
Abstract
Background
Few observational studies have assessed the role of physical activity in oesophago-gastric cancer risk.
Objective
This prospective cohort study aimed to assess the association between physical activity and risk of oesophageal or gastric cancer.
Methods
A cohort of 359,033 adults aged 40–69 years were identified from the UK Biobank, which recruited participants between 2006 and 2010. Adjusted hazard ratios (HRs) and 95% confidence intervals (CIs) for the associations between self-reported levels of physical activity and screen-based sedentary behaviour and risk of oesophageal and gastric cancer were calculated using Cox proportional hazards models.
Results
During eight years of follow-up (mean = 5.5), 294 oesophageal cancer and 217 gastric cancer cases were identified. Physical activity and screen-based sedentary behaviour levels were not associated with overall oesophago-gastric cancer risk. However, when compared with low levels, high physical activity levels were associated with a significantly reduced risk of gastric non-cardia cancer (HR 0.58, 95% CI 0.37–0.95). Moderate physical activity levels were associated with a 38% reduced risk of oesophageal adenocarcinoma (HR 0.62, 95% CI 0.43–0.89), although no dose-response association was apparent.
Conclusion
Moderate, rather than high, physical activity levels were associated with the strongest reductions in oesophageal adenocarcinoma risk in this large UK prospective cohort.
Key summary
1. Summarise the established knowledge on this subject.
Previous systematic reviews indicate an association between physical activity and risk of oesophageal and gastric cancers. However, there is a paucity of evidence from large-scale prospective studies for individual cancer subtypes. 2. What are the significant and/or new findings of this study?
Prospective data indicated that high physical activity levels were associated with a reduced risk of gastric non-cardia cancers, though this association was attenuated after removing potentially prevalent cancers. Moderate but not high levels of physical activity were associated with a reduced risk of oesophageal adenocarcinoma.
Introduction
Oesophageal and stomach cancer patients often have a poor prognosis 1 because of late diagnosis. The reduction of burden from these cancers may be better achieved through implementation of appropriate primary prevention programmes.
Physical activity is a modifiable factor suggested for primary prevention of other cancer sites. 2 However, evidence suggesting a protective role for physical activity in upper gastrointestinal (GI) cancer aetiology is more limited. 3
Previous systematic reviews noted reduced risks of oesophageal4,5 and gastric cancer4,6 in the most physically active individuals compared to the least active individuals. Singh et al. 6 also reported a significant 32% reduced risk for oesophageal adenocarcinoma (OAC) specifically (odds ratio (OR) 0.68, 95% confidence interval (CI) 0.55–0.85) when comparing the most to the least physically active individuals. However, results for oesophageal squamous cell carcinoma (SCC) were less conclusive.7,8 Furthermore, there was considerable heterogeneity observed in meta-analyses by histological subtype, which also relied heavily on case-control study evidence that is prone to recall bias.
Sedentary behaviour, defined as waking activity with low energy expenditure (≤1.5 metabolic equivalents (METS)) and a sitting or reclining posture, has also been associated with an increased risk of a number of cancers in a limited number of studies to date. 9 However, there is a notable paucity of data in relation to upper GI cancer risk.
Additional studies assessing the association between physical activity, sedentary behaviour, and oesophageal and gastric cancer, according to anatomical and histological subsite are warranted. Therefore, we aimed to explore the association between physical activity, sedentary behaviour, and oesophago-gastric cancer risk within a large United Kingdom (UK) prospective cohort.
Methods
Study population
A cohort of 502,640 individuals was identified from the UK Biobank. Individuals aged 40–69 years were invited to participate between 2006 and 2010 if they were registered with the National Health Service and typically lived within a 25-mile radius of one of the 22 study assessment centres. 10 In total, around 9.2 million invitations were mailed to potential participants, from whom there was a 5.5% response rate. The UK Biobank conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a prior approval by the North West Multi-Centre Research Ethics Committee (10 May 2016). All participants provided written informed consent.
For the purposes of our analysis, participants who were diagnosed with malignant cancer (excluding non-melanoma skin cancer) on or before baseline were excluded (n = 26,875). Participants who did not have complete information for physical activity as defined by the standard International Physical Activity Questionnaire (IPAQ) guidelines 11 (n = 110,592) or important baseline characteristics (education, Townsend deprivation, 12 smoking status, alcohol consumption, height, body mass index (BMI) and waist:hip ratio, total n = 6140) were also excluded. This resulted in a total of 359,033 individuals being retained for inclusion in our analysis (Supplementary Figure 1).
