
Abstract
Introduction
Endoscopic retrograde cholangiopancreatography (ERCP) is an important diagnostic and therapeutic modality for pancreatic and biliary disorders. Perforation is one of the most dreaded complications of ERCP. Since it is uncommon, there has been little study of incidence, risk factors, and outcomes of management.
Objectives
We aim to assess the incidence of ERCP-related perforations and outcomes at a large tertiary referral center.
Methods
We undertook a review of an ERCP database for all perforations from 2002 to December 2012.
Results
The cumulative incidence of ERCP-related perforations was 0.14% (12 out of 8264), and sphincterotomy-related perforations constituted the most common cause. The mean age of these 12 patients was 58.6 years and majority were female (83.3%). The most common indications for ERCP were: suspected sphincter of Oddi dysfunction (SOD) 41%, and common bile duct stones (CBD stones) 41%. Nine of the 12 patients (75%) had a leak and were managed medically, and four who had a perforation had surgical repair (25%).
Conclusions
In our study, leaks were much more common than perforations and the majority of patients were successfully managed with conservative therapy alone. We report a very low perforation rate and most perforations can be managed conservatively with a good outcome.
Introduction
Endoscopic retrograde cholangiopancreatography (ERCP) is an important diagnostic and therapeutic modality for pancreatic and biliary disorders. With the availability of non-invasive imaging techniques such as magnetic resonance cholangiopancreatography (MRCP) and endoscopic ultrasonography (EUS), ERCP has become primarily a therapeutic procedure. 1 While relatively safe, ERCP is still associated with complications, most commonly pancreatitis, post-sphincterotomy bleeding and perforation.2,3 Perforations are one of the most dreaded complications of ERCP, with a reported incidence of 0.3–6%;3–7 however, this data has come from retrospective database studies, case series or older studies. Studies from large prospective databases or from large tertiary centers in the current era of therapeutic ERCP are few.1,2,5
There is no consensus on the management of post-ERCP perforations. Current data is important to examine, as ERCP has evolved to be mainly a therapeutic procedure. In addition, data on outcomes and complications is essential to establish current prevalence and incidence rates, standards for quality indicators and risk factors for perforation. Thus, the primary objectives of this study were to assess the incidence, characteristics and outcomes of ERCP-related perforations at a large, tertiary medical center, where a high volume of ERCPs are performed per year, over a 10-year period in the new millennium.
Patients and methods
Since 1 January 2002, we have entered all patients undergoing ERCP into a prospective database.
When a patient is referred to our center for an ERCP procedure, the staff, after scheduling the patient for the procedure, also save the patient information in the database. The data collected contains information on patient demographics, indication for the procedure, radiological and laboratory data, endoscopic findings, and interventions and referring physician’s information. We also prospectively track all complications through a trained nurse coordinator who follows up all patients or caregivers on day 1 and day 30 after the procedure. The patients are also informed to call with any abdominal pain, fever, nausea/vomiting, etc. During the period of study, all procedures were performed by a total of five experienced therapeutic endoscopists.
We reviewed the database for all perforations from 2002 to December 2012. For all identified patients, computerized medical records and any additional records were further reviewed to ensure complete medical information and follow-up. The following data was extracted from the database and medical records for our study: the patient’s demographics, ERCP indication, findings during ERCP, time of diagnosis of perforation (intraprocedure vs. post-procedure), clinical and radiological presentation of the perforation, diagnostic methods, time to diagnosis and surgery, location of the duodenal leak if identifiable, methods of management, surgical procedures performed, complications, length of hospital stay and patient outcomes. We defined perforation as the presence of air or oral contrast in the retroperitoneal space with or without frank visualization of the peritoneum during the procedure. 4 Leak was defined as no extravasation of oral contrast but presence of intraperitoneal or extraluminal air on abdominal imaging in an otherwise asymptomatic or minimally symptomatic patient. This study was approved by our institutional review board as a part of our long-term prospective ERCP database (X030409001).
