
Abstract
Background and aims
Muscle cramps markedly affect the quality of life in cirrhotic patients with no available highly effective treatment. The aim of this study was to assess the safety and efficacy of orphenadrine in the treatment of muscle cramps in cirrhotic patients.
Methods
The study enrolled 30 liver cirrhosis patients complaining of frequent muscle cramps (≥3 per week), who were randomized to receive either orphenadrine 100 mg or calcium carbonate 500 mg twice daily as a control for one month. Severity, frequency, and duration of the muscle cramps were assessed before and after treatment as well as recurrence after washout of the drug for two weeks. Side effects were recorded.
Results
One month after treatment with orphenadrine; the frequency of muscle cramps decreased significantly to 0.6 ± 0.74 per week compared to 12.53 ± 6.01 at baseline (p < 0.001), the duration of muscle cramps decreased from 1 min to 0.1 min after treatment (p < 0.001). The pain score improved significantly from a score of 8/10 to 0/10 (p < 0.001). The side effects were few, such as dry mouth, drowsiness, and nausea, with no significant difference between their occurrences in the two groups.
Conclusion
Orphenadrine is safe and effective in treatment of muscle cramps in patients with liver cirrhosis.
Introduction
Muscle cramps affect many aspects of quality of life in cirrhotic patients including sleep, physical functioning and mobility, general health, mental health, energy levels, and social isolation with no available highly effective treatment.1–4
However, despite the obvious association of muscle cramps with liver disease, there is a paucity of information regarding pathogenesis and treatment in these patients. 5 Until now the mechanism of muscle cramp occurrence in cirrhosis has remained unclear. Alterations in nerve function, energy metabolism, electrolytes, and plasma volume have been considered. 6
There appear to be a number of promising treatments for muscle cramps in cirrhosis. Several agents including vitamin E, human albumin, zinc, taurine, eperisone hydrochloride, and branched-chain amino acids targeting the postulated mechanisms have been used to treat these cramps and have shown some benefit in small uncontrolled studies, although large randomized controlled trials are lacking. 2
Orphenadrine is an anti-cholinergic drug that has been used to treat painful muscle spasms due to its potent central nervous system (CNS) and peripheral actions. 7 The combination of anticholinergic effects and CNS penetration make orphenadrine useful for pain of all etiologies, including pain from radiculopathy, muscles, and headaches. 8
Orphenadrine is structurally related to diphenhydramine and carries relatively stronger anticholinergic and weaker sedative properties, it is mostly excreted through the kidneys. 9 Therefore, its suitability for evaluation in the treatment of muscle cramps occurring with liver cirrhosis seems to be logical.
The aim of the study was to assess the efficacy and safety of orphenadrine in the treatment of muscle cramps in patients with liver cirrhosis.
Patients and methods
Study design and patients
This was a randomized, controlled, four-week, double-blind, parallel-group, pilot study conducted in Egypt. A total of 47 cirrhotic patients with muscle cramps were screened for participation in this study. The patients had been admitted at the Department of Tropical Medicine and Infectious diseases in Tanta University Hospital from January 2015–June 2015. Of these, 30 patients with post-hepatitis C liver cirrhosis with muscle cramps were enrolled and randomly assigned to receive either orphenadrine or calcium carbonate as a control group for one month. The rationale for utilizing calcium carbonate was that it is a safe and inexpensive drug commonly prescribed for treatment of muscle cramps in Egypt. We believed it unethical to perform a placebo-based trial in this category of patients. The included patients were randomized using a computerized random number generator to select randomly permuted blocks with a block size of four and an equal allocation ratio. Sequentially numbered, opaque, sealed envelopes were used to ensure concealment. WA and RB recruited and enrolled participants. An independent observer assigned participants to a computer-generated randomization sequence. Both investigators and patients were blinded to the treatment administered. The appearance, packaging, and labeling of the orphenadrine and calcium tablets were identical.
Patients were randomized into two groups: Group I: 15 patients receiving orphenadrine 100 mg twice daily for one month and Group II: 15 patients receiving calcium carbonate 500 mg twice daily for one month.
Inclusion criteria included patients with liver cirrhosis and frequent muscle cramps (≥3 cramps/week) for at least a month before entry to the study. Liver cirrhosis was diagnosed on the basis of clinical and laboratory findings as well as abdomino-pelvic ultrasound.
