
Abstract
Background
Accurate risk evaluation of choledocholithiasis prior to laparoscopic cholecystectomy is essential to determine optimal management strategy.
Objective
Our study aimed to evaluate the accuracy of separate predictors and Vilnius University Hospital Index (VUHI = A/30 + 0.4 × B; A = total bilirubin concentration (µmol/l), B = common bile duct (CBD) diameter (mm) measured by ultrasound) diagnosing choledocholithiasis and to assess different management strategies (cholecystectomy with intraoperative cholangiography and endoscopic retrograde cholangiopancreatography (ERCP)).
Methods
The retrospective study included 350 patients admitted to a tertiary care centre for laparoscopic cholecystectomy for cholecystolithiasis who were investigated for concomitant choledocholithiasis.
Results
Choledocholithiasis was diagnosed in 182 (76.2%) cases in the high-risk group (VUHI value ≥4.7) and 44 (39.6%) in the low, odds ratio is 4.86 (95% CI: 3.00–7.88). Its sensitivity was 80.5%, specificity 54.0%, accuracy 71.1%. Dilated CBD had the highest sensitivity (92.5%) of predictors.
ERCP showed better diagnostic performance than intraoperative cholangiography. Complications of ERCP were more frequent for patients without stones. There was no significant difference of outcomes between the two management strategies.
Conclusion
The prognostic index has good diagnostic accuracy but dividing patients into two risk groups is insufficient. The suggested model allows determining an intermediate-risk group, which requires additional investigation. Both management approaches are appropriate.
Keywords
Key summary
Common bile duct (CBD) obstruction by stones in case of cholecystolithiasis can lead to some serious outcomes; use of endoscopic retrograde cholangiopancreatography (ERCP) for diagnostic means should be minimised as the procedure itself carries a certain risk of complications; in the study centre an original prognostic index is being used for prediction of choledocholithiasis; a value of the index indicating high risk (>50%) of choledocholithiasis showed 80.5% sensitivity, 54% specificity and 71.1% accuracy; new thresholds for low, intermediate and high risk of choledocholithiasis are established; additional non-invasive CBD investigation for the intermediate risk group is proposed; no significant differences between two management strategies – ERCP before laparoscopic cholecystectomy and intraoperative cholangiography plus ERCP on demand – were observed.
Introduction
Choledocholithiasis is a common complication of cholecystolithiasis occurring for 10–18% of people undergoing cholecystectomy. 1 Common bile duct (CBD) obstruction by stones can lead to acute biliary pancreatitis, mechanical jaundice, acute ascending cholangitis and even to fatal outcomes. Diagnosis of choledocholithiasis depends on a combination of biochemical tests and imaging studies’ findings. There is no clear consensus on the best therapeutic approach – surgical or endoscopic management of choledocholithiasis. 2 Use of endoscopic retrograde cholangiopancreatography (ERCP) as a diagnostic tool should be minimised as it carries considerable risk (5–10%) of post-procedural complications: acute pancreatitis (1.3–6.7%), bleeding (0.7–2%), acute cholangitis (0.5–5%), duodenal perforation (0.3–1%).3,4 It is noticed that adverse events occur more often in patients with low risk of choledocholithiasis. 4 Therefore the best possible patient selection for ERCP procedure is needed.
At the Centre of Abdominal Surgery of Vilnius University Hospital Santariskiu Klinikos, an original prognostic index (Vilnius University Hospital Index (VUH Index or VUHI)) has been used for evaluation of risk of choledocholithiasis since 1999. 5 It is calculated by the formula VUHI = A/30 + 0.4 × B, where A = total bilirubin concentration (µmol/l), B = CBD diameter measured with ultrasound (US). When the value of the VUHI is equal to or higher than 4.7, the risk for choledocholithiasis is considered high and VUHI up to 4.7 is associated with low risk of choledocholithiasis. Considering diagnostic possibilities two decades ago, ERCP before laparoscopic cholecystectomy (LC) was the management of choice for high-risk patients and intraoperative cholangiography (IOC) was performed for the low-risk group.6,7 Currently non-invasive investigation methods (magnetic resonance cholangiography, endoscopic ultrasonography (EUS)) enable us to reduce unnecessary invasive examinations proportionally. So, revision of prognostic VUHI potential is essential in establishing the best diagnostic algorithm of choledocholithiasis.
The aims of our study were to evaluate the accuracy of separate predictors and the prognostic index, diagnosing choledocholithiasis for patients with gallbladder stones before LC, and to determine thresholds of VUHI values for intermediate choledocholithiasis risk, i.e. distinguish patients who would benefit from additional investigation. In addition, we aimed to assess safety and outcomes of different management strategies.
Patients and methods
The study consisted of patients admitted to the tertiary care centre Vilnius University Hospital Santariskiu Klinikos from January 2012 through December 2015 for LC for cholecystolithiasis for whom concomitant choledocholithiasis was suspected by clinical, radiological or biochemical findings. To identify study participants, we reviewed all the case records in our institution’s reporting database from this four-year period which included keywords ‘laparoscopic cholecystectomy’ in the operation protocol. Patients who underwent investigations for suspected choledocholithiasis (ERCP or IOC) were included. Exclusion criteria were: age under 18 years; surgically altered anatomy (Billroth II, Roux-en-y anastomosis, gastric bypass); a history of biliary surgery or stenting; suspected or known hepatopancreatobiliary malignancy; other known liver or biliary disease.