Statistical analysis
Means and proportions were calculated using SAS software, version 9.3 (SAS Institute Inc., CARY, NC).
Results
Demographics of the patient population
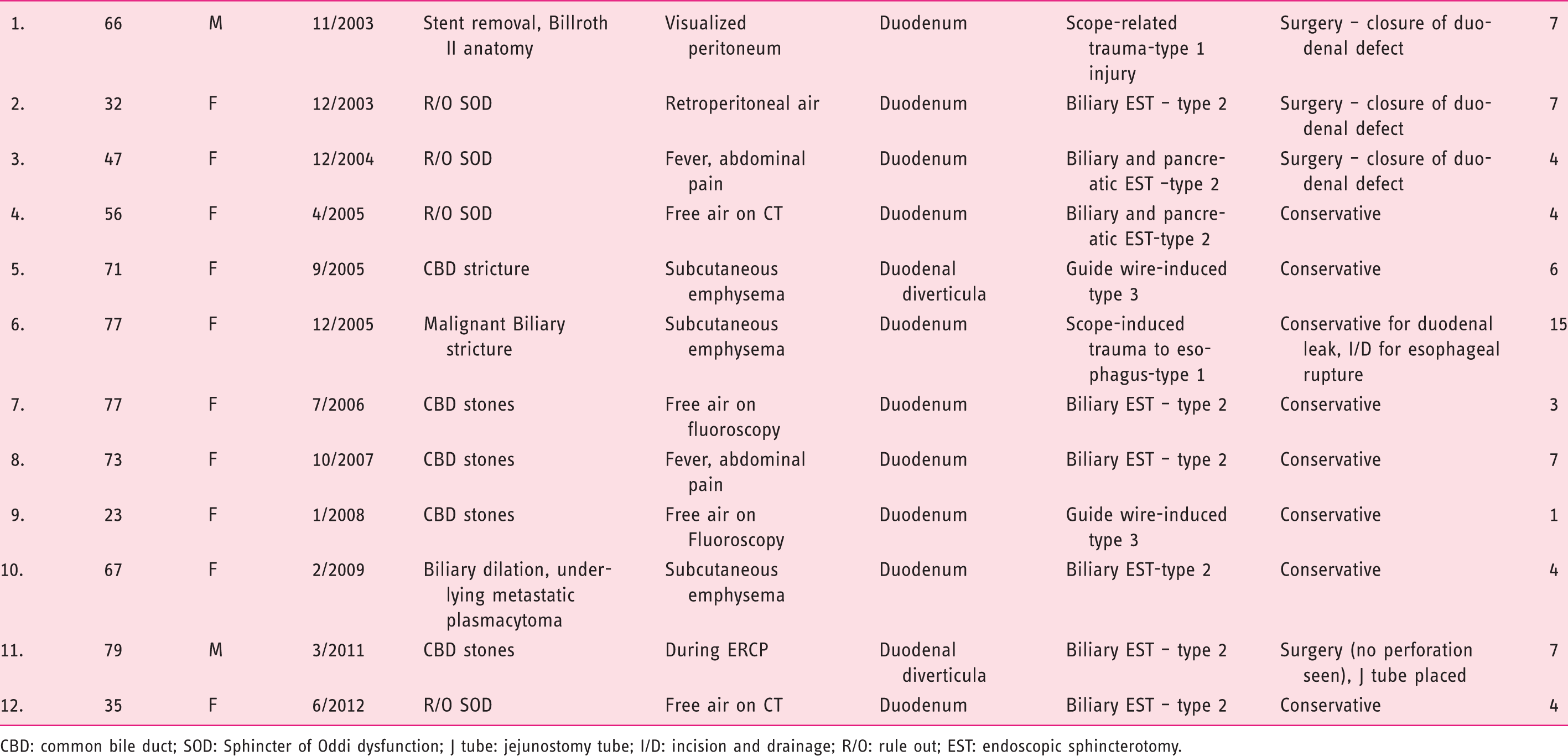
CBD: common bile duct; SOD: Sphincter of Oddi dysfunction; J tube: jejunostomy tube; I/D: incision and drainage; R/O: rule out; EST: endoscopic sphincterotomy.
