
Abstract
Background
Meckel’s diverticulum is present in about 2% of the population. The literature reports 3.2% incidence of tumors within Meckel’s diverticulum; the tumors are predominantly benign.
Objective and methods
The purpose of this study was to evaluate malignant tumors in Meckel’s diverticulum through systematic review of the literature and review of electronic medical records including pathology reports over 14 years at the Mayo Clinic, Rochester, USA.
Results
A literature review over the last 10 years identified 37 citations with 402 patients (median age: 58 years; 68.9% males). The predominant malignancy reported was neuroendocrine tumor 84.6%, followed by gastrointestinal stromal tumor 8.2%, and adenocarcinoma 6%. At the time of diagnosis, 29.5% of patients had metastases. In the Mayo Clinic electronic medical records review, there were 19 patients (5.1% of them surgically removed Meckel’s diverticulum) who had a malignancy associated with Meckel’s diverticulum: 63.2% neuroendocrine tumor, 10.5% gastrointestinal stromal tumor, 5.3% adenocarcinoma, 5.3% pancreatic epithelial neoplasia, and 15.8% metastases from secondary location. Median size of the malignancy was 7 mm, and 17/19 malignancies were coincidental findings. Most neuroendocrine tumors infiltrated the submucosa, while gastrointestinal stromal tumor and adenocarcinoma invaded the serosa. At the time of diagnosis, 33.3% of patients had metastases.
Conclusion
About 5% of Meckel’s diverticulums resected were associated with malignant tumors, most commonly neuroendocrine tumor, and a significant portion of Meckel’s diverticulum malignancy was metastatic at the time of discovery.
Introduction
Meckel’s diverticulum (MD) is a true diverticulum of the small bowel, typically found within 100 cm proximal to the ileocecal valve. It results from incomplete obliteration of the omphalomesenteric duct. MD affects ∼2% of the population. 1 Of all patients with a MD, it is estimated that ∼4% will present with induced symptoms or develop a complication. Common manifestations of symptomatic MD include: intestinal obstruction (36.5%), intussusception (13.7%), inflammation (12.7%), and hemorrhage (11.8%). 1 Symptomatic patients are mostly men with average age (±standard deviation (SD)) of 31 ± 23.6 years. Based on a study of 227 patients with MD, the average length of MD was 2.99 cm, with a range of 1–11 cm.2
Approximately 3.2%1 of patients with a symptomatic MD have a tumor in the MD, with most being benign. 3 The majority of malignant MDs are diagnosed either during surgery or reported pathologically after removal of a symptomatic MD. The literature regarding malignant MD is comprised of case reports and case series. The predominant types of malignancies are neuroendocrine tumors (NETs), gastrointestinal stromal tumors (GISTs), adenocarcinomas, metastases, and lymphomas in that order of prevalence.1,4,5
Treatment of symptomatic MDs is by surgical removal. However, treatment of asymptomatic MDs has been extensively debated.1,6 The aim of our study was to evaluate malignant tumors in MD through systematic review of the literature and a review of electronic medical records (EMRs) over 14 years at Mayo Clinic.
Methods
Systematic literature review
Design
We conducted a systematic review of the literature concerning malignancies in MD. A database search was performed in August 2017 using Ovid MEDLINE (2007 to present) and included epublication ahead of print, in-process, and other non-indexed citations, and Embase (2007–2017). An expert librarian conducted the electronic literature search with input from the investigator (Figure 1). Search terms used were: “Meckel’s diverticulum,” “malignan*,” and “metastas*.” We limited our search to literature published in the last 10 years to coincide with the period of the medical records review conducted as part of the same study. Articles not available in English or Dutch were excluded. Additional articles were included after reviewing literature references and discussion with a content expert (MC). Studies were excluded if there was no malignancy within the MD reported.
