
Abstract
Background and aims
The safety and efficacy of radiofrequency ablation (RFA) in treatment of Barrett’s esophagus (BE)-associated dysplasia has been well established. The effectiveness of focal and balloon RFA devices has not been compared. Therefore, the aim of our study was to assess the effectiveness of focal and balloon RFA devices in the treatment of BE by calculating absolute and percentage change in BE length with RFA therapy by comparing pre- and post-treatment BE length.
Patients and methods
This is a retrospective cross-sectional study of patients who underwent at least one treatment with either focal and/or balloon RFA devices who were identified from two tertiary centers. Patients’ demographics, hiatal hernia, pre- and post-treatment BE length, prior use of endoscopic therapies and number of sessions were recorded.
Results
Sixty-one patients who had undergone 161 RFA treatment sessions met inclusion criteria. There was no significant difference in percentage change in BE length with greater number of RFA sessions. RFA with a focal device resulted in greater percentage reduction in BE length compared to the balloon system (73% vs. 39%, p < 0.01). After adjusting for initial BE length, pre-treatment BE length, hernia status, prior endoscopic mucosal resection (EMR), prior RFA, and prior EMR/RFA sessions, RFA with a focal device at each session remained an independent predictor for a significant reduction in BE extent as compared to the balloon system.
Conclusion
The focal RFA device alone was more effective in treatment of BE compared to the balloon system, with a greater reduction in extent of BE. The focal RFA device for endoscopic eradication therapy of BE should be considered the preferred technique.
Keywords
Background
From 1975 to 2001 there has been a six-fold increase in the number of patients diagnosed with esophageal adenocarcinoma, making its incidence one of the highest in the United States (US).1–3 Barrett’s esophagus (BE) represents a metaplastic change of the esophageal epithelium. It can progress to esophageal adenocarcinoma from low- to high-grade dysplasia. 2 The reported incidence of esophageal adenocarcinoma arising in patients with BE is 0.12% to 0.5% per year.4,5 Invasive esophageal adenocarcinoma has a very poor five-year survival rate of 19% despite treatment. 6 As such, it is important to maintain a surveillance program for those patients known to have BE and to take steps to eradicate any dysplastic change before it can progress. Endoscopic eradiation therapy is the treatment of choice to prevent dysplastic change in the setting of BE (specifically high-grade dysplasia (HGD)) from progressing to invasive cancer. 7
Radiofrequency ablation (RFA) is the best studied of the endoscopic eradication therapies for BE. 6 It has also been shown to be a safe and effective treatment modality. 8 Rates of complete eradication of intestinal metaplasia (CE-IM) using RFA in recent studies have ranged between 62% and 82%.7,9,10 Recurrence of intestinal metaplasia following ablation was noted in 9%-23% of the patients with progression to cancer in 0.7%–0.9% of patients who achieved CE-IM.7,9,10
RFA can be delivered using either a balloon with 360-degree coverage of the esophageal segment or a focal device. However, the effectiveness of each method has not yet been compared in a head-to-head fashion.
The primary aim of our study was to compare the effectiveness of RFA treatment via a focal device and balloon device in achieving ablation of BE. Secondary aims were to compare the total number of total RFA sessions of each modality required to achieve CE-IM.
Materials and methods
Patients and study design
We conducted a multicenter study (Kansas City Veterans Administration Hospital and University of Kansas Medical Center) in which patients with BE were identified from prospectively maintained endoscopy databases from September 2006 to August 2013. This study was approved by the local institutional review board.
Patient demographics (age, sex, and ethnicity), endoscopy results (presence of hiatal hernia, BE length, RFA device size, endoscopic mucosal resection (EMR)), and histologic diagnosis at each endoscopic procedure were recorded.
Inclusion criteria
One or more RFA treatments, (ii) age greater than 18, (iii) presence of endoscopic and biopsy-proven BE of equal to or greater than 1 cm.
