
Abstract
Background
Current recommendations on training in endoscopic retrograde cholangiopancreatography are predicated on a performance-centred approach designed to ensure that trainees achieve appropriate skills. We aimed to analyse how competence in endoscopic retrograde cholangiopancreatography is defined in the literature and what proportion of trainees actually reach this threshold.
Methods
We conducted a systematic MEDLINE search for studies reporting on endoscopic retrograde cholangiopancreatography training programmes in a clinical setting. The main outcome measure was threshold for achieving competence in endoscopic retrograde cholangiopancreatography; the secondary outcome measure was assessment of trainee performance. Quality was assessed using the Cochrane Risk of Bias tool and the Methodological Index for Non-Randomized Studies criteria.
Results
Of 522 initially identified articles, 20 were included in the analysis; most studies showed a high risk of bias. Cannulation rate of the desired duct was the main marker of competence in all studies; however, only 8/20 studies reported on the performance of individual trainees, who achieved their respective standard of competence in only 25.6% of reported cases.
Conclusions
Current literature identifies cannulation rate of a native papilla to be the most appropriate measure of endoscopic retrograde cholangiopancreatography competence; however, most trainees do not reach predefined competence thresholds. Furthermore, due to the limitations of available studies, the most appropriate competence measure remains subject for debate.
Keywords
Key summary
Summarise the established knowledge on this subject.
Competence in endoscopic retrograde cholangiopancreatography (ERCP) is usually quantified using a surrogate marker such as successful cannulation rates for the desired duct. ERCP training methods have not been standardised yet, with high variations between different training programmes. Most guidelines recommend that trainees perform a predefined number of procedures or reach a certain rate of successful cannulation of the native papilla. What are the significant and/or new findings of this study?
Most studies on ERCP training have a high risk of bias. There is a high variation between studies with respect to what constitutes competence in ERCP. Most trainees do not reach predefined competence thresholds during their training period.
Introduction
Endoscopic retrograde cholangiopancreatography (ERCP) has evolved rapidly over the past decades, from a diagnostic to a mainly therapeutic procedure, facilitating complex interventions in the bilio-pancreatic system. The advent of ERCP as a mainstream technique with ever-expanding indications has also brought increased awareness and attention to associated complications, ranging from mild to life-threatening. 1 As a result, quality measures focused on technical and safety-related outcomes have been proposed, with the aim of improving general practice in this field. 2
Training programmes for advanced endoscopy techniques such as ERCP have also been the focus of intense debate. The old training paradigm focusing on a threshold number of procedures 3 is gradually being replaced by a performance-centred approach in recognition of the fact that sheer case volume is not a guarantee of competence. The American Society of Gastrointestinal Endoscopy (ASGE) currently recommends a minimum caseload of 200 ERCPs per trainee followed by competence assessment, with selective cannulation rates of the common bile duct >80–90% of native papilla cases usually considered as a good surrogate marker of trainee competence. 4 However, it is increasingly recognised that most trainees do not cross this threshold during training5,6 and some experts are calling for an overhaul of the way competency is assessed altogether. 7 One of the main obstacles in improving training programmes for ERCP is the limited availability of good-quality data reporting on training methods and outcomes for advanced endoscopy trainees.
We aimed to review and analyse currently available data on how competence in ERCP is defined and measured and how often this is achieved across available studies.
Materials and methods
We conducted a systematic review of studies that report results of ERCP training programmes in a clinical setting, studies of trainee learning curves in achieving competence in various aspects of ERCP and/or studies which reported on outcomes of ERCPs with trainee involvement. The main outcome measure for our search was the characterization of the threshold for achieving competence in ERCP; the secondary outcome measure was assessment of trainee performance according to predefined criteria within each study.
