
Abstract
Background
Research increasingly focuses on identifying individuals at greater risk of colorectal cancer (CRC) to enhance colonoscopy screening efficacy.
Objective
The objective of this article is to determine associations between chronic liver disease and lesions along the colorectal adenoma-carcinoma sequence.
Methods
This retrospective study encompasses consecutive liver disease patients (LDPs) of all etiologies evaluated for liver transplantation at a single institution and a control group of liver-healthy patients (LHPs) undergoing colonoscopy as part of the German CRC screening program.
Rates of polyps, adenomas, high-risk situations (HRS) and CRC were analyzed in univariable and multivariable settings adjusting for age, gender, body mass index and number of colonoscopies. Differences between LHPs and LDPs and between cirrhotic and noncirrhotic hepatopathy were assessed.
Results
In total, 1046 patients (52.6% male, median age 59.6 years) were included, of whom 38.9% had liver disease. A total of 41.0% of all patients showed polyps, 23.2% adenomas, 10.0% HRS, and 0.5% CRC. LDPs were more likely to develop polyps, adenomas and HRS than LHPs, both in univariable and multivariable analysis. There were no significant differences between cirrhotic and noncirrhotic patients.
Conclusion
Chronic liver disease of any etiology is associated with colonic lesions of the colorectal adenoma-carcinoma sequence, independent of cirrhosis. LDPs should receive intensified, and earlier, colonoscopy screening.
Key summary
Background
Patients with increased risk of colorectal cancer (CRC) need to be identified to enhance colonoscopy screening efficacy. Some studies have suggested associations between specific hepatopathies and colon polyps, while others have disagreed. Findings
Polyps, Adenomas, high-risk situations (according to the German CRC guidelines) and CRC were more prevalent in patients with chronic liver disease of any etiology compared with liver-healthy patients. These associations apply both to cirrhotic and noncirrhotic hepatopathy. Screening colonoscopy needs to be intensified in patients with any liver disease and should be started at the age of 45.
1. Introduction
Colorectal cancer (CRC) represents a major cause of mortality in the developed world.1,2 In most cases, the cancer develops along the adenoma-carcinoma sequence. Precancerous lesions mostly arise as adenomatous colon polyps that can be detected and resected by screening colonoscopy. 3 In Germany, this procedure is well established for patients starting at the age of 55. 4 Recently, studies have established patient subgroups that profit from enhanced screening. 5 Personalizing screening protocols to account for individual risk factors might be a key step to enhance screening efficacy5,6 and is increasingly considered in several guidelines.5,7
Lately, some studies have linked specific hepatopathies to an increased risk of colonic polyps,8,9 while others have disagreed,10–12 underlining the need for further study.
Furthermore, most studies have focused on assessing only liver disease in its last stages (cirrhosis) as a risk factor for colon adenomas.8,13,14 Meanwhile, smaller studies analyzed the impact of single entities.9,13,15,16 However, to accommodate the wide range of disorders leading to chronic liver impairment, larger studies investigating multiple liver disease entities and especially earlier stages of hepatopathy are needed to further understand the associations between liver and colonic pathologies. In this setting, we aimed to address several questions:
Is liver disease in general associated with colonic polyps and adenomas? According to the literature, cirrhosis may be associated with colonic polyps. Do patients with noncirrhotic chronic liver disease show similar associations? Should patients with chronic liver disease (liver disease patients, LDPs) receive regular screening earlier than liver-healthy patients (LHPs)?
To address these questions, our study comprises one of the largest cohorts to date in this field, with 1046 patients.
2. Methods
2.1. Patients
LDPs were examined for liver transplantation assessment, LHP in the course of the German screening protocol. 17
We included all consecutive patients who received colonoscopy between 2011 and 2017 at the Department of Transplantation Medicine of the University Hospital Münster. Furthermore, we enrolled the same number of patients from the same time frame who underwent colonoscopy in a cooperating gastroenterology practice. We then merged these two groups and stratified them for diagnosis of chronic liver disease.
For each patient, we summarized all documented colonoscopies. Exclusion criteria encompassed groups that are known to influence colonoscopy findings (Figure 1).
