
Abstract
Background
Radiofrequency ablation (RFA) is currently recommended for dysplastic Barrett’s oesophagus (BO); however, there are limited data on treatment response when stratified by baseline histology.
Objective
The objective of this article is to evaluate RFA outcomes and durability for BO with different baseline histology.
Methods
Patients treated with RFA between 2007 and 2017 at a single institution were retrospectively included. Outcome measures were: (a) complete remission of dysplasia (CRD) and intestinal metaplasia (CRIM) at 18 months, (b) complication rate and (c) durability of CRD and CRIM.
Results
A total of 148 patients underwent RFA, of whom 113 completed the treatment protocol (21 low-grade dysplasia (LGD), 46 high-grade dysplasia (HGD) and 46 intramucosal carcinoma (IMC)). CRD and CRIM were achieved in 94.7% and 78.8% of patients, respectively. When stratified by baseline histology, there was no significant difference in CRD between groups (LGD, 95.2%; HGD, 95.7%; and IMC, 93.5%; p = 0.89). Similarly, there was no significant difference in CRIM between groups (LGD, 71.4%; HGD, 76.1% and IMC, 87.0%; p = 0.39). CRD and CRIM durability at 24 months for LGD, HGD and IMC were 100%, 97.7% and 100% (log rank p = 0.31), and 100%, 89.0% and 95.5%, respectively (log rank p = 0.62).
Conclusion
Baseline histology is not a predictor of RFA response. Once CRD and CRIM are achieved, these effects are durable over time.
Keywords
Key summary
Established knowledge on this topic
Radiofrequency ablation (RFA) is the therapy of choice for flat dysplastic Barrett’s oesophagus (BO). The eradication of oesophageal intestinal metaplasia is durable over time. There are limited data on the treatment outcomes and long-term durability of BO when stratified by baseline histology.
New findings from this study
Baseline histology is not a predictor of short-term response to RFA. Long-term durability of the initial ablation effect is not affected by the original grade of neoplasia.
Introduction
Barrett’s oesophagus (BO) is a premalignant condition which predisposes to oesophageal adenocarcinoma (OAC), an aggressive tumour with increasing incidence in the Western population over the past four decades. 1 Malignant progression of BO occurs in a stepwise manner through early neoplastic stages known as low-grade dysplasia (LGD), high-grade dysplasia (HGD) and intramucosal carcinoma (IMC). Although BO is the only known precursor to OAC, the risk of progression of non-dysplastic BO to OAC is low, ranging from 0.12% to 0.40%.2–5 However, the presence of dysplasia significantly increases this risk, with reports estimating the risk of progression from LGD to HGD or IMC to be as high as 9.1% per patient-year. 6
Radiofrequency ablation (RFA) is an endoscopic ablative technique which utilises thermal energy to ablate BO mucosa. Until recently, gastroenterology societies recommended RFA only for treating BO with HGD and flat IMC. However, following a recent randomised, controlled trial (RCT), the indication has been extended to LGD. 7 In addition, given the risk of metachronous cancer following endoscopic mucosal resection (EMR) for IMC, 8 RFA has also been recommended for residual BO post-EMR regardless of the presence of dysplasia elsewhere.9,10
There is limited evidence on the comparative outcomes of RFA for BO when stratified by baseline histology. The aim of this study was to compare RFA outcomes and durability in patients with different baseline histology.
Methods
Inclusion criteria
This was a retrospective study on prospectively collected data on patients receiving RFA between years 2007 and 2017. Indications for RFA were flat, dysplastic BO and residual BO following EMR for visible nodular lesions. BO was defined as the presence of endoscopically visible columnar-lined oesophagus with intestinal metaplasia (IM) confirmed on biopsies.
The study was performed with approval from the Joint UCL/UCLH Committees on the Ethics of Human Research (approval number 08/H0714/27118, approval date: 3 September 2008). Written, informed consent was obtained from each patient. The study protocol was conducted in accordance to the ethical guidelines of the Declaration of Helsinki.