Search strategy
We conducted an electronic database search of Medline (from inception to 8 August 2018) according to the following search strategy (‘Cholangiopancreatography, Endoscopic Retrograde’ [Mesh] OR ERCP [tiab] OR ‘endoscopic retrograde cholangio*’ [tiab]) AND (‘Learning’[Mesh] OR train*[tiab] OR fellow* [tiab] OR competen*[tiab] OR audit[tiab] OR ‘Professional Competence’[Mesh] OR residen*[tiab] OR skill*[tiab]) NOT (‘Animals’[Mesh] NOT ‘Humans’[Mesh]) NOT (‘Case Reports’ [Publication Type] OR ‘Letter’ [Publication Type] OR ‘Comment’ [Publication Type] OR letter*[ti] OR comment*[ti] OR case report*[tiab] OR rat[tiab] OR rats[tiab] OR mouse[tiab] OR mice[tiab] OR animal*[tiab]).
Study selection
For a citation to warrant inclusion it had to fulfil the following criteria: (a) original study; (b) full text available; (c) report on at least one aspect of competence in ERCP (i.e. cannulation rate, overall technical success rate, trainee learning curve for a specific manoeuver) as a main or secondary outcome. Studies focusing only on simulator models were excluded from the analysis. Letters to the editor, comments, reviews and editorial articles were also excluded. Only articles published in English were included.