ERCP procedures were performed by experienced endoscopists (each had more than five years of experience in ERCP and more than 500 procedures completed) with Olympus side-viewing endoscopes TJF-160VR using standard technique.
All patients underwent a standard four-port LC. IOC was performed after distal clipping of the cystic duct that was incised and cannulated with a cholangiography catheter. A contrast material was injected gradually to visualise the lower end of the CBD and observe flow into the duodenum and then to outline the intrahepatic ducts. Cholangiograms were assessed by the operating surgeon and radiologist.
The following data were collected for each eligible participant: sex; age at the time of admission; duration from admission to intervention (IOC or ERCP) in days; total bilirubin concentration; CBD diameter and stones if seen on ultrasound (US), computed tomography (CT) or magnetic resonance cholangiopancreatography (MRCP); diagnosed acute cholecystitis, acute ascending cholangitis or acute biliary pancreatitis prior to ERCP; value of VUHI; physical status assessment according to the American Society of Anesthesiologists (ASA) classification; which investigation method of bile ducts was chosen first (ERCP or IOC), its results and outcome; type of cholecystectomy; adverse events of ERCP and their management; surgical complications (Clavien-Dindo classification); ERCP performed after cholecystectomy and its results; length of hospital stay. Jaundice was stated at a total bilirubin level of 34 µmol/l and higher. 8 Diagnosis of acute biliary pancreatitis was acknowledged when stated in medical records or when lipase or amylase activity was at least three times higher than the upper limit of normal. Diagnosis of acute cholangitis was declared when stated in medical records. Diagnosis of acute cholecystitis was declared when suspected by clinical findings and confirmed histologically. CBD stone (CBDS) was considered detected when it was found and removed during ERCP, IOC or choledochotomy. CBDS at cholangiography (IOC or ERCP) was suspected when there was a filling defect seen on radiogram or delayed passage of contrast material into the duodenum was observed.
Statistical analysis was performed using SPSS version 17.0 (SPSS, Chicago, IL, USA) and statistical software R. Quantitative data were described as mean ± standard deviation (SD) and qualitative data as proportions. Independent-samples T-test was used to compare quantitative variables and chi-square test was used to compare categorical variables. Odds ratio (OR) was used to evaluate predictors. Two-sided hypotheses were checked and a p value <0.05 was considered statistically significant. For risk predictors and risk groups statistical measures of the performance of a binary classification test (sensitivity, specificity, positive predictive value, negative predictive value and accuracy) were assessed. A receiver operating characteristic (ROC) curve was evaluated to measure diagnostic accuracy. The relationship between VUHI and presence of S was selected using the analysis of variance (ANOVA) method and defined by logistic regression model.
This study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki and was approved by the Vilnius Regional Research Ethics Committee, certificate date 13 December 2016, number 158200-16-870-395. Written, informed consent for procedures was obtained from each patient included in the study.
Results
Patient characteristics and differences between patients with and without CBDS
During the study period 2313 patients had a cholecystectomy performed at our institution. Among them 350 patients (63.4% female, mean age 65.2 years, SD 17.89) underwent the aforementioned investigations for suspected choledocholithiasis and were eligible for the study.
Characteristics of patients with and without CBDS.
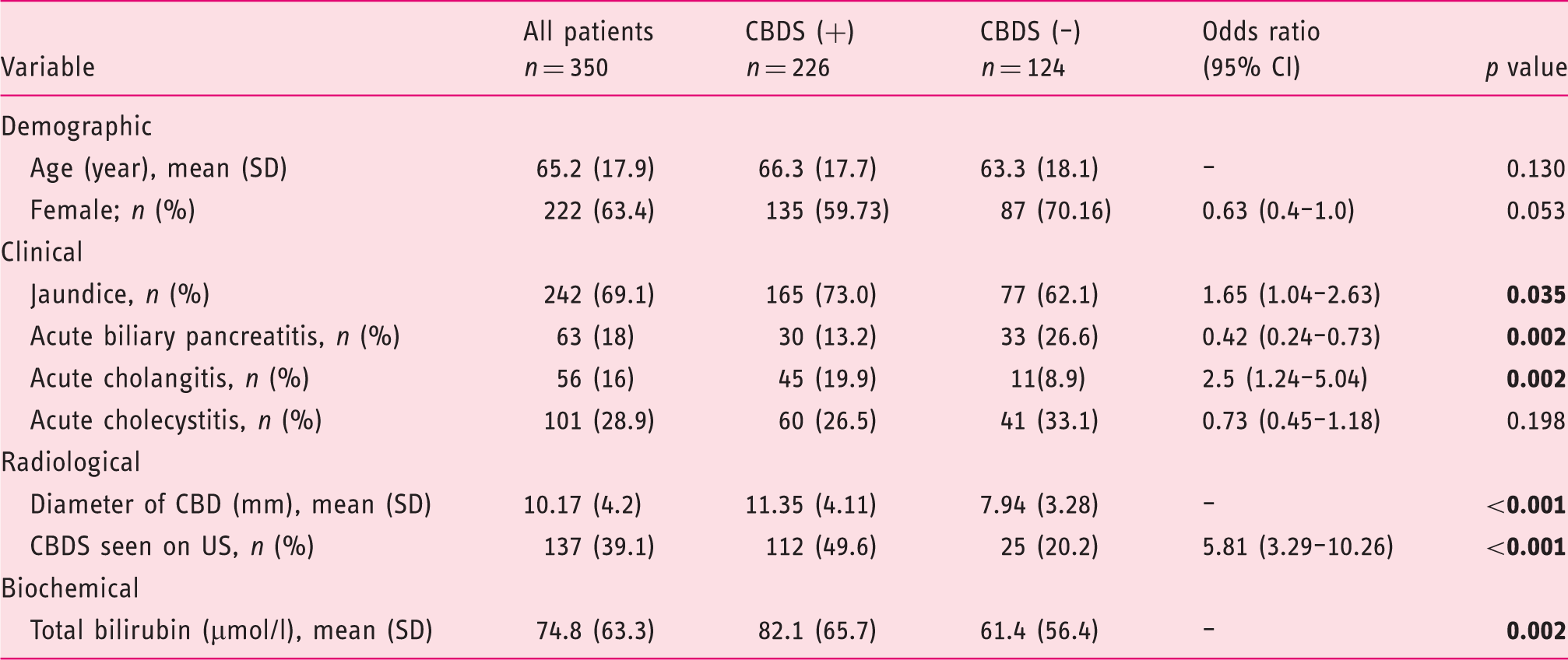
CBDs: common bile duct stones; US: ultrasound; CI: confidence interval; SD: standard deviation. Statistically significant values are typed in bold.