Systematic 10-year literature review of Meckel’s diverticulum (MD) and malignancy.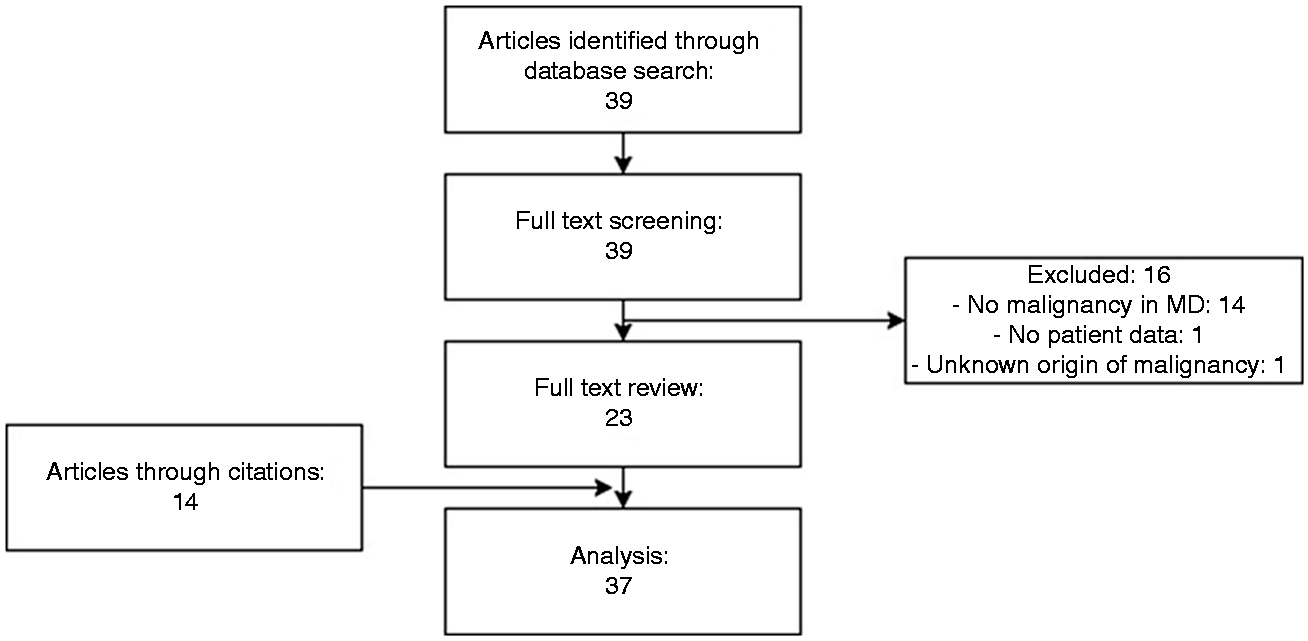
Data extraction
Systematic literature review.
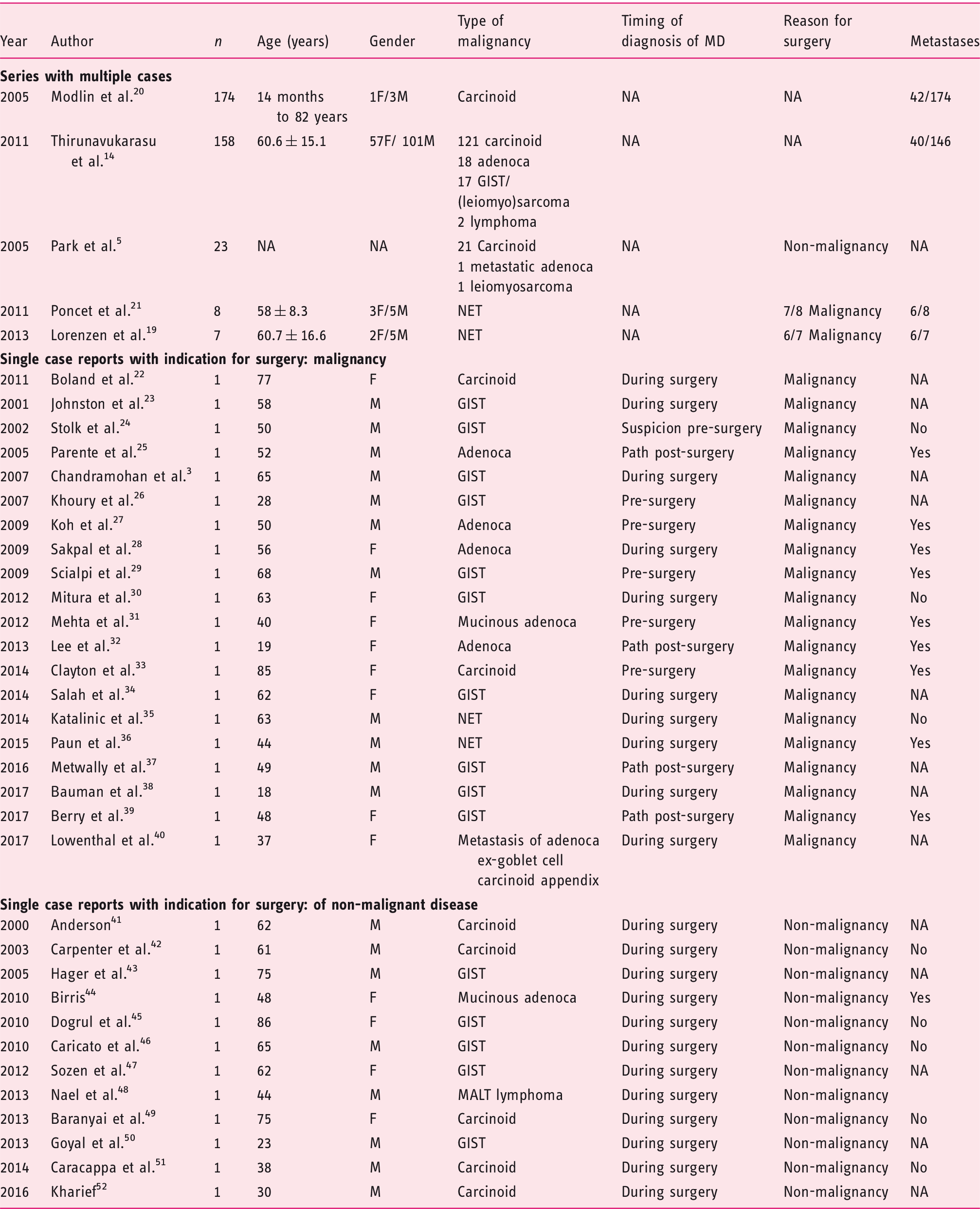
F: female; GIST: gastrointestinal stromal tumor; M: male; MD: Meckel’s diverticulum; NET: neuroendocrine tumor; SD: standard deviation.
Data show mean ± SD.
When absent in the multi-patient studies in the published literature, absolute numbers were estimated based on reported ratios and analysis in the papers.
Retrospective electronic medical records review
Design
We conducted a retrospective review of all available electronic medical records of patients with MD with proven malignancy based on pathology reports at Mayo Clinic, Rochester, from 1 January 2003–1 August 2017. We started our medical records search in 2003 because a previous publication had described MD evaluated at Mayo Clinic, Rochester, from 1950–2002. 5
This study was approved by the Mayo Clinic Institutional Review Board on 4 August 2017 (IRB# 17-006614). The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki. Patients included in the study provided written research authorization.
Records identification and analysis
Data were collected via the Advanced Cohort Explorer (ACE) application available at Mayo Clinic. ACE is a clinical data repository maintained by the Unified Data Platform. We documented symptoms, age at presentation, gender, indication for surgery, surgical and pathology reports, and outcomes.
We estimated median and interquartile ranges (IQRs) of age, length of the MD, size of the malignancy, and depth of infiltration.
Results
Literature review
Search results
As demonstrated in Figure 1, 39 citations were identified via the literature search. After a complete study review, 16 articles were excluded since there were no reports of malignancy found within the MD or because of a lack of data regarding the origin of the MD malignancy. After reviewing references and consulting with our content expert (MC), 14 additional articles were found suitable for analysis. In total, 37 articles were included: four case series, one review, and 32 case reports.