Physical activity and sedentary behaviour assessment
Physical activity assessment within the UK Biobank was measured using the validated IPAQ short form. 13 Participants self-reported the frequency (days per week), intensity and duration (minutes per day) of walking, moderate and vigorous activity on a typical day/week over the past four weeks. These measures were all added to create a composite physical activity score, 11 weighted as the summation of the duration (in minutes) and frequency (in days) of walking, moderate-intensity and vigorous-intensity activity. Time spent in vigorous, moderate and walking activity was weighted by the energy expended for these categories of activity, to produce MET minutes per week of physical activity. One MET is considered a resting metabolic rate obtained during quiet sitting. 14 Met-minutes were computed by multiplying the MET score for each type of physical activity by the minutes performed. MET scores for each type of physical activity are as follows: minutes of walking (×3.3), moderate exercise (×4.0) and vigorous exercise (×8.0). Data processing rules published by IPAQ were followed. 11
Individuals meeting one of the following criteria were assigned to the high physical activity group:
Vigorous-intensity activity on at least three days achieving a minimum total physical activity of at least 1500 MET-minutes per week Seven or more days of any combination of walking, moderate-intensity or vigorous-intensity activities achieving a minimum total physical activity of at least 3000 MET-minutes per week.
Remaining individuals meeting one of the following criteria were assigned to the medium physical activity group:
Three or more days of vigorous-intensity activity of at least 20 minutes per day Five or more days of moderate-intensity activity and/or walking of at least 30 minutes per day Five or more days of any combination of walking, moderate-intensity or vigorous intensity activities achieving a minimum total physical activity of at least 600 MET-minutes per week.
Remaining individuals who did not meet criteria for medium or high physical activity groups were assigned to the low physical activity group.
Screen-based sedentary behaviour was based on self-reported hours spent using a computer or watching television. In the baseline questionnaire, participants reported how many hours they spent watching television and using a computer (excluding at work) in a typical day. Participants reported the average time for a 24-hour day in the previous four weeks if this varied. The two variables were summed (1) and total hours per day of screen-based sedentary behaviour was divided into three categories for analysis: low (0–3 hours), moderate (>3–4) and high (>4). 14
Anthropometric assessment
Height and weight were measured by UK Biobank study centre staff. BMI was then calculated as weight (kg) divided by height (m) squared. Study centre staff also measured hip and waist circumference respectively to allow calculation of waist:hip ratios. Waist circumference measurements were taken from the level of the umbilicus.
Assessment of other covariates
Age, sex, ethnicity, smoking status, alcohol intake and medical history were derived from touchscreen questionnaires. Townsend scores, a measure of area-based socioeconomic deprivation, 12 were derived from postcode of usual residence.
Definition of cancer outcomes
Incident cancer cases within the UK Biobank cohort were identified through linkage to national cancer registries (Health & Social Care Information Centre and the NHS Central Register). Participants were followed up until upper GI cancer diagnosis, death, emigration or end of follow-up (30 September 2014). The histology for neoplasms is presented in the data showcase for UK Biobank and is coded according to the International Classification of Diseases for Oncology, 3rd edition. Oesophageal and gastric cancers were defined as C15 and C16, respectively. 15
Statistical analysis
Proportions for categorical variables and means for continuous variables were compared for baseline characteristics between individuals by their category of physical activity (low, moderate and high).
Cox proportional hazards models were used to estimate the hazard ratios (HRs) and corresponding 95% confidence intervals (CIs) for the associations between categories of physical activity, screen-based sedentary time (hours per day), and risk of oesophago-gastric cancer. Analyses were adjusted for age (as the underlying timescale variable), sex, Townsend deprivation index quintiles, educational attainment (university degree or not), height (metres), smoking status (by pack-years; never, former < 20 pack-years, former 20+ pack-years, current < 20 pack-years and current ≥ 20 pack-years), and alcohol intake (never drinker, former drinker, current light to moderate/occasional drinker (<14 units per week), current heavy drinker (≥14 units per week)). Further analyses additionally adjusted for BMI and waist:hip ratio at baseline as restricted cubic splines, without including height. Screen-based sedentary behaviour analyses were additionally adjusted for total MET hours of physical activity. Tests for trend were assessed by including physical activity categories as a continuous variable in survival analyses.
Subgroup analyses were conducted by histological (adenocarcinoma and SCC) and topographical subtype (gastric cardia and non-cardia), sex, smoking status, BMI and comorbidity status at baseline, with interactions assessed using likelihood ratio tests. Additional sensitivity analyses were conducted by type and intensity of physical activity (walking, other moderate physical activity and vigorous physical activity) and separately, restricting analysis to cancers diagnosed at least three years after baseline to evaluate the impact of prevalent disease. Post-hoc analyses also assessed physical activity categorised according to MET-minutes per week (<600, 600– < 1500, 1500 + MET-minutes per week).
Analyses were conducted using Stata/IC (version 14.1, TX, USA).
Results
During eight years of follow-up (mean = 5.5 years, standard deviation, SD = 1.1 years), 294 oesophageal cancer and 217 gastric cancer cases were identified. Mean age at baseline was 56.5 years (SD = 8.1 years) and mean age at diagnosis was 64.8 years (SD = 6.3 years).
Characteristics by physical activity category amongst 359,033 UK Biobank participants.