Two independent reviewers (TV and PB) screened all the titles and abstracts for potentially relevant articles. If there was disagreement on eligibility between two reviewers, then this was settled by consensus. Full-text articles were then also independently reviewed and the reference sections of included studies were analysed to retrieve relevant studies not identified by the original search.
Data extraction
Each reference included was independently reviewed by two reviewers. Using a structured approach, the following categories of data were extracted from the included studies: (a) study characteristics (authors, year of publication, study design, number of trainees in the study, total number of procedures); (b) baseline characteristics of the ERCP training (trainee and trainer experience, training protocol); (c) definition and assessment of trainee competence, including number of cases per trainee required to gain competence as defined within each individual study and the proportion of trainees in each study reaching the proposed competency threshold; and (d) safety outcomes and adverse event rates.
Quality assessment of the studies was jointly conducted by the two reviewers, using the Cochrane Risk of Bias Tool 8 and the Methodological Index for Non-Randomized Studies (MINORS) criteria. 9
The final results were compared and, where necessary, consensus was reached to settle any divergence in opinion between the reviewers. Due to the high heterogeneity of studies included in the analysis, a meta-analysis of the results was not attempted; the final results of the systematic review were narratively reported.
Results
After the initial search, 28 full text articles were retrieved and analysed, with 20 articles included after bibliographical analysis of full-text articles (see Figure 1).
Flow-chart of studies included in the final analysis according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) reporting guidelines.19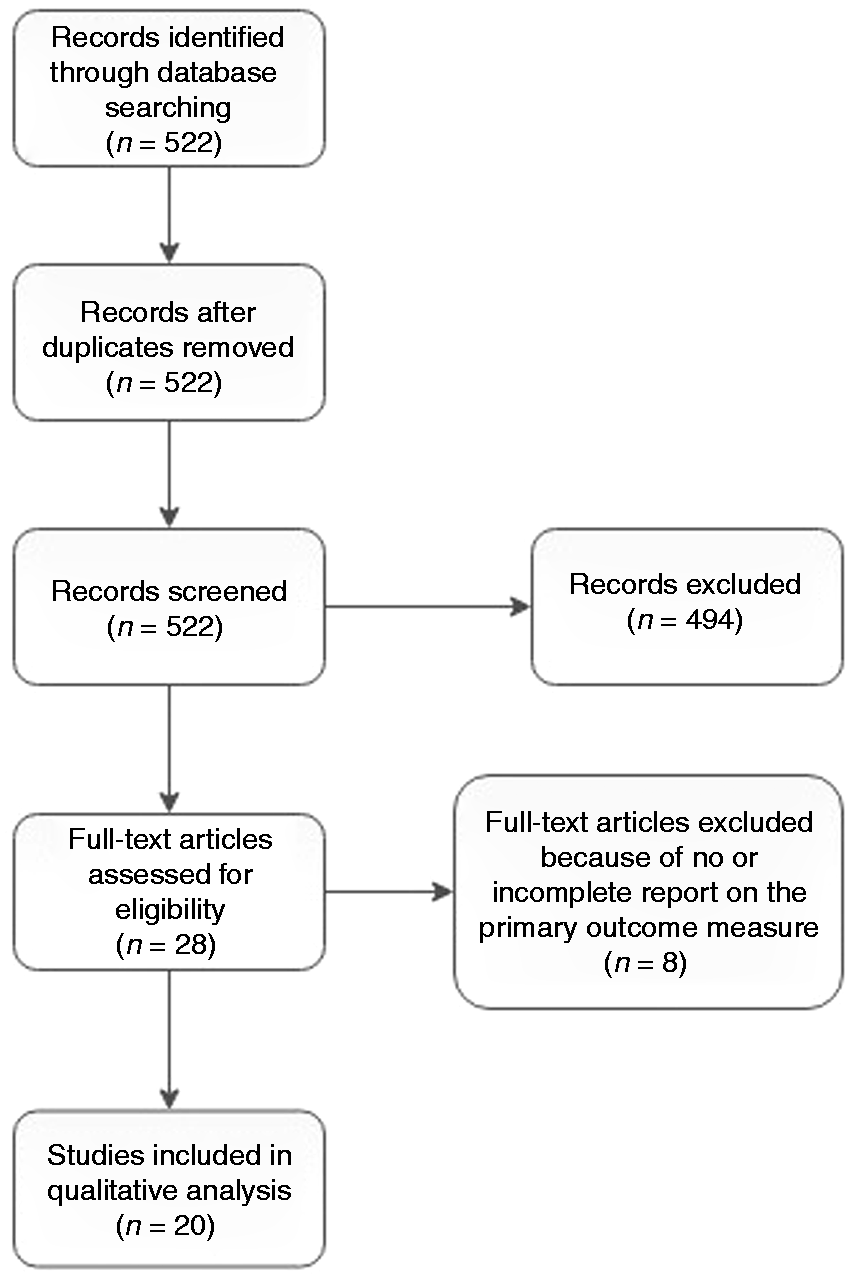
Synthetic presentation of data on endoscopic retrograde cholangiopancreatography (ERCP) training protocol and outcomes extracted from the 20 studies included in the final analysis.
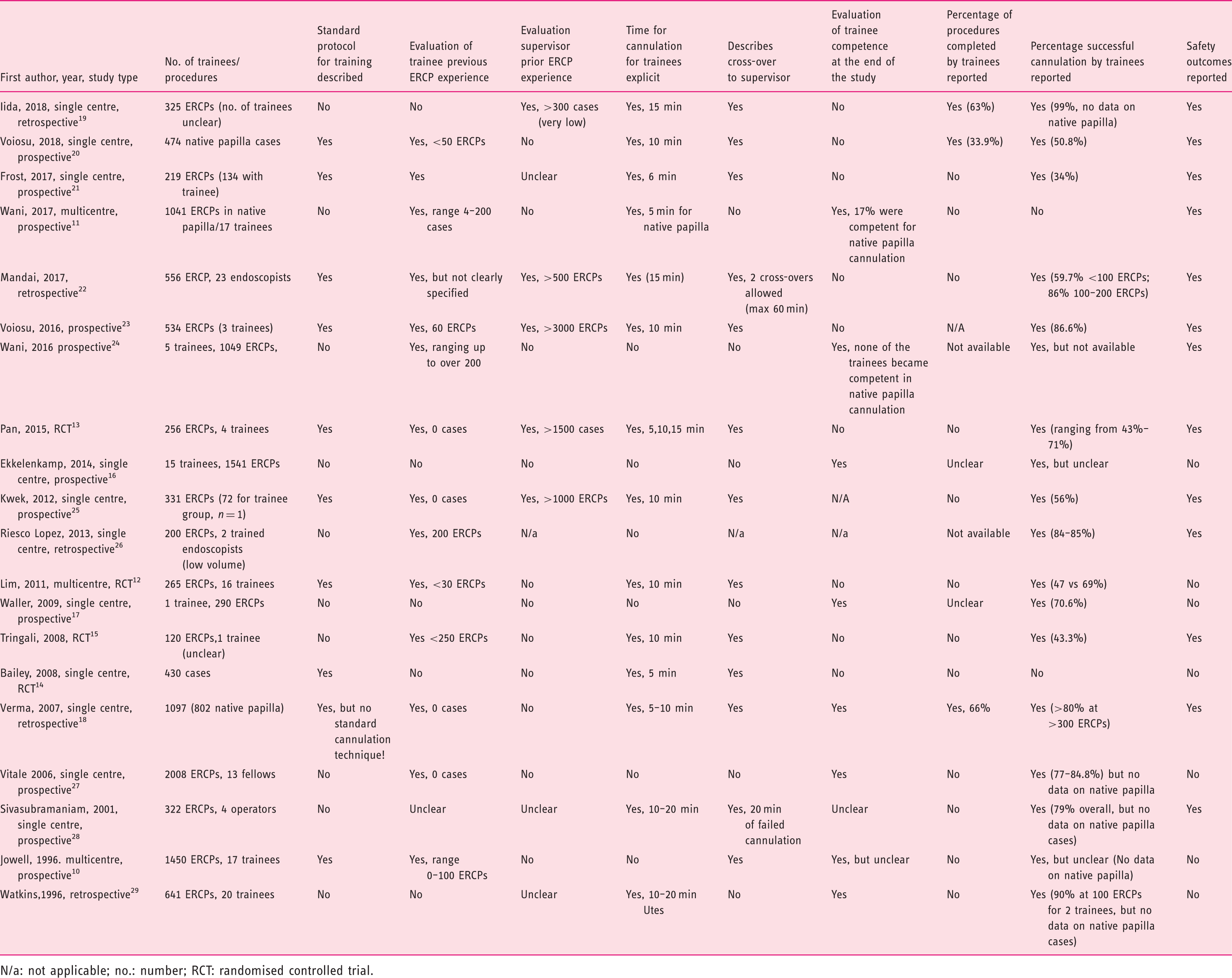
N/a: not applicable; no.: number; RCT: randomised controlled trial.
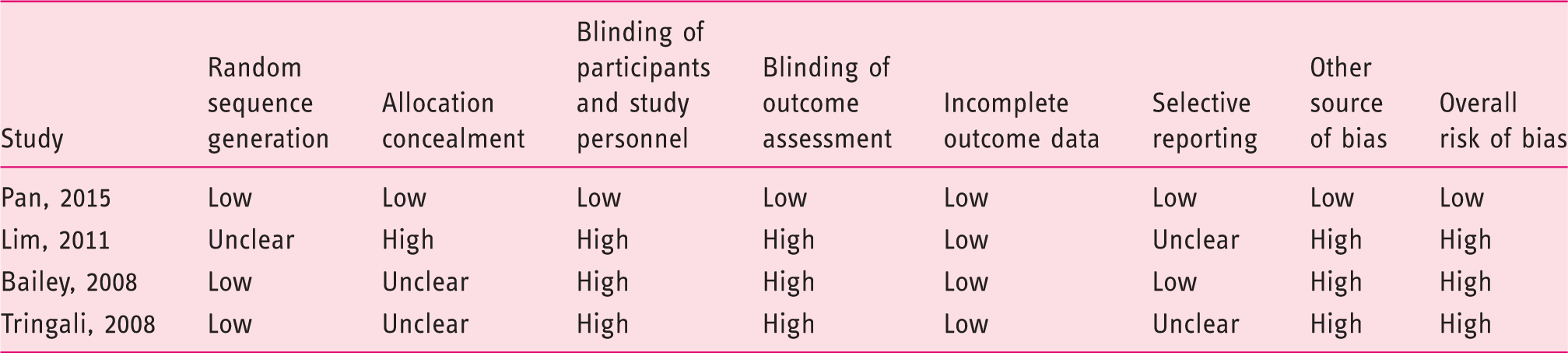
Quality assessment of randomised controlled trials with Cochrane Risk of Bias Tool.
Quality assessment of nonrandomised studies with the Methodological Index for Non-Randomized Studies (MINORS).
