
Abstract
Background
The diagnosis of small-bowel neuroendocrine tumors (SbNETs) has improved with the advent of video capsule endoscopy (CE) and double-balloon enteroscopy (DBE). The data describing the efficacy of CE/DBE in the detection of SbNETs are scanty.
Aim
The aim of this article is to review the current evidence on the role of DBE and CE in the diagnosis of SbNETs.
Material and methods
A bibliographical search was performed in PubMed using the following keywords: “neuroendocrine tumors and enteroscopy/and capsule endoscopy” and “small bowel neuroendocrine tumors.”
Results
CE and DBE can be complementary and show a similar diagnostic yield. The number of false-negative results has not been established yet because of the “work-up bias” observed in the majority of the studies.
Conclusions
DBE and CE appear to be both safe and effective procedures useful in the diagnosis of SbNETs. Further studies are required to clarify their potential complications and relationship with other techniques, particularly nuclear imaging.
Introduction
Neuroendocrine tumors (NETs) account for about one-third of all small-bowel (Sb) neoplasms. 1 The small intestine, and particularly the ileum, is the most common NET site in the human body. SbNETs usually occur in the sixth and seventh decades of life, although they may affect all age groups and there is no a gender difference. The estimated prevalence is 0.32–1.12 per 100,000 of the population per year.2–4 Autoptic prevalence has been estimated as 1.22%. 5 Of note, over the last 30 years, the incidence of SbNETs has increased by 460%. 6
SbNETs can be classified as functioning and non-functioning tumors. 7 The majority of SbNETs are well differentiated and exhibit a slow growth; however, on rare occasions they may be poorly differentiated, with rapid growth and a poor prognosis,6,8 thus their prompt diagnosis is urgently needed.
Historically, SbNETs have proven difficult to diagnose, given their nonspecific presentation and poor accessibility of the distal Sb. 9 The diagnosis of SbNETs is based on clinical (i.e. symptoms of carcinoid syndrome and abdominal pain or obstructive symptoms in functioning and non-functioning forms, respectively), biochemical (i.e. plasma chromogranin A (CgA) and 5-hydroxyindoleacetic acid (5-HIAA) excretion in urine), radiological (i.e. computed tomography (CT) and magnetic resonance imaging (MRI) or nuclear imaging) and endoscopic data. The identification of an Sb primary tumor on CT and MRI either via the standard technique or in combination with enteroclysis is challenging. 10 Somatostatin receptor-based imaging, particularly positron emission tomography (PET)/CT with 68Ga-DOTA-peptides, appears to be the most sensitive modality in the detection of low-grade NET,11,12 although small tumors may be misdiagnosed. In the presence of metastatic disease the detection of the primary tumor is recommended both in resectable and nonresectable disease. In view of the high risk of abdominal complications, resection of the primary tumor is advocated even in metastatic disease for palliative purposes;2,13 furthermore, resection is usually suggested in order to facilitate treatment in clinical trials considering specific primary tumor site as inclusion criterion. 14 In addition, the approval of medical therapies as targeted therapy depends on the primary tumor site, therefore the knowledge of the primary tumor site is crucial in terms of evidence-based medicine to plan treatment for patients. However, in 5%–10% of patients with neuroendocrine metastatic disease, the primary tumor site remains unknown despite extensive morphological and/or functional imaging work-up.15,16
The diagnosis of SbNETs has been importantly improved with the advent of video capsule endoscopy (CE) in 2000 and double-balloon enteroscopy (DBE), the most promising device-assisted enteroscopy (DAE) system, in 2001, which allow for direct visualization of the entire Sb. CE has emerged as a first-line modality in detection of Sb pathologies,17–19 including obscure bleeding, 20 suspected Crohn’s disease, 21 tumors,22,23 irregular findings on standard imaging and clinical symptoms in the presence of normal imaging results.24–26 As regards DAE, different systems have been developed, such as single-balloon enteroscopy (SBE) and spiral enteroscopy (SE), but DBE is the most widely used, with a large number of studies proving its efficacy in a range of Sb diseases.
Both CE and DBE have been reported to achieve similar outcomes in terms of diagnostic yield for Sb lesions, 27 even if DBE has the advantage of being an operative technique, allowing the performance of biopsies, polypectomy, argon plasma coagulation, and balloon dilation. CE is usually performed first-line in the case of a suspected lesion located in the Sb; in the case of positive findings on CE (or on standard imaging) DBE is the preferred choice in a two-step process because of its diagnostic and therapeutic potential.