RFA protocol
RFA was performed using the BARRX™ system (Medtronic, Dublin, Ireland). The BARRX™ 360, BARRX™ 60, BARRX™ 90, BARRX™ Ultra or through-the-scope ablation devices were used depending on the length of the BO with selection of the device at the discretion of the operator. An intermediary cleaning phase between ablations was used up until November 2012, after which and following a European consensus meeting, the cleaning phase was abandoned.11,12 Patients were scheduled for repeat RFA at approximately three-monthly intervals until endoscopic and histologic remission were achieved. Endoscopic remission was defined as the lack of visible columnar epithelium of ≥1 cm. The presence of an irregular Z-line (short tongues of BO <1 cm) post-RFA was also considered remission if quadrantic biopsies excluded IM. For nodular lesions, EMR was performed for therapeutic purposes and to allow full extent of histopathological staging. Residual areas of BO post-EMR were treated with RFA if dysplasia was diagnosed on EMR specimens. Argon plasma coagulation was performed at the discretion of the endoscopist to ablate small, visible BO islands during follow-up.
Histological analysis
All cases of LGD and HGD were confirmed by at least two gastrointestinal pathologists. Patients with adenocarcinoma were included in this study if histopathology showed low-risk features (T1a with no lymph vascular invasion, or T1b tumours confined to the upper third of the submucosa, within 500 µm, moderately or well differentiated and no evidence of lymphovascular invasion). 9
Outcome measures
Outcome measures assessed were: (a) complete remission of dysplasia (CRD) and complete remission of intestinal metaplasia (CRIM) at 18 months, (b) complication rate including strictures and (c) durability of CRD and CRIM. CRD was defined as eradication of dysplasia but with persistent columnar epithelium with IM. CRIM was defined as eradication of both dysplasia and IM on biopsies taken once endoscopic remission (absence of visible BO) was achieved. If IM was found at the gastro-oesophageal junction (GOJ) at the first post-RFA follow-up, circumferential ablation of the GOJ with focal BARRX™ device was performed. Presence of focal IM at the GOJ (at most in one of the four quadrantic biopsies) following CRIM was not considered relapse. Stricture was defined as oesophageal narrowing requiring dilation to achieve symptom resolution or to allow further RFA treatments. Asymptomatic strictures which did not affect passage of endoscope were not considered a complication. Rescue EMR was defined as EMR to treat endoscopically visible nodular lesions suspicious for BO-related neoplasia following commencement of RFA. We also assessed whether age, gender, length of BO, prior EMR and baseline histology were predictors of response to therapy.
Statistical analyses
Normality testing for continuous variables was performed using Shapiro–Wilk test. One-way analysis of variance or Kruskal–Wallis was used to compare means between groups. Rates of CRD and CRIM between groups were compared with Pearson chi-square test or, when not applicable, Fisher’s exact test. Predictors or RFA response were studied with multiple regression with covariates selected using the backward stepwise elimination method. Durability of CRD and CRIM were assessed with Kaplan–Meier analysis. A p value of <0.05 denotes statistical significance. Statistical analyses were performed using IBM SPSS for Windows version 24.0 (Armonk, NY, IBM Corp).
Results
Patient characteristics
Patient baseline characteristics stratified according to grade of dysplasia.
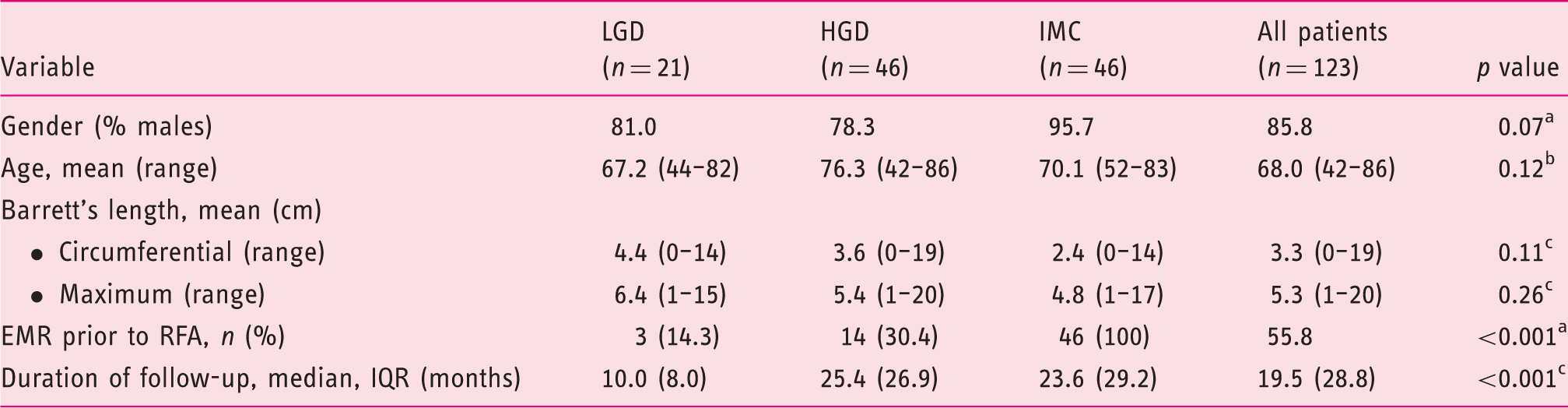
Chi-square test. bAnalysis of variance. cKruskal–Wallis test.