Of the two with scope-related perforation, one patient suffered from esophageal perforation and another patient with Billroth II anatomy suffered from a perforation of the afferent limb. Endoscopic closure of the perforation site was not performed in any patient, and most commonly the diagnosis was made after the procedure (n = 7, 58.3%) or the patients were felt not amenable to endoscopic intervention and needed surgery. Nine of the 12 patients (75%) were managed medically and four surgically. All of the patients who were managed medically improved with conservative therapy and were discharged home. Overall, the mean hospital stay was 5.8 days (range 1–15 days). There were no deaths related to ERCP perforations.
Clinical features and diagnosis
Duodenal perforation/leak was observed during the procedure in six patients and a leak was diagnosed after the procedure in one patient who developed subcutaneous emphysema. The peritoneum was visualized in one patient with Billroth II anatomy of the afferent limb during the procedure, who was immediately taken to the operating room.
Overall, duodenal leak was diagnosed in six patients; three patients developed subcutaneous emphysema (one also had air around the kidneys) and three showed intra-abdominal free air. All of these patients were stable hemodynamically throughout the hospital stay and none developed peritoneal signs.
Two patients presented within 24–36 h after the procedure to the emergency room with abdominal pain and fever and were found to have free air on CT scan and had oral contrast extravasation.
Management and outcome
Eight patients, all without contrast leak and with no frank perforation, were managed conservatively with intravenous fluids, antibiotics and analgesics; some patients had nasogastric suction. All of these patients had clinical improvement and were discharged home. The average length of hospital stay for this group was 5.8 days (range 1–15 days).
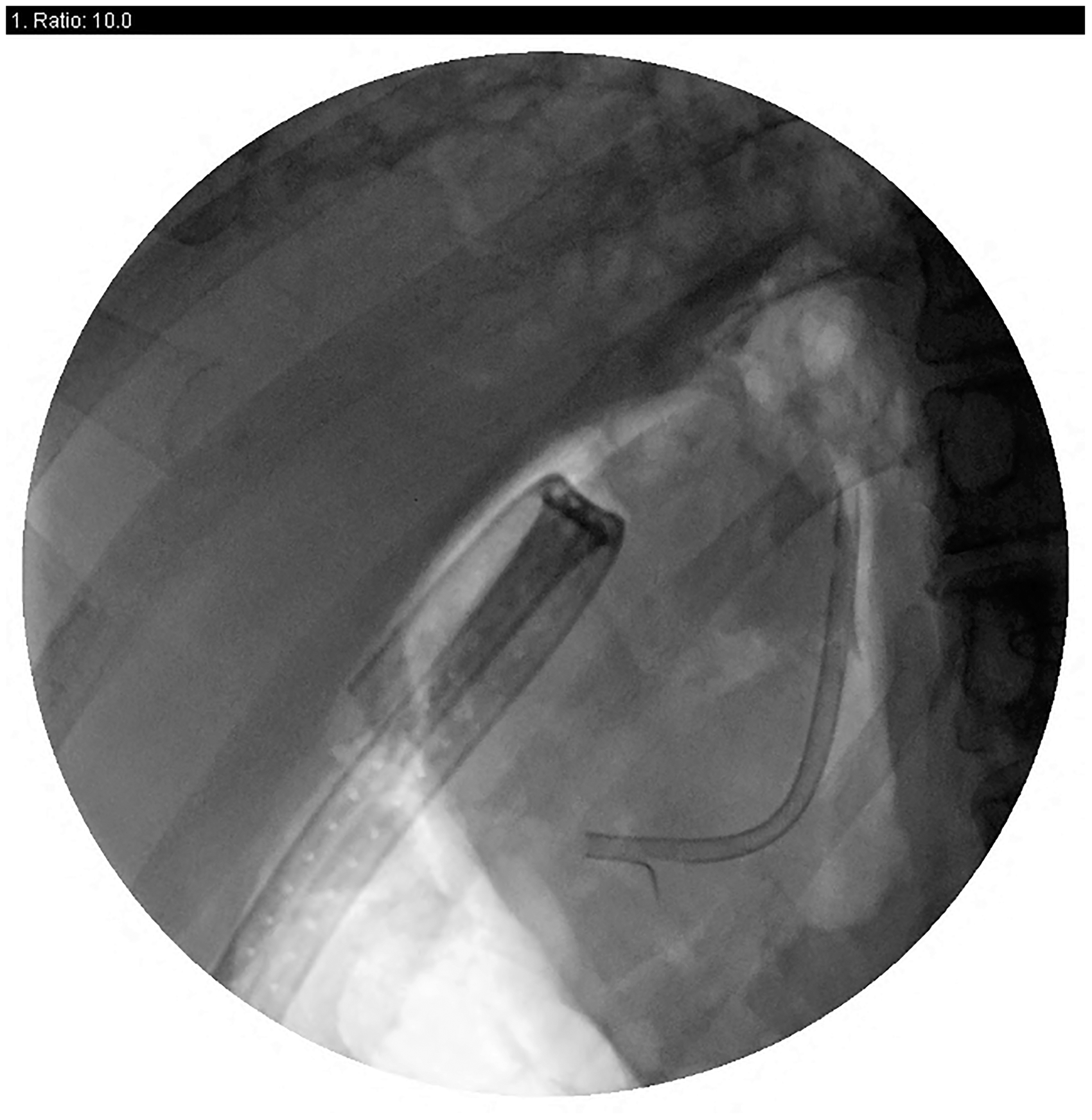