Patients with allergy to orphenadrine, renal impairment, peripheral vascular disease, peripheral neuropathy, glaucoma, prostatic enlargement, pregnancy, lactation, and patients taking calcium-channel blockers, conjugated estrogens and naproxen were excluded from the study.
All participants were advised not to take any vitamin E, taurine, carnitine, narcotic pain medications, muscle relaxants, Non steroidal anti-inflammatory drugs, or anti-spastic agents during, and for a two weeks following, the study. None of the participants had poorly controlled diabetes mellitus.
Institutional ethical committee approval was obtained before the start of the study and informed consent was signed by every patient before enrolment in the study; the study was registered on clinicaltrials.gov (ClinicalTrials.gov Identifier: NCT02423395). The study was approved in 2015 by the Ethics Committee of the Faculty of Medicine, Tanta University (code approval number: 30128/03/31). The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in prior approval by the institution's Human Research Committee. All authors had access to the study data, and reviewed and approved the final manuscript.
Assessments
Baseline evaluation included clinical, radiological, and laboratory testing. Also, assessment of muscle cramps with a questionnaire to analyze the character, location, intensity (using 1–10 analog scale), duration (in minutes) and frequency of muscle cramps (times/week). The cramp questionnaire we used was a modification of the questionnaire proposed by Chatrath et al., 2014, 6 that could be filled in over the telephone on patient follow-up.
All patients were followed weekly during the period of treatment and up till two weeks after the end of therapy. Patients' contact numbers were taken and they were called weekly and asked about the frequency, duration, and severity of muscle cramps and any side effects of treatment during the previous week.
Outcomes
The primary outcome of the trial was the difference in the number of muscle cramps between the orphenadrine and calcium groups at the end of four weeks of treatment. Secondary outcomes were the severity, duration of cramps, and side effects at the end of the study, and the numbers of days till the patients reported a start in relief of muscle cramps.
Statistical analysis
The statistical data are reported as the mean ± standard deviation (SD), median (interquartile range), frequencies (number) and percentages when appropriate. A comparison of numerical variables between the study groups was performed using Student’s t-test to compare independent samples from two groups when the samples were normally distributed and the Mann–Whitney U-test was used to compare independent samples when the samples were not normally distributed. Paired t-test used to compare paired samples from two groups when the samples were normally distributed and Wilcoxon sign-rank test when the samples were not normally distributed. To compare categorical data, chi square test or Fisher’s exact test were performed. Values of p less than 0.05 (two-tailed) were considered statistically significant. Outcome measures were analyzed using paired t-test, Wilcoxon sign-rank test, Mann–Whitney U-test, and Fisher’s exact test.
All statistical calculations were performed using the computer program SPSS (Statistical Package for the Social Science; SPSS, Chicago, Illinois, USA) version15 for Microsoft Windows.
Results
In total, 47 patients were screened for study participation out of whom 17 were excluded from the study; of these, 11 failed to fulfill the inclusion criteria, and six declined to participate. Thus, 30 patients were randomized to receive either orphenadrine or calcium carbonate as a control group for one month (Figure 1). The baseline characteristics of patients of the studied groups are summarized in Table 1.