Data describing the efficacy of CE and DBE in the detection of SbNETs are scanty, given the low incidence of NETs and the still-limited use of these techniques in routine clinical practice. However, series reporting the diagnostic yield of CE or DBE for small-intestinal lesions usually report data on SbNETs as well. According to the European Neuroendocrine Tumor Society (ENETS) guidelines, CE and DBE may be considered for investigation of more proximal parts of the ileum or of the jejunum, although their diagnostic accuracy has to be established and they are not widely available. Furthermore, data on potential procedural risks of these methods in NETs are lacking. 2
Herein, we aimed to review current evidence from the literature on the role of CE and DBE in the diagnostic pathway of SbNETs.
Methods
An extensive bibliographical search was performed in PubMed using the following keywords, including both medical subject heading (MeSH) terms and free language words/phrases: “neuroendocrine tumors and enteroscopy,” “neuroendocrine tumors and capsule endoscopy” and “small bowel neuroendocrine tumors” in order to identify all pertinent articles published between 2000 and 2015. The lists of references from the selected studies were manually examined to identify further relevant reports. Non-English language papers were excluded. The quality and strength levels of the results were considered and, when available, meta-analyses and systematic reviews, large epidemiological studies and randomized control trials represented the main data sources.
Results
There were a very large number of results returned for each of our search parameters; 112 records were identified through PubMed searching and nine additional records were retrieved through other sources (lists of references from the selected studies, conference reports). After filtering for year range, human studies, and article type, and removing duplicates, we identified a total of 55 articles (of which there were 11 epidemiological NET studies, 29 papers concerning CE and 15 concerning DBE) that show the strongest level of evidence, as for the scope of this systematic review. The flowchart elucidating the process of study selection is shown in Figure 1.
