
Abstract
Background and objective
Despite intensive colonoscopic surveillance, a substantial proportion of Lynch syndrome (LS) patients develop colorectal cancer (CRC). The aim of this study was to characterize incident CRC in LS patients.
Methods
All patients diagnosed with incident CRC after start of colonoscopic surveillance were identified in the Dutch LS Registry of 905 patients. A retrospective analysis of patient records was carried out for patient characteristics, survival, CRC characteristics and findings of previous colonoscopy.
Results
Seventy-one patients (7.8%) were diagnosed with incident CRC. Median interval between incident CRC diagnosis and previous colonoscopy was 23.8 (range 6.7–45.6) months. Median tumor diameter was 2.5 cm, and 17% of the tumors were sessile or flat. Most patients (83%) had no lymph node metastases. There was no association between tumor size and colonoscopy interval or lymph node status. Most patients (65%) had no adenomas during previous colonoscopy. Two patients (2.8%) eventually died from metastatic CRC.
Conclusion
The high frequency of incident CRC in LS likely results from several factors. Our findings lend support to the hypothesis of fast conversion of adenomas to CRC, as 65% of patients had no report of polyps during previous colonoscopy. High-quality colonoscopies are essential, especially as tumors and adenomas are difficult to detect because of their frequent non-polypoid appearance. Early detection due to surveillance as well as the indolent growth of CRC, as demonstrated by the lack of lymph node metastases, contributes to the excellent survival observed.
Key summary
Established knowledge
‐ Colonoscopic surveillance and the timely removal of adenomas have been shown to decrease the risk of colorectal cancer in patients with Lynch syndrome. ‐ Possible reasons for developing cancer despite surveillance include missed tumors due to suboptimal colon preparation, incomplete colonoscopy and incomplete removal of adenomatous tissue during previous colonoscopy. ‐ Until now, the adenoma and tumor characteristics and their contribution to colorectal cancer development in Lynch syndrome patients have not been investigated in detail.
Significant findings of this study
‐ Most patients (65%) had no polyps during previous colonoscopy, which supports the hypothesis of fast conversion of adenomas to cancer. ‐ The tumors were generally small (median diameter 2.5 cm), the majority of patients (83%) had no lymph node metastases, and no association was found between screening interval and tumor size or tumor size and lymph node metastases, all of which support the hypothesis of indolent growth of colorectal cancer in Lynch syndrome. ‐ The frequent non-polypoid appearance of adenomas and tumors makes colonoscopic detection of these lesions more difficult.
Introduction
Colorectal cancer (CRC) is one of the most common cancers both in women and in men, with a yearly incidence rate of more than 470,000 in Europe. 1 In approximately 3% of the cases, CRC can be attributed to Lynch syndrome (LS). 2 LS is caused by mutations in one of the DNA mismatch-repair (MMR) genes MLH1, MSH2, MSH6, and PMS2, and is inherited in an autosomal-dominant manner. 2
The prevention of CRC in LS patients is based on regular colonoscopic surveillance and the removal of adenomas. Current guidelines recommend a screening interval between one and two years. 2 However, despite intensive surveillance, the CRC incidence rate in the LS population is as high as 13% per 10 years. 3 In Finland, where the surveillance interval was set at two to three years, the cumulative risk of CRC at 60 years was found to be 35% in men and 22% in women. 4
The high rate of incident CRC in LS patients under surveillance has prompted several studies in the field. Possible explanations for the development of CRC include missed tumors due to suboptimal colon preparation, incomplete colonoscopy and incomplete removal of adenomatous tissue during previous colonoscopy. 5 Adhering to quality parameters such as documentation of cecal intubation or prolonged withdrawal time can increase adenoma detection rates. 6 Furthermore, non-polypoid adenomas are more frequently observed in LS patients than in people at an average risk for CRC. 7 Compared to regular polyps, these flat lesions might be more difficult to detect. It has further been suggested that the adenoma-carcinoma sequence is accelerated in LS. In contrast to sporadic CRC where adenomas take 10 years to develop into cancer, in LS small adenomas may develop into cancer even within a time frame of one to two years. There is also some evidence that some LS tumors might follow a non-polypoid pathway in which invasive growth occurs directly from seemingly normal mucosa. 8
At the moment, it is unclear which factors contribute the most to the development of incident CRC in LS patients. Understanding how these cancers arise will help to more effectively prevent CRC in this population. To this end, we designed a study with data from a prospectively collected database in Dutch LS patients. We evaluated the features of incident CRC in LS patients, both at the patient level and at tumor level. We assessed patient survival after CRC diagnosis. Finally, we examined the quality and findings of previous colonoscopy.
