
Abstract
Background
There is no consensus on what constitutes adequate training for needle knife precut sphincterotomy.
Objective
The purpose of this study was to determine the number of procedures required before effective and safe precut sphincterotomy can be achieved.
Methods
This retrospective study examined the cumulative experience of a single endoscopist from January 2006–December 2015. Precut sphincterotomy success and complication rates were analyzed as a function of number of procedures performed. Acceptable success and complication rates were defined as 85% and 10% respectively. A one-sided binomial test was used to test success and complication rates of every 25 precut sphincterotomies performed.
Results
The index endoscopic retrograde cholangiopancreatography was successful in 141/158 (89.2%) patients who underwent precut sphincterotomy. This increased to 148/158 (93.7%) when endoscopic retrograde cholangiopancreatography was repeated on another day. Six precut sphincterotomies were required to achieve an 85% success probability. This was maintained consistently above 85% after 13 precuts, and was significantly higher (91.2%; p = 0.029) than 85% at the 125th precut. Bleeding and pancreatitis developed in 2/158 (1.3%) and 5/158 (3.2%). Probability of either complications remained below 5% after 50 precuts. No perforation occurred.
Conclusion
At least 13 precut sphincterotomies were required to achieve a sustained success rate greater than 85%. The probability of bleeding or pancreatitis was less than 5% after 50 precut sphincterotomies.
Keywords
Introduction
Selective deep cannulation of the common bile duct (CBD) or pancreatic duct (PD) is the most important step for successful endoscopic retrograde cholangiopancreatography (ERCP). Successful cannulation rates of more than 85% are achievable by most practicing endoscopists although, in the hands of experts, the success rates are higher than 95%. 1 Precut sphincterotomy (PS) is a technique used to achieve selective cannulation when standard techniques of selective cannulation fail. “Pre-cutting” is simply de-roofing the duodenal part of the ampulla by electrocautery using a free hand technique to expose the biliary orifice to enable deep cannulation. Most commonly a needle knife papillotome is used; another option is to use the Erlangen-type sphincterotome. The concept was first introduced by Siegel 2 and later popularized by Huibregtse et al. 3 and Soenhendra. 4 PS has been associated with post-ERCP complications such as acute pancreatitis, bleeding and perforation, with complication rates as high as 12–22%.5,6 In expert hands it is generally regarded as safe with a low complication rate.7,8 In fact, results from meta-analyses report that early PS, as opposed to prolonged attempts at cannulation, did not increase complications and was actually associated with a trend towards lower post-ERCP pancreatitis rates.9,10
A learning curve has been demonstrated for ERCP training. The consistent achievement of ≥80% success at deep biliary cannulation is now regarded as a standard for ERCP training programs.11–13 Studies have shown that a case-training volume in excess of 200 is generally required to achieve this level of competency, and that the success rate continued to improve post training as more procedures are performed.14–16 In the context of needle knife PS, there is no recommendation in terms of the numbers required to achieve competency. This is due to the fact that it is not frequently performed, and during a fellow’s formal training experience, it may not be possible to obtain adequate exposure. Nonetheless it is a very important tool in the armamentarium of the endoscopist.
To optimize training outcome and patient safety, it would be relevant to examine, where available, the learning curves of individual endoscopists in the context of precut. To date, five retrospective studies have examined the learning curve for PS.17–21 These studies used a similar methodology, dividing consecutive cases where PS was utilized into chronological groups. The success and complication rates between these groups were then compared against one another. While the studies showed in general that initial and/or overall success rates improved and complication rates declined in the later chronological groups, they did not formally address the learning curve for PS in terms of the minimum number of cases required to achieve a particular success rate or for the complication rate to be consistently below a predefined threshold.
The aim of this study was to determine the number of precut procedures required before effective and safe precut can be achieved, based on predefined acceptable success and complication rates.