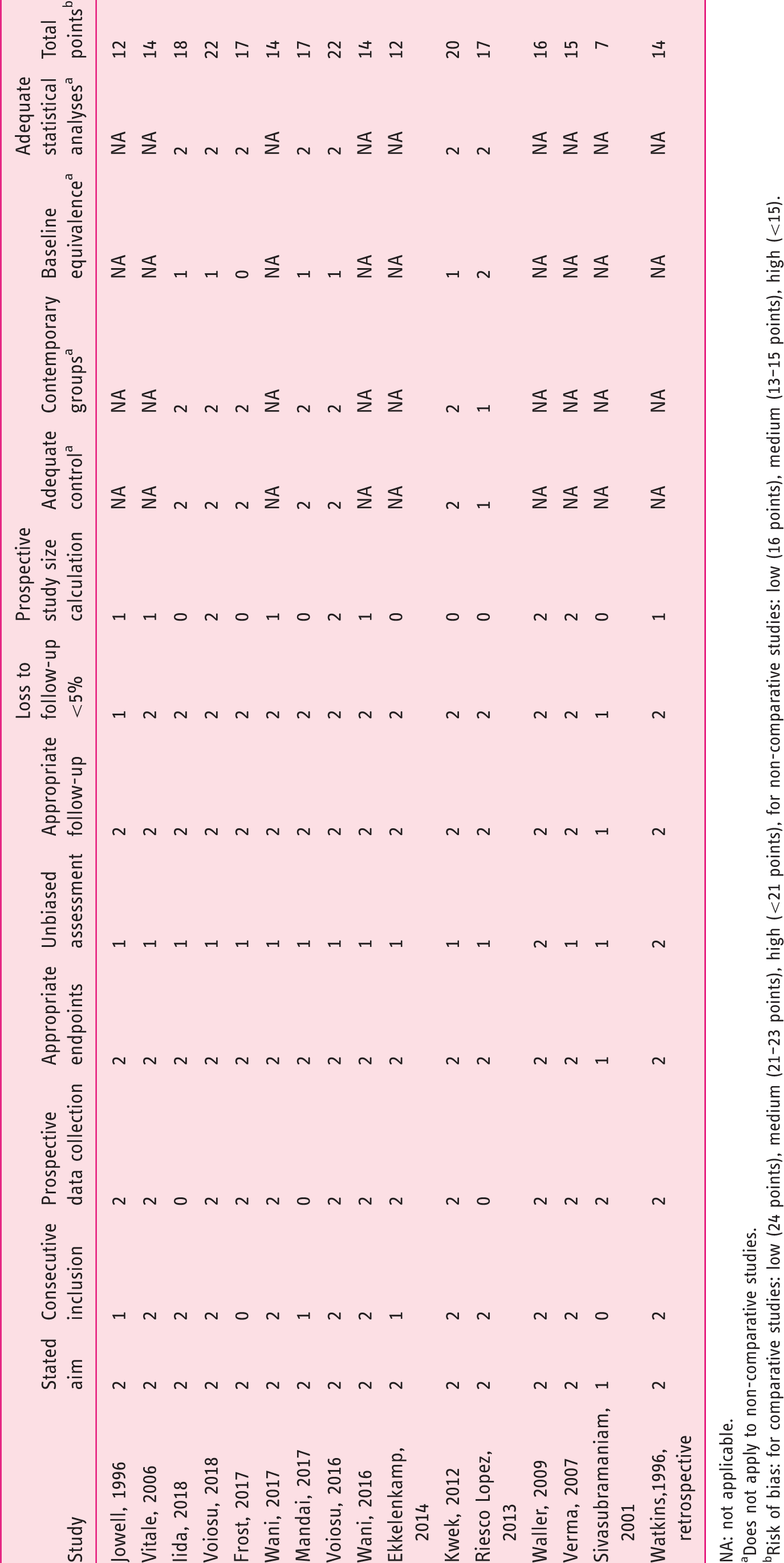
NA: not applicable.
Does not apply to non-comparative studies.
Risk of bias: for comparative studies: low (24 points), medium (21–23 points), high (<21 points), for non-comparative studies: low (16 points), medium (13–15 points), high (<15).
Training protocol, ERCP trainees and supervisors
Only 10 out of 20 included studies included a clear description of a standardised training protocol for the ERCP trainees during the study period (i.e. time allowed on the papilla, standard approach to cannulation and other manoeuvers, duration of training period, timing of supervisor intervention etc.), with high variability between the studies. Fourteen out of 20 studies reported the average time allowed for the trainee to attempt cannulation of the desired duct, which varied between 5–20 min; however a standard rule for cross-over from trainee to supervisor in case of trainee failure to complete a manoeuver during ERCP was only explicitly described in 12/20 studies (60%) (see Table 1).