The flowchart elucidating the study selection process.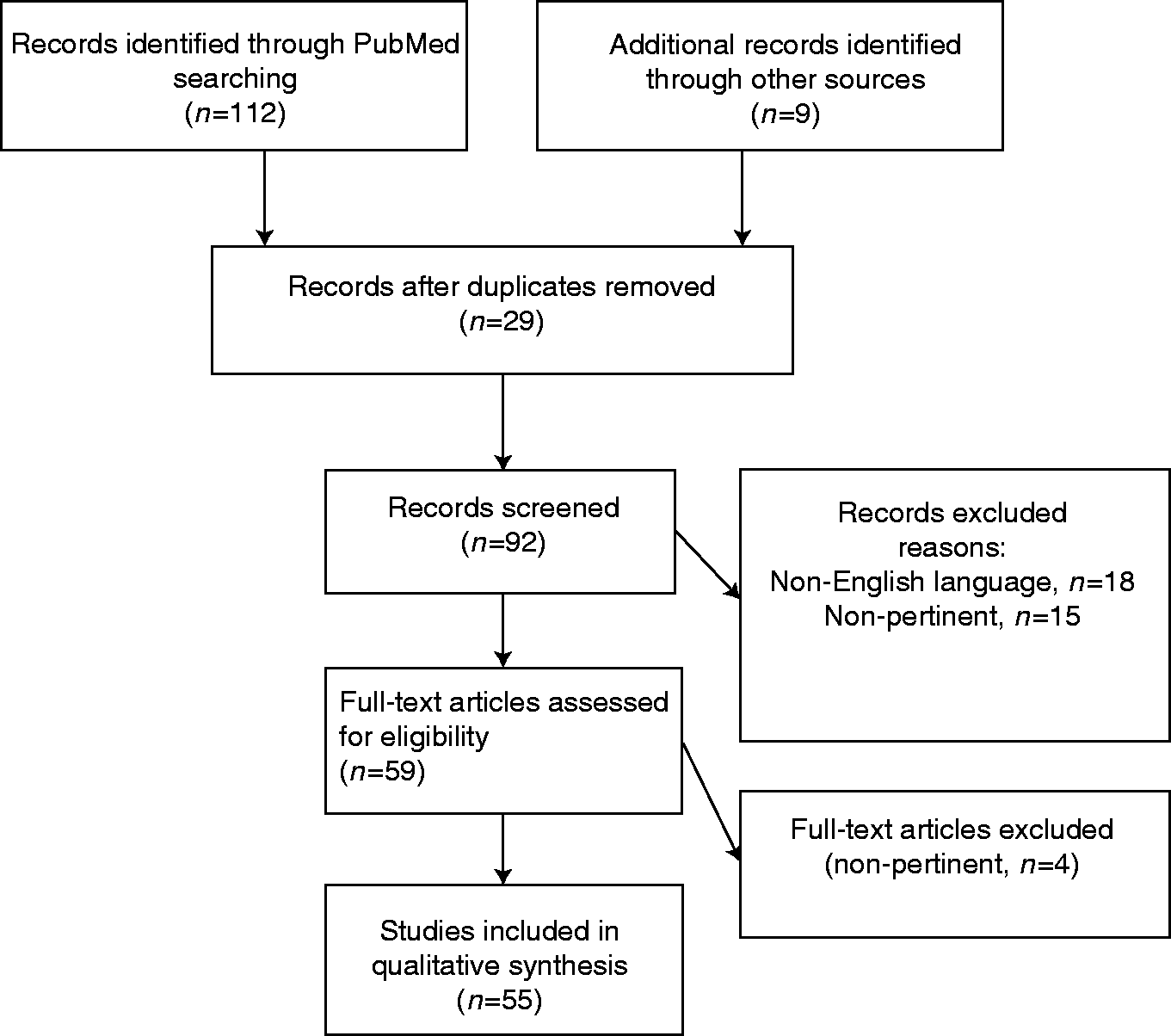
CE
Wireless CE was invented by Gavriel Iddan et al. 17 in the mid-1990s. CE provides visualization of the entire Sb by transmitting wireless images from a disposable capsule to a data recorder worn by the patient. Obscure gastrointestinal bleeding in patients with normal upper and lower endoscopy represents the main indication for CE, even if CE has become a well-established tool for several pathologies, including suspected Sb tumors and Crohn’s disease. 14 CE has proven to be a safe, patient-friendly and minimally invasive modality for visualization of the Sb.
The introduction of CE has improved the early detection rate of SbNETs, which may be difficult to diagnose through standard imaging. A comparison of CT, enteroclysis, nuclear imaging, and CE of the Sb showed that CT and enteroclysis were unable to detect a primary tumor, whereas nuclear imaging identified abnormalities in the abdominal area in about two-thirds of patients but was unable to differentiate between intestinal and mesenterial localization. 28 In contrast, in the same study, CE showed a high diagnostic yield (45%) in identifying primary tumors. Of note, in 12 of 20 patients (60%), CE showed small-intestinal lesions that were then confirmed histologically as NET in six of seven patients who underwent surgery. 28
Cobrin et al., in a retrospective analysis of 562 patients who underwent CE for bleeding alone or in addition to another indication, such as abnormal imaging, reported that a final diagnosis was obtained by CE in 49.3% of the patients; of note, 10 (1.8%) out of the 50 patients (8.9%) who were diagnosed with Sb tumors had NETs. 24 An Australian multicentric study including 416 patients observed that CE detected Sb tumors in 26 (6.2%) patients, including 23.1% with SbNETs. 29 Rondonotti et al., in their multicentric study, showed that of 5129 patients undergoing CE for different indications, 124 (2.4%) had Sb tumors including 15% with NETs. 30
Sidhu and McAlindon conducted a retrospective review of consecutive patients who underwent CE over a seven-year period. 31 Twenty-four patients (1.5% of all patients included) were found to have an Sb tumor on CE, of which two were found to be NETs. Patients had a mean number of 4.7 tests prior to CE, which included gastroscopy, colonoscopy, Sb radiology, CT scanning, mesenteric angiograms and red cell-labeled scans. 31