Study flow chart. Patient baseline characteristics.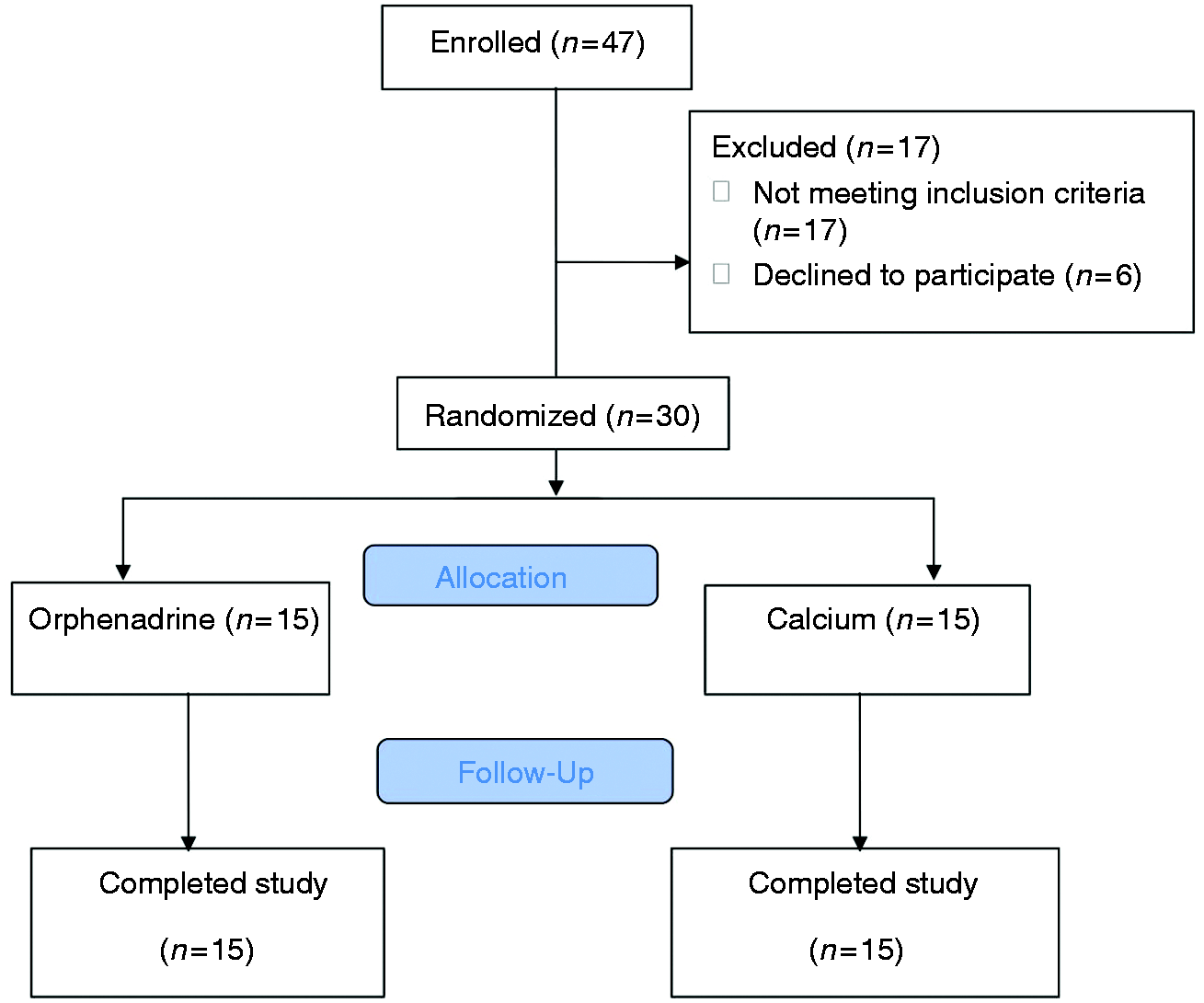
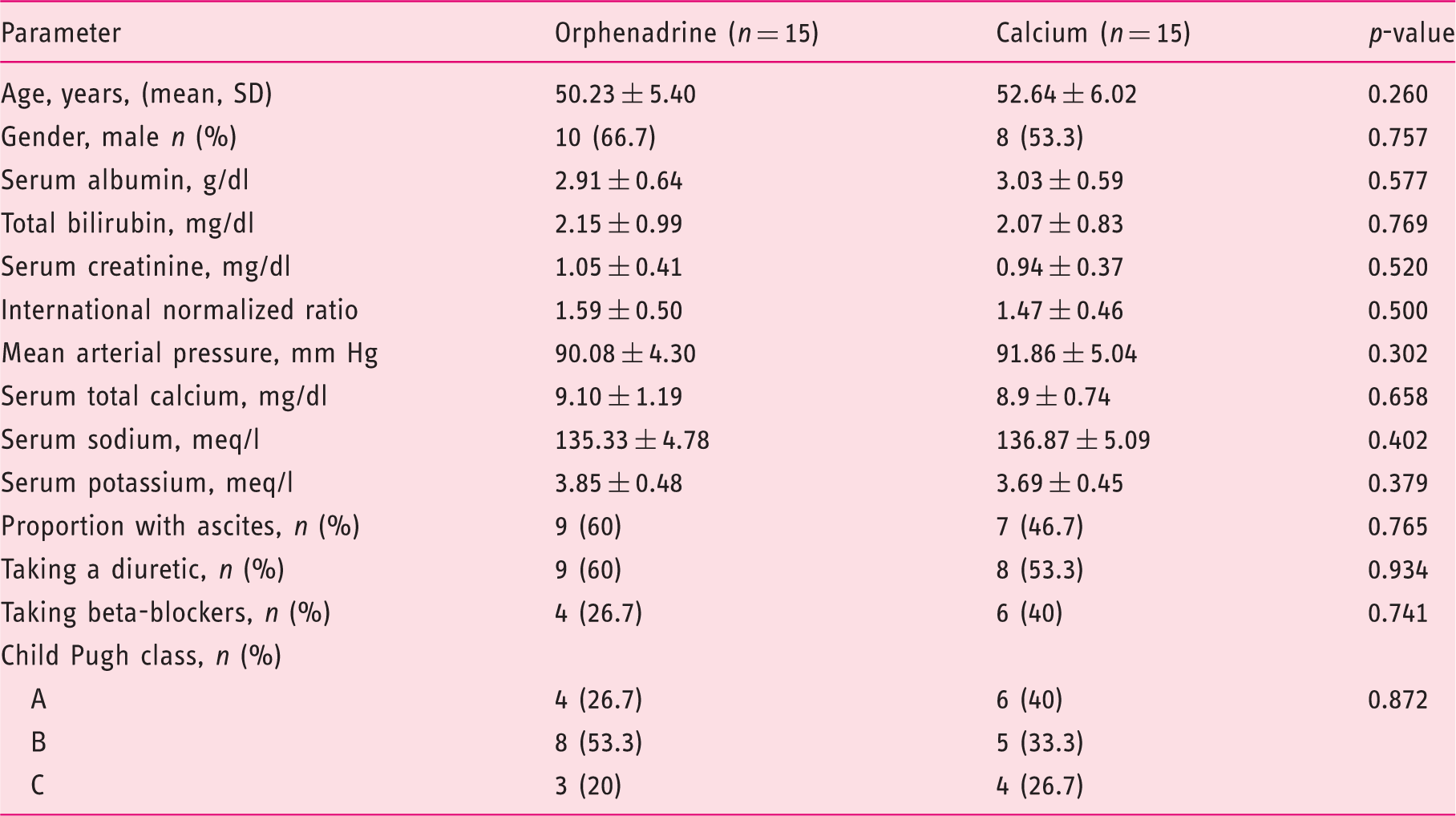
Patient groups were similar with regard to demographic characteristics; in particular, there were no statistically significant differences between the two treatment