
Abstract
Background
To date, no reliable marker for predicting the severity of post-endoscopic retrograde cholangiopancreatography (ERCP) pancreatitis exists. A previous animal study reported a correlation between serum phosphate level and the severity of acute pancreatitis.
Objective
The purpose of this study was to evaluate the feasibility of serum phosphate as a marker for predicting the severity of post-ERCP pancreatitis in humans.
Methods
A cohort of patients that were diagnosed with post-ERCP pancreatitis between January 2005 and December 2016 was queried. In addition to serum phosphate levels measured between 12 and 24 hours after ERCP, several candidates deemed suitable for accurately predicting the severity of post-ERCP pancreatitis were also explored.
Results
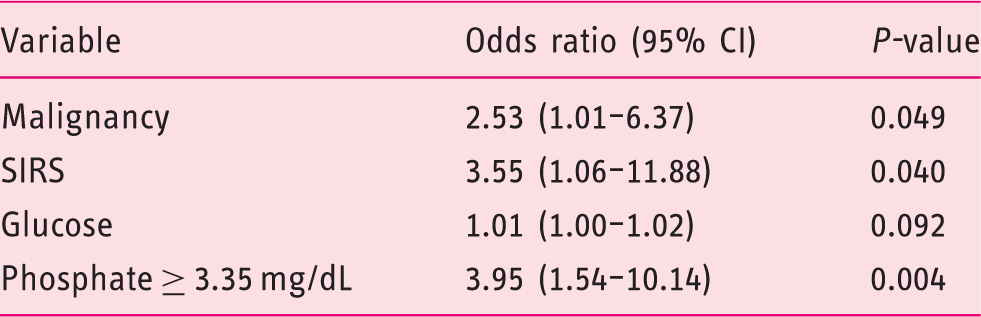
A total of 191 patients with severe (n = 42, 22.0%) and mild-to-moderate (n = 149, 78.0%) post-ERCP pancreatitis were included. Several factors for predicting severe post-ERCP pancreatitis were identified in the multivariate analysis: malignancy as the primary indication for ERCP (odds ratio (OR) 2.65, P = 0.038), systemic inflammatory response syndrome (OR 4.49, P = 0.016) and serum phosphate level (OR 1.97, P = 0.040). In the receiver operating characteristic analysis, the area under the curve of serum phosphate level for severe post-ERCP pancreatitis was 0.65 (95% confidence interval, 0.56–0.75). The optimal cut-off value of serum phosphate level for prediction of severe post-ERCP pancreatitis was 3.35 mg/dL (sensitivity, 0.62; specificity, 0.73).
Conclusions
Serum phosphate level after ERCP can be used as a reliable prognostic marker in predicting the severity of post-ERCP pancreatitis. Future prospective studies would be the cogent next step in validating its value.
Key summary
To date, no reliable marker for predicting the severity of post-ERCP (endoscopic retrograde cholangiopancreatography) pancreatitis exists. This is the first study of serum phosphate that can be considered as a marker for predicting the severity of post-ERCP pancreatitis. This study showed that serum phosphate is useful for predicting severe post-ERCP pancreatitis rather than the BISAP (bedside index of severity in acute pancreatitis) score used to predict the prognosis of acute pancreatitis. This study presented a cut-off value of serum phosphate, measured in the first 24 hours after ERCP, which is appropriate for predicting severe post-ERCP pancreatitis.