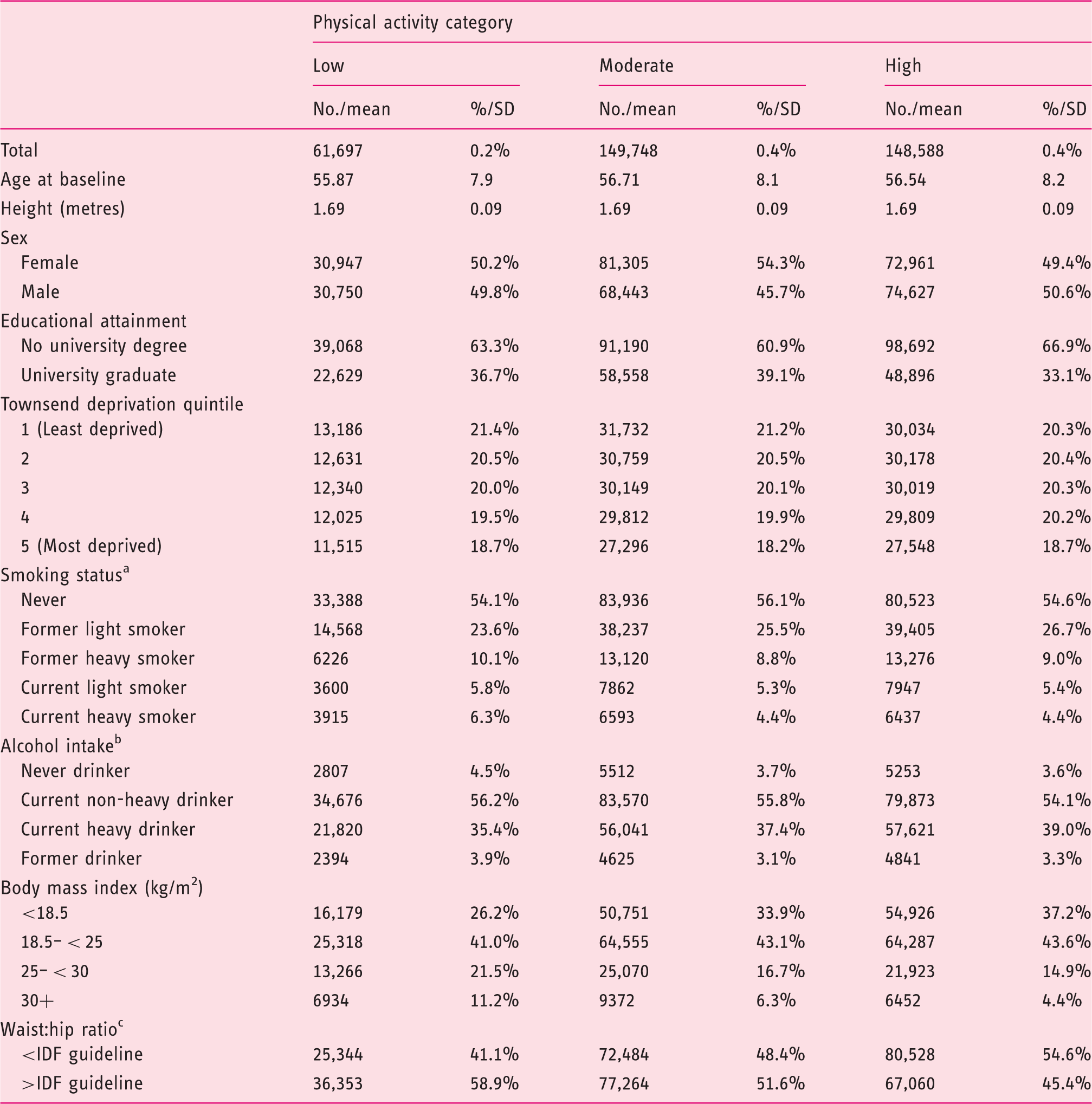
IDF: International Diabetes Federation; UK: United Kingdom.
By pack-years (light ≤ 20 pack-years; heavy ≥ 20 pack-years).
Light to moderate (special occasions, one to three times per month, < 14 units/week). Heavy (>14 units/week)
Based on IDF criteria (>94 cm in men; > 80 cm in women).
Cox proportional hazards results for the association between measures of physical activity and types of oesophago-gastric cancers amongst 359,033 participants of the UK Biobank study.