Patients’ age and sex distribution did not differ significantly statistically. Patients in the stone-positive group had significantly higher total bilirubin concentration and CBD diameter, more cases of acute cholangitis (19.9% vs. 8.9%) but fewer cases of acute biliary pancreatitis (13.2% vs. 26.6%) as compared with the stone-negative group.
A total of 111 (31.71%) patients were classified as having a lower risk for choledocholithiasis (VUHI <4.7) and 239 (68.29%) patients were assigned to a higher-risk group (VUHI ≥4.7).
Predictors of choledocholithiasis
Performance characteristics of separate predictors: elevated bilirubin concentration, dilated CBD (diameter >6 mm) and CBDS seen or suspected by US were evaluated. In the stone-positive group, bilirubin was elevated above the upper limit of normal value in 189 cases (83.6% of patients with CBDS), dilated CBD was found in 209 cases (92.5%) and CBDS on US were seen in 112 cases (49.6%). In the stone-negative group, concentration of bilirubin was abnormal in 94 cases (75.8% of patients without CBDS), CBD was dilated in 84 cases (67.7%) and CBDS on US were seen or suspected in 18 cases (14.5% of US performed).
Prognostic values of different CBDS predictors and VUHI.
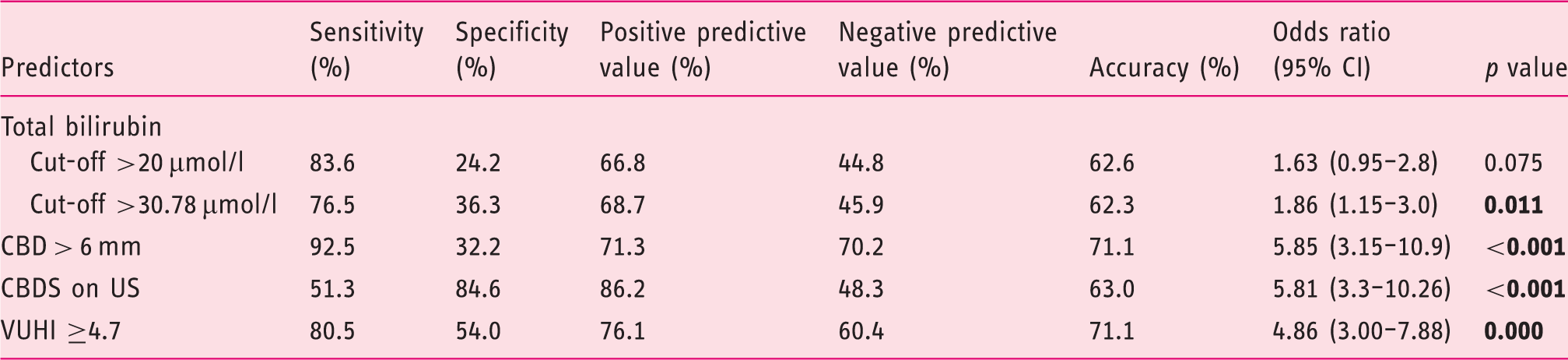
CBDS: common bile duct stones; VUHI: Vilnius University Hospital Index; US: ultrasound; CI: confidence interval. Statistically significant values are typed in bold.
Evaluation of VUHI
The area under the ROC curve for VUHI was 0.742. VUHI ≥4.7 was found to be associated with more than a four-fold greater risk of having CBDS than VUHI <4.7 (OR 4.86) (Table 2). When counting CBDS on US as an additional factor for the higher-risk group (‘VUHI ≥4.7 or CBDS on US’) OR and performance rates improved, except specificity (OR 7.07). Additionally we included benign CBD strictures (n = 14) as a positive outcome presuming these patients would also benefit from ERCP. This modification raised the OR to 6.09 and overall accuracy to 74.0%.
In the higher-risk group ERCP was scheduled for 205 patients, and no pathology was detected (i.e. ERCP was performed unnecessarily) in 20 (9.76%) cases.
Distribution of detected CBDS according to VUHI value intervals is shown in Figure 1.