Frilling et al., in their recent retrospective study including 390 patients with metastatic NETs, showed that in the 11 (2.8%) patients in whom the primary tumor was not located radiologically, CE identified SbNETs (confirmed histologically) in 8/10 patients in whom it was successful. 14
Aside from the impossibility of obtaining biopsy samples or performing therapeutic procedures, the main limitation of CE is the possible miss rate in case of submucosal lesions, which could affect the diagnostic potential in the setting of SbNETs, often presenting as submucosal masses without a mucosal component.32,33
Enteroscopy complications
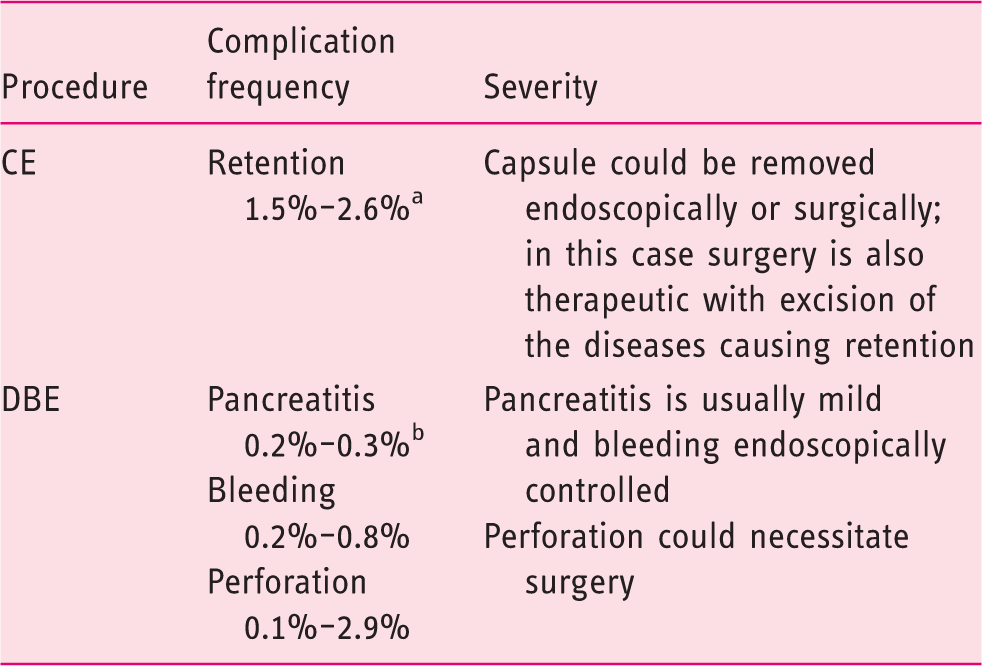
In the absence of obstructive symptoms. In this case a patency test or other investigations should be considered.
In case of diagnostic procedure, pancreatitis is the only possible complication.
CE: video capsule endoscopy; DBE: double-balloon enteroscopy.
Studies showing diagnostic performances of small-bowel endoscopic techniques in the specific setting of neuroendocrine tumors (NETs)

Diagnostic yield was defined as the ratio of the number of cases of small bowel neuroendocrine tumors to the number of all cases examined.
CE: video capsule endoscopy; DBE: double-balloon enteroscopy; NA: not available.
Retained capsules are usually asymptomatic, although intestinal obstruction, partial or complete, may occur. According to the 2009 consensus by the European Society of Gastrointestinal Endoscopy, an Sb imaging or a patency capsule (in the case of the GIVEN® system) should precede CE in patients with suspected strictures. 36 Another very rare complication is perforation of the Sb. 33 Capsule aspiration may also occur, especially in elderly male patients with comorbidities and/or swallowing difficulties. 34 In the study by Frilling et al., 14 capsule retention occurred in one patient who presented with extensive abdominal metastatic disease. This patient remained completely asymptomatic. In addition, one patient only showed difficulties in swallowing the capsule.