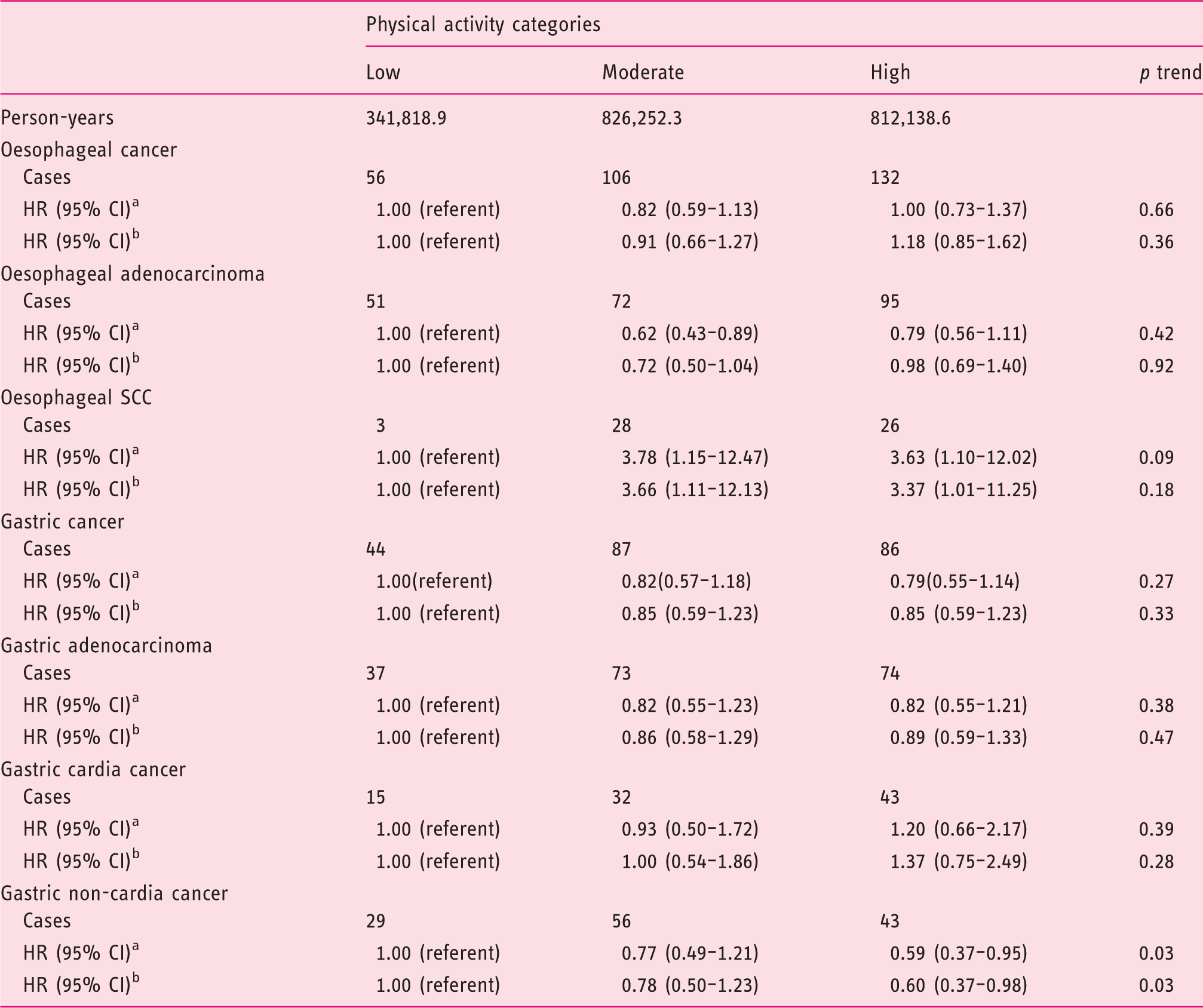
CI: confidence interval; HR: hazard ratio; SCC: squamous cell carcinoma; UK: United Kingdom.
Adjusted for sex, educational attainment (degree vs not), Townsend deprivation index (quintiles), smoking status (never, former light, former heavy, current light, current heavy), height at baseline (metres), alcohol intake (never drinker, former drinker, current light to moderate drinker, current heavy drinker) and baseline date. Age was used as the timescale.
Additionally adjusted for body mass index (<18.5, 18.5–<25 (ref), 25–<30, 30+) and waist:hip ratio (>94 vs ≤ 94 in men; > 80 vs ≤ 80 in women).
Moderate physical activity levels were also associated with a reduced risk of OAC (HR 0.62, 95% CI 0.43–0.89), although there was no evidence of a dose-response association as the association was not statistically significant for high physical activity levels (p for trend = 0.42). Conversely, moderate and high physical activity was associated with an increased risk of oesophageal SCC (HRmoderate 3.78, 95% CI 1.15–12.47; HRhigh 3.63, 95% CI 1.10–12.02) when compared with low levels. After additionally adjusting for BMI and waist:hip ratio, most results remained unchanged, though the reduced risk of OAC associated with moderate physical activity levels was no longer statistically significant (HR 0.72, 95% CI 0.50–1.04) (Table 2).
Cox proportional hazards results for the association between measures of physical activity and types of oesophago-gastric cancers amongst 359,033 participants of the UK Biobank study after excluding events within the first three years of follow-up.