Methods
Study design and data collection
We analyzed prospectively collected data from the Dutch LS Registry. The LS Registry coordinates surveillance in hereditary CRC and was established in 1989. Its aims are to improve identification of hereditary CRC, to promote participation in surveillance programs, and to evaluate the screening protocol. In clinical practice, reminders for surveillance are sent to treating physicians and results of screening are collected in the database. All patients who had been registered before October 2012 and diagnosed with incident CRC after registration and before January 2017 were included. Some of the patients in this cohort were included in an earlier cohort study examining the associations between colonoscopy quality and incident CRC. 5 Most of the patients in this study were included in a recent European study 3 that compared the effect of various surveillance intervals (one to three years) in LS patients on the incidence of CRC and tumor stages. The study was approved by the research committee of The Netherlands Foundation for the Detection of Hereditary Tumors on July 1, 2017. All patients have given written permission for registration and anonymous evaluation of results. The study protocol conforms to the ethical guidelines of the Declaration of Helsinki.
Study cohort
Proven and obligate carriers of an MMR gene mutation who developed CRC during the surveillance period were included in the analysis. Patients with CRC before registration who were diagnosed with a new CRC after registration were also included, but only CRC diagnosed after registration was included in the analysis.
Collected data
For each patient, birth date, gender, gene defect, history and surgical treatment of CRC, date of last contact or date of death and cause of death were recorded. The histological grade, size, morphology, TNM stage, and location of incident CRC were recorded. In case of synchronous tumors, only the highest TNM stadium was considered. Cancer was considered metastatic if radiological evidence for metastases was available at the time of surgery. The location of the tumor was classified according to the colon segments cecum, ascending colon, hepatic flexure, transverse colon, splenic flexure, descending colon, sigmoid, and rectum. The date of incident CRC diagnosis was defined either as the date of colonoscopy where the tumor was found or the date of surgery if colonoscopy date was not recorded. For patients with multiple CRCs during the surveillance period, information on the first CRC was collected. Characteristics of previous colonoscopy were noted as follows: colonoscopy date, visualization of the whole colon, degree of bowel preparation, whether polypectomy had been performed, and the number, location, grade, size and morphology of removed polyps.
Statistical methods
Frequencies are presented as absolute numbers and percentages. Continuous data are presented as mean (standard deviation (SD)), and in the case of non-normally distributed data as median (interquartile (IQR)) range. The Shapiro-Wilk statistic for testing normality was used. To test for an association between two variables or a difference between two groups, Pearson χ2 test or Spearman’s rho were used depending on the distribution of the data. To test for a difference between three groups, a one-way analysis of variance was used. The tests were considered statistically significant if p < 0.05. All analyses were performed using IBM SPSS Statistics for Mac, version 24.0.
Results
1. Patient characteristics
Mutation distribution and incident CRC.
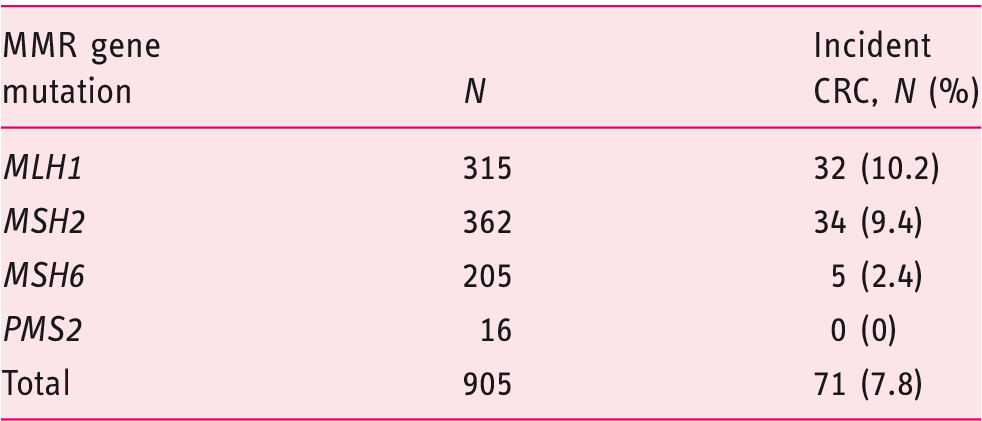
CRC: colorectal cancer; MMR: mismatch repair.