DBE
DBE is based on the combined use of a balloon-loaded enteroscope and a similarly balloon-loaded overtube. A stepwise progression of the enteroscope throughout the small intestine is achieved by alternately inflating and deflating the two balloons as well as straightening the endoscope with the overtube. The procedure can be carried out through the oral (antegrade) or the anal (retrograde) route. With a combined oral and anal approach a complete Sb examination can be achieved in up to 86% of patients.38,39
DBE has gained acceptance as a reliable tool for the detection of Sb lesions and allows for direct access to the lesion. Studies focused on DBE in the setting of NETs are scanty. Bellutti et al., in their study involving 12 consecutive patients who underwent DBE to detect the primary tumor in patients with suspected NET or with liver metastases of a NET, found a diagnostic yield of DBE for primary tumor search of 33%. 1 Of note, biopsies were unable to provide evidence of a NET in any of the patients with a visible tumor of the Sb, likely because of a sampling issue and/or the submucosal location of the tumor; thus, DBE results were not as advantageous for detecting SbNET as previously assumed, in comparison to CE, even if a direct comparison was not possible as not all of the patients underwent CE. 1 Moreover, in two patients with suspected NET (17% of their series), laparotomy and intraoperative endoscopy did not confirm the tumor, thus resulting in 17% of false-positive results. The authors themselves suggested that DBE should be performed only in selected patients, on the basis of a previous positive work-up. Scherübl et al. reported their single-center experience, which highlights that DBE should be taken into account as an effective new technique for localizing and verifying NETs of the jejunum and ileum. 40 In their series, five consecutive patients suffering from metastatic midgut carcinoids underwent DBE over a 12-month period and a NET of the ileum was detected in four out of the five men; histopathological evaluation of biopsy specimens confirmed the diagnosis revealing well-differentiated NETs. DBE failed to localize the primary tumor in only one of the five patients, while conventional radiologic imaging did not visualize any of the primary tumors. 40
The entire exploration of the Sb is crucial in selected cases such as in patients with NETs, as these tumors can be multiple and their proper detection may affect further management. 41 Such tumors are extremely difficult to diagnose and localize before surgery with conventional imaging techniques. 42 When a NET is found in the Sb, the possibility of multiple tumors should be considered, as one-fourth of SbNETs are reported to be multiple. Multiple SbNETs usually occur in younger patients and have both a significantly greater risk of developing carcinoid syndrome, and a poorer prognosis than patients with solitary tumors. 43 DBE may be useful in these cases prior to surgery in order to get a histological diagnosis by a biopsy specimen and to determine the excision range of the Sb by tattoo injection. 44
Studies on DBE efficacy in detecting Sb tumors are available in the literature. In a recent large retrospective study including 1106 patients who underwent 1652 DBE procedures, 134 (12.1%) patients were found to have an Sb tumor and NET was detected in 19.4% of patients,
9
mainly located at the ileum, as described in previous studies.
45
Similar findings were reported in the retrospective study including 555 patients by Partridge et al.,
46
who reported that NET was the most common Sb cancer identified by DBE (eight patients with ileal NETs out of 20 patients diagnosed with Sb tumors (40%); two of these eight patients had multiple tumors). However, these results may have been affected by the peculiar geographical distribution of the cases, considering the increasing incidence of NETs reported in the United States.
45
Different results have been reported in a Japanese study of DBE, in which lymphoma, followed by gastrointestinal stromal tumor (GIST) and adenocarcinoma, were found to be the most common Sb tumors detected by DBE.
47
Furthermore, Robles et al. in a recent European single-centre retrospective study including 627 patients, of whom 28 (4.5%) were diagnosed with a malignant tumor, suggested that DBE is critical in the management of Sb tumors and may affect their management by providing information to guide a possible surgery or other procedures and by delaying or avoiding emergency surgery.
41
In this series, GIST was the most common Sb tumor detected by DBE followed by adenocarcinoma; NETs were diagnosed in four (14.3%) patients.
41
Figure 2 shows the endoscopic appearance of an SbNET.