LGD: low-grade dysplasia; HGD: high-grade dysplasia; IMC: intramucosal cancer; EMR: endoscopic mucosal resection; RFA: radiofrequency ablation; IQR: interquartile range.
When stratified by baseline histology, patient characteristics did not differ significantly between groups. There was no significant difference in circumferential and maximum BO length between groups. Rate of prior EMR was significantly higher in the IMC group (100%) compared to HGD (30.4%) and LGD (14.3%) (p < 0.001). There was a significant difference between the number of RFAs between groups with the IMC cohort having the fewest number of ablations (p < 0.01). There was also a significant difference in the duration of follow-up between the groups with the LGD cohort having the shortest follow-up (p < 0.001).
RFA outcomes at 18 months
At 18 months, 94.7% and 78.8% of patients achieved CRD and CRIM, respectively, with a mean of 2.5 (±1.1) ablations. There were nine (8%) patients that required rescue EMR due to development of new nodular lesions after commencing RFA. Ten (8.8%) patients developed stricture following RFA and required dilation.
RFA outcomes at 18 months.
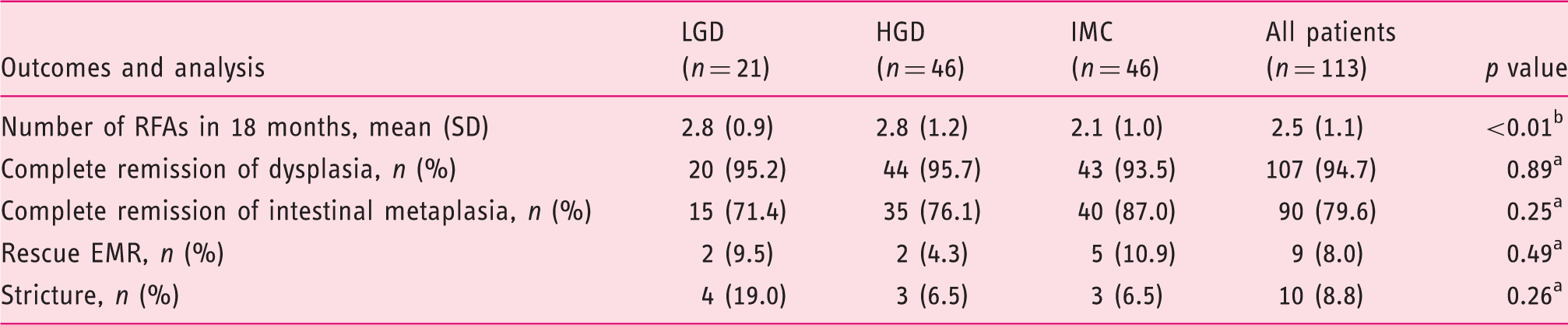
Chi-square test. bKruskal–Wallis Test.
RFA: radiofrequency ablation; LGD: low-grade dysplasia; HGD: high-grade dysplasia; IMC: intramucosal cancer; EMR: endoscopic mucosal resection.
Durability of CRD and CRIM
For patients who achieved CRD and CRIM at 18 months, Kaplan–Meier analysis was performed to assess the durability of RFA. In total, 107/113 (94.7%) patients achieved CRD at 18 months. For this analysis, any subsequent dysplasia diagnosed on follow-up after achieving CRD at 18 months was considered an event, even if subsequent RFA reinstated a CRD state. At 24 and 36 months’ follow-up, 99% and 97% of patients remained free of dysplasia, respectively. When stratified by baseline histology, there was no significant difference in the durability between the groups (log rank p = 0.31). All patients with a baseline of LGD who achieved CRD at 18 months (n = 19, 100%) remained free of dysplasia at 24 months. Similarly, all patients with IMC who achieved CRD at 18 months remained free of dysplasia at 24 and 36 months. For patients with HGD who achieved CRD at 18 months (n = 44), durability was 97.7% at 24 months, and 93.6% at 36 months (Figure 1).