Inclusion and exclusion criteria.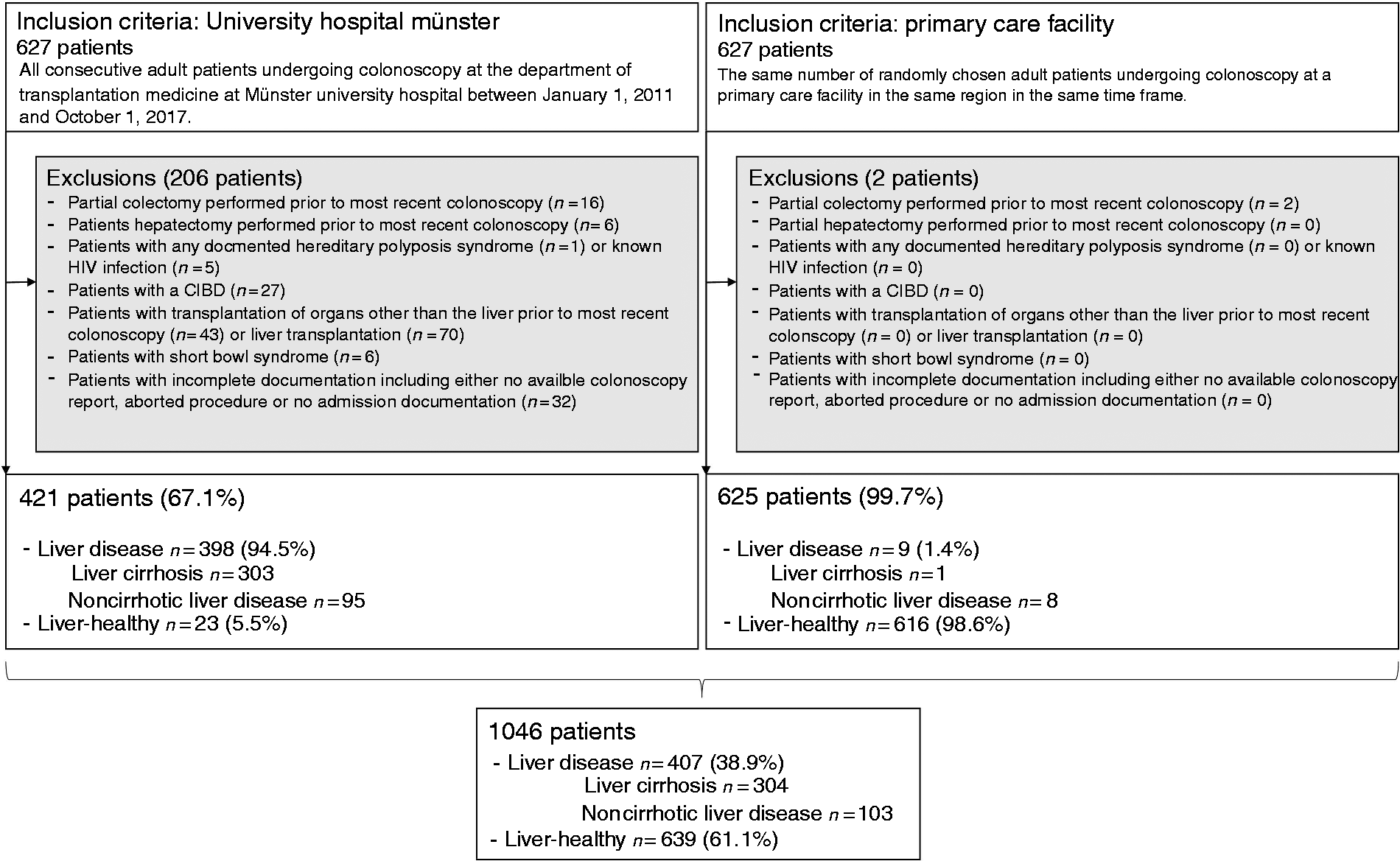
Patients were subdivided into those with a known chronic liver disorder and a liver-healthy control. Furthermore, liver disease was categorized as either noncirrhotic or cirrhotic.16,18
All patients received at least one colonoscopy. Number, size and histology of each polyp were recorded, as was CRC.
Based on histology reports, high-risk situations (HRS) were identified according to German colonoscopy guidelines and included the following findings:
Patients with
≥ 3 adenomas, or high-grade intraepithelial neoplasia, or tubular adenomas ≥ 10 mm, or tumor with a villous component.
17
2.2. Study design
This project was designed as an observational retrospective cohort study. Written informed consent was obtained from each patient prior to intervention. The study was approved by the University of Münster Ethical Committee (Ref. 2017-659-f-S, 23 January 2018) and conforms to the ethical guidelines of the 1975 Declaration of Helsinki.
2.3. Statistical analysis
Patient groups were characterized by age, gender, number of colonoscopies received and body mass index (BMI). Additionally, LDPs were described by etiology and cirrhosis, as well as model for end-stage liver disease (MELD) score.
As primary outcome, we defined the rates of lesions according to the adenoma-carcinoma sequence: polyps, adenomas, HRS and CRC.
As secondary outcomes, we assessed the number of adenomas, stratified based on implication for clinical follow-up as defined by the German CRC guidelines. 17 Accordingly, number of adenomas was defined as 0, 1–2, 3–4 and ≥5 adenomas.
Patient characteristics were analyzed using respective median and interquartile range (IQR) or mean±standard deviation, as appropriate. Prevalence data were summarized as absolute and relative frequencies. Differences between variables were determined by χ2 or Mann-Whitney U tests, as applicable.
Dependent variables were assessed in stepwise univariable regressions using χ2 or Mann-Whitney U tests. Subsequently, multivariable or ordinal logistic regressions were used to assess findings in a multivariable setting. Prior to the study we conducted literature research to identify covariables known to be associated with the occurrence of colorectal polyps. To explore the role of liver disease independently, we later included these characteristics in our multivariable model (age, gender, BMI, and number of colonoscopies).
We used our model to calculate predicted probabilities to illustrate associations between hepatopathy and colonic polyps:
For evaluation of risk of colorectal polyps in cirrhotic vs noncirrhotic LDPs, in our model, we preset the values of age, BMI and number of colonoscopies as their median and gender as male. Based on our data set and on our model, we could now calculate the risk of polyps in case of liver-healthy, cirrhotic or noncirrhotic liver disease by varying only this value. Thus, we can illustrate risk differences—based on our model—in a male patient of otherwise median characteristics that can be attributed only to presence of liver disease, and not to any of the other covariables as they are preset and remain unchanged. For calculation of onset age of screening, we used the same technique but modified the values accordingly: We defined the values of BMI and number of colonoscopies as their median and calculated the risk of colorectal lesions varying by age (40 years, 45 years, 50 years, 55 years, 60 years) and presence of liver disease. All these calculations were repeated presetting gender as male and again as female.
Significance level was defined as p < 0.05. All statistical tests were conducted using SPSS 25.0 software (IBM; Armonk, NY, USA).
3. Results
3.1. Patients and patient characteristics
Patient characteristics.