Five patients underwent surgery. Four of the five were diagnosed during or immediately after the procedure (patients 1, 3, 6, 11) and developed peritoneal signs and also had free air on imaging (Figure 1, CT scan of patient 2, and Figure 2, fluoroscopy during ERCP for patient 6). The fifth patient (patient 2) presented to the ER within 24 h of the procedure with fever and peritoneal signs and was also managed surgically. Of the five patients who were taken to the operating room, the perforation/defect could not be identified in one patient (patient 11) and a feeding tube was placed and abdomen closed. In the one patient in whom the omentum was visualized during ERCP with Billroth II anatomy (patient 1), a 3 cm-long perforation on the afferent limb of the jejunum was identified and repaired. The third patient had bile staining of an area of the duodenum, but through and through perforation was not seen; the area was sutured (patient 3). In the fourth patient (patient 11) no perforation was identified at laparotomy, but a posterior duodenal wall microperforation could not be ruled out, and hence a feeding jejunostomy tube was placed and no actual repair of perforation done; surgery was aborted and the patient improved with antibiotics and conservative management alone. The fifth patient (patient 6) who had the ERCP for malignant biliary stricture was found to have extensive metastatic disease with adhesions on laparotomy and perforation could not be seen; surgery was aborted after J tube placement and the patient improved with antibiotics and conservative management alone. She also had an esophageal rupture during the procedure and was taken to the operating room by ENT surgeons, but was found to have healing pyriform sinus rupture; a drain was placed to drain the retropharyngeal space, though there was no abscess formation. She had metastatic gall bladder cancer with peritoneal carcinomatosis. There was no mortality associated with either conservative or surgical management.
CT scan with free air. Contrast extravasation during ERCP.
Discussion
This is one of the largest studies evaluating the incidence, management and outcome of perforations associated with ERCP in the present century. We found a very low incidence over this 10-year period, despite the evolution of ERCP to a therapeutic modality. Leaks were much more common than perforations, and the majority of patients were successfully managed with conservative therapy alone.