Proportion of CBD stones detected at different VUHI intervals. VUHI: Vilnius University Hospital Index.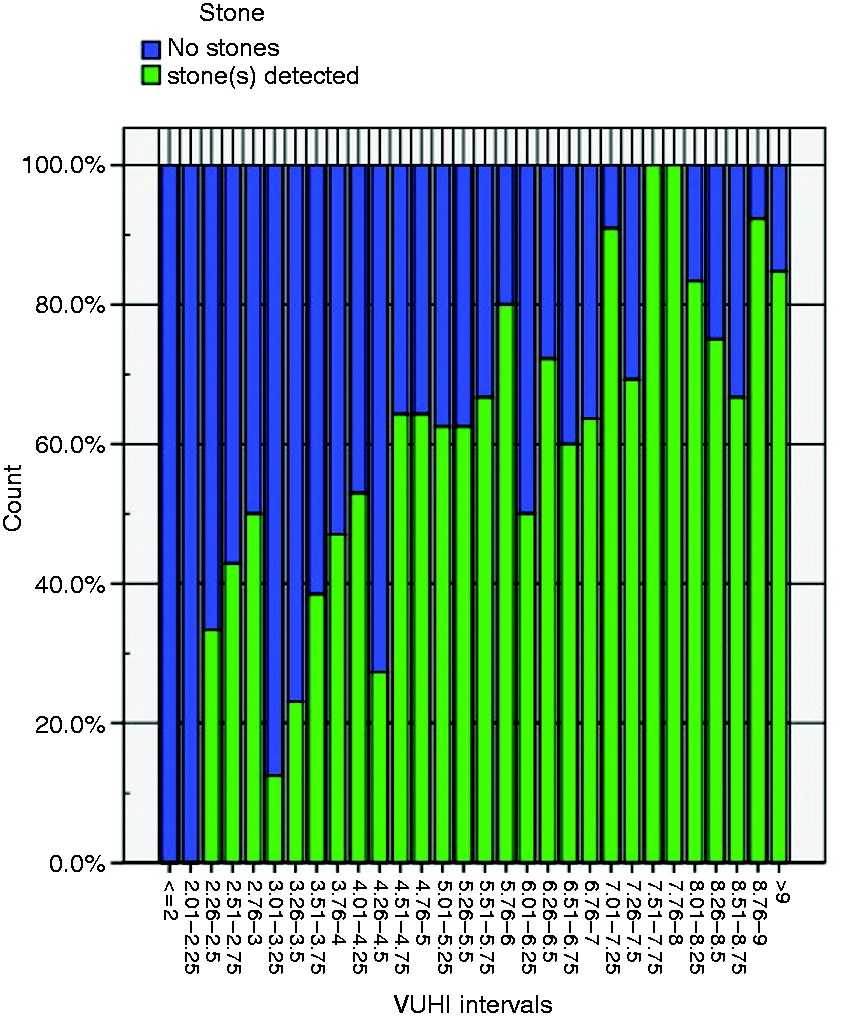
The relationship between VUHI and presence of S was defined by the logistic regression model

The predicted probability (πi) of finding an S while having a certain value of VUHI is obtained by the formula

Relation of predicted probability for CBDS and VUHI value is shown in Figure 2.
Probability of CBD stones depending on VUHI. VUHI: Vilnius University Hospital Index.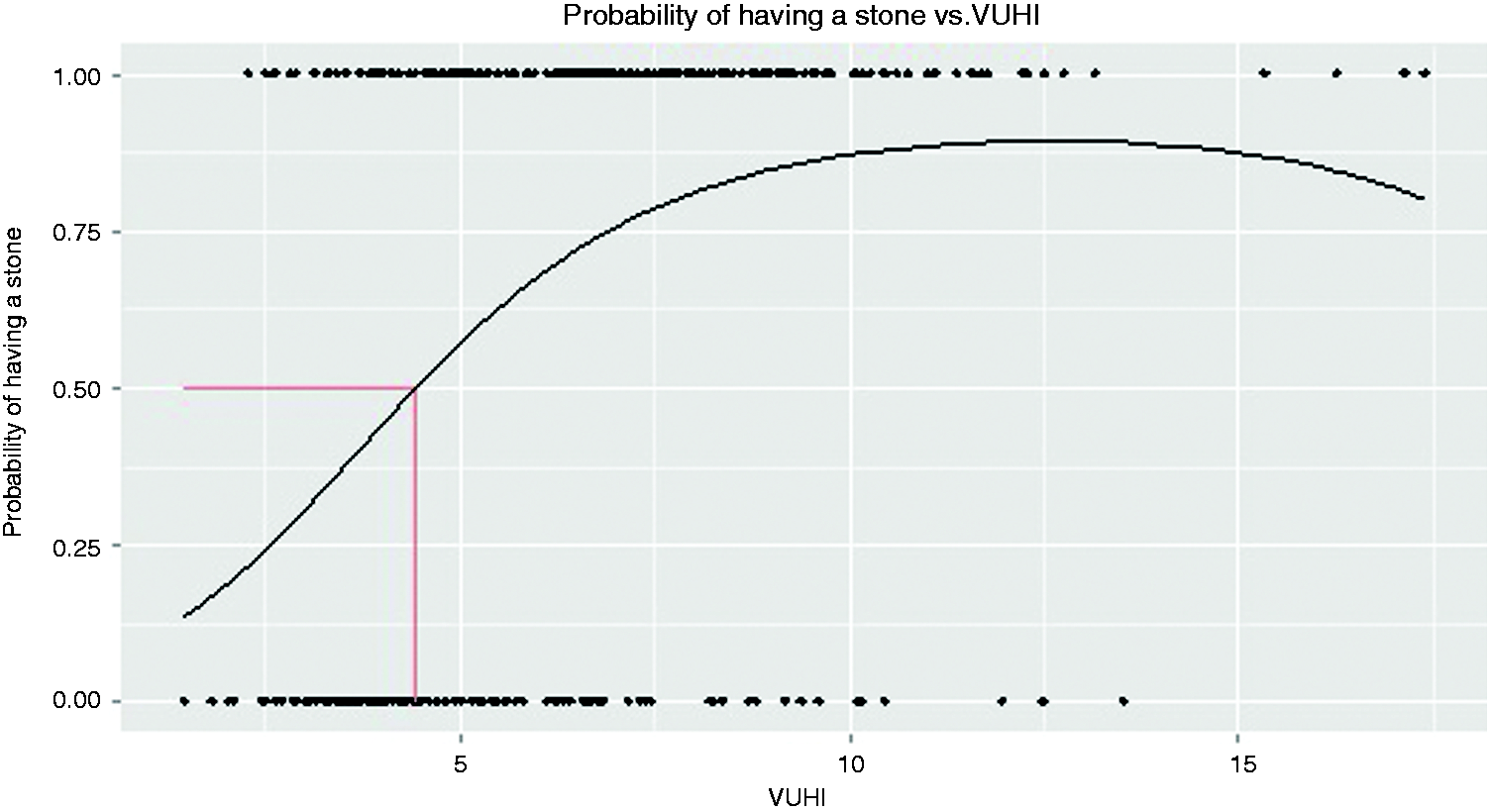