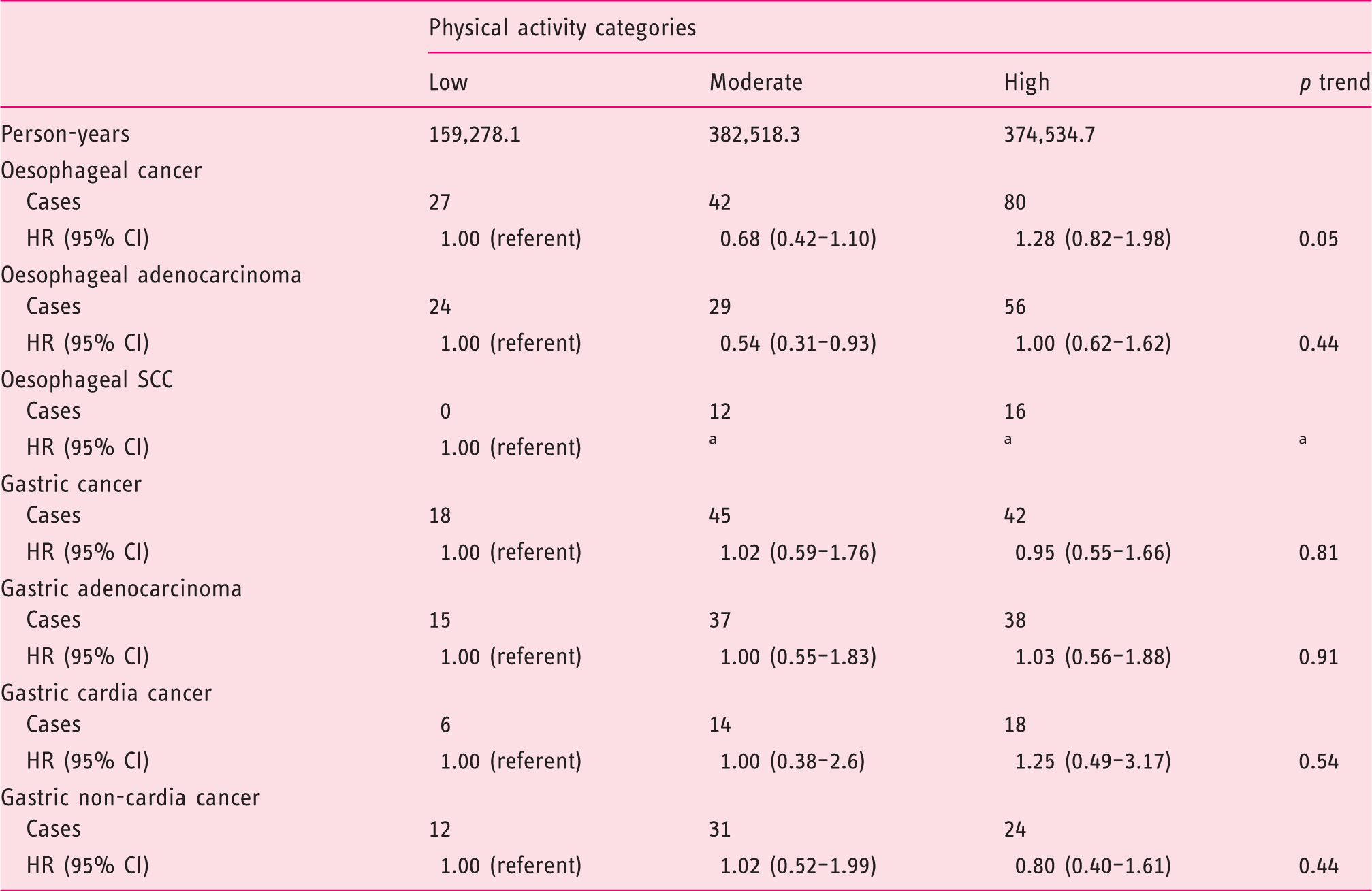
CI: confidence interval; HR: hazard ratio; SCC: squamous cell carcinoma; UK: United Kingdom.
Adjusted for sex, educational attainment (degree vs not), Townsend deprivation index (quintiles), smoking status (never, former light, former heavy, current light, current heavy), height at baseline (metres), alcohol intake (never drinker, former drinker, current light to moderate drinker, current heavy drinker) and baseline date. Age was used as the timescale.
Unable to calculate estimate because of small numbers.
Cox proportional hazards results for the association between types/intensities of physical activity and types of oesophago-gastric cancers amongst 359,033 participants of the UK Biobank study.