Introduction
Acute pancreatitis is the most common major adverse event after endoscopic retrograde cholangiopancreatography (ERCP). 1 The reported rate of post-ERCP pancreatitis ranges between 1.6 and 13.3%, and depends on patient selection and endoscopists’ proficiency.2–5 Post-ERCP pancreatitis incurs substantial morbidity, increased health care costs and even occasional death. 6 Several established risk factors of post-ERCP pancreatitis to date include prior episode of post-ERCP pancreatitis, suspected sphincter of Oddi dysfunction (SOD), female gender, younger age, pre-cut or pancreatic sphincterotomy, and difficult cannulation.2,7,8 Numerous studies have been conducted focusing on the prevention of post-ERCP pancreatitis in high-risk patients.8–14 To date, the prognostic marker predicting the severity of post-ERCP pancreatitis has not clearly been established. Instead, various prognostic scoring systems that were originally developed to predict the severity of acute pancreatitis are utilized in prognosticating the severity of post-ERCP pancreatitis without validation. Furthermore, as these scoring systems contain many components, but some parameters are not commonly measured in practice, not only may they be cumbersome but they may also be less clinically useful. A recent animal study in rats has found that the severity of acute pancreatitis correlates with serum phosphate levels. 15 This study suggests that extracellular purinergic metabolism is activated in acute pancreatitis, leading to increased nucleotide hydrolysis by ectonucleotidases, which in turn increases serum phosphate. To our knowledge, no studies investigating the association between serum phosphate levels and the severity of acute pancreatitis, including post-ERCP pancreatitis, exist in humans. Thus, we sought to assess the feasibility of using serum phosphate level as an early marker of accurately predicting the severity of post-ERCP pancreatitis in humans.
Methods
Patient and data collection
A prospectively collected database registry on 11,715 patients who underwent ERCP from Seoul National University Hospital between January 2005 and December 2016 was queried and reviewed. All ERCPs were performed by three expert endoscopists who performed more than 500 cases of ERCP annually. The patients who met the criteria for the diagnosis of post-ERCP pancreatitis were divided into two groups, severe vs. mild-to-moderate post-ERCP pancreatitis, and the relationship between serum phosphate level and the severity of post-ERCP pancreatitis was ascertained.
Demographic and endoscopic data including age, sex, underlying diagnosis (malignant vs. benign) and purpose (diagnostic vs. therapeutic) of ERCP, clinically suspected SOD, pre-cut or pancreatic sphincterotomy, and placement of pancreatic stent were obtained from archived and electronic medical records. The clinical data consisting of laboratory values containing serum amylase, lipase, complete blood counts, C-reactive protein (CRP), albumin, glucose, blood urea nitrogen (BUN), creatinine, calcium and phosphate, which were collected between 12 and 24 hours after ERCP, were also obtained. Mental status and the physiological data including body temperature, heart rate and respiratory rate were routinely checked immediately after ERCP and after four hours, and every eight hours thereafter. Of these, we collected data between 12 and 24 hours after ERCP. The presence of pleural effusion was confirmed by chest X-ray performed between 12 and 24 hours after ERCP. The two groups were compared on several parameters; haematocrit, BUN, CRP and bedside index of severity in acute pancreatitis (BISAP) score (≥3 points), all of which are known to possess a variable degree of prognosticating capability for the degree of acute pancreatitis.16–19 Several variables with significant differences between the two groups found in baseline characteristics were also analyzed for possible candidacy as a predictor of severity of post-ERCP pancreatitis. The study protocol was based on the Declaration of Helsinki and approved by the Institutional Review Board (IRB) of Seoul National University Hospital (IRB approval number/date: 1708-049-876/Aug-16-2017). The requirement for informed consent was waived.