Applying this equation, 50% probability of detecting stones would be at a VUHI value 4.42. The currently used value of 4.7 gives 53.6% probability.
Comparison of different management approaches
Comparison of different management approach groups.
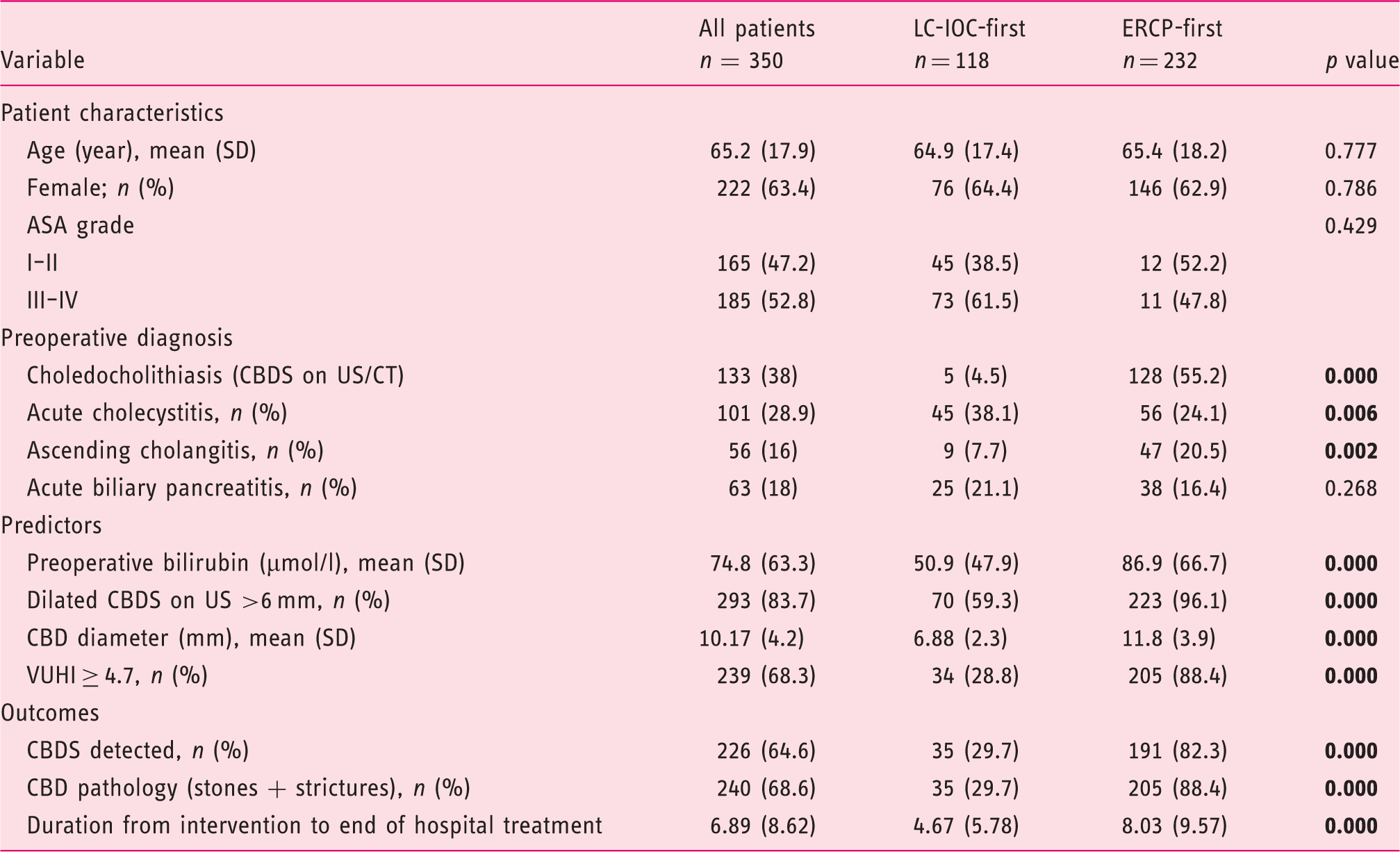
LC-IOC: laparoscopic cholecystectomy with intraoperative cholangiography; ERCP: endoscopic retrograde cholangiopancreatography; ASA: American Society of Anesthesiologists; VUHI: Vilnius University Hospital Index; CBDS: common bile duct stones; US: ultrasound; CT: computed tomography; CI: confidence interval; SD: standard deviation. Statistically significant values are typed in bold.