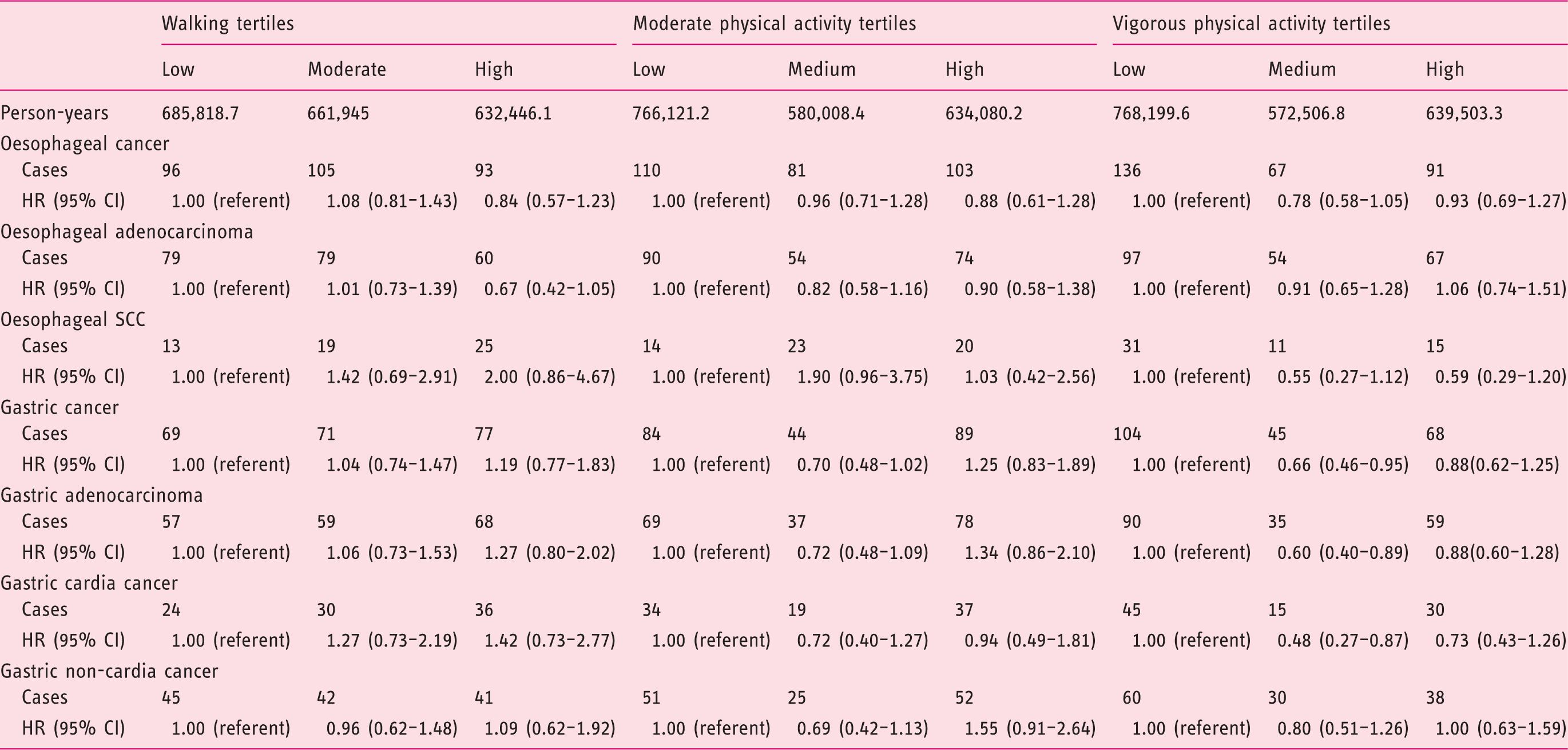
CI: confidence interval; HR: hazard ratio; SCC: squamous cell carcinoma; UK: United Kingdom.
All analyses adjusted for sex, educational attainment (degree vs not), Townsend deprivation index (quintiles), smoking status (never, former light, former heavy, current light, current heavy), height at baseline (metres), alcohol intake (never drinker, former drinker, current light to moderate drinker, current heavy drinker), baseline date and total minutes of physical activity per week. Age was used as the timescale.
Cox proportional hazards results for the association between tertiles of screen-based sedentary behaviour and types of oesophago-gastric cancers amongst 359,033 participants of the UK Biobank study.