Methods and materials
Study design
This retrospective study was based on the cumulative experience of a single endoscopist (TLA) in a tertiary center upon commencement of independent ERCP practice. The endoscopist had hands-on experience in one PS during his ERCP training. Prospectively gathered data in an ERCP registry from the period January 2006–December 2015 were reviewed. The experience of the endoscopist from his first PS to the most recent PS at the end of the study period was examined. Data collected was used to plot a learning curve from which success and complication rates could be derived, and this information was used to determine the minimum threshold at which effective and safe PS could be performed. All patients in the study were admitted for observation for at least 24 h following ERCP and PS. Approval was obtained from the institutional Ethics Committee before study commencement.
Definitions
Success was defined as successful deep cannulation of the CBD following needle knife PS. The success rate was calculated as a function of the number of procedures performed. Based on the fact that competent ERCP endoscopists should expect to cannulate the duct of interest in more than 90% of ERCP procedures of mild-to-moderate difficulty, while successful cannulation rates of more than 80% are a goal of training programs in ERCP, we decided to define the minimum acceptable success rate for PS arbitrarily at 85%. 1 The analysis was then repeated using a lower threshold of 80% success rate. A successful index ERCP in this study referred to a successful deep cannulation of the CBD following PS in the same session where the first PS was made. Delayed success was defined as successful deep cannulation of the CBD at a separate session after the one where the first PS was performed. The overall success rate refers to the total number of successful and delayed ERCPs where deep CBD cannulation was achieved. Complications were defined as adverse events related to PS that required hospitalization or which prolonged the duration of hospitalization. They were defined according to previously accepted guidelines and consensus. In particular, the diagnosis of post-ERCP pancreatitis was based on new or worsened abdominal pain and either serum lipase or amylase three times or more the upper limit of normal, measured more than 24 h after the procedure.22,23 We defined 10% as the acceptable threshold for developing a complication for purposes of analysis.
Technique of needle knife PS
Standard selective cannulation of the CBD was first attempted using guidewire-assisted biliary cannulation with a papillotome. If selective deep CBD cannulation could not be achieved after 10 min, or if the PD was cannulated inadvertently more than three times, PS was performed for biliary access. PS was performed using a needle knife (KD-441Q, Olympus, Tokyo, Japan) using the conventional precut technique where a stepwise incision of the mucosa starting at the upper margin of the papillary orifice in the direction of the CBD was performed until the underlying biliary orifice was visualized. The biliary orifice was identified by the pinkish mucosa of the bile duct and the contractile motion of the sphincter which was often associated with bile flow during gentle aspiration. 8,13
Statistical methods
Data such as patient demographics, co-morbidities, American Society of Anaesthesiologists (ASA) score, indication for ERCP, success of PS (index, delayed, and overall) and complications were recorded. Categorical data was presented in terms of frequency as a percentage, while continuous data was presented as a mean (with standard deviation) for parametric distribution and median (with interquartile range) for non-parametric distribution. In addition to plotting the learning curve of the endoscopist studied, we further divided the patients in our study into chronological groups of 25 (except for the last group which has 33 patients). A one-sided binomial test was used to test the success and complication rates to the predefined thresholds specified above at every 25 PS procedures performed. A one-tailed, p-value of <0.05 was considered statistically significant.
Results
Demographic data and outcomes for population studied.