Previous studies have reported variable incidence rates of 0.3–6%.4,5 In a large retrospective study, Fatima et al. described 75 perforations in 12,427 patients. 8 In another study by Morgan et al., the incidence of perforations was 0.2%. 9 Importantly, most of these studies were retrospective, and the percentage of ERCP-related therapeutic interventions performed in the majority of previous studies has ranged from 50–70%.4,10 Such results underscore the importance of our study, as our findings reflect current trends associated with therapeutic ERCP.
There are several potential explanations for the low perforation rate in our study. Firstly, to a large extent, it may be related to the experienced endoscopists at our center, and also early recognition and treatment of the patients. Secondly, information bias is also possible but unlikely, as all the patients who had their procedure and were discharged home could have sought medical care locally or at other hospitals. Thus, we might not have captured 100% of complications, especially the ones who would improve with minimal intervention.
ERCP-related perforations have been categorized into four different types based on the location of the injury. 11 The lateral duodenal wall is affected in type 1 injury. 12 Review of the literature shows that these have been managed surgically secondary to high risk of peritonitis, but if diagnosed during the procedure, endoscopic closure with clips and/or fibrin glue can be attempted and may prevent surgery in some patients. Peri-vaterian or type 2 injuries are injuries at the sphincter of Oddi and can be managed conservatively to a large extent, either endoscopically if diagnosed during ERCP or with nasobiliary drainage, intravenous fluids and antibiotics. 12 Distal bile duct injuries are classified as type III injuries, and are usually secondary to instrumentation. These injuries can present late, but if diagnosed early on, can be treated medically with good outcomes.6,12,13 Type IV injuries are not considered true perforations as they can be an incidental finding of free air during or after the procedure, and may be related to insufflation of air during the procedure which can dissect through the duodenal wall. 14 Free air in an otherwise asymptomatic patient can be categorized as type IV injury and needs no surgical intervention, though the patient may require close monitoring to ensure peritoneal signs do not develop;6,15 this type of injury was most common in our series.
While selected patients with ERCP-related perforations can be managed endoscopically, if diagnosed during the procedure, with clips, 14 surgical repair should be reserved for patients in whom endoscopic measures are unsuccessful, if the medical measures fail, and for those with frank perforation performed.11,15,16
Based upon our experience reported here and the literature, we have devised a protocol for management (Figure 3). Patients with a suspicion for perforation must be evaluated with early imaging, preferably a CT scan of the abdomen with oral contrast. Patients who have free retroperitoneal air and are otherwise asymptomatic can be managed conservatively, though may need to be observed in the hospital for 1–2 days and generally do not require any further procedures/surgery, etc. Patients with remote perforation, those who are not diagnosed early on and present several days after the procedure, may require surgical intervention if an active leak of oral contrast is seen at the time of CT scanning; if no leak is appreciated, conservative therapy is warranted. Patients with a frank perforation that is visualized during the procedure, if not amenable to endoscopic intervention, should be referred for immediate surgical repair.