Follow-up of the Lynch syndrome cohort and incidence of CRC per surveillance period.
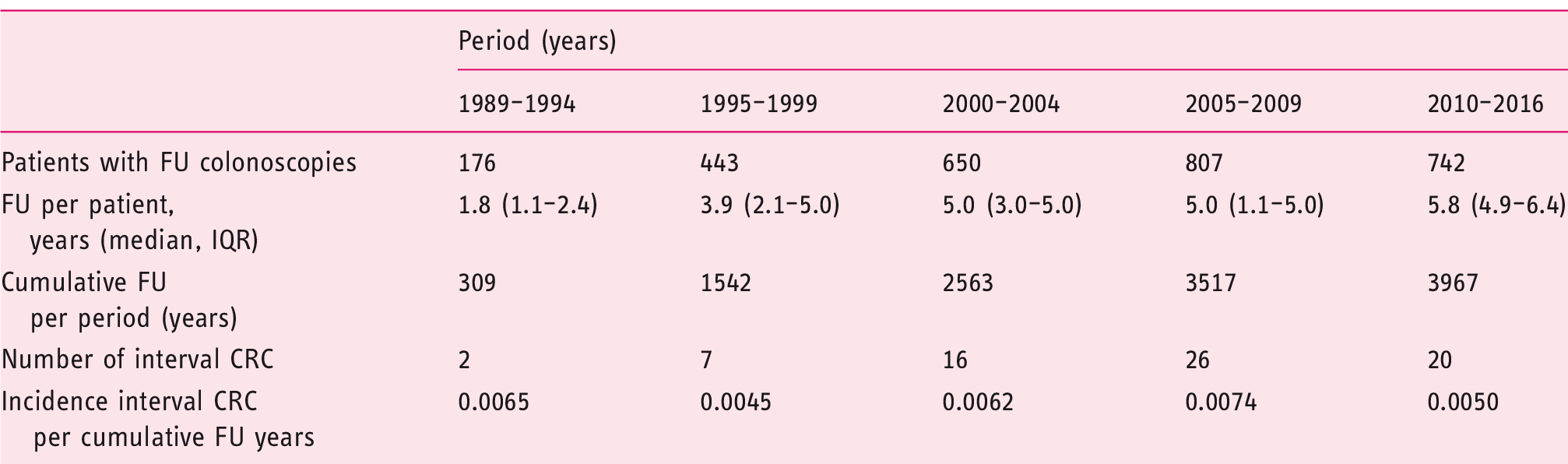
CRC: colorectal cancer; FU: follow-up; IQR: interquartile range.
Twenty patients had been diagnosed with CRC prior to registration. Nineteen patients had undergone a partial colon resection. The median observation time between registration and incident CRC diagnosis was 8.9 (range 0–20.2) years. Mean age at incident CRC diagnosis was 51.6 (SD 10.3) years. Half of the patients were male. The difference in age at CRC diagnosis between the three groups of MMR mutation carriers was not statistically significant. The mean screening interval was 23.2 (SD 8.9) months, ranging from 6.7 to 45.6 months.
Patient characteristics.