Explicit estimates of trainee and supervisor caseloads prior to study inception were lacking or unclear in 8/20 (40%) and 16/20 (80%) of studies respectively. Furthermore, the threshold between trainee and trainer is further muddled by the fact that in two studies the definition of expert/supervisor is based on previous experience of only 300 and 500 ERCPs respectively,20,23 a low volume which practically overlaps caseloads accrued by some trainees during the study period in some of the other included articles.18,25
Achieving competence in ERCP
Comparison of definition of competence and trainee performance across studies included in the final analysis.
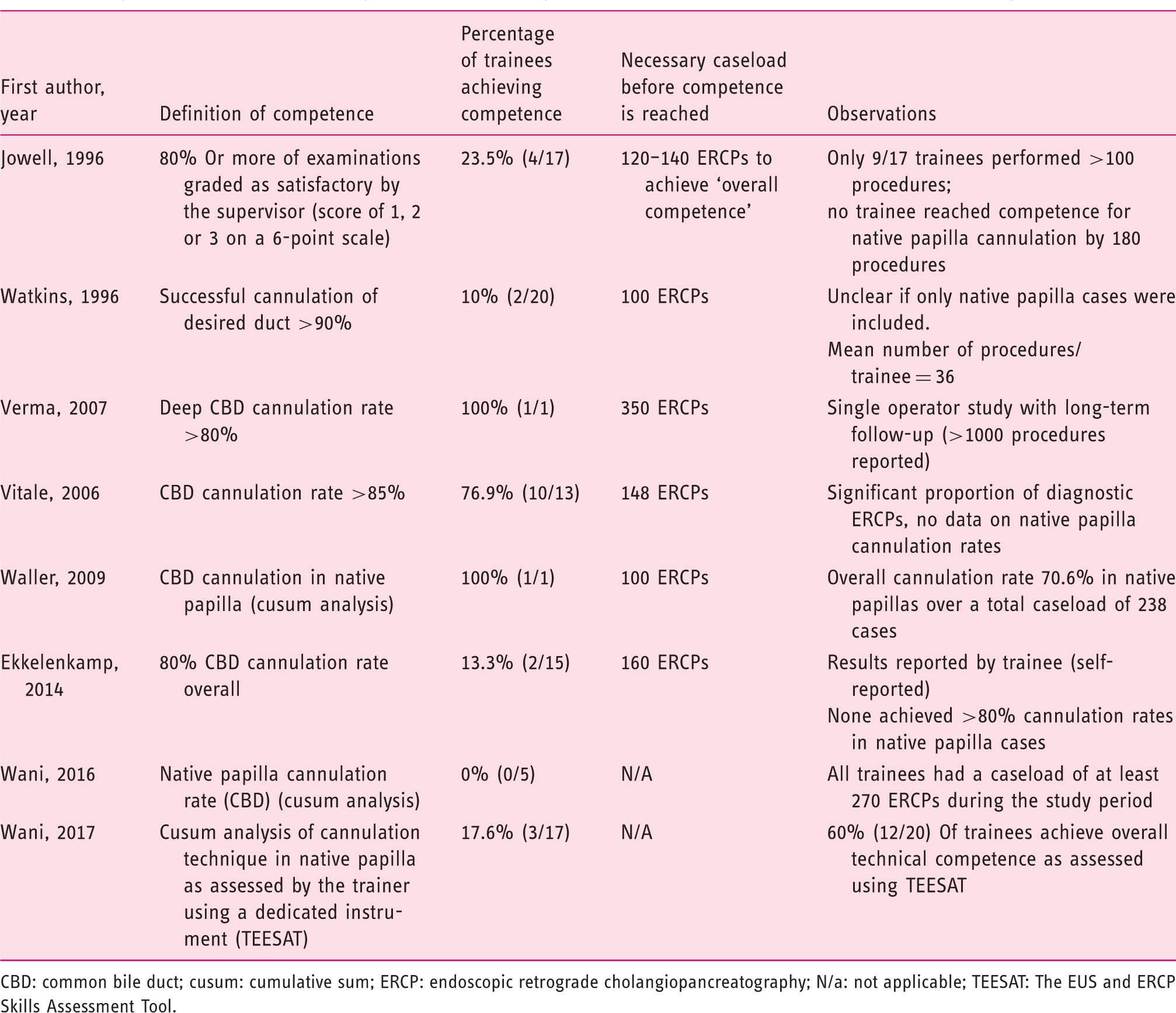
CBD: common bile duct; cusum: cumulative sum; ERCP: endoscopic retrograde cholangiopancreatography; N/a: not applicable; TEESAT: The EUS and ERCP Skills Assessment Tool.