groups with respect to baseline diuretic use (60% vs 53.3%), serum sodium (135.33 ± 4.78 meq/l vs 136.87 ± 5.09 meq/l) and serum potassium (3.85 ± 0.48 meq/l vs 3.69 ± 0.45meq/l) (p > 0.05) (Table 1).
Baseline muscle cramps questionnaire in the studied groups.
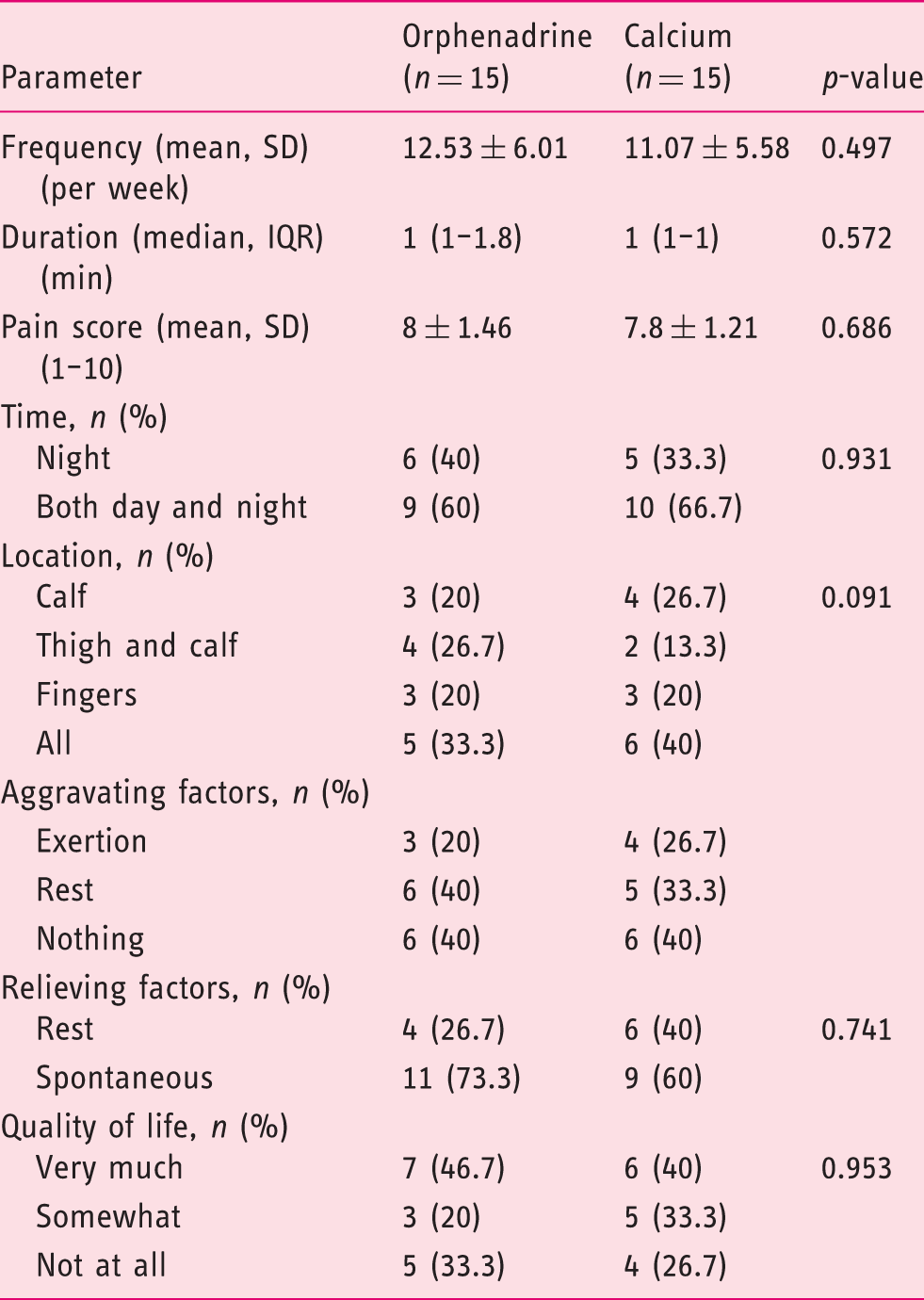