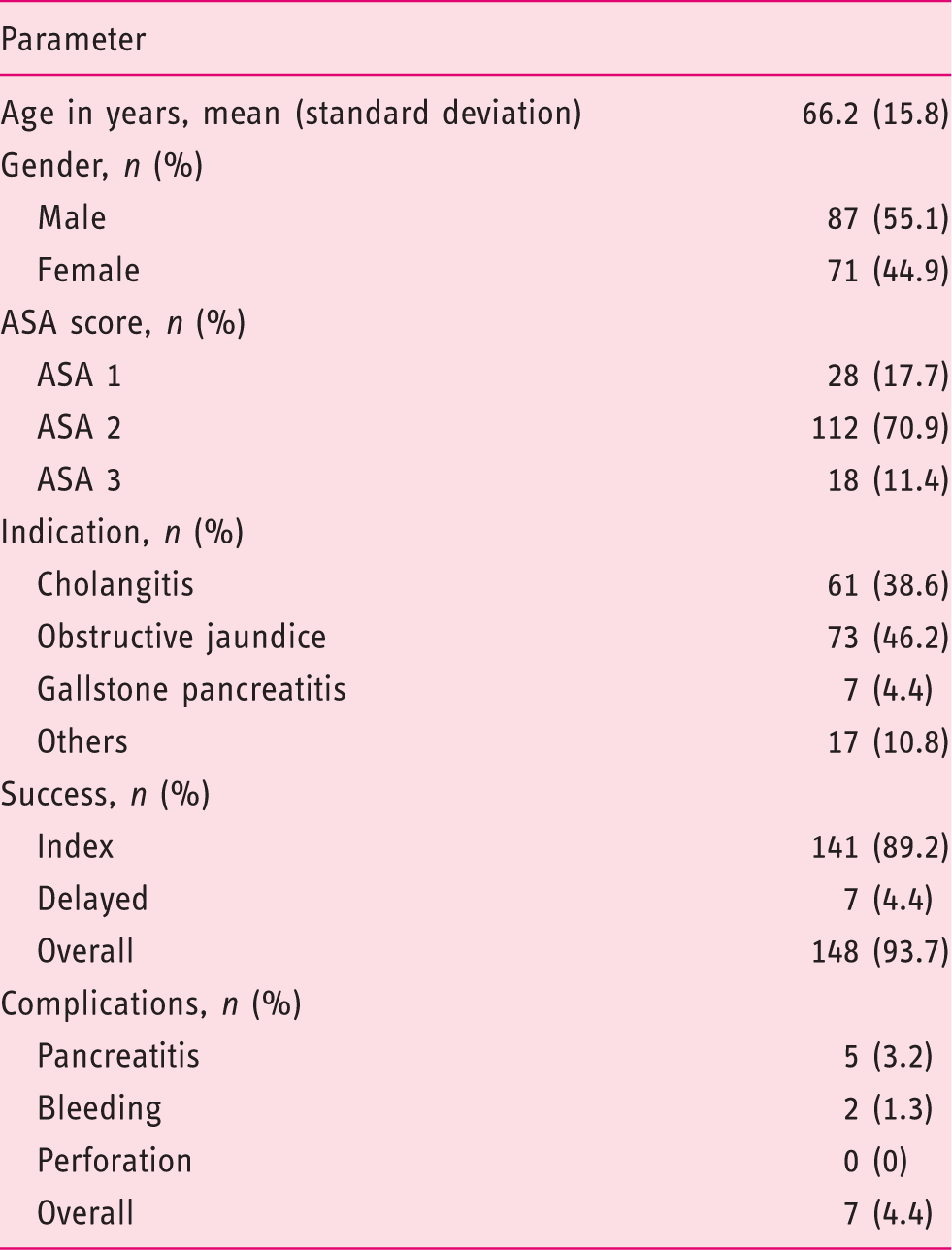
ASA: American Society of Anaesthesiologists.
Among the 158 included cases, 141 (89.2%; 95% confidence interval (CI) 83.4%–100.0%) had a successful index ERCP following PS. The cannulation success rate after PS at the index ERCP according to underlying disease was 101/108 (93.5%) for CBD stones, 34/42 (81%) for malignant strictures, 4/6 (66.7%) for benign strictures and 2/2 (100%) for bile duct leak. The cannulation success rate after PS in the context of CBD stones was significantly higher than that for malignant strictures (p = 0.021) and benign strictures (p = 0.018). The number of procedures required to achieve a probability of success of 85% was six and a success rate of 85% and above was maintained consistently after 13 PS procedures (Figure 1). The exact one-sided binomial test showed that the probability of a successful PS was not statistically higher than the threshold of 85% for the first 100 precut procedures. At the 125th precut, the probability of achieving a successful index ERCP following PS was significantly higher (91.2%; 95% CI 85.9%–100.0%, p = 0.029) than the predefined threshold of 85% (Figure 1). However, this became insignificant at the 150th PS performed. The analysis was repeated using 80% success rate as the threshold. With this lower threshold, the number of procedures required to achieve and consistently maintain a probability of success of 80% was five. At the 50th PS, the probability of a successful index ERCP following PS became significantly higher (90%; 95% CI 80.1%–100.0%; p = 0.04890) than the 80% threshold.