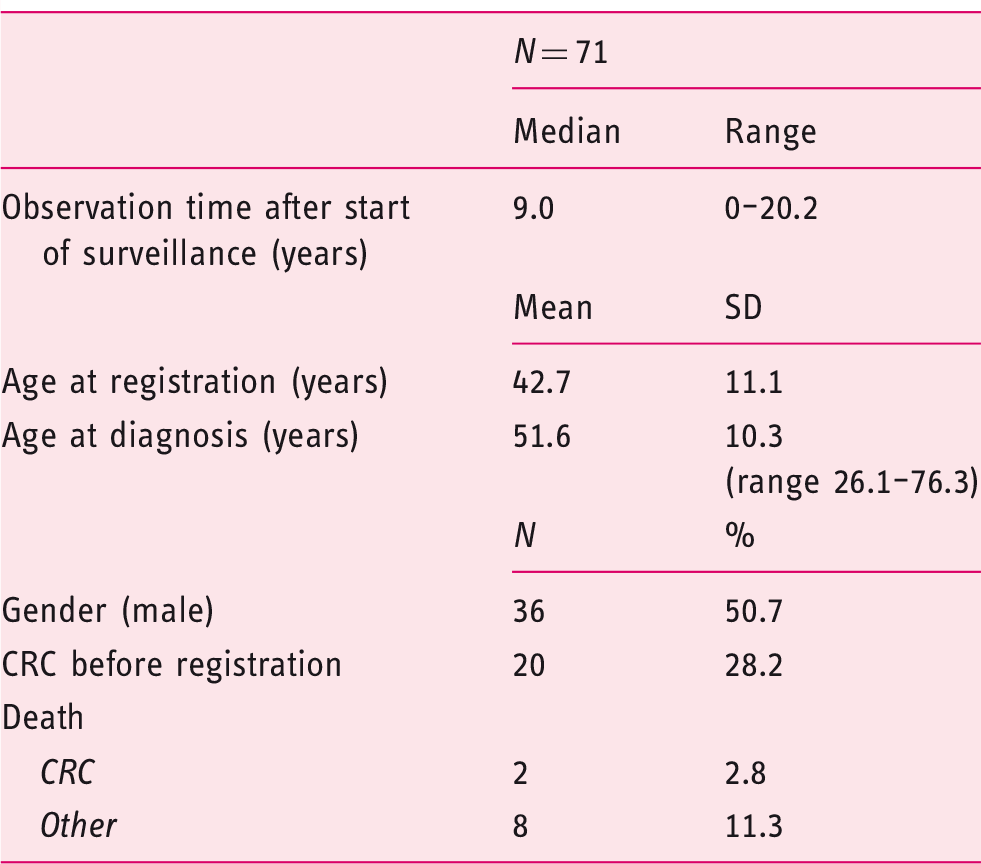
CRC: colorectal cancer.
2. Characteristics of incident CRC
(a) Tumor staging
A total of 76 tumors were discovered in 71 patients. Most tumors were located in the proximal colon, the cecum being the most common location.
Tumor stage according to the TNM classification was available for 70 patients: Eighteen patients had T1, 26 patients had T2, 25 patients had T3, and one patient had T4. One patient had a T3 or T4 tumor. Fifty-nine patients had no lymph node metastases, 11 had N1, and one patient had N2. No patients had distant metastases at the time of diagnosis.
(b) Tumor size and morphology
Features of incident CRC.
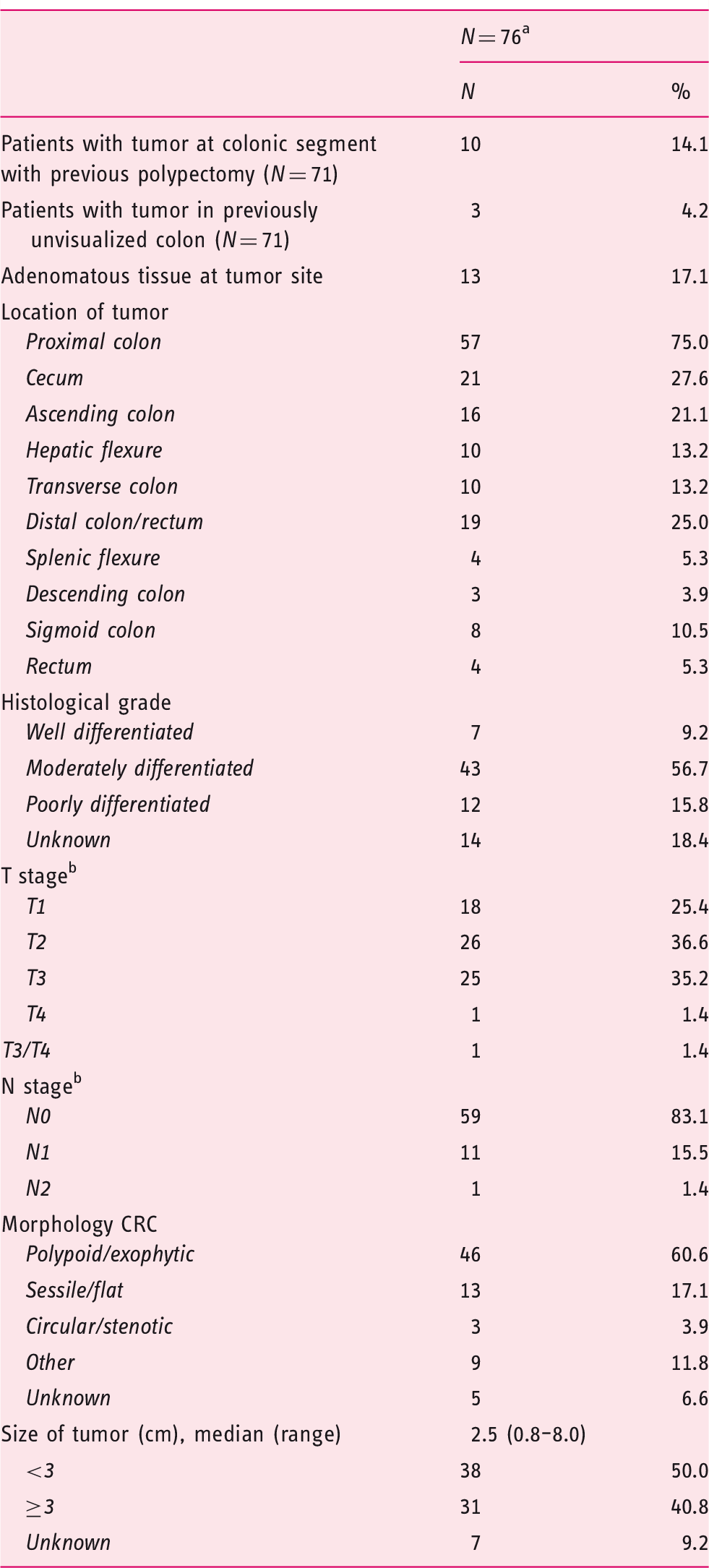
CRC: colorectal cancer.
Five patients had two synchronous tumors.
Only highest stage CRC considered per patient.
3. Quality and outcome of previous colonoscopy
For 66 patients, information was available on the colonoscopy preceding incident CRC diagnosis. Suboptimal colon preparation was described in two cases. Full colon visualization was not performed in three cases. Two of these patients had undergone a barium enema or computed tomography-colography, and for one patient it was unclear whether a barium enema had been performed. All three patients developed subsequent CRC in the previously unvisualized part of the colon.
Polypectomy was performed in 22 patients during their previous colonoscopy; a total of 34 polyps were detected and removed. Most patients had one polyp removed. The median diameter of the polyps was 3 mm (range 1–14 mm).