Demographics
In the 37 articles, a total of 402 patients were evaluated. A male predominance was noted, with 261 males compared to 118 females. One case series, including 23 patients, did not provide information regarding gender. Median age was 58 years (IQR 44.5–65 years). This was calculated from data available from 47 patients identified in 34 of the 37 articles. One case series (including 23 patients) did not provide individual patient ages; the second case series reported a mean age of 60.6 ± 15.1 (SD) years, and the review documented an age range from 14 months to 82 years.
Diagnosis of Meckel’s diverticulum in association with malignancy
Thirty-two single-case reports described MD time of discovery in cases where malignancy was found. Six cases were diagnosed before surgery based on symptoms and imaging. Of the remaining 26 patients, 22 MDs were diagnosed coincidentally during surgery, and the remaining four underwent a segmental intestinal resection (e.g. for obstruction) and MD was identified in the resected specimen by pathological examination.
Thirty-five articles, involving 70 patients, reported the original indication for abdominal surgery. In 33/70 cases, the primary indication for surgery was treatment of a known or presumed malignancy, including six case reports where MD was diagnosed before surgery. In the remaining 37/70 cases, primary indication for surgery was unrelated to malignancy. No additional details were available regarding the sizes of the malignant lesions.
Malignancy in Meckel’s diverticulum
There were a total of 402 malignancies within the MD in the 37 citations. The majority of malignancies were NETs (340/402). Most of these NETs (331/340) were recorded in three of the five case series. Following NET, other tumor types were GISTs (33/402), adenocarcinomas (24/402), lymphomas (3/402), and metastasis of an adenocarcinoma (2/402).
Abdominal metastases from the primary malignancy originating within the MD were demonstrated in 104 patients. One case series reported 40 cases with metastatic disease associated with and possibly originating from the MD, but did not document the type of tumor. Among the remaining 64 cases, 56 patients had metastatic NETs, six metastatic adenocarcinomas, and two metastatic GISTs originating from the MD.
Electronic medical record review
Between 1 January 2003–1 August 2017, 629 patients were diagnosed with a MD at Mayo Clinic, Rochester, of which 373 had the MD surgically removed. Review of pathology reports showed that 5.1% (19/373) of these patients had evidence of malignancy. The remainder of this report focuses on the 19 patients with a malignancy within the MD.
The median age of the 19 patients was 57 years (IQR, 50–68 years), with 14 male and five female patients.
Diagnosis of Meckel’s diverticulum in association with malignancy
As shown in Figure 2, 3/19 patients underwent MD removal at the time of surgery, with coincidental identification of NET or GIST on pathological examination; 14/19 cases underwent surgery for an indication of preoperatively diagnosed malignancy in the abdomen with additional finding of a malignancy in the MD. In addition, 2/19 patients had preoperative diagnosis of malignancy in the distal ileum without precise location, later identified as MD: one NET and one pancreatic intraepithelial neoplasia in the MD.