Probability of successful precut as a function of the cumulative number of precuts performed.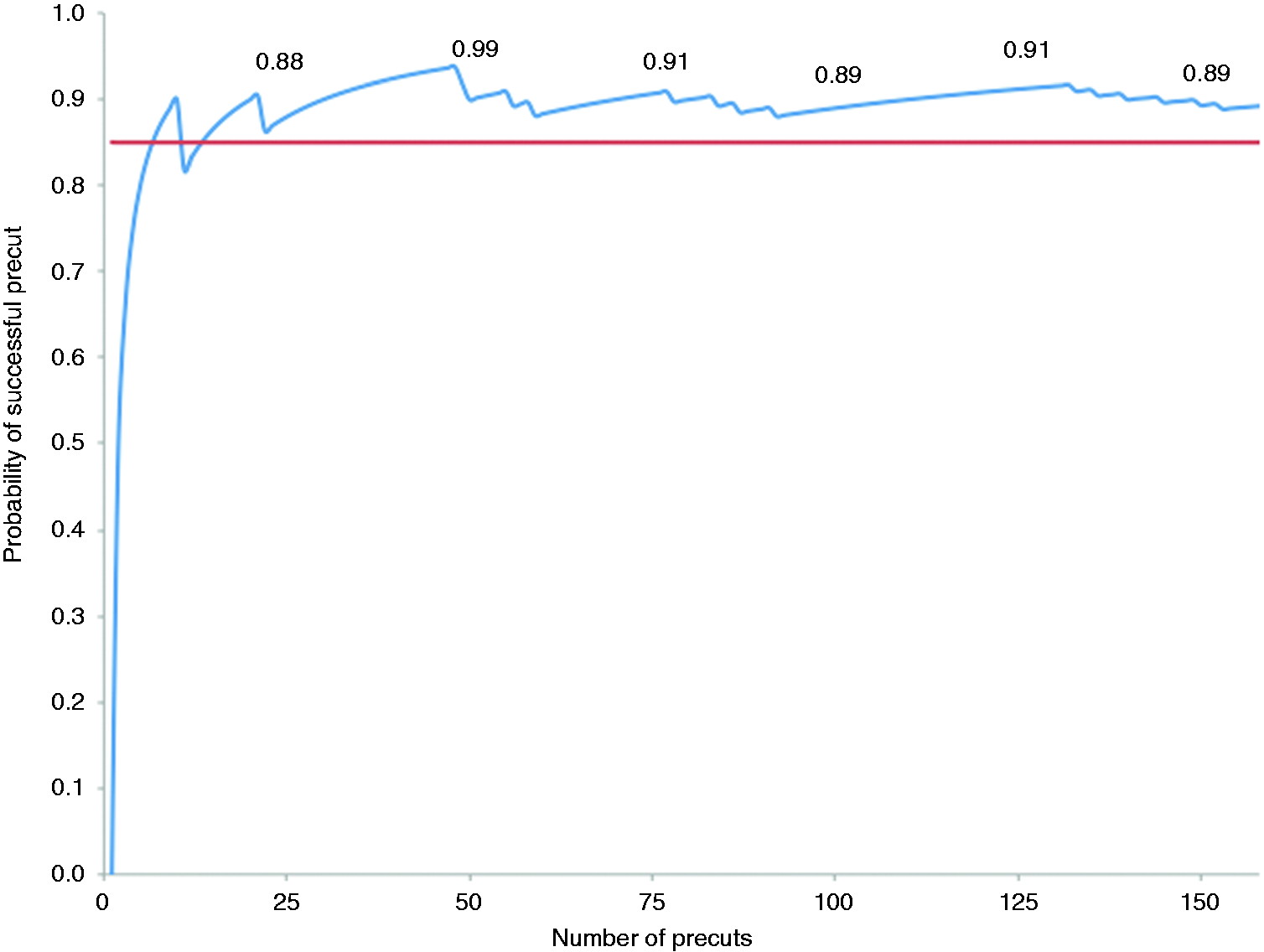
Of the 17 patients who had an unsuccessful ERCP following PS, seven patients had delayed success, with selective deep CBD cannulation achieved in all of these patients at the next ERCP. Nine of the remaining patients required salvage therapy for biliary access and drainage, with eight patients undergoing percutaneous transhepatic biliary drainage (PTBD) first followed subsequently by PTBD-ERCP rendezvous procedures and one patient with unresectable malignant biliary obstruction undergoing endoscopic ultrasound guided transduodenal stenting. The last remaining patient refused further interventions due to advanced age.
In terms of complications, five out of 158 patients (3.2%; 95% CI 0.0%–6.5%) in the study developed pancreatitis after PS. The rate of pancreatitis was 2.0% (n = 1; 95% CI 0.0%–9.1%) after the 50th precut, and this was significantly lower than