Twenty-one polyps had low-grade dysplasia, one had high-grade dysplasia, and six were hyperplastic. Of the adenomatous polyps, 12 were described as sessile or flat, and one was described as pedunculated. Serrated polyps were not described in any of the colonoscopy or histopathology reports.
Quality and findings of previous colonoscopy.
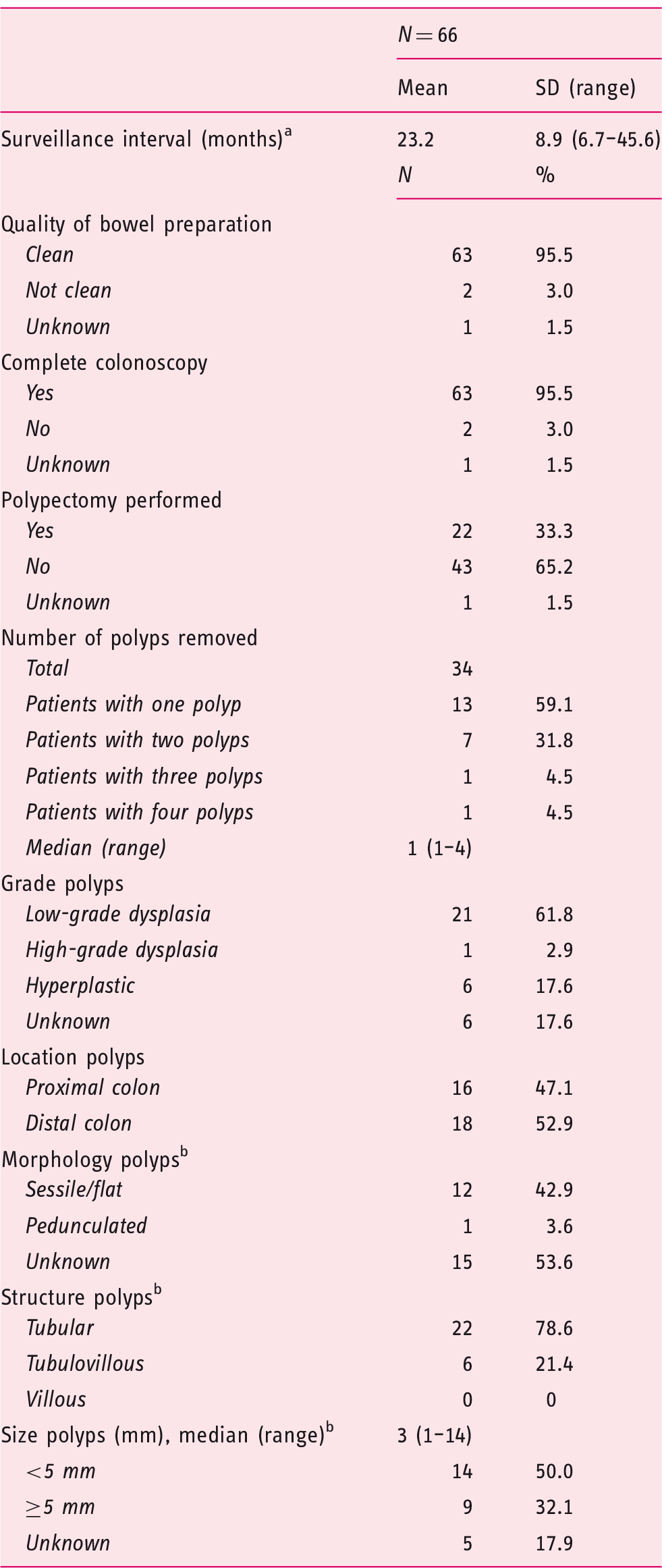
Available for 65 patients.
Adenomatous polyps, N = 28.
Discussion
Despite intensive colonoscopic surveillance, 7.8% of LS patients in the Dutch LS Registry developed CRC. Incident CRC was more often found in MLH1 and MSH2 mutation carriers compared to MSH6 mutation carriers, and no incident CRC was diagnosed in PMS2 mutation carriers. These results are in agreement with other previously published studies.9,10 MSH6 mutation carriers generally develop cancer at a later age than patients with MLH1 or MSH2 mutations. 11 However, as our cohort included only five MSH6 mutation carriers with incident CRC, we lacked statistical power to detect a difference in age among the three groups.
More than 60% of the patients had T1/2 disease, less than one-fifth had lymph node metastases, and no patients had distant metastases at the time of diagnosis. Accordingly, the overall survival in our cohort exceeded 85% with less than 3% dying from metastatic CRC. Similar survival figures have been previously reported by Møller et al. 11 Early diagnosis probably contributes to the excellent survival.