Endoscopic appearance of a small bowel neuroendocrine tumor (SbNET). Double-balloon enteroscopy (DBE) brings the advantage of allowing the obtaining of tissue samples.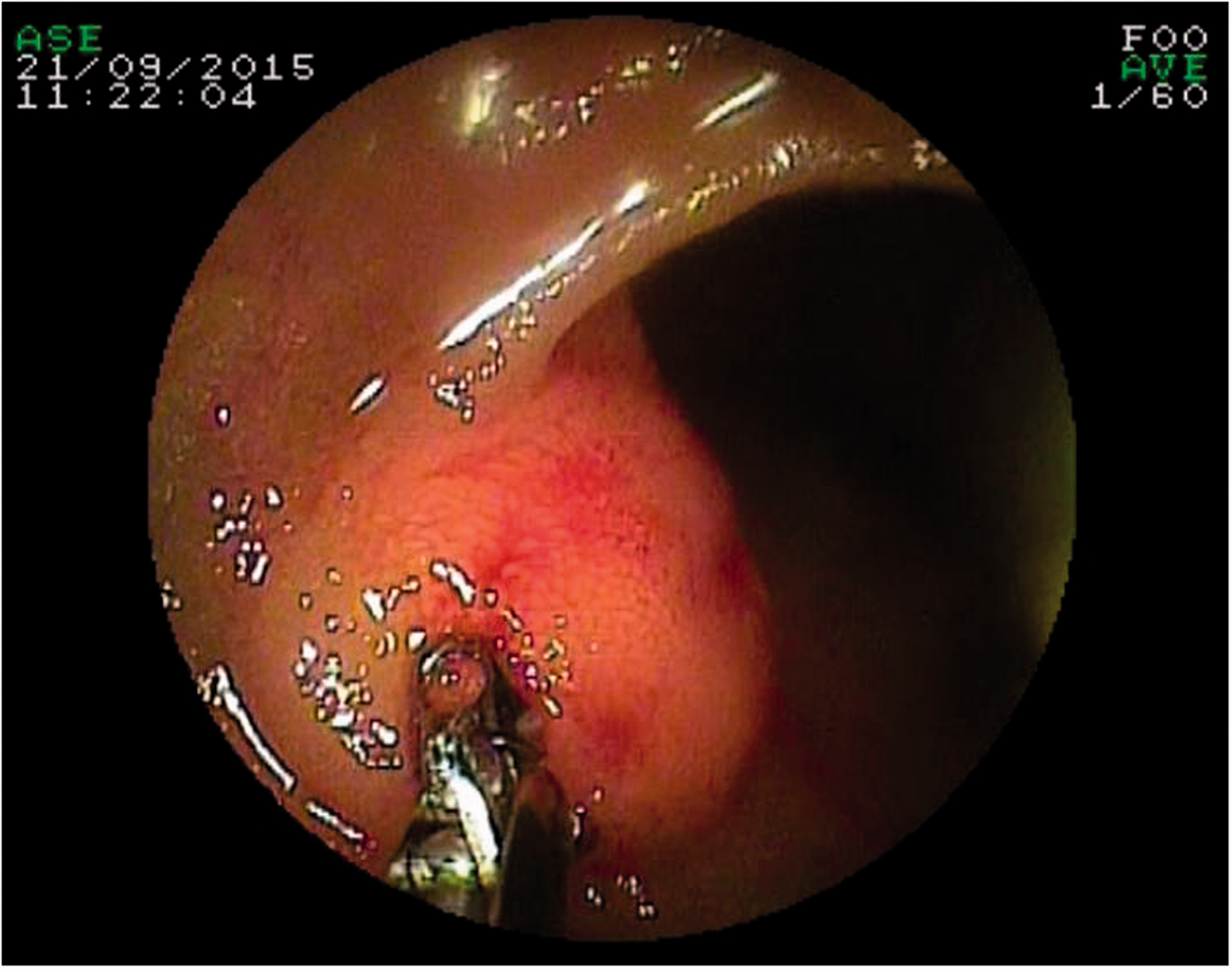
DBE is usually considered a safe technique also in the elderly; however, because of its invasive nature, some complications may occur including Sb perforation, hemorrhage, mucosal damage, especially in the case of therapeutic DBE, as well as acute pancreatitis. 46 In case of diagnostic DBE, pancreatitis (usually mild) is almost the unique possible complications, occurring in about 0.3%–0.4% of enteroscopies from the oral route, without the necessity of surgery. Endoscopic experience, procedure duration and balloon insufflation after Treitz are the main factors reducing complications 48 (Table 1).