Kaplan–Meier analysis of the durability of complete remission of dysplasia (CRD). All patients included in this analysis achieved CRD at 18 months (n = 107). Time 0 included in this analysis denotes the first finding of CRD within 18 months from the start of treatment. At 24 and 36 months’ follow-up, 99% and 97% of patients remained free of dysplasia, respectively (left panel). When stratified by baseline histology, durability at 24 months for the low-grade dysplasia (LGD) cohort was 100%. Durability at 24 and 36 months for the intramucosal carcinoma (IMC) cohort was 100%, respectively. Durability at 24 and 36 months for the high-grade dysplasia (HGD) cohort were 97.7 and 93.6%, respectively (right panel).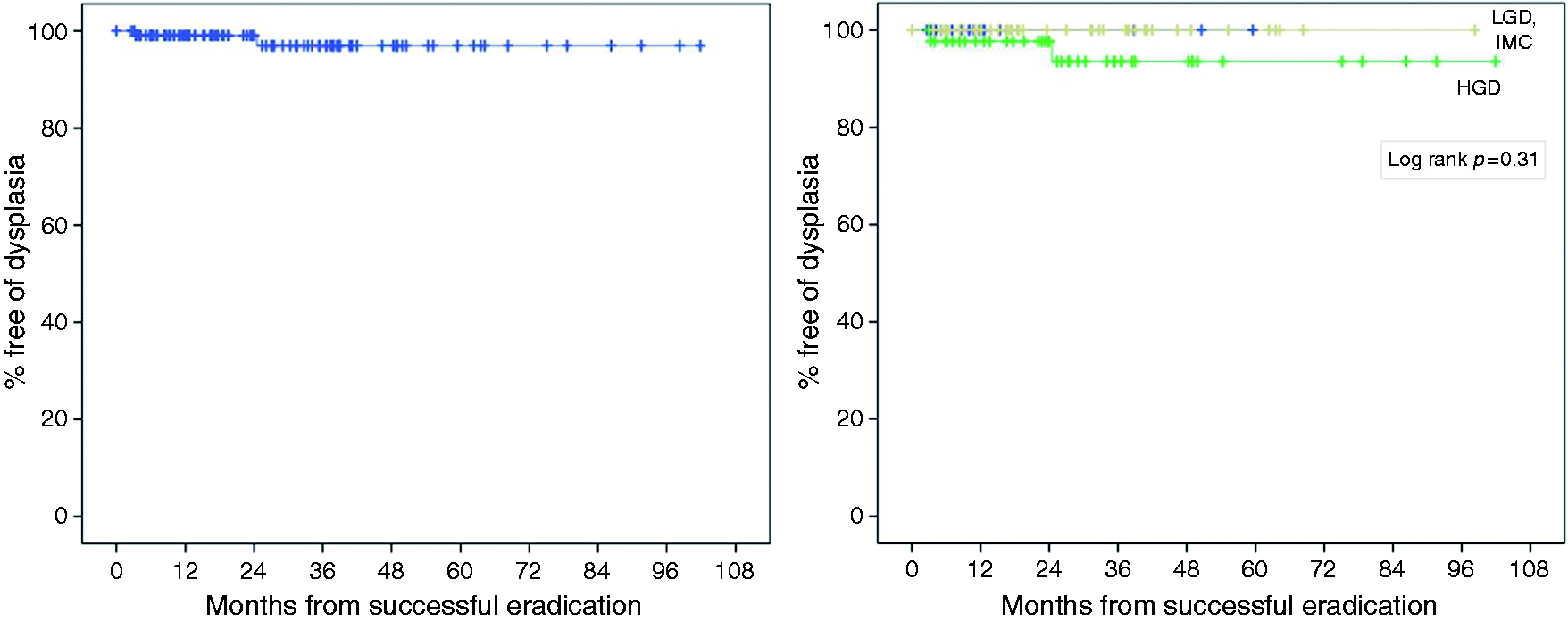
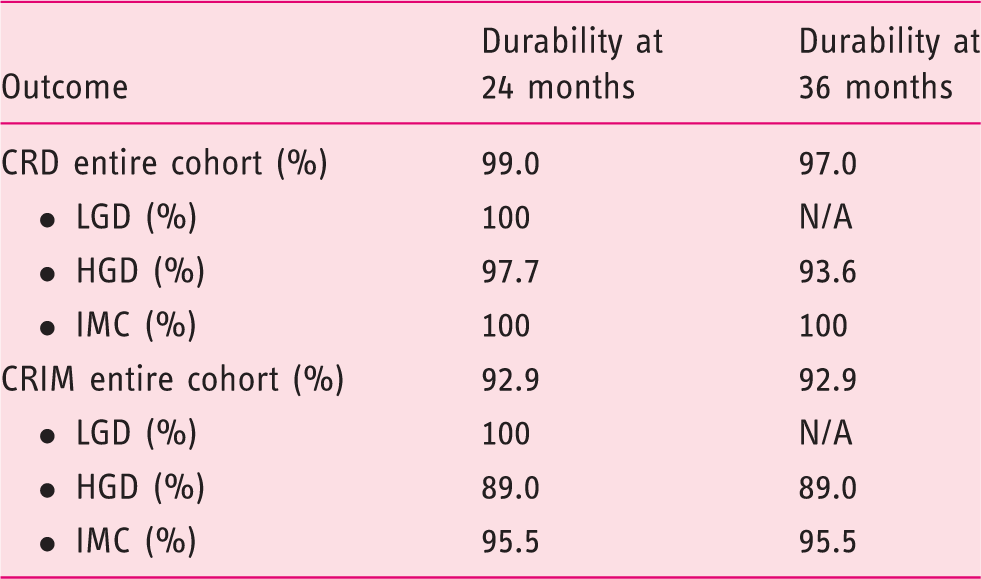
When assessing CRIM durability, 90/113 (79.6%) patients achieved CRIM at 18 months. At 24 and 36 months, 92.9% of patients remained in CRIM (Figure 2). When stratified by baseline histology, there was no significant difference in CRIM durability between groups (log rank p = 0.62). All patients (n = 15, 100%) with LGD who achieved CRIM at 18 months remained in CRIM at 24 months. For patients with HGD (n = 35), durability of CRIM was 89.0% at 24 and 36 months, respectively. For patients with IMC, 95.5% remained in CRIM at 24 and 36 months, respectively (Figure 2). Overall durability of CRD and CRIM at 24 and 36 months is summarised in Table 3.