Study outcomes and definition
The primary outcome of interest was the capability of serum phosphate level to accurately predict the severity of post-ERCP pancreatitis. The secondary outcome of interest was to identify the cut-off value of serum phosphate level for optimal sensitivity and specificity in predicting severe post-ERCP pancreatitis. The diagnosis of post-ERCP pancreatitis was established when the serum amylase or lipase levels were elevated to more than three times the upper limit of normal with newly developed abdominal pain lasting at least 24 hours after ERCP. 20 We defined the severity of post-ERCP pancreatitis according to the consensus guidelines: mild (post-ERCP pancreatitis requiring hospitalization for less than or equal to three days); moderate (post-ERCP pancreatitis requiring hospitalization of 4–10 days) and severe (post-ERCP pancreatitis requiring hospitalization for more than 10 days). 20 Systemic inflammatory response syndrome (SIRS) was defined by at least two or more of the following clinical manifestations: a body temperature of > 38℃ or < 36℃, heart rate of > 90 beats/minute, respiratory rate > 20 breaths/minute, and white blood cell count of > 12,000 cells/mm3 or < 4,000 cells/mm3. 21
Statistical analysis
Data were shown as the mean ± SD for continuous variables and the number (%) for categorical variables. Comparisons between groups were performed using the independent samples Student’s t-test, χ2-test and Fisher’s exact test as deemed appropriate. The correlations of serum phosphate were assessed using the Spearman’s rank correlation coefficient (rs). Univariate analysis was performed to screen predictors of severe post-ERCP pancreatitis. In addition, multivariate analysis calculating the odds ratio (OR) using logistic binary regression was added on the variables that were deemed significant for predicting severe post-ERCP pancreatitis in the univariate analysis. A receiver operating characteristic (ROC) curve was generated and area under the curve (AUC) was calculated to determine the cut-off value of the serum phosphate for predicting severe post-ERCP pancreatitis. The optimal cut-off value for serum phosphate in the ROC curve was determined on the basis of the Youden index (sensitivity + specificity – 1). Stratified analysis was performed on malignancy to assess the interaction effect with serum phosphate. A P-value < 0.05 was considered statistically significant. Statistical analyses were performed with SPSS 23.0 (SPSS Inc., Chicago, Illinois, USA).