IQR: interquartile range; SD: standard deviation.
Muscle cramps frequency, duration, and severity in the orphenadrine and calcium group at baseline and after one month of treatment.
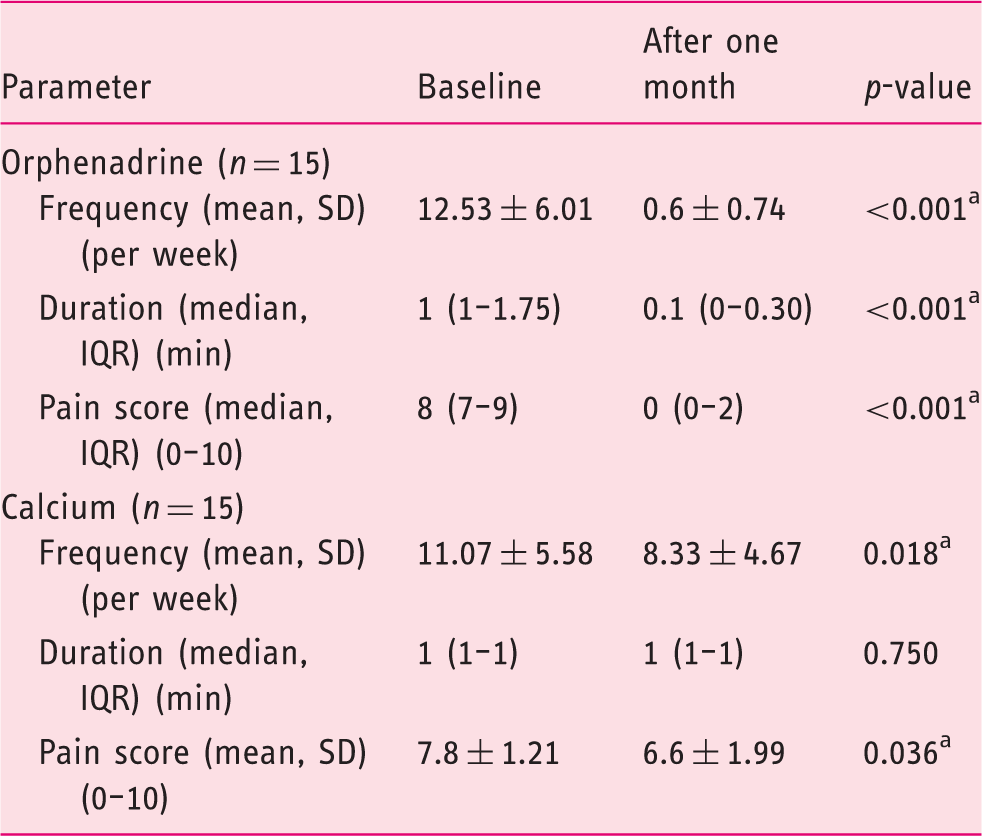
IQR: interquartile range; SD: standard deviation. ap-value < 0.05.
