity of data on pediatric ERCP, concerns about effectiveness and safety, and ongoing debate on the examiner’s qualification. Frequently, pediatric ERCPs are performed by adult gastroenterologists with high technical expertise, but less familiarity with pediatric diseases. Series on pediatric ERCP published since 2010 cover a wide range as to age (<3 months to <21 years) and indications,2–13 and subsequently analyzed 27–432 procedures retrospectively. ERCPs were performed by either adult or pediatric endoscopy specialists. Combined analyses report outcomes comparable to the adult population, 14 although with variable success rates of 70–100%. Children-specific recommendations on minimizing adverse events, which are usually extrapolated from the adult population, 1 may include prophylactic rectal nonsteroidal anti-inflammatory drugs (NSAIDs) or prophylactic pancreatic duct stenting. However, a single large series reported a negative effect of prophylactic pancreatic duct stenting on post-ERCP pancreatitis (PEP) rates. 7
We retrospectively analyzed pediatric ERCPs performed in our high-volume interdisciplinary endoscopy department.
Patients and methods
Patients and setting
In our tertiary care center, the pediatric gastroenterology and hepatology unit offers an in- and outpatient service for children of all ages suffering from gastrointestinal, liver, or pancreatic diseases. Care for these children is organized in multidisciplinary teams, including a full-range endoscopy service and pediatric and transplantation surgery programs including liver and intestinal transplantation. ERCPs were performed by adult ERCP expert endoscopists (MG, FG, DS) with attending pediatricians on-site, whenever necessary.
Pediatric patients who underwent ERCP were identified from our database. From January 2012 to March 2015, 54 ERCPs were performed in 31 children (female:male 16:15, including one previously published technique-related case).
15
Patients were between 3 weeks and <18 years old (mean age 7.6 ± 6.1 years, median age 11 (range 0–17) years) (Figure 1). Patients underwent a median of one intervention (range 1–7). Median weight was 22 kg (range 3.3–142.7 kg). Indications for ERCP were suspected choledocholithiasis (n = 13 interventions in 9 patients, 13/9), anastomotic stenosis after liver transplantation (10/4), malignant stenosis (10/5)), chronic pancreatitis with dominant dorsal duct syndrome (7/1), biliary atresia (6/6) or anomaly (2/2), postoperative or traumatic biliary leak (4/4), or primary sclerosing cholangitis (PSC)-associated stenosis (2/1) (see Supplementary table 1 online). High-end ultrasonography and/or cross-sectional imaging was available for all patients before ERCP. Infants with suspected biliary