Kaplan–Meier analysis of the durability of complete remission of intestinal metaplasia (CRIM). All patients included in this analysis achieved CRIM at 18 months (n = 90). Time 0 denotes the first finding of CRIM within 18 months from the start of treatment. At 24 and 36 months’ follow-up, 92.9% of patients remained free of dysplasia (left panel). When stratified by baseline histology, durability at 24 months for the low-grade dysplasia (LGD) cohort was 100%. For the high-grade dysplasia (HGD) and intramucosal carcinoma (IMC) cohorts, 89% and 95.5% of patients remained free of IM at 24 and 36 months, respectively (right panel). Durability of CR-D and CR-IM at two- and three-year follow-up and stratified to baseline histology. CRD: complete remission of dysplasia; CRIM: complete remission of intestinal metaplasia; LGD: low-grade dysplasia; HGD: high-grade dysplasia; IMC: intramucosal cancer; N/A: not available.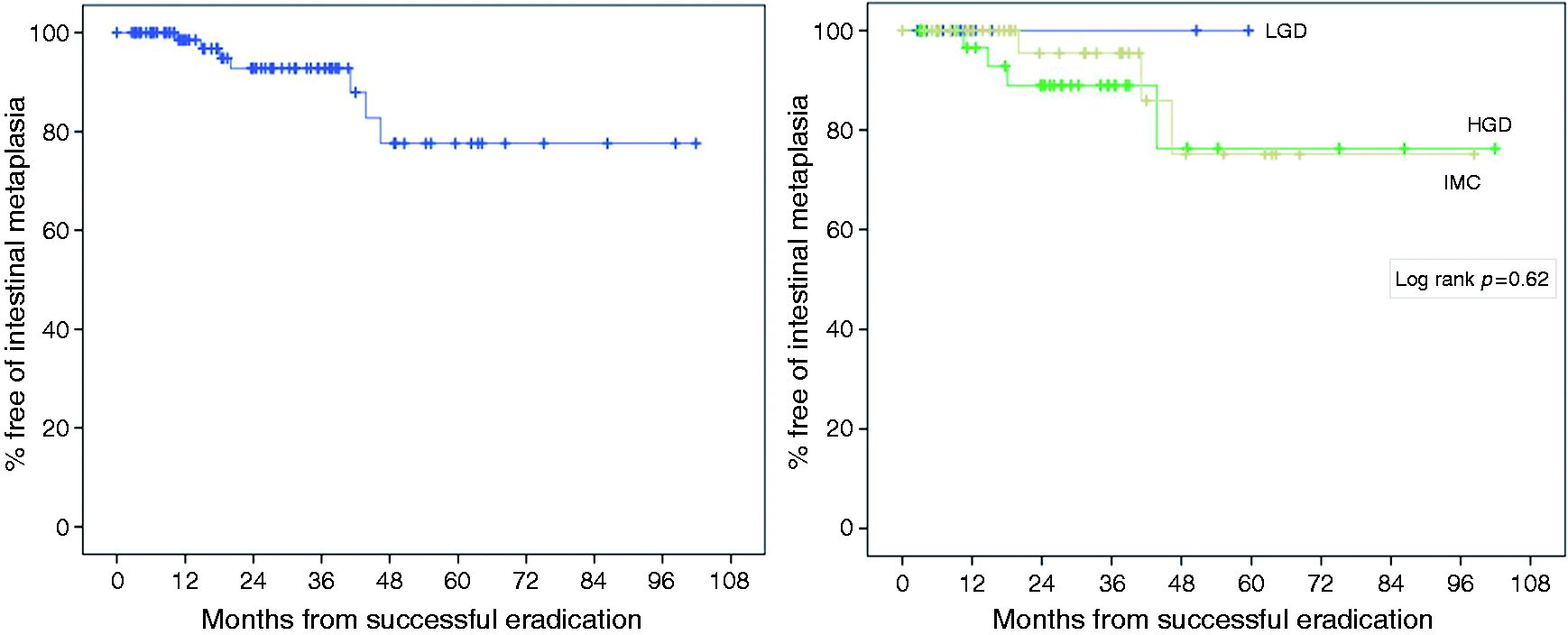
Predictor of response to ablation
We assessed age, gender, maximum length of BO, prior EMR and baseline histology as predictors of CRD and CRIM at 18 months. Multiple regression showed that only length of BO was a significant predictor of response to RFA. For every 1 cm increase in BO length, the chances of attaining CRIM decreases by 13.1% (odds ratio = 0.869, SE = 0.055; 95% confidence interval (CI): 0.780–0.968, p = 0.011). Similarly, length of BO was a poor predictor of CRD response. For every 1 cm increase in BO length, the rate of CRD decreases by 15.2% (odds ratio: 0.848, SE = 0.082; 95% CI: 0.722–0.995, p = 0.044).
Discussion
Combination therapy with RFA and EMR has been shown to be an effective therapy for dysplastic BO with an acceptable safety profile and durable response.13–15 We were able to achieve CRD and CRIM in 94.7% and 79.6% of patients with BO treated with RFA at 18 months. Our outcomes were comparable to the United Kingdom (UK) National RFA Registry, which reported 95% CRD and 83% CRIM at 12 months. 14 When IMC cases were excluded, our CRD and CRIM rates (95.5% and 74.6%, respectively) were comparable to the Ablation of Intestinal Metaplasia Containing Dysplasia (AIM-Dysplasia) RCT, which attained 86% CRD and 77% CRIM at 12 months. 16 In our study, we selected 18 months as the protocol end-point as we felt this more fairly reflects the demands and delays in endoscopic provision seen in most UK hospitals. One could argue that our patients received a longer RFA treatment protocol of 18 months and higher number of ablations, which could inflate our CRD and CRIM rate. However, the mean number of ablations in our study was 2.5, compared to 3.5 ablations in the AIM-Dysplasia study, 16 and 2.5 ablations in the UK Registry. 14 This confirms that our patients did not receive a higher number of ablations.