Mayo Clinic patient data of Meckel’s diverticulum (MD) and malignancy. GIST: gastrointestinal stromal tumor; NET: neuroendocrine tumor.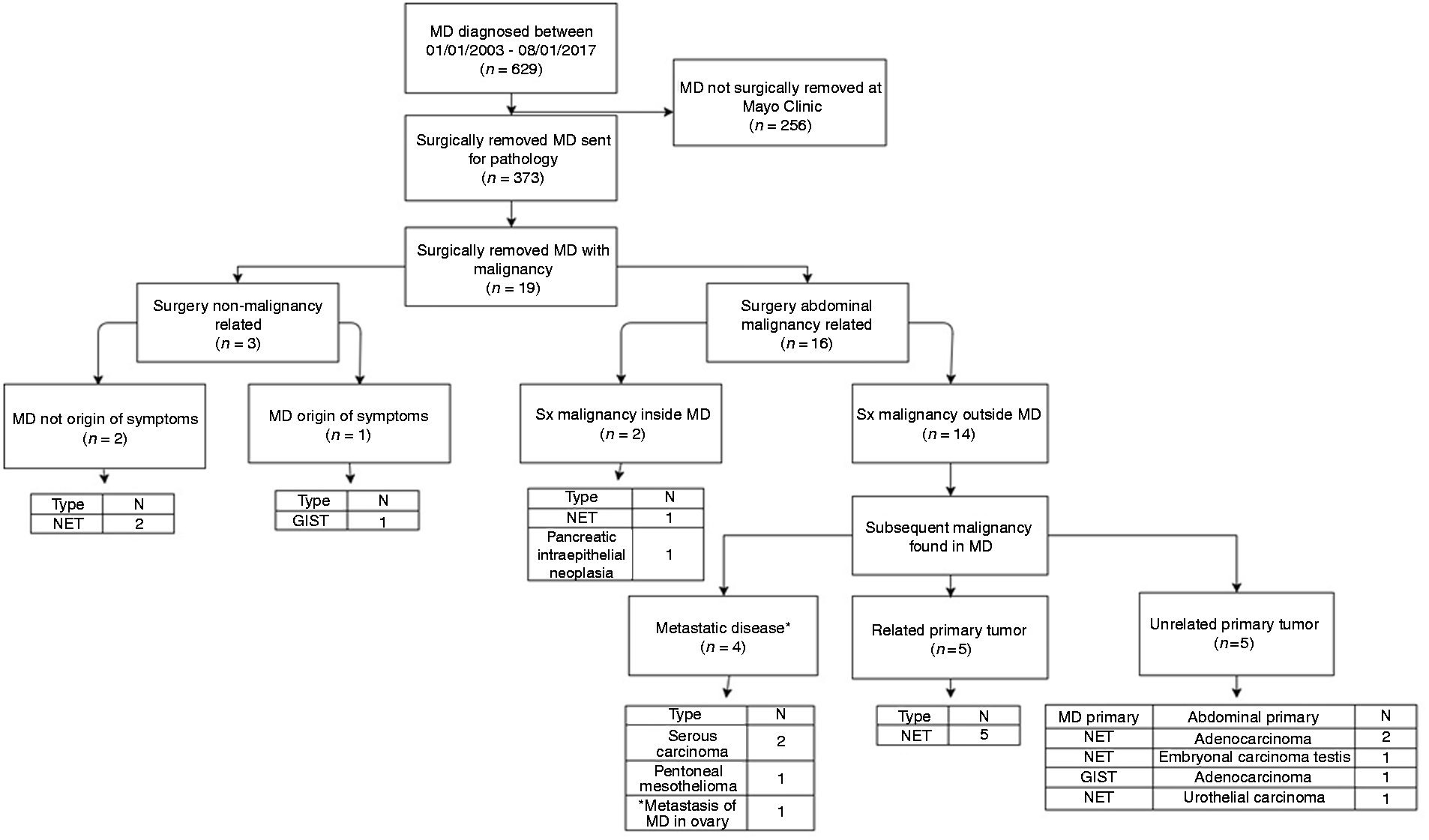
Among the 14 patients with malignancy outside the MD, a separate malignancy was identified in the MD: three were metastatic to the MD, and one was MD primary metastatic to the ovary. Five were NET in the MD, which were associated with NET at another site. Five other patients had NET or GIST in the MD and had a primary tumor of a different histological type elsewhere in the abdomen. In the remaining 3/19 cases, the abdominal surgery was conducted for a nonmalignant indication, and tumor within the MD was found coincidentally (two NET and one GIST).
Mayo Clinic patient data review; there were 19 patients with malignancy associated with Meckel’s diverticulum (MD) (2003–2017).