For higher-risk patients (VUHI ≥4.7) the ERCP-first strategy was chosen in 205 cases and LC-IOC-first strategy in 34 cases. For patients with lower risk for choledocholithiasis (VUHI <4.7) LC-IOC as the first intervention was chosen in 84 cases and ERCP-first strategy in 27 cases, mostly when CBDS were seen on US/CT or other signs of possible choledocholithiasis were present (e.g. intrahepatic cholestasis).
Patients’ age, sex, physical status according to ASA grade and waiting time for the first intervention did not differ significantly between the different strategy groups. Duration from admission to the hospital to first intervention was less than two days (mean 1.34 days, 1.43 in the LC-IOC-first group and 1.29 in the ERCP-first group, p = 0.538). Values of separate predictors and VUHI were higher for ERCP-first patients. Acute cholecystitis was more frequent for the LC-IOC-first group, as a likely indication for urgent LC. Duration of hospital stay, both total and post-procedural, was longer in the ERCP-first group.
No significant differences were found for ERCP success rates and percentage of applied interventions between both groups. ERCP was successful at the first attempt for 93% of all patients (90.3% in LC-IOC-first, 93.3% in ERCP-first). Endoscopic treatment was unsuccessful for four (1.5%) patients; all of them belonged to the ERCP-first group. The complication rate was higher in the ERCP-first strategy group (14 vs. 1).
Results of diagnosing and managing CBDS and treatment outcomes in different strategy groups.
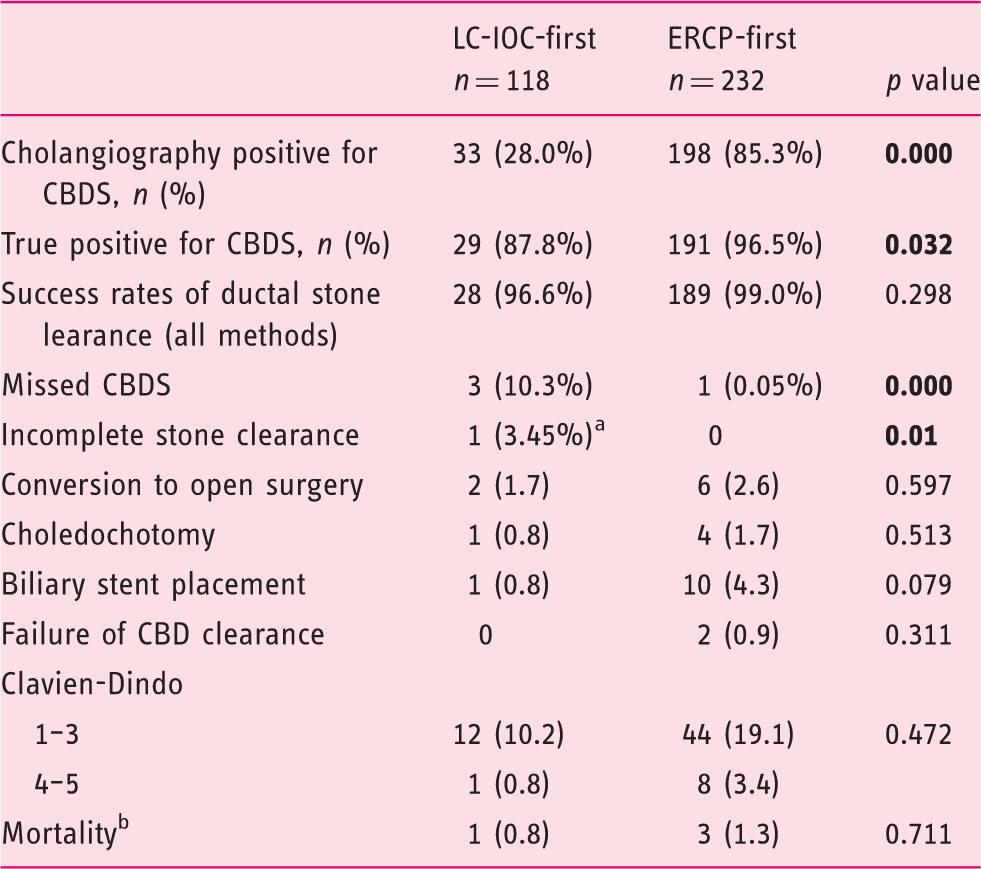
Endoscopic plastic stent insertion followed by postoperative ERCP after two days (n = 1).
Fatal outcomes were due to poor physical status, septic course of the disease and exacerbation of chronic illnesses. No deaths were caused by complications of surgical or endoscopic treatment.