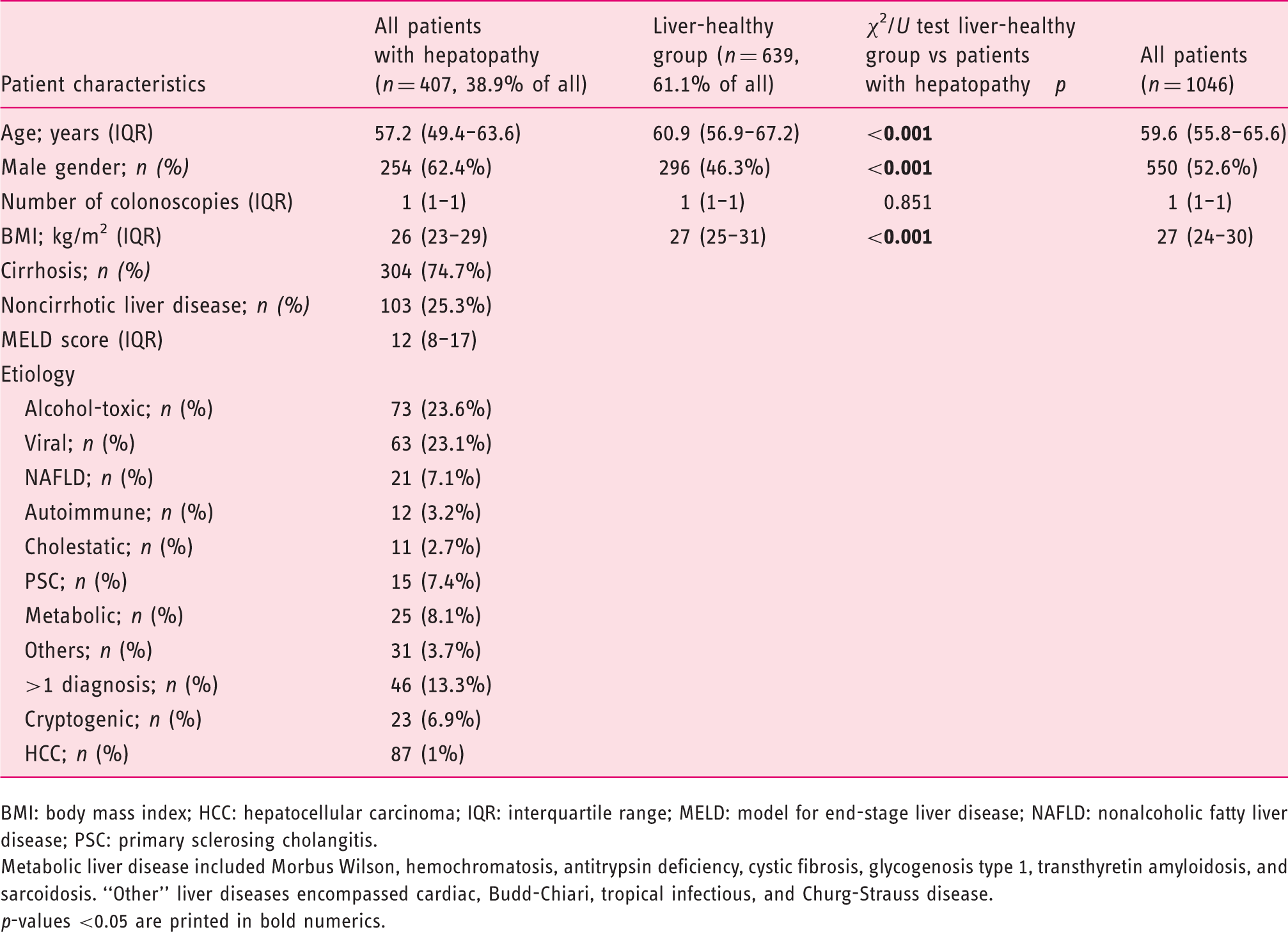
BMI: body mass index; HCC: hepatocellular carcinoma; IQR: interquartile range; MELD: model for end-stage liver disease; NAFLD: nonalcoholic fatty liver disease; PSC: primary sclerosing cholangitis.
Metabolic liver disease included Morbus Wilson, hemochromatosis, antitrypsin deficiency, cystic fibrosis, glycogenosis type 1, transthyretin amyloidosis, and sarcoidosis. “Other” liver diseases encompassed cardiac, Budd-Chiari, tropical infectious, and Churg-Strauss disease. p-values <0.05 are printed in bold numerics.
Characteristics of patients with noncirrhotic and cirrhotic liver disease.