Good-quality surveillance colonoscopies are important in preventing CRC in LS. Poor bowel preparation is associated with a reduced detection of small or flat lesions. 12 Visualization of the entire colon is necessary because of the high frequency of LS CRC in the proximal colon. Furthermore, residual adenomatous tissue after incomplete polypectomy can develop into cancer. In our cohort, 4% of patients developed CRC in previously unvisualized segments of the colon, and almost 50% of patients had CRC in the same colonic segment where polypectomy had previously been performed. Other factors such as sedation practice and withdrawal time can affect the quality of the surveillance colonoscopy. 6 Given that data for this study were gathered over a 30-year period, information on modern parameters assessing the quality of the colonoscopy was largely missing from the reports. Even so, it seems that colonoscopy quality has been improving in recent years as the incidence of CRC per cumulative follow-up years decreased by almost 40% from 2000–2009 to 2010–2016.
The morphology of colorectal neoplasms in LS may differ from that in sporadic CRC. Most tumors in our cohort were exophytic similar to non-LS CRCs, but nearly one-fifth were sessile or flat and at least one-half had a diameter of less than 3 cm. In contrast, flat cancers represented 10% of all CRC found in 1026 consecutive colonoscopies in a series of patients that also included patients with a family history of cancer. 13
Almost one-half of the polyps in the previous colonoscopy were also described as sessile or flat. Previous research has reported on a high frequency of non-polypoid lesions in LS.