Results
Clinical characteristics of patients
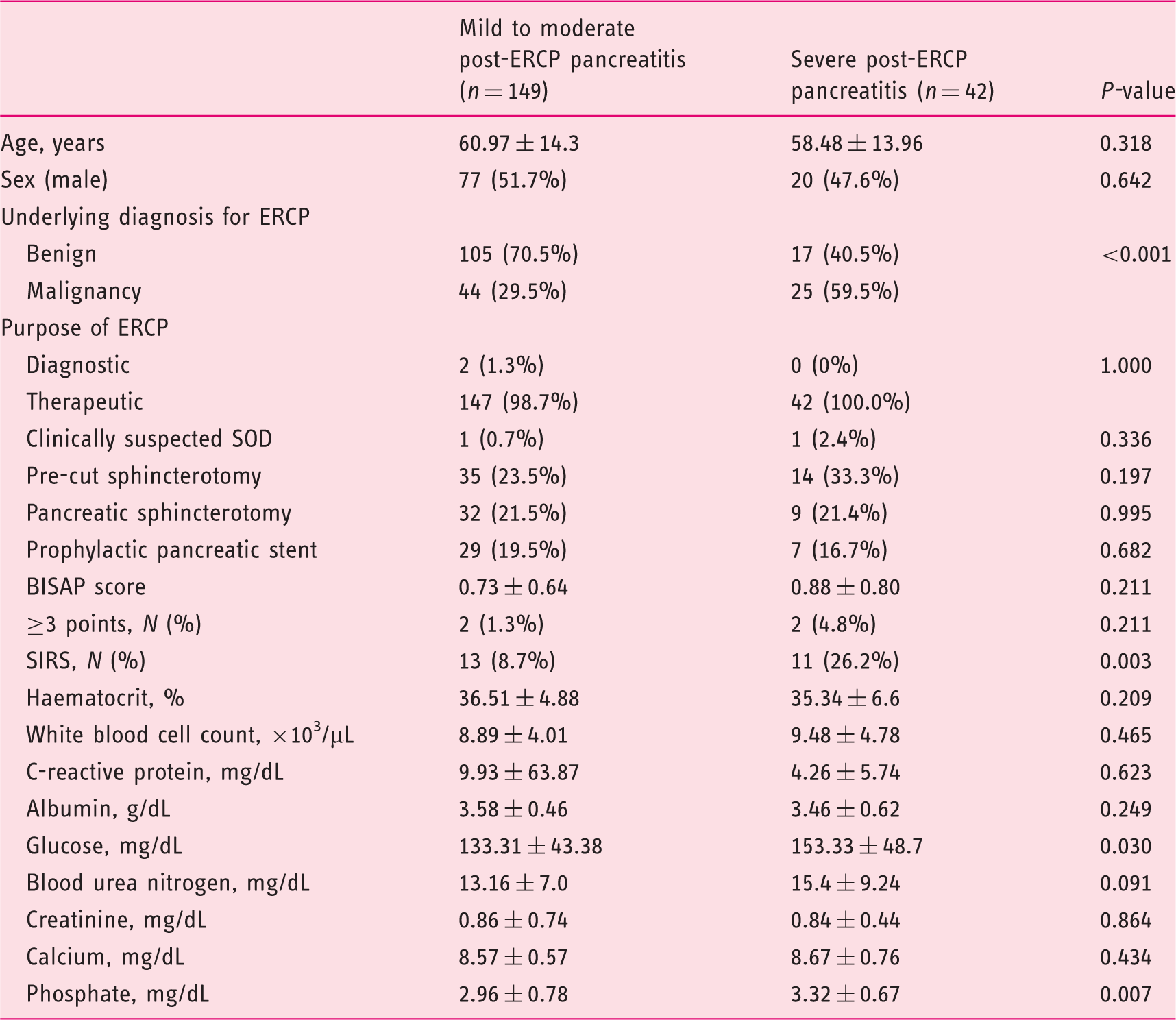
From 11,715 patients who underwent ERCPs during the study interval, 323 patients (2.8%) met the criteria for post-ERCP pancreatitis. Of these, 191 patients (59.1%) had serum phosphate level measured during the designated time interval, hence were included (Figure 1). Of the 191 post-ERCP pancreatitis patients, 69 (36.1%) had mild, 80 (41.9%) had moderate and 42 (22.0%) had severe post-ERCP pancreatitis. The severe post-ERCP pancreatitis (n = 42) group did not differ significantly from the mild-to-moderate post-ERCP pancreatitis group (n = 149) with respect to age, sex, purpose of ERCP, clinically suspected SOD, pre-cut or pancreatic sphincterotomy, pancreatic stent insertion rate for post-ERCP pancreatitis prevention, and laboratory data except glucose and phosphate (Table 1). Malignancy as the underlying diagnosis for ERCP was observed more frequently in the severe post-ERCP pancreatitis group than the mild-to-moderate post-ERCP pancreatitis group (59.5% vs. 29.5%, respectively, P < 0.001). The incidence of SIRS was also significantly higher in the severe post-ERCP pancreatitis group. No significant difference in BISAP score was observed between the two groups. Spearman’s correlation coefficient measurement revealed a significant positive correlation between serum phosphate level and the severity of post-ERCP pancreatitis (rs = 0.217, P < 0.003) (Table 2).
Study flow chart. Baseline characteristics of patients. ERCP: endoscopic retrograde cholangiopancreatography; SOD: sphincter of Oddi dysfunction; BISAP: bedside index of severity in acute pancreatitis; SIRS: systemic inflammatory response syndrome. Correlations between serum phosphate and severe post-ERCP pancreatitis. ERCP: endoscopic retrograde cholangiopancreatography.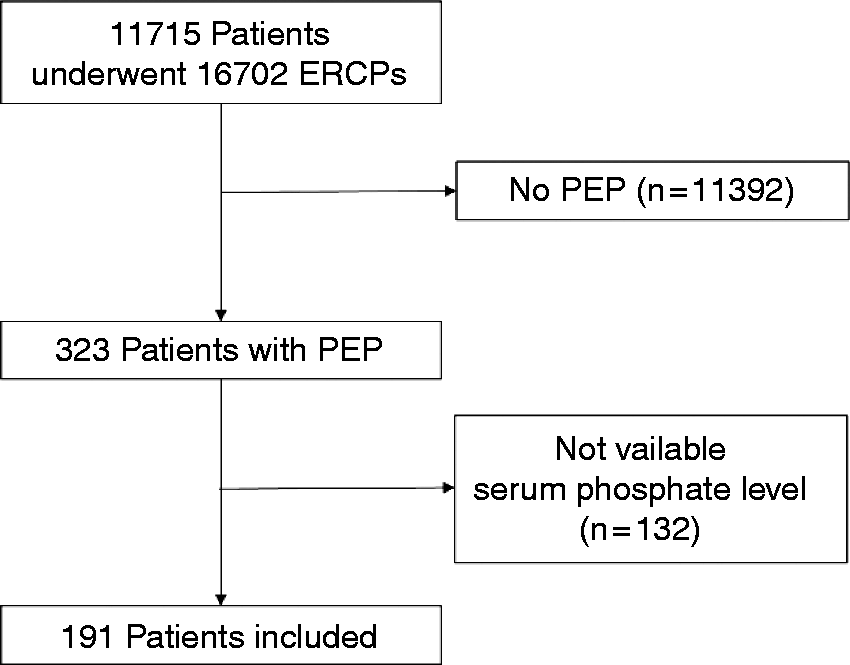

Factors predicting severe post-ERCP pancreatitis
The results of simple logistic regression to predict severe post-ERCP pancreatitis.