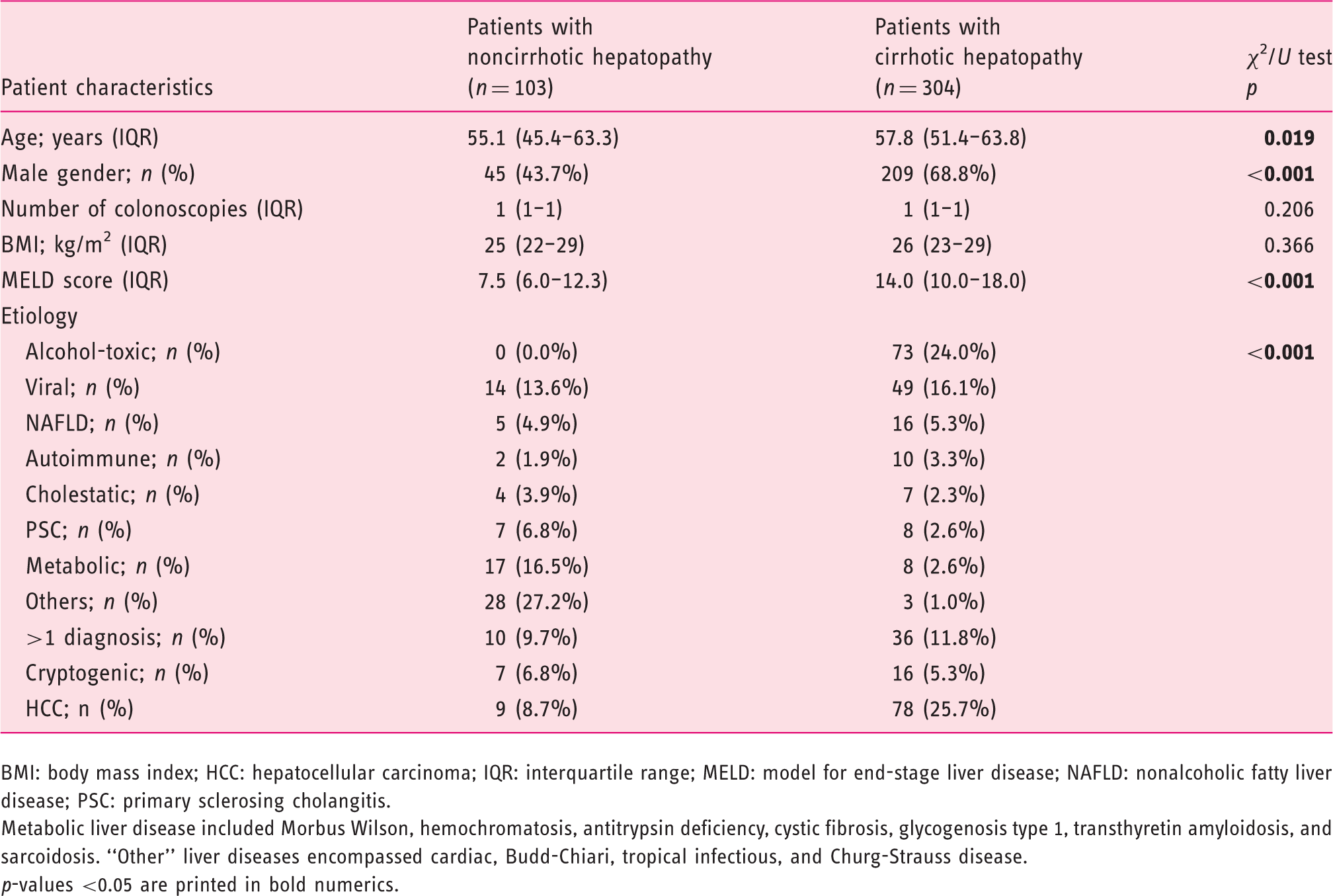
BMI: body mass index; HCC: hepatocellular carcinoma; IQR: interquartile range; MELD: model for end-stage liver disease; NAFLD: nonalcoholic fatty liver disease; PSC: primary sclerosing cholangitis.
Metabolic liver disease included Morbus Wilson, hemochromatosis, antitrypsin deficiency, cystic fibrosis, glycogenosis type 1, transthyretin amyloidosis, and sarcoidosis. “Other” liver diseases encompassed cardiac, Budd-Chiari, tropical infectious, and Churg-Strauss disease. p-values <0.05 are printed in bold numerics.
3.2. Associations between liver disease and colonic polyps
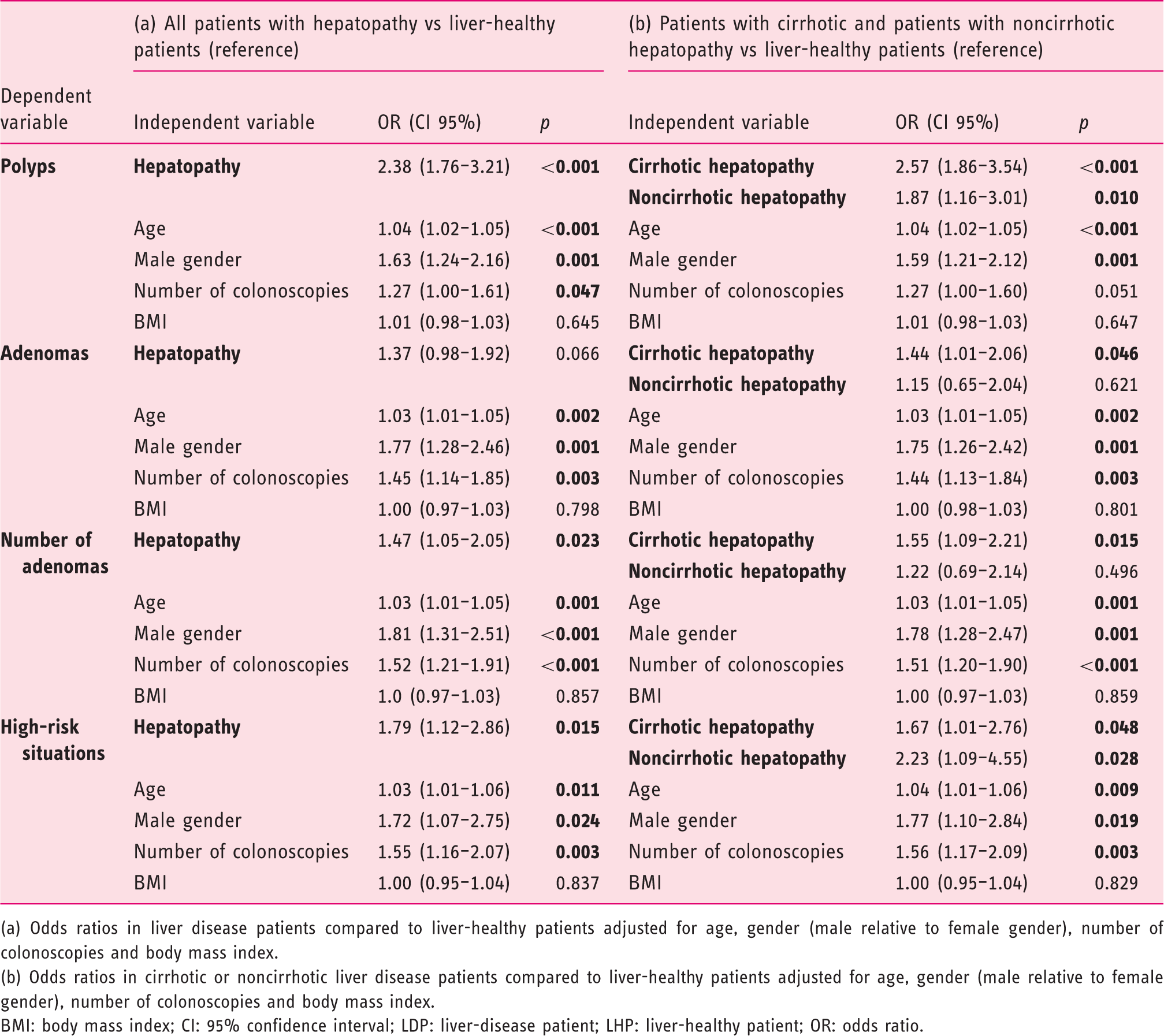
We structured our analyses according to the adenoma-carcinoma sequence, studying all increasingly dysplastic lesions—polyps, adenomas, HRS and CRC (Figure 2(a), Supplementary table S1). After univariable tests, we also compared both groups in a multivariable model, adjusting for age, gender, BMI and number of colonoscopies (Table 3(a)).