the predefined threshold of 10% (p = 0.034) (Figure 2). Two out of the 158 patients (1.3%; 95% CI 0.0%–3.9%) developed bleeding after PS. After the 75th precut procedure, the rate of bleeding was 2.7% (n = 2; 95% CI 0.0%–8.2%), which was significantly lower than the predefined threshold of 10% (p = 0.016) (Figure 2). Both complication rates were consistently maintained below 5.0% beyond the 50th PS performed (Figure 2). Bleeding rates showed a continual decline to 1% up to the 150th PS, while pancreatitis rates remained relatively constant between 2.0%–4.0%. There were no patients with perforation in our study. In addition, no complications occurred in patients requiring repeat procedures after the initial unsuccessful PS.
Probability of complications as a function of the cumulative number of precuts performed.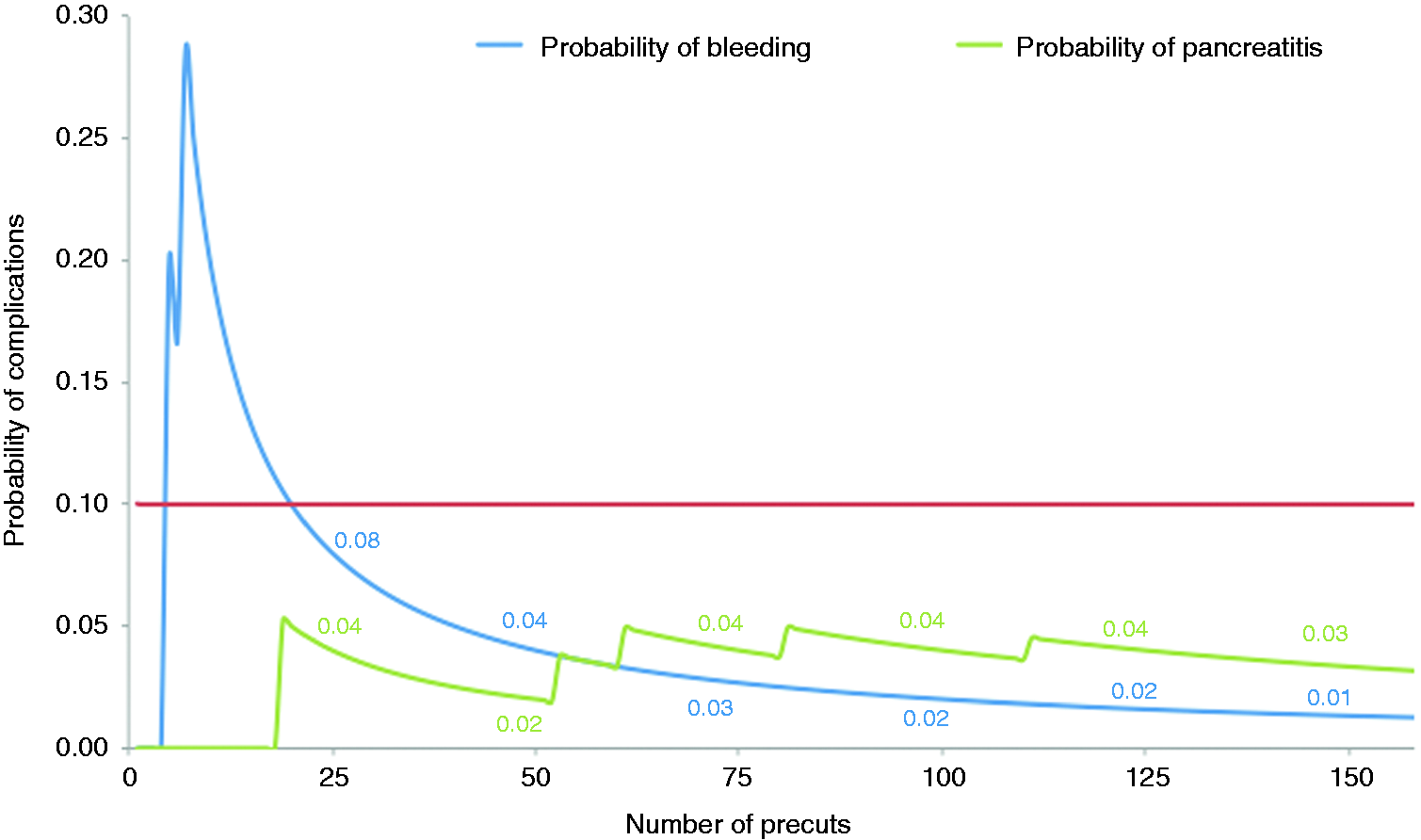
Discussion
This is the first published study to determine the number of PS required to achieve a minimum success rate of 85% at index ERCP, and further evaluated the additional number of PS needed before this success rate can be maintained consistently above 85%. Although there are currently no guidelines which state the minimum acceptable success rate for PS, a benchmark is still required if competency in PS were to be measured by quality indicators and the learning curve and practices of individual endoscopists assessed against these indicators of quality. In general, for all indications, competent ERCP endoscopists should expect to cannulate the duct of interest in more than 90% of ERCP procedures of mild-to-moderate difficulty, even though successful cannulation rates more than 80% are a goal of training programs in ERCP. 1 As PS is considered an advanced technique requiring considerable expertise before fellows can safely attempt to learn how to perform, we decided to use a target of 85% as minimum threshold of success for training and accreditation in PS. 11 We also analyzed the data using a lower target of 80%.