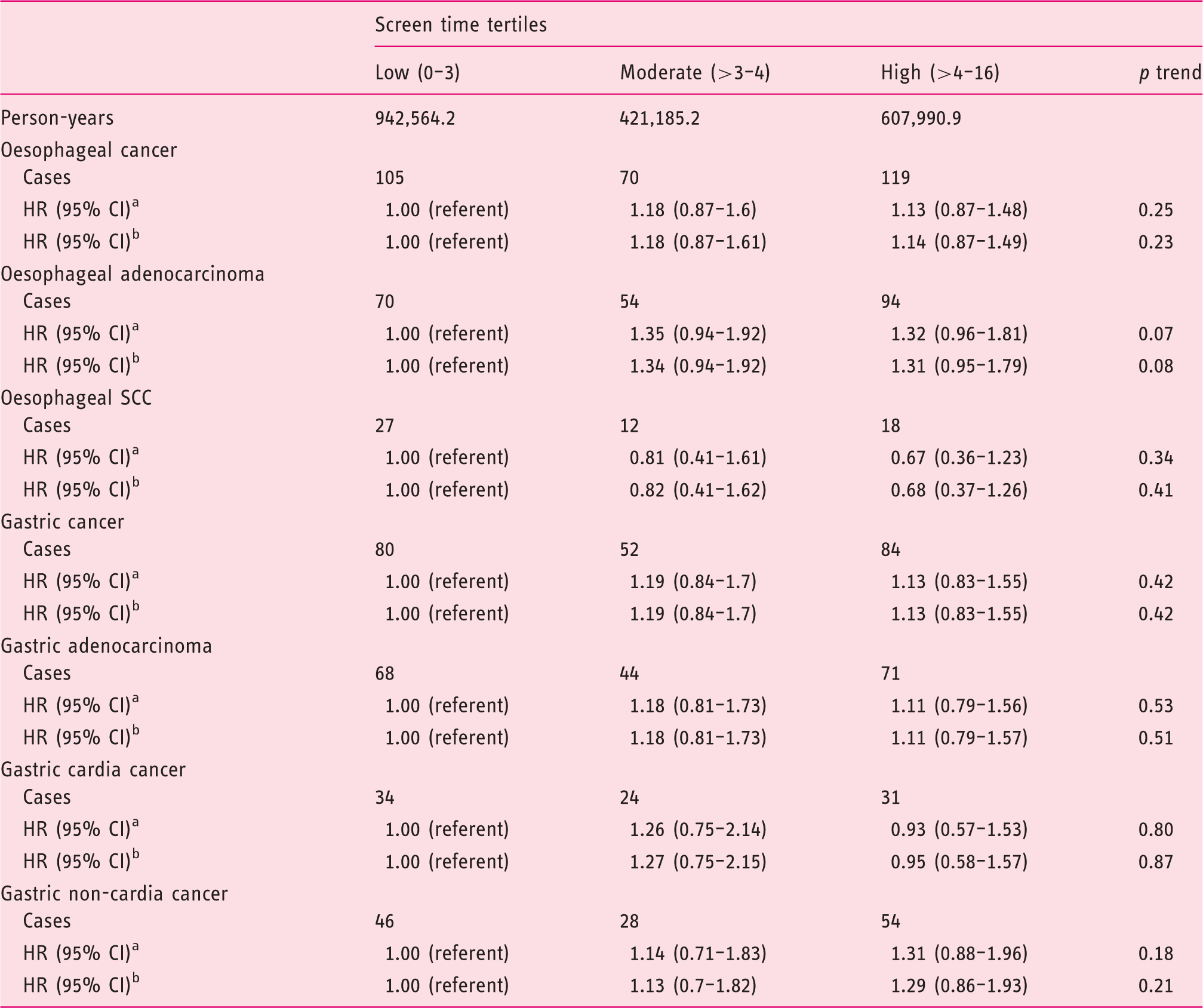
CI: confidence interval; HR: hazard ratio; SCC: squamous cell carcinoma; UK: United Kingdom.
Adjusted for sex, educational attainment (degree vs not), Townsend deprivation index (quintiles), smoking status (never, former light, former heavy, current light, current heavy), height at baseline (metres), alcohol intake (never drinker, former drinker, current light to moderate drinker, current heavy drinker) and baseline date. Age was used as the timescale.
Additionally adjusted for total MET hours of physical activity.
The associations between physical activity and risk of oesophageal and gastric cancer were similar when stratified by comorbidity status, smoking, BMI and sex (Supplementary tables 1–4) and no statistically significant interactions were apparent.
In post-hoc analyses using MET-minutes per week, individuals reporting 600–1500 MET-minutes per week were at a reduced risk of OAC, gastric cancer, gastric adenocarcinoma and gastric non-cardia cancer compared to individuals reporting < 600 MET-minutes per week (Supplementary table 5).
Discussion
This large, prospective cohort study indicates that physical activity was not associated with overall risk of oesophago-gastric cancer; however, results differed by subtypes. Moderate, rather than high, physical activity levels were associated with the strongest reductions in OAC risk. Non-significant increased risks of OAC were also observed for individuals reporting the highest hours of sedentary behaviour.
In contrast with previous systematic reviews,4,5,16 the present study did not report an inverse association with OAC or oesophageal cancer when comparing the most to least physically active. The previous meta-analyses, however, were primarily driven by case-control studies, with only non-significant associations between physical activity and OAC risk observed in cohort studies.8,17 We did, however, observe a 38% risk reduction of OAC when comparing moderate levels to low levels of physical activity.
Our observation of a lack of dose-response relationship between physical activity and OAC is perhaps unsurprising. OAC risk is strongly associated with both the frequency and duration of gastroesophageal reflux symptoms, 18 and these symptoms are common in athletes.19,20 One case-control study 21 observed that moderate physical activity was associated with a 60% reduction in such symptoms, whereas another study noted high-intensity physical activity was associated with a three-fold increase in acid exposure. 22 High-intensity physical activity may increase acid reflux through relaxation of the lower oesophageal sphincter, enhanced pressure gradient between the stomach and oesophagus and increased mechanical stress as a result of bouncing organs. 20 These findings suggest that the experience of reflux symptoms observed during physical activity may be intensity dependent, perhaps explaining why our current study found that moderate, rather than high, physical activity levels were associated with reductions in OAC risk.