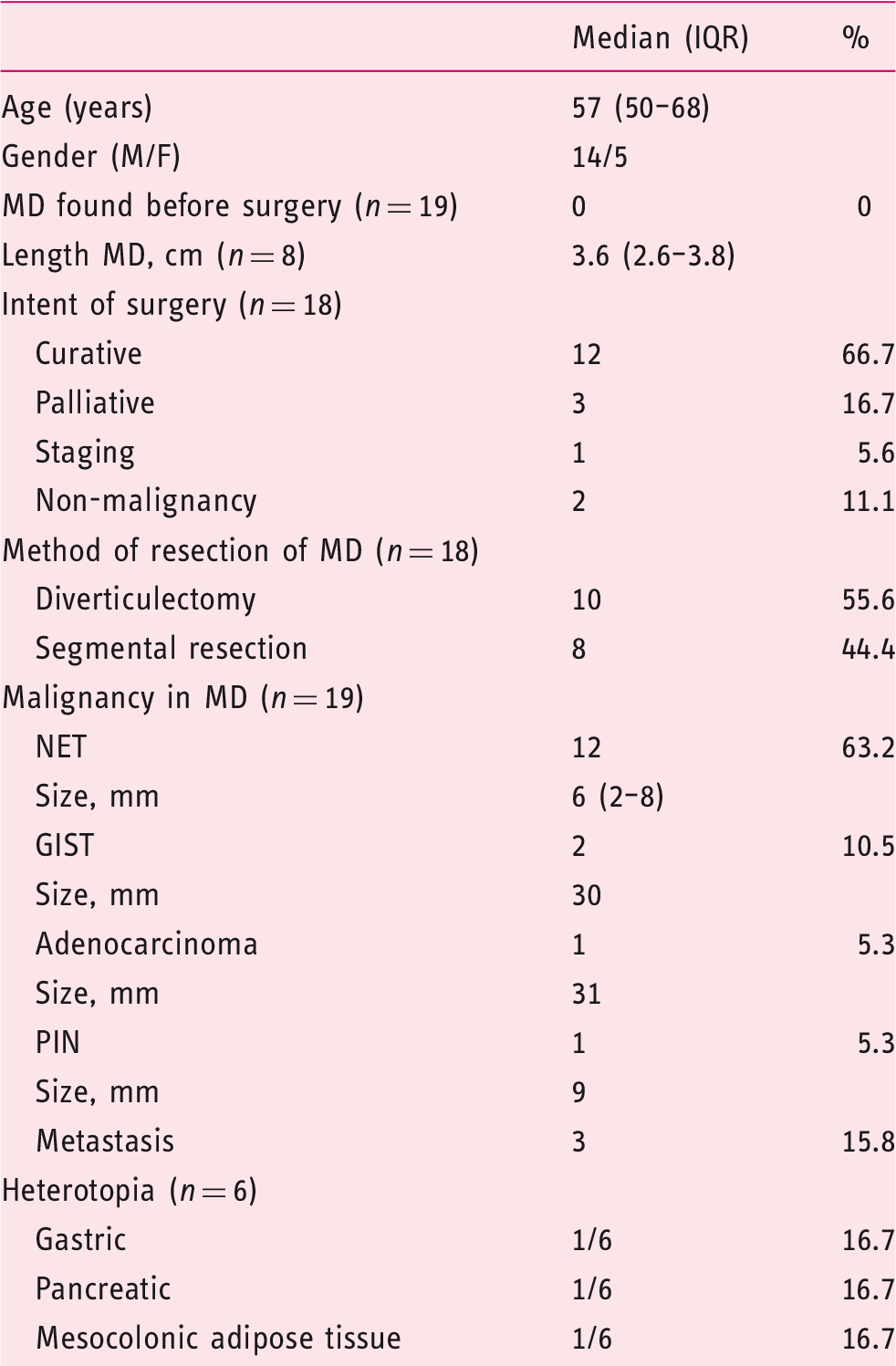
GIST: gastrointestinal stromal tumor; IQR: interquartile range; NET: neuroendocrine tumor; PIN: pancreatic epithelial neoplasia.
The median length of the MD was 3.6 cm (IQR 2.6–3.8 cm). In three cases, heterotopia was present (gastric, pancreatic, and adipose tissue). In three other patients, there was specific exclusion of heterotopia on histological examination.