Achieving competence in ERCP: duct cannulation rate
Selective cannulation rate of the desired duct was used as a measure of competence in ERCP in all studies, however there were important difference between studies with regard to the definition and assessment of trainee competence. Three studies used cumulative sum (cusum) analysis to plot learning curves for trainees; two of these studies used a grading system which required the trainer to assess trainee performance on each procedure while the third study used a binary report of trainee success in cannulation.
The other four studies divided each trainee’s caseload in blocks of 10–20 procedures, and analysed cannulation rates per each consecutive block to assess when the threshold for competence was crossed for each trainee.
It is worth noting that in the studies by Jowell et al., 10 Watkins et al. 30 and Vitale et al. 28 cannulation rate is, most likely, not limited to native papilla cases, while in the study by Ekkelenkamp et al. 16 none of the trainees reach competence if the analysis of their performance is limited to native papilla cases only.
Achieving competence in ERCP: looking beyond cannulation rates
Only three out 20 studies (15%) report the percentage of procedures completed by trainees without hands-on intervention from a supervisor. 18,20 ,21 Iida et al. 20 report a success rate of 63.3% for common bile duct (CBD) stone clearance, while Voiosu et al. 21 and Verma et al. 18 report a success rate of 33.9% and 66% respectively for trainees completing procedures with a wide range of indications (i.e. stone extraction, stenting of benign and malignant strictures, treatment of bile leaks, etc.).
Three more studies11,16,17 report on trainee success in performing therapeutic manoeuvers such as sphincterotomy, stent placement or stone clearance from the CBD, and estimate the threshold for achieving competence in these manoeuvers. It is interesting to point out, however, that selective cannulation of the CBD in the native papilla seems to be the most challenging part of the procedure for the trainees, who achieve higher success rates for manoeuvers such as stent placement and stone extractions.11,16 However, these data need to be interpreted with caution, since in both studies cited above there is no clear reporting on the involvement of a supervisor or the percentage of procedures completed unaided by the trainees.
Finally, 13 out of 20 studies (65%) provide data about procedure-related adverse events, and none of these studies showed a negative impact of trainee involvement on patient safety. However, it is important to underline the fact that only one study 24 was designed to specifically address this end-point, explicitly providing sample size calculation for this particular outcome measure.
Discussion
Our study provides an in-depth analysis of the methodology of studies reporting on results of ERCP training, taking into account additional relevant variables such as training protocol, previous experience of the trainee, and percentage of procedures completed by the trainee without assistance. In this systematic review we have identified 20 studies focusing on the process of ERCP training and its outcomes in terms of trainees achieving certain predefined competence thresholds. While all studies recognised selective cannulation rate of the desired duct to be the main surrogate marker of competence, some studies also included the proportion of procedures completed without assistance, or successful completion of therapeutic manoeuvers (i.e. stone clearance, stent placement, sphincterotomy) as markers of ERCP competence.