Endoscopy
Standard white light endoscopy was used to initially inspect BE, and Prague criteria were used to describe the BE extent. 11 Four-quadrant biopsies were obtained from each patient as necessary, following the Seattle protocol. 12 All visible flat or nodular lesions were resected by EMR. Eight weeks after initial EMR, the residual BE was eradicated using RFA.
The BE segment is initially sprayed with a mucolytic agent via a spray catheter. Two devices were used to deliver RFA, including balloon (Halo360 catheter) and focal (Halo90 catheter) devices. The Halo360 catheter uses a 3 cm cylindrical balloon with a circular electrode to deliver a preset energy and ablate the area in a circular fashion. The inner esophageal diameter is assessed with a sizing balloon and a suitable balloon size is chosen. The balloon catheter is then introduced to ablate the BE with a preset energy (12 j/cm2) in a circumferential fashion, starting from the proximal esophagus and moving distally with a small overlap of 1 cm between ablation zones. Two ablations are performed per site with fulgurated tissue removed between sessions. The Halo90 catheter is attached at the end of the endoscope and thus allows direct visualization while delivering energy for ablation, although the area ablated with each delivery is much smaller than that of the Halo360. After the focal catheter is affixed to the end of the endoscope, Barrett’s segments were ablated from the distal to proximal esophagus with a preset energy (12 j/cm2). Patients received a twice-daily dose of proton pump inhibitors between the treatment sessions.
RFA was performed to treat patients with HGD and intramucosal cancer, and low-grade dysplasia (LGD), per current practice guidelines. 13 Repeated ablations (every two to four months in patients with HGD/intramucosal cancer or every six to 12 months in patients with LGD) were performed to treat residual BE after EMR was performed to treat cancer (in those with cancer). All histology specimens were reviewed and confirmed by a single pathologist.
CE-IM was defined as no visible columnar-lined epithelium and biopsies of neo-squamous mucosa revealing no IM in the surveillance endoscopy immediately following remission. Biopsies taken during this follow-up endoscopy were obtained in four-quadrant fashion every 2 cm of previously documented BE.
No patient included in this study had received prior RFA therapy. For the purpose of this study we included all RFA treatments that the patient received to help control for possible confounding variables (including pre-treatment BE length and cumulative effect of multiple RFA treatment sessions that may have been conducted using a combination of balloon and focal devices). We then analyzed these patients using both a patient-based and endoscopy-based analysis along with creation of multivariate logistic regression models.
Statistical analysis
Absolute and percentage change in BE length with RFA therapy was calculated by comparing pre-treatment BE length with BE length recorded on the next subsequent endoscopy performed after RFA. Categorical variables were compared with Fisher’s exact test. Normally distributed continuous variables were compared with unpaired t-test and non-normally distributed continuous variables were compared with Wilcoxon rank sum test. Multivariate regression analysis was conducted and models were adjusted for hiatal hernia, pre-treatment BE length, prior EMR, prior RFA, and total number of prior EMR/RFA sessions.
Results
In our study, 61 patients who had undergone a total of 161 RFA treatment sessions met the inclusion criteria. Sixty of these were males with a mean age of 68.8 years. The mean initial BE length was Prague C 3.1 cm (SD 3.7 cm) and M 5.0 cm (SD 3.6 cm). Five patients had intra-mucosal cancer (8.2%), 38 HGD (62.3%), and 18 LGD (29.5%).