As mentioned in the Introduction, previous studies have gauged improvements in success and complication rates by dividing consecutive patients chronologically into groups and comparing these rates between the groups at the beginning and end of the respective studies. Rollhauser et al. analyzed 68 PS cases performed by a single endoscopist over a six-year period. The cases were divided into the first 22 and the next 46. Immediate, delayed and overall cannulation rates were: 64% vs 74%, 62.5% vs 92% and 86% vs 98%, respectively. 17 Harewood et al. examined 253 PS performed over seven years and divided these chronologically into five groups of 50, with 53 in the final group. The rates of successful cannulation after precut were 88%, 94%, 90%, 88%, and 98%, respectively (p < 0.05 for groups 1–4 vs group 5). Overall complication rates were similar in all groups (12%, 18%, 20%, 12%, and 14%), with no differences in severity of complications. 18 Akaraviputh et al. reported on their experience over three years. A total of 200 consecutive patients underwent PS. All of the procedures were divided into four chronological groups of 50. The success rates of prompt bile duct cannulation after PS were 88%, 86%, 94%, and 82%, respectively (p > 0.05). 19 Robison et al. reviewed their data over an eight-year period. A total of 150 PS procedures were performed. These were divided arbitrarily in chronological order into six groups, with 25 patients in each group. The overall success rate of precut increased over the study period from 84% in group 1 to 92% in group 6. Success during the first attempt at PS also increased from 64% in group 1 to 84% in group 6. The complication rate eased over time from 8% in group 1 to 0% in group 5 and 4% in group 6. However, statistical significance was not reached in any of the analyses. 20 Fukatsu et al. evaluated 104 PS performed over 4 years. The procedures were grouped into two time periods (period A: October 2002–September 2004; period B: October 2004–July 2006). There was no significant difference in the overall success rate between periods A (90%) and B (98%) However, the initial success rate was higher in period B (95%) than in period A (80%) (p < 0.05). The complication rates were similar between both groups. 21
Our findings suggest that an experienced endoscopist requires a minimum of six PS procedures to achieve a probability of success of 85% at index ERCP. However, in order to maintain the success rate above 85%, a total of 13 PS procedures was required (i.e. an additional seven PSs). Furthermore, there was only significant improvement in the success rates following PS after the 125th precut. If a lower competency threshold of 80% is accepted, then the number of procedures required to consistently achieve an 80% success rate was five, and 50 PS was required to achieve further improvement in success rate. These findings confirm that a learning curve for PS exists even for an experienced endoscopist. This is consistent with previously reported improvements in success rates, both initial and overall, with increasing number of procedures performed using PS.
Our study also demonstrated a decrease in complication rates with increasing number of PS. This trend is consistent with the previous studies mentioned. The low overall complication rate in our study (pancreatitis 3.2% and bleeding 1.3%) is also in keeping with low PS complication rates reported in centers where endoscopists perform precut early and routinely for biliary access.7–10 Bleeding rates showed a continued decline up to the 150th PS, whereas pancreatitis rates remained relatively constant beyond the 50th PS. This could arguably be due to the fact that pancreatitis may have resulted from trauma to the papilla by repeated attempts at cannulation before PS is performed, rather than due to needle knife PS in itself. This may explain why the rate of pancreatitis did not seem to decrease in a similar fashion to the rates of bleeding with increasing number of precut procedures, as it may be due to the decision to use this technique after several unsuccessful CBD cannulation attempts rather than a reflection of the proficiency of the endoscopist with PS.
We acknowledge the intrinsic limitations of our study due to its study design. This was a single center retrospective study of the experience of a single endoscopist and hence there is a risk of systemic bias. Also, we could not analyze the time taken to cannulate after PS and how it evolved with time, as this information was not specifically captured. However, all data were captured in a prospective registry and electronic source documents could be retrieved for verification. In addition, the study provides new information over pre-existing studies by defining the minimum number of PS procedures required to achieve acceptable predefined success and complication rates.
In conclusion, an experienced endoscopist requires at least 13 PS procedures to achieve a sustained success rate of 85% or more. Significant improvements in complications of pancreatitis and bleeding below a predefined threshold of 10% were achieved after 50 PSs. Bleeding rates continued to improve beyond this point, but pancreatitis rates remained relatively constant.
Conclusion
Precut is an important ERCP technique for achieving selective cannulation when standard techniques of cannulation fail. However there is no consensus on what constitutes adequate training for needle knife precut. This study revealed that the number of precut procedures required to achieve a probability of success of 85% was six and a success rate of 85% and above was maintained consistently after 13 precut procedures.
Footnotes
Declaration of conflicting interests
The authors have no conflicts of interest to declare.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.