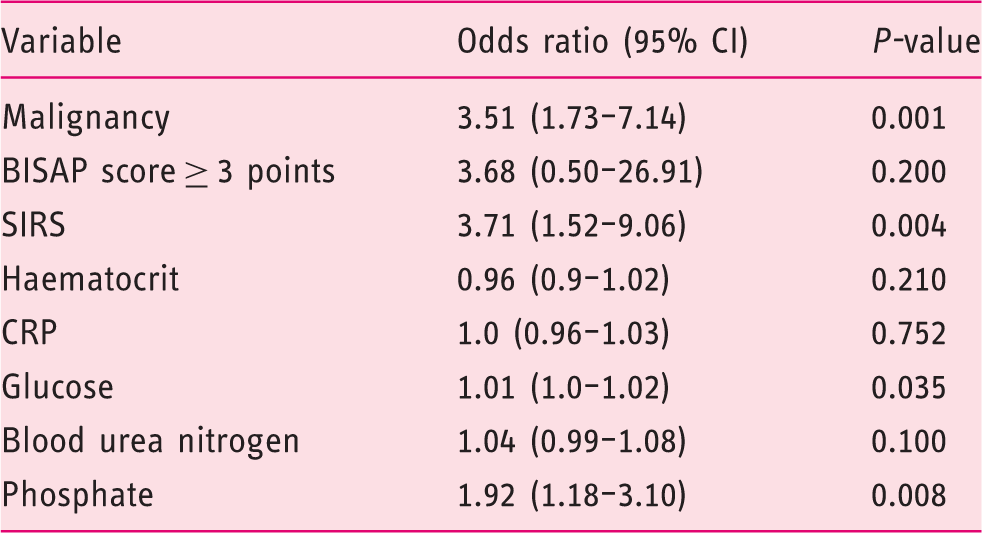
ERCP: endoscopic retrograde cholangiopancreatography; CI: confidence interval; BISAP: bedside index of severity in acute pancreatitis; SIRS: systemic inflammatory response syndrome.
The results of multiple logistic regression to predict severe post-ERCP pancreatitis.
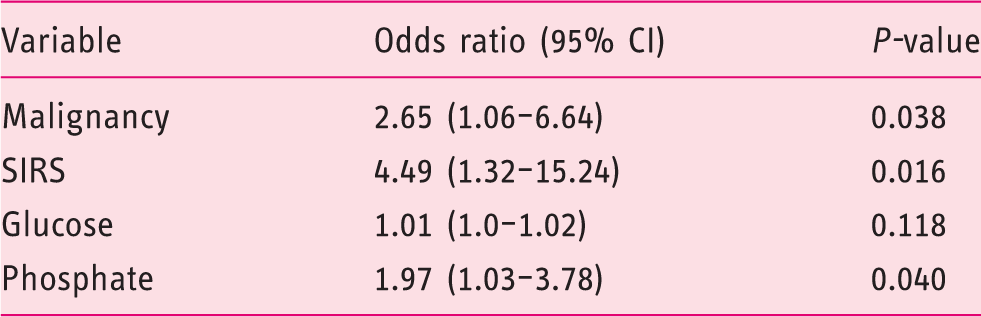
ERCP: endoscopic retrograde cholangiopancreatography; CI: confidence interval; SIRS: systemic inflammatory response syndrome.