Relative frequencies of polyps, adenomas, high-risk situations and colorectal cancer in patients with and without liver disease. (a) All patients; (b) patients ≤ 55 years. Comparison by χ2 test. Multivariable tests. (a) Odds ratios in liver disease patients compared to liver-healthy patients adjusted for age, gender (male relative to female gender), number of colonoscopies and body mass index. (b) Odds ratios in cirrhotic or noncirrhotic liver disease patients compared to liver-healthy patients adjusted for age, gender (male relative to female gender), number of colonoscopies and body mass index. BMI: body mass index; CI: 95% confidence interval; LDP: liver-disease patient; LHP: liver-healthy patient; OR: odds ratio.
Polyps
Overall, 429 patients (41.0%) were found to have at least one polyp. These findings were significantly more frequent in LDPs compared with LHPs (51.8% vs 34.1%; p < 0.001).
Increased polyp rates in LDPs were confirmed in our multivariable model (odds ratio (OR) = 2.38; p < 0.001).
Adenomas
Among all patients, 243 (23.2% of total) were diagnosed with at least one adenoma.
More LDPs had adenomas (26.0% vs 21.4%, p = 0.086) compared with LHPs. Furthermore, LDPs tended to have higher numbers of adenomas per patient (1–2 adenomas: 17.7% vs 17.7%, 3–4 adenomas: 5.4% vs 2.8%, ≥ 5 adenomas: 2.9% vs 0.9%; p = 0.012).
Our multivariable model confirmed increased adenoma rates in LDPs compared with LHPs (OR = 1.37; p = 0.066), as well as higher numbers of adenomas (OR = 1.47; p = 0.023).
HRS
HRS were identified in 10.0% of patients, with significantly higher frequencies in LDPs (12.8% vs 8.3%, p = 0.019). In the multivariable model, LDPs were 1.79 times more likely to be diagnosed with HRS compared with LHPs (p = 0.015).
CRC
In total, five CRCs were detected (0.5%), four (1.0%) in LDPs and only one (0.2%) in an LHP (p = 0.059). Low absolute numbers did not allow further multivariable testing.
Lesions in patients ≤ 55 years
Univariable analyses performed in patients ≤55 years, the current onset age of screening, confirmed these tendencies (Figure 2(b)).
3.3. Cirrhotic vs noncirrhotic patients
For this evaluation, we subdivided LDP into a group with cirrhotic (n = 304) and noncirrhotic hepatopathy (n = 103). We then compared those groups to LHPs (n = 639) in our multivariable model (Table 3(b)). Furthermore, based on our model, we calculated and compared predicted probabilities in scenarios of a male patient of median age and BMI and a single colonoscopy in case of liver-healthy status, or hepatopathy with or without liver cirrhosis (Figure 3).