The orphenadrine group on a dose of 100 mg twice daily for one month showed a significant decrease in the mean number of muscle cramps, pain intensity, and muscle cramp duration compared to baseline (p < 0.001).
In the calcium group, on a dose of 500 mg/day calcium carbonate, the mean number of muscle cramps significantly decreased from 11.07 ± 5.58 at baseline to 8.33 ± 4.67 per week after treatment (p = 0.018) and the severity of pain of muscle cramps decreased significantly from a mean score of 7.8 ± 1.21 at baseline to 6.6 ± 1.99 after treatment (p = 0.036).There was no significant change in the duration of muscle cramps following treatment with calcium (p = 0.750) (Table 3).
Muscle cramps frequency and severity in the orphenadrine and calcium group after one month of treatment and two weeks after withdrawal of treatment.
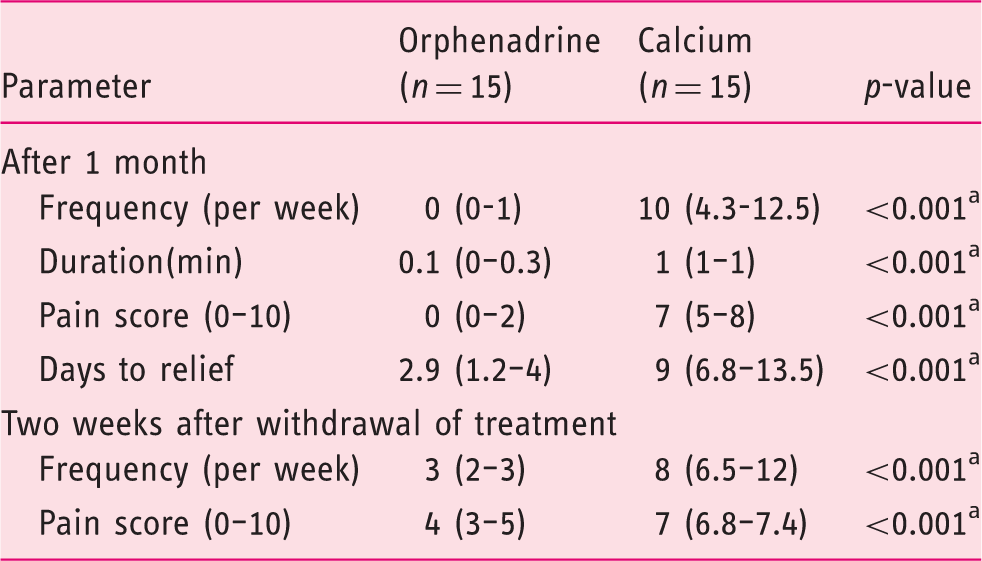
Data are presented as median (interquartile range). ap-value < 0.05.
Following a two-week period for washout of the two treatments; the orphenadrine group had significantly less cramps (three versus eight per week) (p < 0.001) and a lower pain score than the calcium group (4/10 versus 7/10) (p < 0.001) as shown in Table 4.