Figure 2 illustrates the ROC curve for serum phosphate level to predict severe post-ERCP pancreatitis. The AUC of serum phosphate for severe post-ERCP pancreatitis was 0.65 (95% confidence interval: 0.56–0.75). On the basis of the Youden index, the optimal cut-off value for serum phosphate level was 3.35 mg/dL for predicting severe post-ERCP pancreatitis (sensitivity, 0.62; specificity, 0.73).
Receiver operating characteristic (ROC) curves for serum phosphate in the prediction of severe post-ERCP (endoscopic retrograde cholangiopancreatography) pancreatitis. The selected cut-off value is highlighted, and the values of area under the ROC curve (AUC) with 95% confidence intervals are shown on the graph.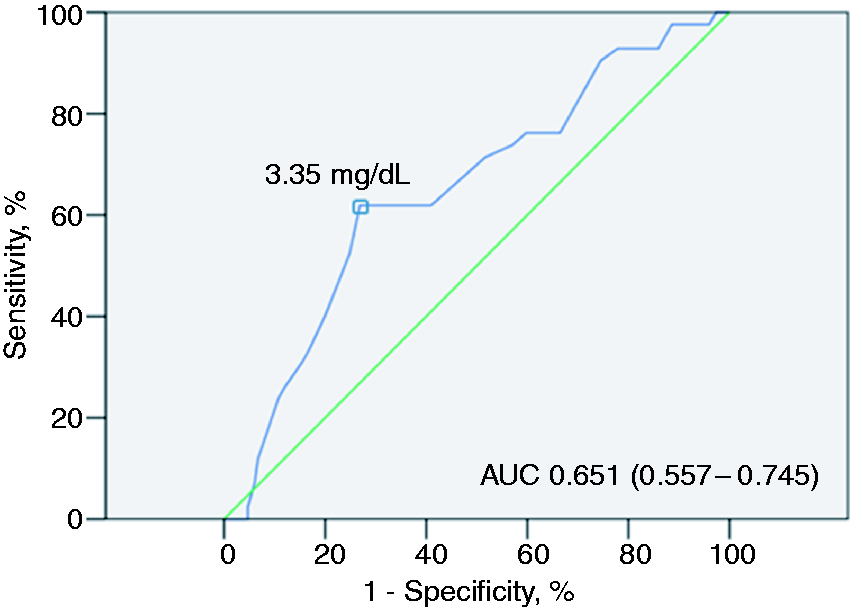
Stratified analysis of a subgroup with malignancy and a subgroup with benign disease showed that serum phosphate levels above the cut-off value (3.35 mg/dL) were significantly associated with severe post-ERCP pancreatitis in both the subgroup with malignancy (OR 3.71, P = 0.015) and subgroup with benign disease (OR 3.35, P = 0.026).
The results of multiple logistic regression with cut-off value of serum phosphate.
CI: confidence interval; SIRS: systemic inflammatory response syndrome.
Discussion
In this study, we demonstrated the statistically significant association between serum phosphate measured between 12 and 24 hours after ERCP in patients with post-ERCP pancreatitis and the severity of post-ERCP pancreatitis. The first study ever to report a relationship between serum phosphate and the severity of acute pancreatitis was an animal study by Mazzini and colleagues. 15 To our knowledge, this is the first study to date reporting such relationship with post-ERCP pancreatitis, a type of acute pancreatitis in human subjects.
Post-ERCP pancreatitis is one of the common adverse events of ERCP and requires an appropriate level of care according to its severity. Even if one can readily recognize the presence of post-ERCP pancreatitis, lack of ability to predict its severity early on may hamper the administration of judicious and appropriate management. Currently available prognostic scoring systems are not designed for post-ERCP pancreatitis, and no study has compared the prognosis of post-ERCP pancreatitis with several established prognostic factors/scoring systems used in acute pancreatitis.