Predicted probabilities to detect (a) a polyp or (b) neoplasia (adenoma or high-risk situation) in the first colonoscopy of a male patient of median age (59.6 years) and body mass index (27 kg/m2) without liver disease, with noncirrhotic or cirrhotic liver disease.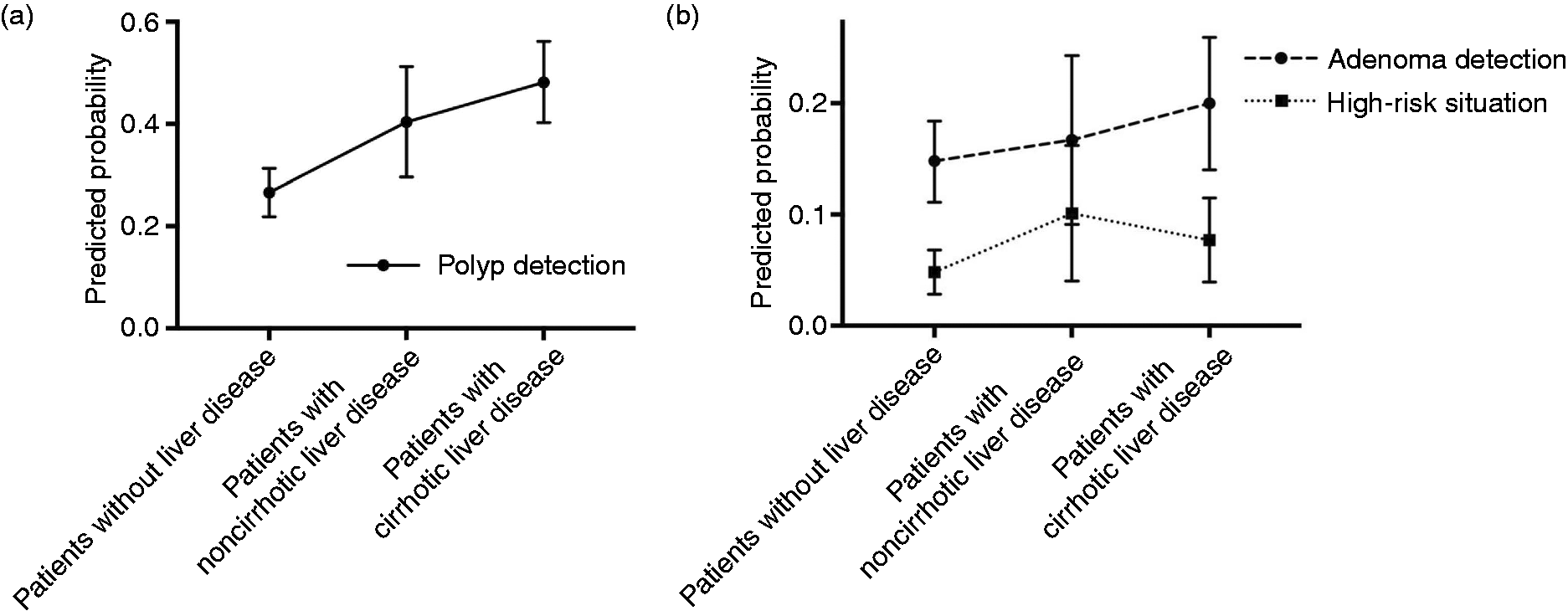
Polyps
Compared with LHPs, noncirrhotic LDPs showed higher polyp rates (OR = 1.87; p = 0.010), as did LDPs with cirrhosis (OR = 2.57; p < 0.001).
Based on the model, in a man of median age and BMI, the risk of detecting a polyp would be 26.6% if liver-healthy, 40.4% if noncirrhotic and 48.2% with cirrhotic hepatopathy.
Adenomas
Cirrhotic LDPs had a higher adenoma rate than LHPs (OR = 1.44; p = 0.046). Adenomas were also more often encountered in noncirrhotic LDPs compared with LHPs, but findings were not significant (OR = 1.15; p = 0.621).
Again, based on our patients, a man of median age and BMI would have a 14.8% chance of an adenoma if liver-healthy. In case of noncirrhotic liver disease, the risk rises to 16.7% and with cirrhosis, to 20.0%.
HRS
Cirrhotic (OR = 1.67; p = 0.048) and noncirrhotic LDPs (OR = 2.23; p = 0.028) had more findings defined as HRS than LHPs.
Based on our data, the risk of a man of median age and BMI of exhibiting an HRS would be 4.8% if liver-healthy. With noncirrhotic hepatopathy, the risk would amount to 10.1% and with cirrhotic liver disease to 7.7%.
CRC
As noted, four CRCs were found in LDPs. Of these, two were found in noncirrhotic (1.9%) and two were detected in cirrhotic LDPs (0.7%). When each rate was compared with LHPs (n = 1; 0.2%), the rate in noncirrhotic LDPs was significantly higher (p = 0.008), while the rate in cirrhotic LDPs was nonsignificantly increased (p = 0.201).
Direct comparison of patients with and without cirrhosis
Subsequently, we directly compared cirrhotic (n = 304) and noncirrhotic LDPs (n = 103) without including LHPs in the same multivariable settings. There were no significant differences regarding polyp and adenoma rate, adenoma numbers and HRS between cirrhotic and noncirrhotic LDPs.
3.4. Other influencing factors
Apart from liver disease, the covariables age, male gender and number of colonoscopies showed significant associations with the presence of the evaluated colonic lesions (Table 3(a) and (b)). The only exception in which one of these covariables—number of colonoscopies—barely missed significance level (p = 0.051) was the evaluation of the associations of cirrhotic and noncirrhotic LDPs with colorectal polyps. BMI did not prove to be of significant impact on colorectal polyps in any of our analyses.
3.5. Onset age of screening
Based on our full dataset, we calculated predicted risks for a man of median BMI undergoing his first documented colonoscopy, but varied both age (40 to 60 years in five-year increments) and presence of liver disease (yes/no; Figure 4). Risk of detecting an adenoma in a man without liver disease aged 55—the onset age of colonoscopy screening—would amount to 20.9%. With liver disease, a similar risk probability (21.2%) is reached at age 45.