Algorithm for suspected perforation during ERCP.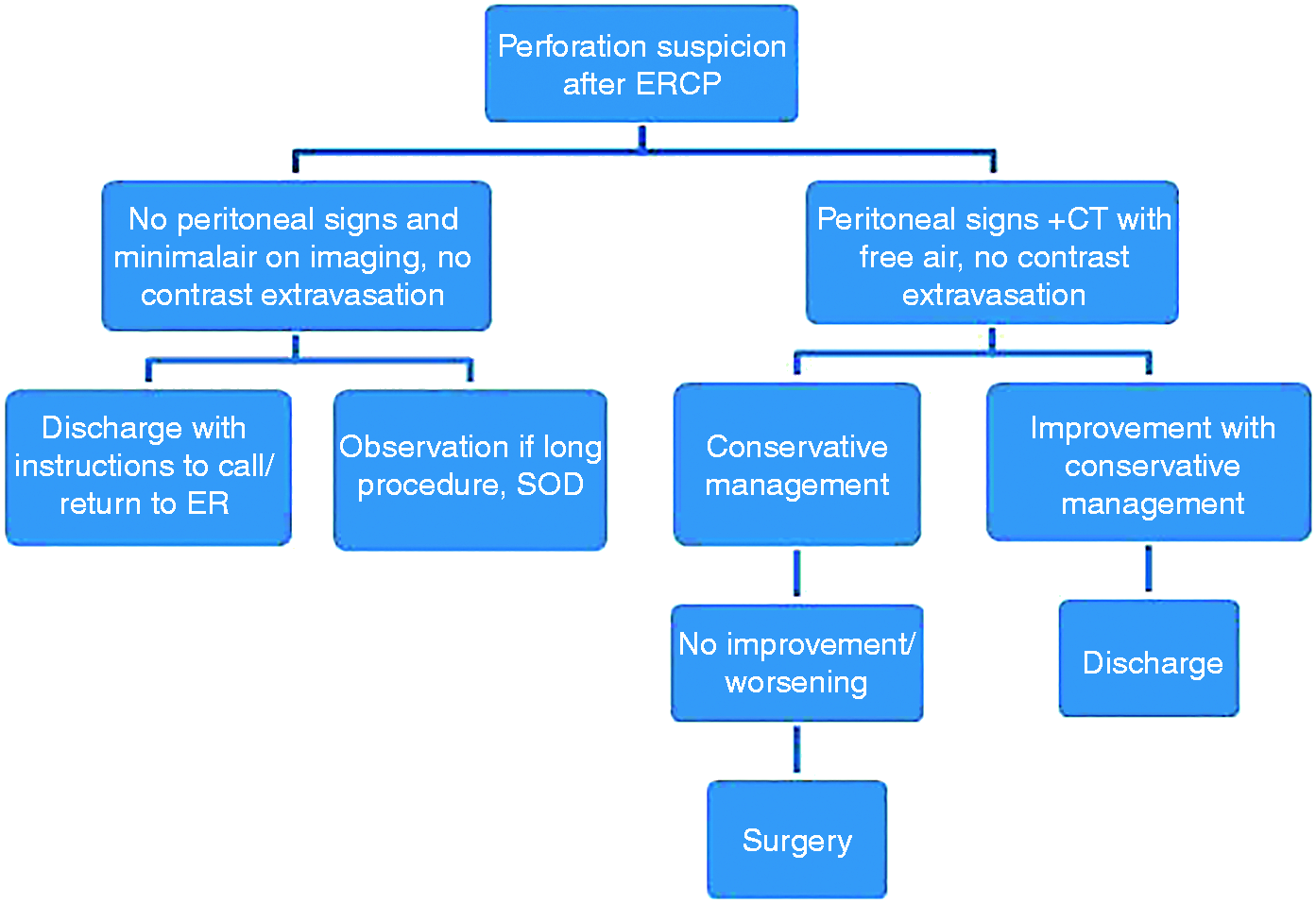
Our study has several potential limitations. First, we are a tertiary referral center and the population may not reflect those of other centers. However, current data supports the performance of advanced therapeutic procedures in tertiary centers, as low-volume centers may have lower rate of success and higher rates of complications. 17 Second, the percentage of therapeutic cases was very high at our center, about 20–30% higher than previous reports. Nonetheless, ERCP should primarily be a therapeutic procedure except for situations where MRCP is still not a gold standard, such as an occasional patient with post-liver transplant strictures. Third, we evaluate and treat a large number of patients in whom previous ERCP failed. A logical assumption from this fact is that the perforation rates in practices where there are less complex cases should be lower. This emphasizes the importance of our study, as it adds incidence rates for high-volume centers performing therapeutic ERCP often in the most difficult cases. Last, although our database is collected prospectively, it is possible we still may have missed patients on follow-up, as noted above.
In summary, we report a perforation rate related to ERCP of 0.14%. This is an extremely low rate compared with much higher rates reported at other centers. Sphincterotomy-related perforations constituted the majority of the causes. Early recognition, such as by fluoroscopy at the time of ERCP or visualization, can help to institute appropriate therapy.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.