Endoscopy-based analysis
Of 161 RFA sessions, 50 were performed using the Halo360 balloon and 111 using the focal Halo90 device. RFA sessions conducted with the focal device were less likely to have been performed when hiatal hernia was present (86.4% vs. 100%, p < 0.01). The focal device was more likely to be used when the patient had received prior RFA therapy (71.9% vs. 40.0%, p < 0.01) and when shorter BE lengths were present (mean 1.7 cm vs. 6.5 cm, p < 0.01). RFA with the focal device resulted in a greater percentage reduction in BE length compared to the balloon system (73% vs. 39%, p < 0.01) (Figure 1 Treatment flowchart.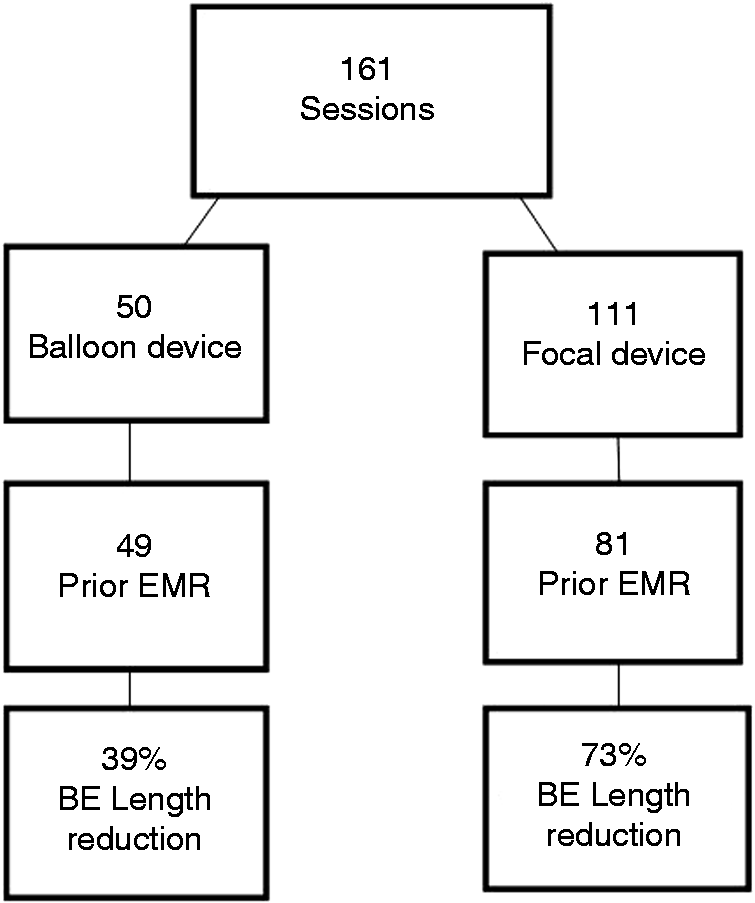
Patient-based analysis
Thirty-one patients received RFA therapy only with the focal device, and 30 received RFA therapy with the balloon device ± additional focal device sessions. Fifty-four of 61 patients who received RFA had complete eradication of BE.
Baseline characteristics of RFA patients
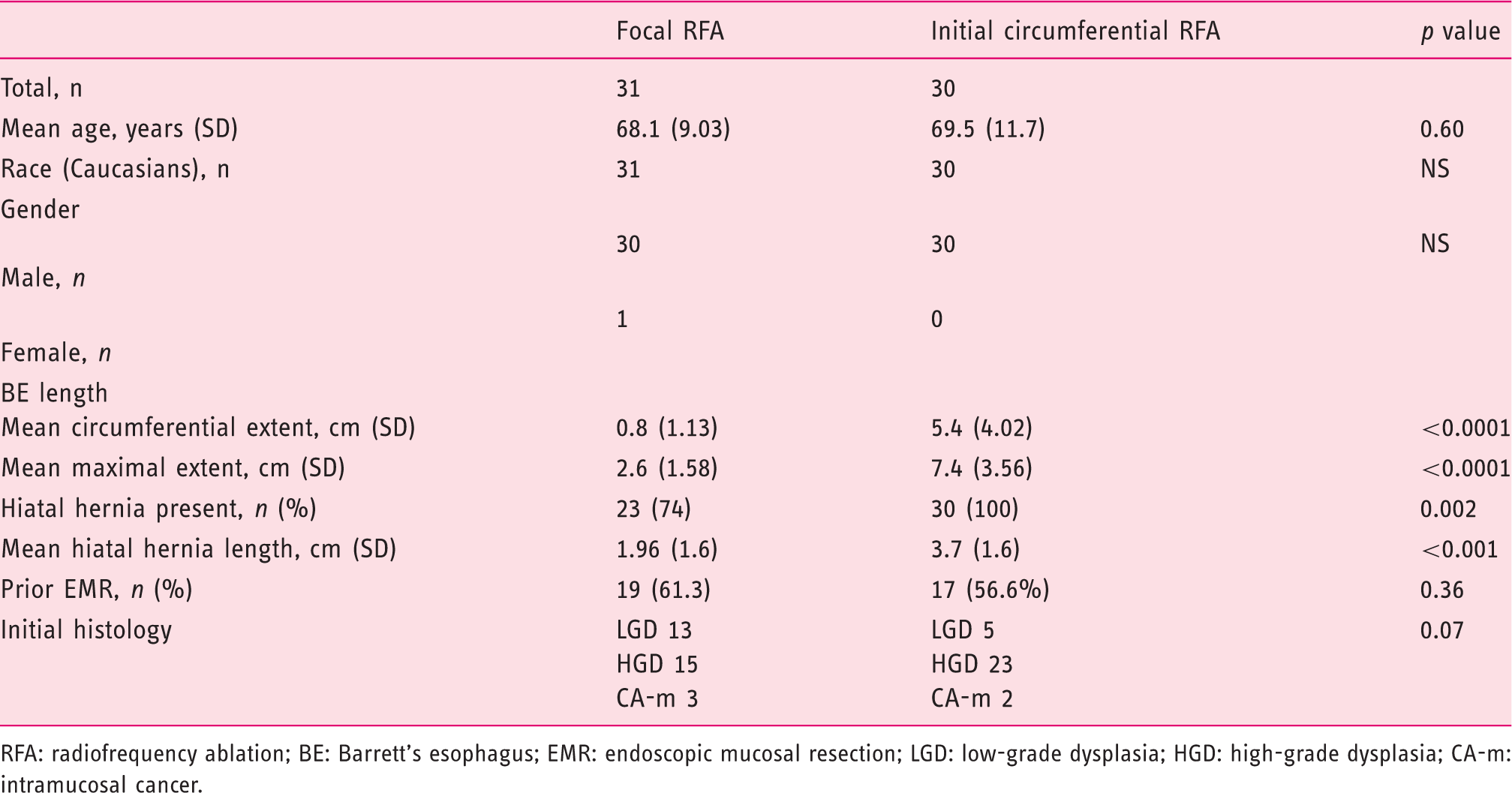
RFA: radiofrequency ablation; BE: Barrett’s esophagus; EMR: endoscopic mucosal resection; LGD: low-grade dysplasia; HGD: high-grade dysplasia; CA-m: intramucosal cancer.
Initial RFA treatment with the focal device led to an 82% reduction in BE length compared to 47% with the balloon device (p < 0.01). The focal device led to an absolute reduction of BE length by 1.3 cm. Those who underwent RFA with the focal device only required fewer RFA sessions to achieve CE-IM (mean 1.6 vs. 3.8 sessions, p < 0.01). After adjusting for pre-treatment BE length, presence of hernia, and prior EMR, RFA with focal device only remained an independent predictor for requiring fewer total RFA sessions to achieve CE-IM (B coefficient –1.6; 95% CI, 0.7–2.6). The stricture rates in this cohort were low. Only one patient in the balloon RFA group had esophageal stricture while none of the patients in the focal RFA group had a stricture.
There was no significant difference in the percentage change in BE length with a greater number of RFA sessions (62% for first session, 56% for second session, 61% for third session, and 70% for fourth session).