Predicted probabilities to detect an adenoma in a (a) male or (b) female patient of median body mass index (27 kg/m2), with one colonoscopy and either with or without liver disease, depending on age. The horizontal line illustrates the adenoma risk in a median liver-healthy patient at the onset age of screening (55 years). It demonstrates that, in the same patient with liver disease, a similar risk probability is reached approximately 10 years before onset age of screening.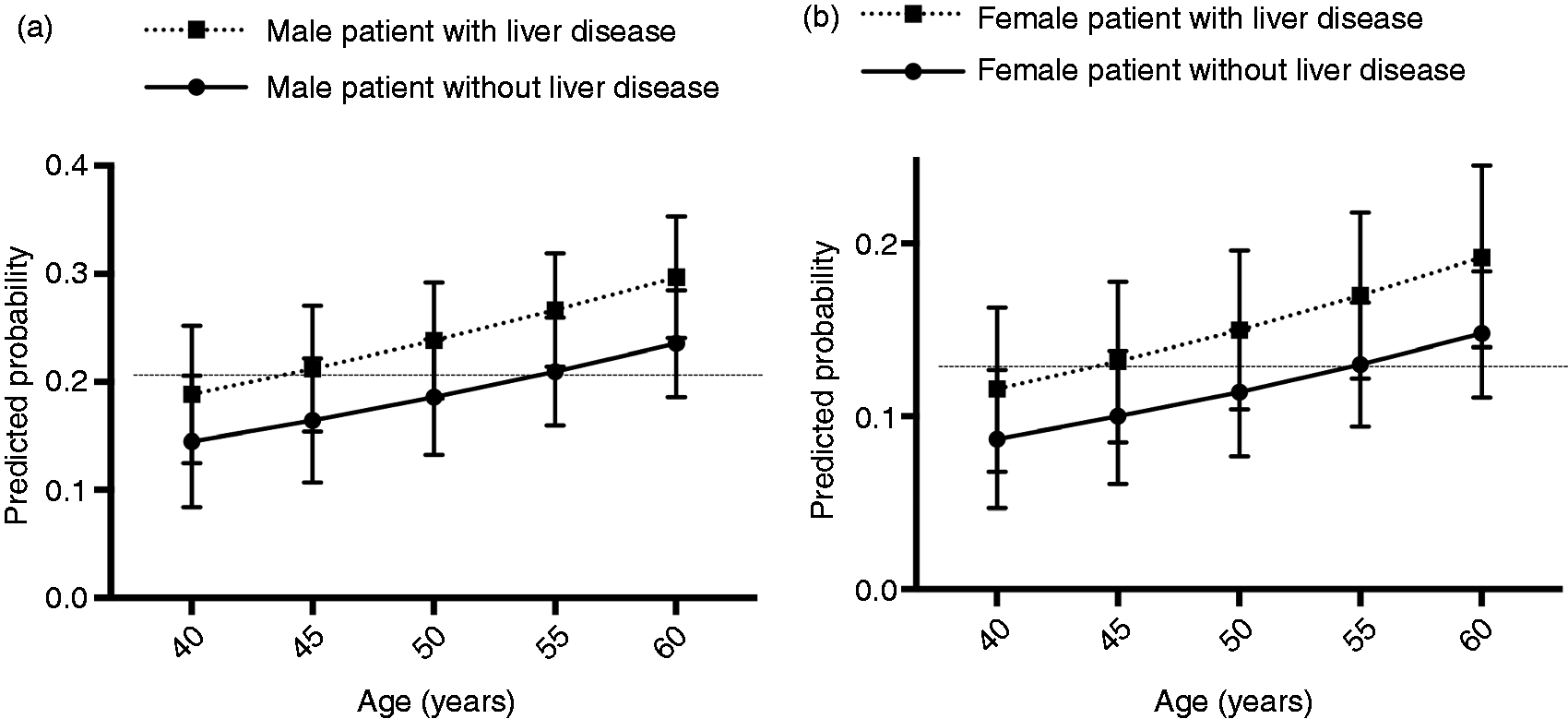
Using the same model in female patients of median BMI, the adenoma-risk in 55-year-old liver-healthy women is 13.0%. Like male patients, female LDPs had the same risk profile (13.2%) at age 45.
4. Discussion
Our study aimed to investigate associations between chronic liver diseases and the development of lesions along the colorectal adenoma-carcinoma sequence. To our knowledge, the present study is the first to examine the link between liver disease and colonic polyps taking a variety of etiologies and liver disease stages into account. Thus, we hope to provide important insights into a topic that until now has been examined only in very limited settings. Including patients of different etiologies and stages allows a more generalizable view on this issue. Furthermore, none of the studies we found included patient groups that allowed conclusions on patients with both moderate and severe chronic liver disease. Most studies so far focused on the last stage of chronic liver disease only, namely, liver cirrhosis. However, to further understand associations between hepatopathy and colorectal polyps and to even determine groups at higher risk, it is crucial to explore earlier disease stages as well. To our knowledge, we are the first to directly compare patients with moderate and those with severe chronic liver disease.
One further aim of our study was to derive and suggest an onset age of screening colonoscopy in patients with chronic liver disease that is based on established polyp detection rates in liver-healthy individuals. So far, statistical analysis to determine an adequate onset age of screening has not been performed.
At the outset of our study, as exclusion criteria, we identified confounders known to change the risk profile for colorectal polyps or alter the integrity of either gastrointestinal or liver organs.19–22
Patients were in their 60s, the main time frame for colonoscopy screenings. 10 Screening patients tended to be women, which is in line with previous findings and has been attributed to gender roles. 23 As expected, hepatopathy patients in contrast were mostly men. 24
We set out to investigate three major hypotheses:
4.1. Is liver disease in general associated with colonic polyps and adenomas?
Our study clearly reveals associations between hepatopathy and colonic polyps: LDPs displayed significantly higher polyp and adenoma rates and numbers of adenomas compared with LHPs. Thus, according to the German colonoscopy guidelines, 17 shorter follow-up intervals would ensue. Polyps in LDPs were more often HRS or invasive CRCs compared with those found in LHPs.
Prior literature research had indicated age, gender, number of colonoscopies and BMI as important influencing factors of colorectal polyps, which we included in our multivariable model.2,25 Our analysis verified these assumptions, validating the model we chose. Additionally, we were able to show that liver disease has a distinct and independent impact on the occurrence of colorectal polyps.
To our knowledge, there is no literature comparing a heterogeneous group of patients both with and without cirrhosis and of a wide variety of etiologies with a liver-healthy control.
Without similar studies to compare our data with, we will examine our findings in contrast to the literature focusing on subgroups only: There are several studies that focused primarily on the impact of cirrhosis only.8,13,14 As discussed, these analyses do not provide insight into associations between earlier-stage liver disease and colorectal polyps, an investigation that is also crucial for the understanding of the pathogenesis.