7
An example of such a lesion in an LS patient is shown in Figure 1. Besides being more difficult to detect, flat adenomas have been associated with a higher degree of malignant potential. Invasive cancer is found in non-polypoid lesions at a smaller size as compared with polypoid lesions.13,14 High-grade dysplasia14,15 and invasion of the submucosal layer
14
are also more often reported in flat lesions than in polypoid lesions.
Non-polypoid adenoma of 15 mm in the ascending colon in a Lynch syndrome patient with MLH1 mutation.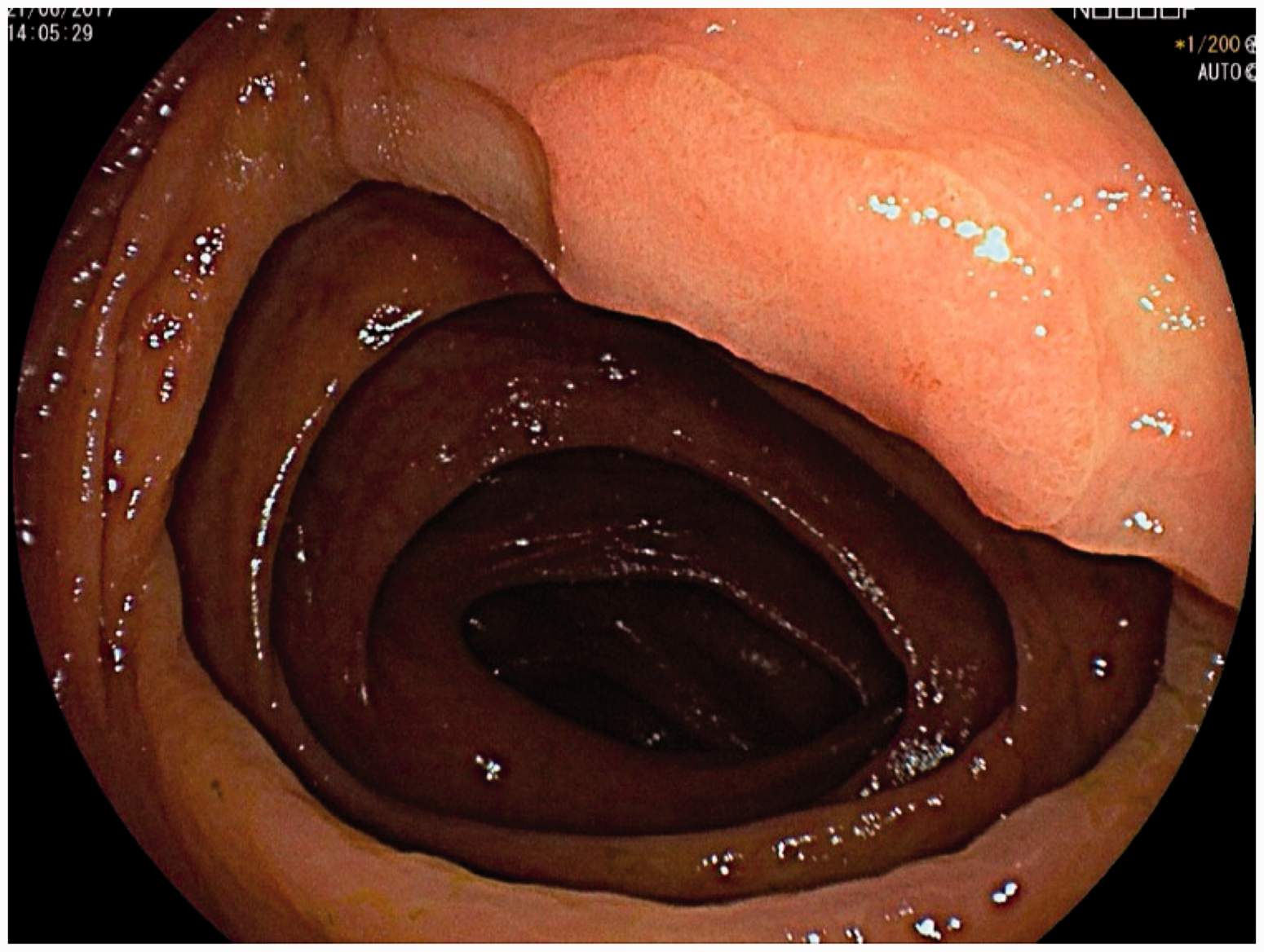
It has been suggested that the development of incident CRC in LS could in some cases follow a non-polypoid pathway where invasive growth occurs directly from seemingly normal mucosa 8 or via the serrated neoplasia pathway. 16 However, the role of adenomas in LS CRC is strongly supported as they are more frequently found in MMR gene mutation carriers, 17 and the efficiency of screening in LS is based on the removal of adenomas. 18 In our cohort, some pathology reports described adenomatous tissue at the cancer site, and incident CRCs were found at the site of previous polypectomies. As we cannot draw any hard conclusions from our data regarding the origin of CRC in our cohort, the role of non-polypoid pathways in LS CRC development needs to be further studied.