CE versus DBE in the detection of Sb tumors, including SbNETs
DBE has been reported to be superior to CE in terms of image clarity, handing controllability, biopsy and endoscopic treatment. 49
Comparing the diagnostic yield of CE and DBE, Ross et al. reported that DBE can detect small-intestinal mass lesions responsible for gastrointestinal bleeding that are missed by CE in some patients. 50 Conversely, Li et al. in their study including 218 patients evaluated for suspected Sb disease found that CE was superior to DBE in the diagnosis of Sb diseases, suggesting that CE should be selected for the initial diagnosis in patients with suspected Sb diseases, especially in patients with obscure gastrointestinal bleeding. 51 However, DBE may be used to confirm suspected findings from CE and may be taken into account as a good complementary approach after initial diagnostic imaging using CE. 51 A recent case report presented by Koornstra et al. showed the complementary roles of CE and DBE: in a patient incidentally diagnosed with a neuroendocrine liver metastasis, CE was used to screen the Sb for abnormalities and determine the route for DBE, and DBE was useful in establishing a histological diagnosis and marking the lesion to facilitate surgical resection. 38
Lewis et al. conducted a pooled analysis of 24 studies (for a total of 530 patients) that prospectively compared CE with other modalities (push enteroscopy in 300 patients, Sb series in 140 patients, and colonoscopy with ileoscopy in 90 patients). 52 CE alone was found to detect 87% of the disease instances, while the comparison method alone detected 13%. The yield for push enteroscopy alone was 14.8%, for Sb series it was 9.9%, and for colonoscopy it was 13.2%. Miss rate was 10% and 73% for CE and the comparison methods, respectively. Based on these findings, the authors concluded that CE is the state-of-the-art method for noninvasive detection of Sb disease. 52
The current European Society of Gastrointestinal Endoscopy (ESGE) guidelines recommend an early use of Sb CE in the search for an Sb tumor when obscure gastrointestinal bleeding and iron-deficiency anemia are not explained otherwise, also considering that the diagnostic yield of CE has been reported to be similar to that of DBE in patients with obscure bleeding. 53 However, the risk of false-negative CE results needs to be taken into account, especially for lesions located in the duodenum and proximal jejunum and for submucosal masses where a mucosal component is absent, such as NETs or gastrointestinal stromal tumors.32,33,54 Furthermore, whenever an Sb tumor is strongly suspected, no specific investigations before CE are recommended in patients without evidence of stenosis or previous Sb resection. In the cases of either uncertain diagnosis of Sb tumor or detection of a submucosal mass at CE, biopsy sampling by DAE is recommended. 33
Conclusion
The identification of a primary tumor site in patients with neuroendocrine metastases is fundamental for both the treatment planning and the estimation and improvement of prognosis. Resection of the primary lesion and loco-regional lymph node metastases even in the presence of liver metastases is generally recommended in order to improve the survival and decrease the risk of complications such as intestinal occlusion or abdominal ischemia. 55
The diagnosis of Sb tumors including NETs has improved with the advent of CE and DBE, the most promising DAE system, which may be complementary and show a similar diagnostic yield. However, considering that they are not widely available, data reporting their efficacy in the setting of SbNETs are scanty (Table 2) and current guidelines are lacking. The ENETS guidelines recognize their potential role in the diagnostic pathway of SbNETs, even if their role in routine staging needs further clarification, also considering the lack of data on potential procedural risks of these methods in NETs. 2
No data on sensitivity and specificity are currently available, mainly because of a “work-up bias” observed in almost all the studies analyzed. In terms of diagnostic yield, data from the literature indicate that DBE shows a variable diagnostic yield ranging from 30% to 80%, whereas CE from 45% to 72% in the diagnosis of SbNETs. Both procedures are considered safe. According to data from the literature, when an SbNET is suspected, CE should be the first choice whenever possible in order to detect any abnormalities (given the lower rate of false-positive results), while DBE should be reserved for those patients with abnormal CE, in order to take biopsies for final diagnosis and tattoo marking prior to surgery, or contraindications to CE (i.e. intestinal occlusion, known bowel stenosis).
However, as stated by ENETS guidelines, the choice between CE and DBE should be based on local expertise as well and potential risks need to be weighed against benefits. 2
Furthermore, as SbNETs are often multifocal, these techniques may be helpful in identifying multiple sites, allowing physicians to tailor the proper surgical intervention to each individual patient even in a preoperative setting. However, CE and DBE should always be considered complementary to surgery.
Nuclear medicine imaging has recently gained acceptance as an accurate technique in the diagnostic pathway of NETs, even if it has been reported to be unable to differentiate between intestinal and mesenterial localization, 28 which may be studied through CE and DBE.
Moreover, NETs of unknown primary location represent a clinical challenge and despite the continuous advances in diagnostic nuclear medicine imaging and immunohistochemical methods, CE/DBE may play an important role in this specific setting to better localize the primary site.
Owing to the paucity of studies focused on CE and DBE in the neuroendocrine setting, further studies are needed to draw more solid conclusions, particularly to better clarify the role of these techniques in the diagnosis of SbNETs, their potential complications and their relationship with other techniques, particularly nuclear imaging.
Footnotes
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.