atresia were evaluated by ERCP if other diagnostic means were non-conclusive and more detailed information on bile-duct integrity was needed to plan a therapeutic concept including the Kasai procedure (see Supplementary table 2 online). All children were routinely followed up as inpatients for at least two days. The retrospective chart analysis was approved by the ethics committee of the University of Tübingen (No. 265/2015R).
Patient’s age and number of procedures performed in each age group.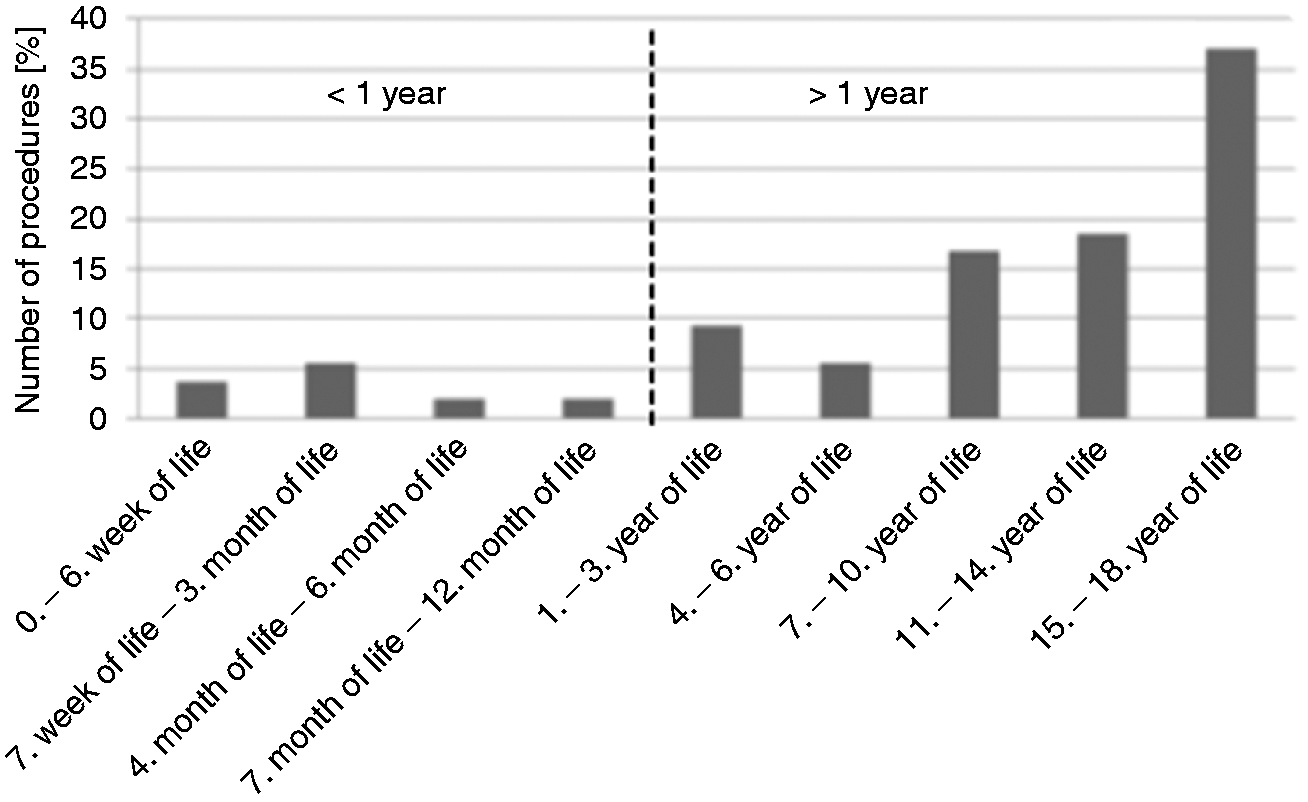
Intervention and accessories
The following duodenoscopes were used: TJF140R, TJFQ180V, TJF160VR, PJF160 (Olympus, Tokyo, Japan), and 34i10E (Pentax, Tokyo, Japan). Sphincterotomes were chosen according to the working channel size and included Standard Cannulation CT-II (Cook Medical, Winston-Salem, NC, USA), Dash Set Children Papillotome (Cook), Billroth Papillotome (Cook). Similarly, guidewires of 0.035″ (Jagwire, Boston-Scientific, Ratingen, Germany), 0.025″ (Boston-Scientific), and 0.018″ (Boston-Scientific) were used. All first-time comers underwent gastroscopy immediately before ERCP.
Success of the intervention was defined as allowing accurate diagnosis and/or adequate therapy as to the pre-specified indication. Details are given online in Supplementary table 1. PEP was graded according to the revised Atlanta classification (mild, moderate, severe). 16 No routine PEP prophylaxis was performed in our cohort, but was recommended or performed according to the examiner’s recommendation in some patients with difficult access and included pancreatic stents (n = 6) or rectal diclofenac (n = 1).
Statistics
Evaluation of success was based on assessment of interventions (i.e. n = 54 correspond to 100%). Statistical analysis was performed with SPSS (IBM SPSS Statistics, Version 20). Two-sided Fisher’s exact test was performed for correlation of body weight with success of the intervention and correlation of age (< vs. >1 year) with diagnostic vs. therapeutic ERCP. A p-value ≤0.05 was considered significant.
Results
Interventions
Pediatric ERCP accounted for 3.3% of our total ERCP caseload. General anesthesia was preferred. A typical setting is shown in Figure 2. Only in 6/54 interventions (in 16- to 17-year-olds) was conscious sedation used. In two patients, retrograde access to the papilla was necessary after Roux-en-Y anastomosis, and via duodenostomy (in ultra-short bowel syndrome, Figure 2(c)). ERCP was finished as therapeutic ERCP in 36 interventions (66.7%) and as diagnostic in 18 (33.3%). In patients younger than 1 year, ERCP was significantly more often diagnostic (9 diagnostic vs.0 therapeutic ERCPs) than in children >1 year (7 vs. 38, respectively; p = 0.000002).