Besides morphological differences, colorectal neoplasms in LS patients might employ another method to escape detection. The adenoma-carcinoma sequence seems accelerated in LS. In our cohort, 65% of patients with incident CRC had no report of polyps during previous colonoscopy. Similarly, in another cohort, 58% of patients with incident CRC had no pathologic findings during previous surveillance colonoscopy. 19 Furthermore, shorter surveillance intervals do not lead to a reduced incidence of CRC. 3 Some adenomas are probably able to develop and undergo malignant change in the time period between two surveillance colonoscopies.
Another feature of LS CRC is its slow growth. In the 2017 study by Engel et al., no association was found between screening interval and tumor stage. 3 In our cohort, the tumors were generally small and most were T1/T2–N0, probably partly because of the short surveillance intervals. However, there was no association between surveillance interval and tumor size or tumor size and the presence of lymph node metastases.
The strength of this study was the analysis of prospectively collected data from a large database spanning almost three decades. However, the length of the data collection period was also one of the limitations. The quality of reporting in colonoscopy and pathology reports was inconsistent, as current quality considerations regarding colon preparation or visualization have not been implemented until recently.
This study has several implications for clinical practice. From the patient’s perspective, incident CRC can be regarded as a phenotype of LS. The 10-year cumulative risk of developing incident CRC is 9%–13% in LS patients. 3 This means that 45%–65% of LS patients will develop CRC during the surveillance period between 25 and 75 years. As mortality from incident CRC was only 2.8%, the risk of dying from CRC during the surveillance period is only 1.26%–1.82%. With improving quality of screening colonoscopies, these numbers can be expected to decline. Patients should be aware that adherence to screening programs is required, as patient-related delayed diagnosis of CRC was the cause of death in 80% of cases in a study on LS patients. 4
From the physician’s perspective, paying attention to the quality of the screening colonoscopies is essential. In case of an incomplete colonoscopy, a repeat examination should be scheduled. Quality parameters such as the Boston Bowel Preparation Scale, 20 recording of withdrawal time, confirming cecum intubation, and the Leiden Quality Score 21 may help to improve the success of screening colonoscopies. Furthermore, the frequently observed small and flat morphology of adenomas and CRC in LS patients pose an additional challenge to the colonoscopist.
Conclusion
The high rate of incident CRC in LS likely results from multiple factors. Our findings support the hypothesis of fast conversion of adenomas to cancer in LS, but to what extent non-polypoid pathways play a role needs to be studied further. The often non-polypoid appearance of colorectal lesions makes them more difficult to detect. Incomplete colonoscopies and the incomplete removal of adenomatous tissue during polypectomy contribute to development of incident CRC. In order to better understand tumor development in LS, a prospective analysis of adenoma and CRC morphology would be helpful.
Footnotes
Acknowledgments
The authors would like to thank Dr M. Bigirwamungu-Bargeman, Dr M.A.J.M. Jacobs, Dr S. Y. de Boer, Dr P. C. van de Meeberg, Dr S. Sanduleanu and Dr M. Verhulst for their help with including patients in the Dutch LS registry.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of conflicting interests
None declared.
Informed consent
All patients have given written permission for registration and anonymous evaluation of results.
Ethics approval
This study was approved by the research committee of The Netherlands Foundation for the Detection of Hereditary Tumors on July 1, 2017. The study protocol conforms to the ethical guidelines of the Declaration of Helsinki.