One of the largest 8 studies described a polyp rate of 46.7% vs 36.9% and an adenoma rate of 29.3% vs 21.5% with 13.9% vs 7.7% of advanced adenomas (cirrhotic LDPs vs LHPs in all instances). Another large study included cirrhotic LDPs of heterogeneous origin but no liver-healthy control. Polyps were found in 42%, adenomas in 23% of patients. 9 Findings in both studies line up well with our data. Ishikawa et al. described even greater adenoma rates, but based their findings on a much smaller cohort of 67 patients. 14 Several studies and case series disagreed, showing no significant impact of liver disease on colonic polyps. However, all of these comprised patient numbers ≤100.10–12
4.2. According to the literature, cirrhosis may be associated with colonic polyps. Do patients with noncirrhotic chronic liver disease show similar associations?
In our study, cirrhotic and noncirrhotic liver disease were identifiable as distinct subpopulations: Cirrhotic LDPs were older and showed a MELD score almost double the score of noncirrhotic LDPs. This is crucial as it allows for conclusions on liver disease in earlier stages than what has been examined so far.
The majority of studies in this field focused only on patients with liver cirrhosis.8,13,14 We could identify only one study that investigated colonic polyps both in cirrhotic and noncirrhotic LDPs, and this study focused only on specific etiologies: Naveau and colleagues 13 compared colorectal pathologies in cirrhotic and noncirrhotic alcohol-toxic LDPs without including noncirrhotic LDPs of other etiologies. The authors found a relationship between cirrhosis and colon neoplasia, and mentioned similar associations between noncirrhotic alcohol-toxic liver disease and neoplasia, but did not include the latter group in their conclusions.
Further studies investigated development of colonic polyps in patients with a single hepatopathy, regardless of cirrhosis, finding increased risks in patients with nonalcoholic fatty liver disease, 26 viral hepatitis 15 and primary sclerosing cholangitis, 18 respectively.
In comparison, our study comprised a wide range of different etiologies of hepatopathy. This reduces the influence of a single entity on the findings and allows a more global deduction. Cirrhotic and noncirrhotic LDPs alike encouraged the development of polyps and adenomas, as compared with LHPs. In general, ORs in cirrhosis were higher, but not significantly.
These findings suggest a common mechanism that links any chronic hepatopathy, independent of cirrhosis, to colon polyps. Furthermore, they strongly suggest that associations between chronic liver disease and colorectal polyps emerge earlier than expected, starting already in an early stage of chronic hepatopathy. Consistently, effects in patients with cirrhosis were slightly more pronounced, suggesting that prolonged and more severe history of disease plays a role as well. This is evidenced by higher MELD scores and older age in cirrhotic LDPs compared with noncirrhotic LDPs.
4.3. Should patients with chronic liver disease receive regular screening earlier than LHPs?
Intensified screening
While some disagree, most studies conclude that cirrhotic LDPs need to be screened more closely as they are at higher risk of colon neoplasia.8,13,14,27,28 Our findings do not only underline this conclusion. More importantly, they help expand the risk group to any patient with any chronic liver disorder regardless of the presence of liver cirrhosis. This has substantial implications on screening by increasing the number of patients considered at risk.
Complications caused by more colonoscopies must be considered: However, several studies on colonoscopy risk profiles in hepatopathy concluded that regular screening does not expose LDPs to an unjustifiable risk.8,29
Onset age of screening
In our study, univariable tests in patients ≤55 years confirmed increased polyp rates in LDPs and thus the need for earlier screening. Ishikawa et al. 14 and Jeschek and colleagues 8 recommend a screening onset age of 40 years, and Díaz-Sánchez et al. 28 an onset age of 50 years, but recommended screening only for patients with advanced liver disease (cirrhosis). Furthermore, all these studies based their threshold on the age of the youngest patient with colonic adenomas.
However, given there will still be some patients with very early-onset colonic adenomas that, as widely acknowledged, are hardly or impractical to be detected earlier, 30 we believe a more practicable approach may have merit. Screening colonoscopy should aim to be equally effective for LDPs as it is for LHPs. Our findings indicate that, to achieve a similar adenoma detection rate in LDPs compared with LHPs, screening would have to start at age 45 instead of age 55.
4.4. Limitations
There are some limitations to this study: First, our experience is limited to one region in Germany comprising only two institutions. Second, it is a retrospective analysis. However, a retrospective analysis may sometimes better reflect the daily clinical situation than a well-organized and -monitored prospective study.
Our study is embedded in a transplantation setting, which means that our patient selection was confined to patients with moderate and severe liver disease, whereas patients with earlier liver disease stages have not been investigated. Nevertheless, based on the characteristics of our cirrhotic and noncirrhotic LDPs, we believe our data allow relevant insight into this topic.
4.5. Conclusion
We found strong associations between chronic liver disease and lesions along the colorectal adenoma-carcinoma sequence. Most of these associations apply both to cirrhotic and noncirrhotic hepatopathy. Based on our findings, we recommend intensified screening colonoscopy in patients with chronic hepatopathy regardless of cirrhosis at age 45.
Supplemental Material
Supplemental material for Chronic liver disease promotes lesions of the colorectal adenoma-carcinoma sequence, independent of liver cirrhosis
Supplemental Material for Chronic liver disease promotes lesions of the colorectal adenoma-carcinoma sequence, independent of liver cirrhosis by Amelie S. Troschel, Alexander Miks, Fabian M. Troschel, Anna Hüsing-Kabar, Miriam Maschmeier, Hauke S. Heinzow, Hartmut H. Schmidt and Iyad Kabar in United European Gastroenterology Journal
Footnotes
Declaration of conflicting interests
None declared.
Ethics approval
This project was designed as an observational retrospective cohort study. The study was approved by the University of Münster Ethical Committee (Ref. 2017-659-f-S, 23 January 2018) and conforms to the ethical guidelines of the 1975 Declaration of Helsinki.
Funding
This study received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Informed consent
Written informed consent was obtained from each patient prior to intervention.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.