A) typical setting of ERCP for infants; B) ERCP in a newborn for exclusion of biliary atresia; C) ERCP via duodenostomy for suspected choledocho- and pancreaticolithiasis prior to cholecystectomy in cholecystolithiasis in a 12-year-old girl with ultra-short-bowel syndrome. A mild stenosis of the distal CBD is treated by bouginage, a pancreatic wire was subsequently used for pancreatic stent insertion.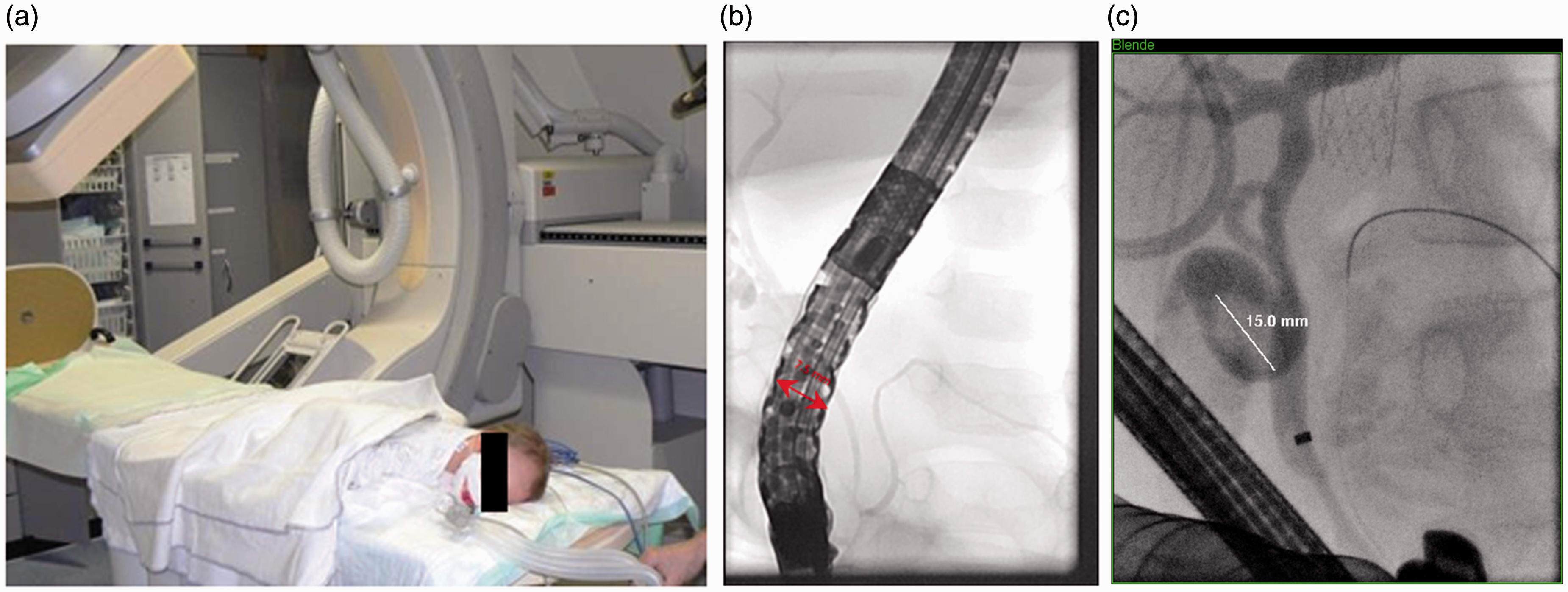
Endoscopic sphincterotomy was performed in 16/54 examinations. Diagnosis after ERCP was anastomotic stenosis after liver transplantation (n = 10), malignant stenosis (10), choledocholithiasis (9), normal duct system (8), pancreatic dominant dorsal duct syndrome (7), biliary atresia (3) or anomaly (2), biliary leakage (3), and stenosis in PSC (2) (Supplementary table 1).
A total of six infants were evaluated for biliary atresia. In three of six infants, patent bile ducts could be demonstrated by ERCP, and laparotomy was cancelled. In the remaining three, the bile duct system could not be contrasted. In all three of these patients, biliary atresia or hypoplasia was confirmed through intraoperative cholangiography (Supplementary table 2).