Malignancy in Meckel’s diverticulum
Primary malignancies in MD
Sixteen cases had primary malignancies in the MD; in order of prevalence: NET (12/19), GIST (2/19), adenocarcinoma (1/19), and pancreatic epithelial neoplasia (PIN) (1/19).
We had data about metastases of the MD in 15 cases; 5/15 had metastases, four from a NET with metastases to lymph nodes (n = 4), liver (n = 1), and ovary (n = 1), which were all completely resected.
Secondary malignancies in MD
Three patients had evidence of metastasis in the MD; two serous carcinoma (one originating in the uterus and one in the ovary), and one peritoneal mesothelioma.
Depth of tumor invasion
Most NETs infiltrated the submucosa. The adenocarcinoma, GISTs, and metastases infiltrated deeper into the subserosa or even the serosa.
Discussion
Complications from MD are rare events, and malignancy associated with MD is even rarer. Thus, we found that, after surgical removal of the MD, 5.1% (19/373) of patients had a MD-associated malignancy. This is slightly higher than the incidence described in the literature of 3.2%. 1 When comparing our patient database to the literature, we found similar demographic characteristics, with a male predominance, 74%, and a median age of 57 years. Similarly, the predominant types of malignancies found in the MD were NETs as the most frequent malignancy, followed by GISTs, and adenocarcinoma. The combination of these similarities, and the fact that most malignancies were found coincidentally, argue against the presence of a tertiary referral bias in our single, tertiary center database.
Management of symptomatic MD is by surgical removal. There is ongoing debate on how best to manage asymptomatic MD. One study, reported in 1976, evaluated 202 patients and concluded that prophylactic removal of MD is not warranted with a number needed to treat of 800 patients. 6 Yahchouchy et al. performed a literature review documenting that the benefits of prophylactic removal of asymptomatic MD outweigh morbidity and mortality associated with surgery. 1 This opinion is supported by improved surgical techniques with decrease in postoperative morbidity and mortality, and postoperative complications associated with the prophylactic removal of the MD are rare. 7 In practice, the decision to resect MDs is currently based on the individual MD and patient characteristics, as well as surgeon preference. Given the estimated prevalence of MD of 0.15–6% in the general population, based on surgical or autopsy studies,8–12 the mere finding of a MD may not necessitate its removal. However, based on the medical experience of Olmsted County, Minnesota residents for the period 1950–1992, Cullen et al. reported that MD had a lifetime risk of complications of 6.4%, and that diverticulectomies for complications of MD carried an operative mortality and morbidity of 2% and 12% respectively, and a cumulative risk of long-term postoperative complications of 7%; whereas, incidental diverticulectomies done in 87 residents during the period carried corresponding rates of only 1%, 2%, and 2%, respectively. This led to the recommendation that MD discovered incidentally at operation should be removed for most patients, regardless of age. 7 On the other hand, other data estimated a lifetime risk of complications of 4.2%, and a number needed to avoid one death of 800 among asymptomatic MDs undergoing diverticulectomy. 6 The most recent analysis of the literature suggests that resection for incidental MD should be restricted to those identified as being at higher risk of complications: male gender, age younger than 40, diverticulum longer than 2 cm, and the presence of macroscopic mucosal alteration noted at surgery. 13
Thirunavukarasu et al. performed a large review of the Surveillance, Epidemiology, and End Results (SEER) database to examine malignancy in MD and compare it to other ileal malignancies. 14 They included 158 patients in their analysis and found 121/158 NETs, similar to the ratio calculated from our patient database. Their Kaplan-Meier curves for overall survival demonstrated NETs had the best prognosis, followed by GISTs and adenocarcinomas. This is in agreement with the high rates of metastatic adenocarcinomas described in the case reports reviewed and with the adenocarcinoma identified in a Mayo Clinic patient, which was larger (31 mm) than the other malignancies in MD and had already metastasized.