We also compared treatment outcomes when stratified by baseline histology. Our results showed that baseline histology was not a predictor of response to RFA. We observed similar rates of CRD in all three subgroups (95.2% in LGD, 95.7% in HGD and 93.5% in IMC, p = 0.89). Similarly, we observed high rates of CRIM among the groups (71.4% in LGD, 76.1% in HGD and 87.0% in IMC, p = 0.25). Our outcomes are consistent with the AIM-Dysplasia and UK Registry, which also showed that baseline histology was not a predictor of response to RFA.14–16 Demographic and clinico-pathological factors such as age, gender, length of BO, and prior EMR and baseline histology have previously been shown to be predictors of response to therapy. 17 However, the UK Registry recently reported their six-year outcomes on 514 patients with HGD and IMC treated with RFA and EMR, and found that these factors were not predictors of response to RFA. 18 Our results are in line with the UK Registry, although we found that longer BO length was associated with treatment failure. Our results also showed a significant difference in the number of ablations when patients were stratified by baseline histology, with the IMC cohort receiving fewest ablations compared to the LGD and HGD cohorts. This could be because all patients in our IMC group received EMR prior to RFA, which eradicated the neoplastic focus and part of the BO tissue, possibly shortening the ablation pathway. This further reinforces the need for endoscopists to meticulously screen the oesophageal mucosa for abnormal tissue or nodularity and to perform EMR on these lesions to allow for accurate histopathological diagnosis and staging.
Although RFA is an effective treatment for dysplastic BO, our data showed that it fails to eradicate dysplasia and IM in 5% and 20% of cases, respectively. This suggests that there may be other factors not relating to dysplastic grade, but likely associated to the patients’ genetic background or the genomic landscape of the disease that made their BO more resistant to RFA. Recently, there has been a surge in studies investigating genetic alteration in dysplastic BO. The mutational landscape of BO and OAC is becoming increasingly clear with evidence showing that the genetic diversity within the BO segment could be a predictor of progression. 19 Also, p53 and SMAD4 mutation has been shown to be gatekeepers for progression of BO; 20 however, whether these biomarkers can be used as predictors of response to therapy has not been thoroughly evaluated.
Durability of RFA and sustained eradication of dysplasia and IM is paramount when assessing the efficacy of ablative therapies. To date, there is still a lack of data reporting on the long-term outcomes of RFA for BO with different baseline histology. Our results showed that once CRD was achieved, this effect was durable over time with 99% of patients remaining in CRD at 24 and 36 months. We also showed that baseline histology was not a predictor of durable response (log rank p = 0.31). Our results compared favourably to the outcomes from the UK Registry, which attained 94% and 85% CRD durability at 19 and 48 months, respectively. 14 Durable response of RFA was also noted for patients who achieved CRIM, of whom 92.9% remained free of IM at 24 months. We included only the 24-month durability for LGD because RFA was approved in the UK as routine treatment for LGD only in 2015. The high level of durability in our study could be due to the strict RFA protocol we employed with at least one GOJ circumferential ablation with focal device in all patients. Further, in keeping with practice from expert centres, we did not consider focal IM at the cardia after achieving CRIM as recurrence, as this was mostly a transient finding which did not progress to endoscopic and histologic BO over time when reflux was well controlled pharmacologically.
This study has some limitations. First, it is a single centre study with small patient numbers; hence, it would be underpowered to detect small differences between groups. Second, patients who failed EMR were not included as we concentrated on RFA outcomes. Therefore, this study does not really reflect overall BO treatment response to endotherapy. Finally, the RFA protocol used changed halfway through the study period from the standard to the simplified regimen. Even though data on single treatment showed no difference in the efficacy between the two protocols, there is a lack of comparative data on these protocols and therefore it is not possible to formally exclude some degree of heterogeneity in the protocol used.
In summary, our results showed that baseline histology is not a predictor of treatment response to RFA and EMR, and that treatment response is durable over time. Thus, with careful staging and close surveillance, endoscopic therapy should continue to form the mainstay treatment for early neoplastic BO irrespective of baseline histology, with surgical resection reserved for fit patients with progressive disease or those with persistent neoplasia despite endotherapy.
Footnotes
Acknowledgement
We would like to thank Dr Philip Kaye for kindly reviewing the dysplasia diagnoses. We would also like to thank the staff of the Cambridge Clinical Research Centre for their help with patient management.
Declaration of conflicting interests
None declared.
Ethics approval
This study was performed with approval from the Joint UCL/UCLH Committees on the Ethics of Human Research (approval number 08/H0714/27118, approval date: 3 September 2008). The study protocol was conducted in accordance with the ethical guidelines of the Declaration of Helsinki.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Informed consent
Written, informed consent was obtained from each patient.