Currently, the Acute physiology and chronic health evaluation (APACHE) II score, 22 the Ranson criteria, 23 and the BISAP score 16 are the most commonly used scoring systems used as prognosticating tools for acute pancreatitis. The APACHE II score and the Ranson criteria are somewhat complex and include factors not commonly measured in clinical practice. The cumbersome nature of these scoring systems can discourage apt and timely utilization, negating their original intent. Borne out of shared frustration, the BISAP score, a simpler scoring system, was created and has shown prognostic accuracy similar to APACHE II or Ranson criteria.16,24 However, our study demonstrated that serum phosphate level was more useful and perhaps more accurate than the BISAP score in predicting the severity of post-ERCP pancreatitis. On the other hand, SIRS, which is a component of the BISAP score and has been reported to be useful in predicting the severity of acute pancreatitis when assessed on the first day of acute pancreatitis, 25 also showed valid results for the prediction of severe post-ERCP pancreatitis in this study. One potential advantage of serum phosphate over SIRS is the simplicity in data collection and consistency in its value. An accurate diagnosis of SIRS requires acquisition of the composite vital signs that may not be consistent depending on the mode and time of acquisition. This study also showed that malignancy was associated with the severity of post-ERCP pancreatitis. One plausible explanation is that as the measurement of severity of post-ERCP pancreatitis rests on the length of hospital stay, the management of malignancy related issues, in addition to the treatment of pancreatitis, may contribute to prolonged hospitalization. We also evaluated several other factors associated with the prognosis of acute pancreatitis, such as haematocrit, BUN and CRP based on previous studies that reported significant associations between the aforementioned factors and the severity of acute pancreatitis.17–19 However, our study did not reveal any significant relationship between their values and the severity of post-ERCP pancreatitis. A retrospective study by Wu and colleagues reported a significant correlation between the mortality rate from acute pancreatitis and the level of change in BUN from admission to 24 hours after admission. 18 As not all of the subjects with post-ERCP pancreatitis in our study had both the admission and 24-hour post-admission BUN levels available, we used one time BUN rather than its change (delta), which may explain the null finding observed in this study. CRP is known to reflect the prognosis of acute pancreatitis when measured at 48 hours after acute pancreatitis. 26 However, CRP level was obtained between 12 and 24 hours after ERCP in our study, hence may not be an accurate reflection of the impending severity of disease due to premature collection. We found an optimal serum phosphate cut-off value of 3.35 mg/dL for the prediction of severe post-ERCP pancreatitis based on ROC analysis, with a sensitivity of 62% and a specificity of 73%. Based on these results, we conducted a multivariate analysis for the variables that were deemed significant in the univariate analysis, with serum phosphate levels > 3.35 mg/dL being the new variable. As a result, we found that the risk of severe post-ERCP pancreatitis increases with an OR of 3.95 for patients with serum phosphate levels > 3.35 mg/dL (Table 5). Therefore, a cogent guideline for assigning an appropriate level of care for patients with post-ERCP pancreatitis based on serum phosphate levels can be considered.
There are some limitations in this study. First, the current study is limited by the fact that observational data were derived from a retrospective analysis. Second, we adopted the absolute level of serum phosphate after ERCP rather than the change from baseline. Since the baseline serum phosphate level was not generally measured prior to ERCP, it was not possible to calculate the change in serum phosphate in this study. Nevertheless, a cogent correlation between phosphate level and the severity of post-ERCP pancreatitis, demonstrated for the first time through this study, certainly warrants further assessments in its validation and clinical utility.
In conclusion, our study showed that serum phosphate level was closely associated with severe post-ERCP pancreatitis. If validated, it can be used as a valuable prognostic marker. Earlier prediction of severe post-ERCP pancreatitis using serum phosphate may lead to more effective decision-making when determining appropriate levels of care for patients with post-ERCP pancreatitis.
Footnotes
Acknowledgement
We thank Medical Research Collaborating Center Seoul National University Hospital for assistance with statistical analysis.
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethics approval
The study protocol was based on the Declaration of Helsinki and approved by the Institutional Review Board (IRB) of Seoul National University Hospital (IRB Approval Number/Date: 1708-049-876/Aug-16-2017).
Informed consent
The requirement for informed consent for this study was waived.