Discussion
There has been a shift toward endoscopic eradication therapy of BE in the last decade. A meta-analysis in 2008 suggested that the risk of HGD progressing to cancer was 6% per year if not treated by endoscopic eradication therapy. 14 Following this, a randomized control trial showed that RFA was superior to sham procedure in preventing the progression of BE to cancer. 15 In a recently conducted randomized control trial, RFA was shown to significantly decrease the rates of progression of LGD to both HGD (26.5% for endoscopic surveillance alone vs. 1.5% for ablation) and esophageal cancer (8.8% for endoscopic surveillance alone vs. 1.5% for ablation). Owing to the significant superiority of RFA compared to endoscopic surveillance alone in decreasing progression of LGD to either HGD or esophageal cancer and concern for patient safety if the trial continued, the study was terminated earlier than expected. 16 Similarly, a few other recently published studies have shown that RFA is effective in eradicating dysplasia.17,18 The above data proved beyond a doubt that RFA has a significant role in treating BE and dysplasia.
Currently, we use a balloon device for circumferential ablation of BE and a focal device for focal ablation of BE. However, with the growing body of literature, a pertinent question remains: Could we improve our performance by using one particular device?
Our study addresses this particular issue. It shows that a focal RFA device is more effective in treatment of BE compared to the balloon device, despite the extent of BE involvement in the esophagus. The focal device both significantly reduces the length of BE and requires fewer treatment sessions.
After adjusting for initial BE length, hernia status, prior EMR, prior RFA, and prior EMR/RFA sessions, RFA delivered by a focal device at each session remained an independent predictor for a significant reduction in BE extent when compared to a balloon system. The focal device achieved 36% greater reduction and 1.1 cm less BE. The focal device required 2.2 fewer sessions to achieve CE-IM when compared to the balloon device. Our hypothesis is that the reason for effective eradication by focal device is because it directly targets the residual BE thereby giving better results in achieving CE-IM. In comparison, good device contact with Barrett’s mucosa is vital to its successful ablation using a circumferential balloon device. Moreover, sizing the circumferential balloon is difficult and varies with operator experience and therefore circumferential ablation zones created by the balloon device can result in under-treatment requiring more treatment sessions and lesser efficacy in achieving CE-IM due to wider area of the device. Furthermore, focal RFA may also provide better treatment of BE at the neo-gastroesophageal junction, where residual neoplasm and recurrences occur.
This study represents the first comparison of effectiveness between the focal and balloon RFA catheters for the treatment of BE. Given the need to prevent progression to esophageal adenocarcinoma, it is essential to determine the most effective therapy to achieve eradication of dysplastic BE in the fewest number of treatment sessions. This study will serve as a guide for future investigations involving RFA in the eradication of BE.
Limitations of this study include its retrospective nature as well as the potential for overestimation of the effectiveness of the focal device based on its use on smaller areas of BE. However, our findings were adjusted for initial BE length, hernia status, prior EMR, prior RFA, and prior EMR/RFA sessions in an attempt to correct for overestimation.
In conclusion, our study suggests the focal RFA catheter is superior to the balloon catheter in achieving BE eradication independent of BE length. Therefore, the focal device should be considered over the balloon RFA in treating patients with BE. Additional investigation through randomized controlled trials is warranted for head-to-head comparison of the efficacy of focal vs. balloon devices in the treatment of BE.
Footnotes
Author contributions
Jesica Brown: acquisition of data; study concept and design; interpretation of the data; drafting the manuscript; technical or material support.
Benjamin Alsop: critical revision of the manuscript for important intellectual content.
Neil Gupta: Study concept and design; acquisition of data; statistical analysis; critical revision of the manuscript for important intellectual content.
Daniel Buckles: interpretation of data, critical revision of the manuscript for important intellectual content.
Mojtaba Olyaee: interpretation of data, critical revision of the manuscript for important intellectual content.
Prashanth Vennalaganti: critical revision of the manuscript for important intellectual content; technical or material support.
Vijay Naag Kanakadandi: critical revision of the manuscript for important intellectual content; technical or material support.
Shreyas Saligram: critical revision of the manuscript for important intellectual content.
Prateek Sharma: study concept and design; acquisition of data; interpretation of data; drafting the manuscript, critical revision of the manuscript for important intellectual content; technical, or material support; study supervision.
Acknowledgment
This study was presented as part of The Barrett’s Esophagus Research Forum during Digestive Diseases Week 2014, Chicago, IL, USA.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.