Evidence from previous studies assessing the association between physical activity and gastric cancer subtypes is mixed. In the present study, physical activity was not associated with reduced risk of gastric cardia cancer. Although our present study initially found a significant reduction in gastric non-cardia cancer for the most physically active, the association became attenuated after excluding events in the first three years of follow-up. This attenuation could be due to lower statistical power or may indicate that reverse causation may have influenced the initial results.
In contrast with previous cohort7,8,23 results, we observed a significant increased risk of oesophageal SCC with both moderate and high levels of physical activity, when compared with low levels even after adjustment for BMI and waist:hip ratio. Previous studies have shown an inverse-relationship between BMI and oesophageal SCC risk.24,25 This finding should, however, be interpreted with caution owing to the small number of cases observed in the reference category group (n = 3), and no calculation of oesophageal SCC was possible after excluding cancers in early years of follow-up.
Identifying a clear biological mechanism linking physical activity and oesophago-gastric cancer and specifically OAC is, however, lacking. One of the most commonly hypothesised mechanisms by which physical activity is thought to reduce the risk of other cancers is through the reduction of systemic inflammation. 26 However, we adjust for body composition in our analyses, and associations were only modestly attenuated, suggesting any changes of physical activity on inflammatory markers such as insulin-like growth factor-1 25 could be partly independent of BMI changes.
While our results suggest a protective effect of high levels of physical activity for gastric non-cardia cancer and moderate levels of physical activity for OAC, further studies are required to confirm these results. A recent feasibility trial 27 of an exercise intervention in males at risk of OAC found that a moderate-intensity aerobic and resistance exercise intervention significantly reduced waist circumference (–4.5 (95% CI 7.5 to –1.4) cm; p < 0.01) in overweight and inactive men with Barrett’s oesophagus, the pre-cursor to OAC. Similar research may provide adequate aetiological evidence to inform on the development and advocacy of future physical activity interventions for cancer prevention.
It is currently recommended that individuals in the UK participate in at least 150 minutes of moderate-intensity physical activity per week 28 for general health, with similar recommendations for cancer prevention guidelines. 29 Therefore, based on our present results, it may be a much more achievable and realistic target to develop interventions aiming to encourage individuals with low levels of physical activity to participate in moderate levels.
Despite previous systematic reviews 9 observing an increased risk of other cancer types in relation to sedentary behaviour, less is known in regard to its association with oesophago-gastric cancer. Results from our current study are supported by a meta-analysis 29 which reported no associations between sedentary time and oesophageal cancer. However, our current study observed non-significant increased risks of OAC for individuals reporting the highest hours of sedentary behaviour, with proposed mechanisms including an increased number of reflux episodes with increased sitting time 30 and increased body weight. 31
Major strengths of this study were its large sample size and prospective design, minimising the impact of recall bias in participants with and without upper GI cancers. In addition, cancers were identified through robust, internationally accepted cancer registry classification systems. The availability of information on BMI, smoking, comorbidities and several other potentially important confounders, as well as information on the anatomical subsite of the tumour, are further major strengths of this study.
There are, however, limitations to this study. Information on Helicobacter pylori status was not available to ascertain potential confounding of the association with gastric cancer risk. Statistical power for stratified analyses was limited. Information on domain-specific physical activity would also be useful to elucidate physical activity context. 16 Self-reported measurement of physical activity and sedentary behaviour may be subject to reporting and social desirability bias. 32 Further research using validated and objective measures of physical activity such as accelerometers and pedometers may resolve these issues. 32 Nevertheless, as data were collected prior to diagnosis, it is unlikely that any misclassification will have been differential between cancer cases and controls. The UK Biobank also had a poor response rate of 5.5%, 33 potentially indicating response biases and differences in sociodemographic variables which may limit generalisability of findings. However, our sample still included a range of educational attainment and deprivation across participants.
In conclusion, findings from this large UK prospective cohort show a decreased risk of OAC associated with moderate levels of physical activity. There were also suggestions of a direct association between screen-based sedentary behaviour and OAC risk.
Supplemental Material
Supplemental material for Physical activity, sedentary behaviour and risk of oesophago-gastric cancer: A prospective cohort study within UK Biobank
Supplemental material for Physical activity, sedentary behaviour and risk of oesophago-gastric cancer: A prospective cohort study within UK Biobank by Andrew T Kunzmann, Kristian P Mallon, Ruth F Hunter, Chris R Cardwell, Úna C McMenamin, Andrew D Spence and Helen G Coleman in United European Gastroenterology Journal
Footnotes
Funding
This work was supported by a Department for Education PhD studentship for K.P.M. and the Ochre charity (registered charity number: SC032343) for A.T.K.
Declaration of conflicting interests
None declared.
Ethics approval
The UK Biobank conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a prior approval by the North West Multi-Centre Research Ethics Committee (10 May 2016). This research was conducted using the UK Biobank Resource under application number 34374. Investigators may apply to access the UK Biobank study data through the processes described at ![]() .
.
Informed consent
All participants provided written informed consent.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.