With regard to CBD cannulation rate, nine out of 20 studies evaluated trainee competence in performing this manoeuver, with only roughly one in four trainees across all included studies reaching the competence threshold predefined in their respective study protocol. Similar findings were described in an earlier review of training in ERCP by Shahidi et al., 31 but the scope of this earlier study is more limited, focused solely on selective cannulation rate as a marker of achieving competence in ERCP. However, the process of developing competence in ERCP is more complex and, in this review, we have aimed for a more wide-ranging overview of the possible markers of competence and, hereby, a more nuanced interpretation of competence in ERCP. The percentage of procedures successfully completed by trainees without hands-on assistance from their supervisor, a marker of competence more relevant to a real-life clinical setting, is only reported as an outcome measure in three of the studies. Furthermore, data from this studies suggests that trainees complete at best two out of three procedures where they are involved, falling well short of the new recommendations for training programmes, such as those from the Joint Advisory Group on Gastrointestinal Endoscopy (JAG) in the UK, which require trainees to achieve a success rate >80% in completing grade 1 procedures unassisted, with an associated complication rate of <5%. 32
Competence in endoscopy is defined as ‘The minimum level of skill, knowledge, and/or expertise derived through training and experience required to safely and proficiently perform a task or procedure’ by the current ASGE guidelines on privileging. 32 In light of this definition, we feel that equating competence in ERCP with a cannulation rate of the CBD above a certain threshold, as implied by most of the analysed studies, is insufficient to adequately reflect competence in performing a high-risk therapeutic procedure. This view is also supported by the upcoming European Society for Gastrointestinal Endoscopy (ESGE) proposal of quality standards in ERCP, which includes successful stone extraction rates>90% and correct stent placement >95% alongside successful cannulation as key performance measures for ERCP (article in press).
In our review of available literature we found only one study which coherently reports on the learning curve of a trainee starting to perform ERCP, 18 including sufficient data on, but not limited to, the training protocol in the unit, indication for all of the procedures, improvement of cannulation rates of native papilla over time, percentage of procedures completed by the trainee without help from his or her supervisor and safety outcomes for the patient. Accordingly, it becomes obvious that further large, multicentric, preferably randomised clinical trials are needed before we can adopt an improved, evidence-based strategy for training in ERCP.
Suggested minimal reporting standards for studies of endoscopic retrograde cholangiopancreatography (ERCP) training.

CBD: common bile duct.
In spite of the broad approach of our study, this review is limited by the narrow design of many of the included studies, quantifying only a single outcome variable as a surrogate marker of competence (i.e. cannulation rate of the desired duct). Most studies available are single-centre observational cohorts and are thus subject to a high risk of bias. The amount and quality of data on competence development in ERCP is fairly poor, as shown in our analysis of the studies. This makes interpreting and comparing results from different studies quite difficult, while also limiting the generalisability of this data.
Another significant limitation of many studies included in our analysis is the fact that most individual trainees observed during the respective study periods accrue case volumes which are well below required standards to assess competence, with only three studies including sufficient caseloads per individual trainee (i.e. >200 ERCPs) to allow adequate analysis of learning curves. If we also take into account the heterogeneity in experience in ERCP for each trainee prior to the respective study period, ranging from zero to over 200 ERCPs across various studies, the task of tracing a roadmap to competence for the individual trainee becomes exceptionally difficult.
In conclusion, our research shows that selective duct cannulation rate remains the most utilised measure of ERCP competence across the available literature, although most trainees fail to reach predefined competence thresholds. Based on these findings, we believe that future studies, providing a more in-depth analysis of the learning process, are required to allow a more comprehensive definition of true competence in ERCP as a basis for improved training programmes.
Footnotes
Acknowledgements
The following author contributions were made: Theodor Voiosu, Paul Bălănescu and Andrei Voiosu were involved in the conception and design of the study, analysis and interpretation of the data, drafting of the article and final approval; Andreea Benguş and Carmen Preda were involved in the design of the study, drafting of the article and final approval; Devica S Umans, Radu Bogdan Mateescu and Jeanin E van Hooft were involved in analysis and interpretation of the data, critical revision of the article for important intellectual content and final approval of the article.
Declaration of conflicting interests
Jeanin E van Hooft has received research grants from Cook Medical and Abbott and consultancy fees from Medtronics, Boston Scientific and Mylan. Theodor Voiosu, Paul Bălănescu, Andreea Benguş, Carmen Preda, Devica Umans, Radu Bogdan Mateescu and Andrei Voiosu have no conflict of interests to declare.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Ethics approval
This is a systematic review so no ethics approval or informed consent is required.
Informed consent
This is a systematic review so no ethics approval or informed consent is required.