The regimen was well-tolerated by all the patients enrolled in the study. In the orphenadrine group, nine (60%) patients had no side effects, four (26.67%) patients had dry mouth, one (6.67%) patient had nausea, and one (6.67%) patient had some drowsiness. In the calcium group, 12 (80%) patients had no side effects and three patients (20%) had nausea. No serious adverse events were reported. None of our patients experienced hepatic encephalopathy during the study period. In our study, one elderly patient with Child A cirrhosis experienced drowsiness, but tolerated the lower dose (100 mg once daily) without any side effects.
There was no significant difference in side effects, dry mouth, drowsiness, and nausea (p = 1.00) between the orphenadrine and the calcium group.
Discussion
Although muscle cramps are benign in nature, their occurrence in cirrhotic patients is associated with pain and decreased physical and social functioning. 10 Currently medications used in attempt to relieve muscle cramps are focused on repletion of vitamin and electrolyte deficiencies, or altered energy metabolism, the results are variable and unsatisfactory. 11 The aim of the study was to assess the efficacy and safety of orphenadrine in the treatment of muscle cramps in patients with liver cirrhosis.
Orphenadrine is a centrally acting skeletal muscle relaxant. It is an analogue of the centrally acting antihistamine diphenhydramine which exhibits a muscle-relaxant effect. Also, orphenadrine has analgesic effects that may contribute to its efficacy in relieving painful skeletal muscle spasm. 12
In our study, patients receiving orphenadrine on a dose of 100 mg twice daily for one month showed a significant decrease in the frequency, severity, and duration of muscle cramps compared to baseline (p < 0.001) and in comparison with the patients receiving calcium (p < 0.001) indicating that orphenadrine is a highly effective drug in the treatment of muscle cramps.
The significant effects of orphenadrine treatment on frequency of muscle cramps and their pain score extended for two weeks after stopping the treatment as confirmed by patient follow-up. This may be explained by decreased elimination of orphenadrine after regular treatment for one month. It may be attributed to pharmacokinetics of orphenadrine in which a competition for biotransformation between orphenadrine and its metabolite N-demethyl orphenadrine had occurred. 13
Few side effects were recorded, such as dry mouth, drowsiness, and nausea but there was no significant difference compared with the calcium group. There were no dropouts because of the side effects of orphenadrine. Adverse effects associated with orphenadrine may occur as a result of the drug's anticholinergic and antihistaminic effects. 14 The elderly may be more susceptible to side effects.
Orphenadrine may cause temporary drowsiness in association with higher doses and can usually be eliminated by reducing the dose. 12
In conclusion, our study revealed that orphenadrine is a safe and effective drug in the treatment of muscle cramps in patients with liver cirrhosis.
This is the first study that assessed the efficacy and safety of orphenadrine as a novel treatment of muscle cramps in patients with liver cirrhosis.
There are limitations in this study, being a pilot study with a small number of patients. However, it was unethical to try a drug in a large number of cirrhotic patients with no previous large randomized controlled study for this drug in this indication for patients with liver cirrhosis. A dose calculated by mg/kg body weight may have been more appropriate for our cirrhotic patients as they have a larger volume of distribution. All our patients had post-viral cirrhosis due to prior Hepatitis C virus infection. Additional double-blinded, randomised, controlled clinical trials on larger numbers of patients are required to support the routine use of this drug in the treatment of muscle cramps in patients with liver cirrhosis of different etiologies.
Key summary
Muscle cramps markedly affect the quality of life in cirrhotic patients and currently there is no available highly effective treatment. This is the first study to assess the efficacy and safety of orphenadrine as a novel treatment of muscle cramps in patients with liver cirrhosis. On comparing frequency, duration, and pain score of muscle cramps before and one month after treatment with orphenadrine, there was a significant decrease indicating that orphenadrine is a highly effective drug in treatment of muscle cramps. The significant effects of orphenadrine treatment on frequency of muscle cramps and their pain score extended for two weeks after stopping the treatment as confirmed by patient follow-up. Side effects were few and mild with orphenadrine and comprised of dry mouth in four patients (26.67%), drowsiness in one patient (6%) and nausea in one patient (6%), indicating that orphenadrine is a safe and effective drug in the treatment of muscle cramps in patients with liver cirrhosis. Orphenadrine is a highly promising drug in the treatment of muscle cramps in cirrhotic patients.
Informed consent
An informed consent was signed by every patient before enrollment in the study.
Footnotes
Ethics approval
The study was approved in 2015 by the Ethics Committee of the Faculty of Medicine, Tanta University (code approval number: 30128/03/31).
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.