Successful intervention was achieved in 90.7% (49/54 ERCPs), and was more often achieved in older children (mean 10.9 vs. 4.2 years for success vs. failure) and/or higher weight (median 34.0 vs. 8.3 kg). Failed cannulation (n = 4) was associated with lower body weight (p = 0.023). In one patient, wire access was achieved, but cholecystectomy instead of endoscopic therapy was performed in microlithiasis and difficult anatomy.
Endoscopes and accessories
Standard adult duodenoscopes were used in children >12.5 kg, pediatric duodenoscopes (PJF160, outer diameter 7.5 mm, working channel 2 mm) in smaller children. No complications were noted secondary to endoscope-patient size mismatch. In some of the smallest children, 5Fr bougies which permit closer working distance to the papilla and smoother lever manipulation at their tip were used to intubate the papilla, and all attempts were successful, whereas two intubation attempts in very small children using pediatric sphincterotomes failed.
Adverse events
Continuous clinical follow-up was available for all patients (100%) for at least 48 hours. Complications were recorded after five of 54 procedures (9.3%), and included four episodes of mild pancreatitis (fever, elevation of lipase, abdominal pain), correlating to a 7.4% PEP rate and including two episodes of aggravation of preexisting recurrent acute pancreatitis (Figure 3). No episodes of moderate or severe PEP were recorded. PEP was noted in none of six children having received a protective pancreatic stent vs. 4/43 without pancreatic stents (n.s.). PEP did not correlate with pancreatic duct intubation, contrast injection, or sphincterotomy (n.s.).
Complications associated with ERCP procedures. Procedure-related complications were rare.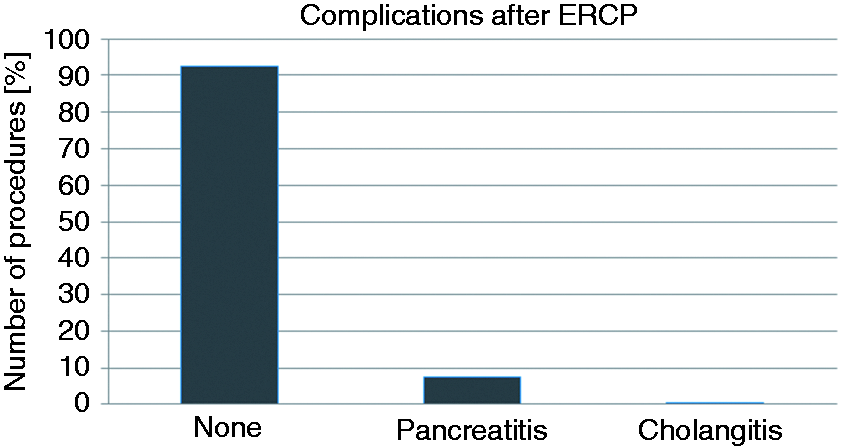
In addition, aggravation of cholangitis (fever, transient further rise in liver serum tests) was seen in one PSC patient despite antimicrobial prophylaxis (tazobactam/piperacillin). All complications were managed conservatively (fasting, analgesia, modification of antimicrobial therapy). A complication-associated prolongation of length of in-hospital stay was recorded in one patient. No complications attributable to mechanical stress on the gastrointestinal tract and no bleedings, perforations or cardiopulmonary complications were observed. Radiation dose was not evaluated due to the use of three different fluoroscopy units by three endoscopists during the observation period.
Discussion
In our experience, ERCP in newborns, infants, and adolescents can be safely performed with a high technical and clinical success rate. This adds to the growing evidence supporting the use of ERCP by skilled endoscopists in this age group. Indications in our series covered a wide range representative for a tertiary care center with a specialist pediatric gastroenterology and hepatology unit, and active liver and bowel transplantation programs as well as high end endoscopic services. Indications differ greatly within this specific population, as was expected: Indications in adolescents were comparable to adult ERCP, and mainly included choledocholithiasis, 6 liver transplantation-related disorders, and malignant disease. In contrast, the main indication in newborns was diagnostic workup of neonatal cholestasis and suspected pancreaticobiliary maljunction. ERCP has recently been shown to be significantly superior to MRCP for visualization of the main pancreatic duct (PD) and pancreaticobiliary ductal union. 13 In these circumstances, where laparotomy may be contemplated and anatomical information from less-invasive imaging modalities is inconclusive, ERCP is specifically useful to rule out biliary atresia/pancreaticobiliary maljunction. Our series, which confirms prior work, 17 shows that laparotomy for Kasai’s procedure was avoided in 50% of infants with suspected biliary atresia. Diagnostic ERCP correctly confirmed or excluded the indication for surgery in all patients, although our overall numbers in this age group are small.