The lining of MD often contains ectopic tissue, and the mechanism responsible is still not fully understood. Currently, the most widely accepted hypothesis is that pluripotent cells, once lining the omphalomesenteric duct, are the source for development of ectopic tissue. 15 However, this hypothesis fails to explain why some ectopic tissues, such as pancreatic and gastric epithelium, are more frequent than others, and it also does not explain the factors influencing differentiation. 15 Further research is needed to clarify these mechanisms leading to the development of ectopic tissue in MD. The presence of ectopic tissue is associated with a higher rate of complications. 15 With the small numbers of MDs containing ectopic tissue, we are unable to comment on the relative prevalence of complications in the presence of ectopic tissue.
NETs are considered rare, slow growing, and, often, indolent tumors. However, in past years, the overall incidence of NETs has been increasing steadily, which is consistent with the high proportion of NETs detected in our database and in the published literature. 16 It is possible that this documented increase in incidence might be secondary to increased detection.17,18 The median size of the NETs found in our patient database was 6 mm, with most of the NETs not penetrating past the submucosa and being found coincidentally. Despite these benign features, 4/5 cases in our patient database review and 56/104 cases from the literature review had abdominal metastases from a NET arising in a MD. This is also consistent with the previous literature which documented that metastases are often noted among MD NETs, despite the small sizes of the tumors. 19 Patients with a concurrent second primary NET in the bowel experience more aggressive tumor behavior; 16 in fact, all of our patients with a metastases from NETs had a second primary NET unrelated to the MD.
Limitations in this study include a possible referral bias because Mayo Clinic is a tertiary care center which could potentially impact the number of malignancies, the lack of follow-up for the 256 patients who did not undergo surgery for MD, and the retrospective nature of this study. Although our patient population was small, we believe it provides an accurate estimate of the prevalence and the type of malignancy compared to the published literature. In the literature review, three out of five studies involving multiple patients rather than single-case reports only appraised NETs; therefore, those data may possibly be skewed. Additionally, 32/37 studies included in the literature review were case reports. Lastly, there is likely to be publication bias given the propensity for only the interesting cases of MD to be reported, particularly in case series or reports.
In conclusion, the literature review and our patient database found similar percentages (∼3–5.1%) of malignancies within the MD. The rate of metastases was ∼33% in our patient database and ∼26% in the literature review. Thus, we believe that prophylactic removal of asymptomatic MD discovered during surgery is warranted. There is insufficient data on the MD complication rate to justify primary prophylactic removal of the MD without another indication for abdominal surgery.
Key points
Summarize the established knowledge on this subject.
Meckel’s diverticulum (MD) is present in about 2% of the population. The literature reports 3.2% incidence of tumors within MD; the tumors are predominantly benign. What are the significant and/or new findings of this study?
From the literature review of 402 patients over the last 10 years, the predominant types of malignancies reported were neuroendocrine tumor (NET) 84.6%, gastrointestinal stromal tumor (GIST) 8.2%, and adenocarcinoma 6%. At the time of diagnosis, 29.5% of patients had metastases. In the review of Mayo Clinic patient records, there were 19 patients (5.1% of the surgically removed MD) with a malignancy associated with MD: 63.2% NET, 10.5% GIST, and 5.3% adenocarcinoma. Median size of the malignancy was 7 mm. In the Mayo Clinic patients, 17/19 malignancies were coincidental findings and, at the time of diagnosis, 33.3% had metastases. These data suggest that prophylactic removal of asymptomatic MD discovered during surgery is warranted.
Footnotes
Acknowledgements
The authors thank Danielle Gerberi, librarian, for the literature search and Cindy Stanislav for excellent secretarial assistance. The author contributions were as follows: Kathleen Van Malderen – data collection and synthesis, authorship of manuscript; Priya Vijayvargiya – research fellow, data synthesis, authorship of manuscript; Michael Camilleri – principal investigator, study concept and design, analysis and interpretation of data, drafting and revising manuscript, study supervisor; David W Larson and Robert Cima – co-investigators, interpretation of data, and co-authorship of manuscript.
Declaration of conflicting interests
The authors have no conflicts of interest.
Ethics approval
The study was approved by the Mayo Clinic Institutional Review Board on 4 August 2017 (IRB Number 17-006614).
Funding
None
Informed consent
Patients included in the study provided written research authorization.