CBDS: common bile duct stones; LC-IOC: laparoscopic cholecystectomy with intraoperative cholangiography; ERCP: endoscopic retrograde cholangiopancreatography. Statistically significant values are typed in bold.
Complications of interventions to CBD
ERCP-related complications occurred in 15 cases; the overall complication rate for 262 patients who underwent ERCP was 5.7%, being 4.5% (10 out of 221) in the stone-positive group and 12.2% (5 out of 41) in the stone-negative group, p = 0.052. The most common adverse event for all patients was post-ERCP pancreatitis (nine cases (4.1%), six in the stone-positive group, three in the stone-negative group) and this was followed by bleeding from the sphincterotomy site (three cases (1.4%)), perforation (two cases (0.9%)) and post-ERCP pancreatitis plus bleeding (one case (0.5%)). All complications were treated conservatively or endoscopically; no surgical treatment was necessary.
There were no complications of IOC reported.
Discussion
Risk assessment of choledocholithiasis for patients with symptomatic cholelithiasis tends to remain a topic of intensive debates recently. As a former gold standard for the diagnosis of CBDS, ERCP has a certain risk of complications, and it is important to distinguish which patients will benefit from ERCP as a therapeutic procedure as well, i.e. what features determine high risk for having concomitant CBDS.
We retrospectively evaluated the prognostic value of the choledocholithiasis index used in our institution. There were 76.2% of patients in the higher-risk category and 39.6% of patients in the lower-risk category who had CBDS, which gives a good sensitivity but unsatisfactory specificity. Analysis of separate constituents of VUHI (bilirubin concentration and US findings) showed them to be significant predictors of choledocholithiasis although elevation of bilirubin was significantly different for patients with and without CBDS just at a level of 30.78 µmol/l. Nevertheless, concentration of bilirubin makes up a distinctly lesser proportion in VUHI and the value of 20 µmol/l gives just 0.67 elevation of the index value. Our results are parallel with previous studies in which dilated CBD and/or hyperechoic shadows in it seen by US are the strongest predictors of choledocholithiasis.3,10–12 The diagnostic value of bilirubin is inconsistent in different studies: It has been found to be of highest specificity and accuracy among five biochemical parameters by Yang et al., 13 although other authors denied its significance.12,14
Clinical gallstone pancreatitis is ranked as a moderate predictor for choledocholithiasis. 15 We found a negative association between biliary pancreatitis and risk for choledocholithiasis (OR = 0.42). Other authors also noticed that biliary pancreatitis is not associated with choledocholithiasis or can even be treated as a protective factor.2,16,17 This supports a hypothesis that biliary pancreatitis is associated with small CBDS size, and a spontaneous passage of such stones is more frequent. 2
Although both non-invasive methods – MRCP and EUS – are available in our institution, we were not able to assess their effectiveness as MRCP was applied in just five cases and EUS was not performed at all for our cohort of patients.
Diagnostic performance of ASGE guidelines.
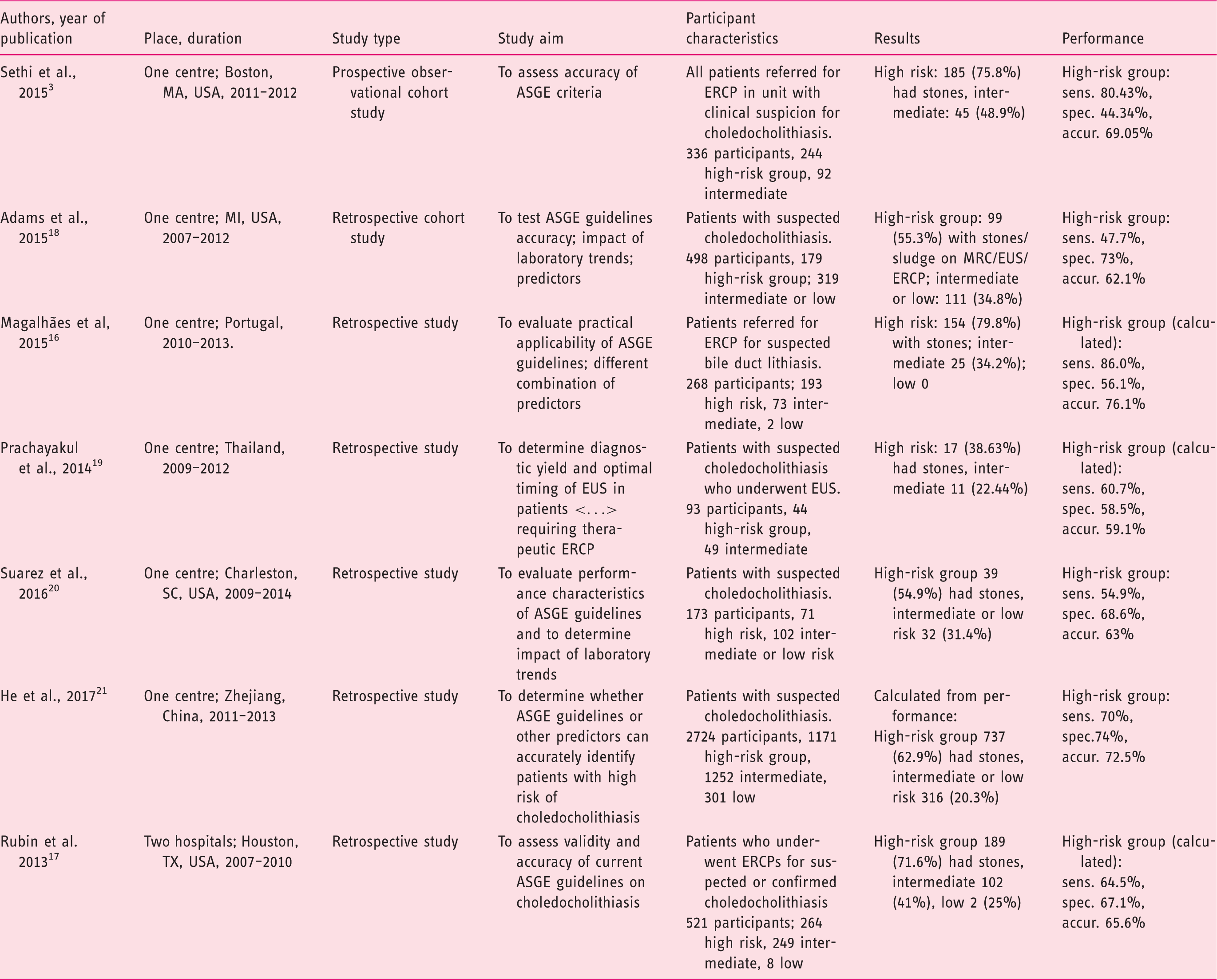
ASGE: American Society for Gastrointestinal Endoscopy; ERCP: endoscopic retrograde cholangiopancreatography; sens.: sensitivity; spec.: specificity; accur.: accuracy; EUS: endoscopic ultrasonography; MRC: magnetic resonance cholangiography; USA: United States of America.
Our prognostic score shows comparable and, at some parameters, superior performance for predicting choledocholithiasis. The poorest measure here is specificity. This implies that the currently used threshold of VUHI is kind of a weak spot in this evaluation system. Our generated model for predicted probability of choledocholithiasis allows setting limits for an intermediate-risk group, i.e. determining which patients should undergo additional non-interventional investigation. The latest European Association for the Study of the Liver (EASL) guidelines state that patients with intermediate probability should undergo further evaluation with EUS or MRCP but do not define what this intermediate probability is. 22