In our series a greater proportion of diagnostic ERCPs of 33.3% and lower therapeutic ERCP rate of 66.7% was recorded than is usually found in the adult population where ERCP is almost exclusively performed with therapeutic intention. This diagnostic rate is in accordance with previous series on pediatric ERCP, reporting therapeutic ERCPs in 64.1% to 81.3% of cases.3,4,10,12 Similarly, the success rate of our series of 90.7% is in the lower range of most adult series.18,19 We defined success not only as success of deep papillary cannulation but as procedural success of delivering adequate diagnosis and/or therapy in response to the clinical scenario. In addition, needle knife papillotomy was usually not performed in cases of diagnostic ERCPs and if the narrow gastrointestinal (or working channel) lumen did not allow safe navigation for precuts. We found failure rates to be mainly associated with low body weight. Similarly, Shteyer et al. reported ERCP failure in 5/27 babies (18.5%) ≤3 months with biliary atresia and biliary stones. 5 Success rates were associated with older age in a series by Saito et al. (92% <3years, 100% >3 years). 11
Pediatric ERCP can be safely performed by specialized pediatricians, 6 but also adult-trained endoscopists. 8 In our experience it is specifically helpful to coordinate findings and further therapeutic steps with the attending pediatrician not only before and after ERCP but also during the procedure itself. We consider this setting a prerequisite for ERCPs in this age group when adult-trained endoscopists may not be intimately familiar with specific pediatric diseases such as biliary atresia or different subsets of pancreaticobiliary maljunctions or choledochal cysts. We used a small diameter pediatric duodenoscope (PJF160) for children <12.5 kg which is in accordance with current ASGE recommendations. 20 This duodenoscope is available for immediate use in our center but can also be obtained for loan on a case-by-case basis. The small working channel makes therapeutic ERCP more challenging as only specialized equipment and small caliber stents (up to 5Fr) are accepted. In addition, the space for navigation in front of the papilla is often limited in small children. In this context, we found the use of a 5Fr bougie (with a 0.018″ wire) for intubation specifically helpful since its soft tip allows for a closer and more subtle navigation at the diminutive papilla of a young infant. Most of our pediatric ERCPs were performed in prone position under general anesthesia to minimize adverse events on the airways which are softer in children and more easily compressed in case of an unfavorable scope/patient size mismatch.
Clinical follow-up was available for 100% of our cohort for two days, and no severe adverse events were recorded. The total percentage of complications is in line with former reports (0–10%).2–4,7,11 Mild episodes of PEP were found after four interventions (which is slightly more frequent than our own safety monitoring data of adult patients showing PEP rates of 3–4% after biliary sphincterotomies). Interestingly, as opposed to a large series on PEP in children, 7 we found a non-significant trend towards a protective effect of PD stenting, similar to the adult population, 1 and found two episodes of mild PEP in a patient with recurrent acute pancreatitis attributed to PD maljunction whereas a negative association of PEP with pancreatic disease in pediatric patients has been previously described.7,9 Rectal NSAIDs were not frequently administered in our cohort. The paucity of data on pediatric PEP prophylaxis in comparison to adults mandates further evaluation in this specific age group. Exacerbation of cholangitis in one PSC patient despite adequate antimicrobial prophylaxis underlines the need for close follow-up secondary to the risk of lack of complete drainage. We did not find any episodes of bleeding, perforations, ileus, or sepsis, all of which have been described in selected cases previously, although delayed complications after discharge cannot be formally excluded.
In summary, our cohort demonstrates that ERCP can be performed safely and with high success rates by advanced adult-trained endoscopists. Age-, disease-, and technique-specific considerations mandate an interdisciplinary setting. The percentage of diagnostic procedures was higher in younger children. The overall rate of adverse events was low, and no serious adverse events occurred. This underlines the beneficial impact of ERCP in a pediatric cohort.
Footnotes
Acknowledgement
Aspects of this work were presented at international meetings (DDW 2016, ESPGHAN 2016, UEGW 2016), and are part of the thesis by JF.
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.