If we presume that the intermediate risk covers probability for CBDS from 25% to 75%, this corresponds to VUHI values of 2.54 to 6.88. In our study we had 202 such patients and CBDS were found for 105 (52.0%) of them. So, every other patient in this group would benefit from additional biliary imaging. In the potential low-risk group (VUHI <2.54) we had just nine patients, two (22.2%) of them had CBDS, both not larger than 5 mm. Respectively, in the presumed high-risk group (VUHI >6.88) we had 139 patients and 85.6% had choledocholithiasis.
Evaluating effectiveness of different management approaches, we found some advantages in both strategies: There were fewer missed stones and false-positive cholangiographies in the ERCP-first group, meanwhile the LC-IOC group had fewer ERCP-related complications. Mean length of hospital stay was approximately two days longer for the ERCP-first group, which in most cases reflected the waiting period for the LC. Meta-analyses of various different trials also show that there is no significant difference in the efficacy, mortality, morbidity, retained stones, and failure rates between single-stage and two-stage choledocholithiasis management.1,23,24 The main drawback of the preoperative ERCP strategy against various single-session approaches (intraoperative ERCP, LC with laparoscopic bile duct clearance, open bile duct clearance) is the time: Usually the waiting period between the two procedures prolongs duration of hospital stay and slightly increases the risk to develop recurrent biliary events and cholecystitis.22,25,26 Additionally, one of the biggest limitations to single-session ERCP and LC is difficult coordination of medical personnel, equipment and location of procedure.27,28 Despite these restraints a large survey of general surgeons in the United States showed that the majority of respondents preferred ERCP to laparoscopic CBD exploration for the management of choledocholithiasis. 29
The most frequent adverse event of ERCP was post-ERCP pancreatitis. Its incidence is comparable to that observed in a systematic survey of 21 studies (3.47%). 30 Among various established risk factors for this complication normal bilirubin level and non-dilated biliary ducts take an important place.31,32 This is compatible with our data that post-ERCP pancreatitis occurred more frequently in the low-risk group – for patients with less dilated CBD and lower bilirubin. Although complication count is too small to significantly confirm these findings, the tendency is seen.
There are some certain limitations of our study. The major limitation is its retrospective nature, which restricted evaluating clinical symptoms, as well as some other predictors, e.g. liver function tests other than bilirubin, because of lacking data. Also, timing from primary work-up to CBD exploration was not standardised as longer waiting duration can determine some spontaneously passed stones. We excluded patients with known or suspected hepatopancreatobiliary malignancy or other diseases; therefore, this model could be best applied before planned LC for relatively healthy patients.
In conclusion, the present study showed that our prognostic index has adequate diagnostic accuracy but dividing patients into two risk groups is insufficient in contemporary clinical practice. The suggested model allows determining an intermediate-risk group, which requires additional investigation. As no clinically significant differences between two management strategies were found, both approaches are suitable.
Footnotes
Declaration of conflicting interests
None declared.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
This study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki and was approved by the Vilnius Regional Research Ethics Committee, certificate date 13 December 2016, number 158200-16-870-395.
Informed consent
Written, informed consent for procedures was obtained from each patient included in the study.