
Abstract
Background
Patients with ulcerative colitis (UC) have an increased risk of colorectal cancer. Scarce data regarding the development of adenomas in these patients are available both for normal and colitic mucosa.
Objective
The objective of this article is to evaluate the prevalence of adenomatous polyps and associated risk factors in patients with UC.
Methods
Patients with UC were identified from the databases of two tertiary referral centers. Medical, endoscopic and histologic reports were reviewed.
Results
A total of 403 patients were included (53% male; 33% extensive colitis) and 1065 colonoscopies (median per patient, 2) were recorded and analyzed. Seventy-four adenomas in 47 patients (11.7%) and three cases of colorectal cancer were found during a median follow-up of 6.3 years. The cumulative risk of colorectal adenoma was 4.7%, 16.7%, 23.6% and 34.4% at 10, 20, 30 and 40 years from UC diagnosis, respectively. The cumulative risk of developing metachronous colorectal adenoma was 66.7%, 87.9%, and 90.9% at 5, 10, and 15 years from first adenoma detection. Older age at UC diagnosis and longer disease duration were independent risk factors for colorectal adenoma development.
Conclusions
The prevalence of colorectal adenomas among UC patients seems to be higher than previously reported, although lower than in the background population.
Key summary
Established knowledge on this subject. The development of colorectal adenomas in patients with ulcerative colitis (UC) has not been accurately assessed, even though it seems to be lower than in the background population. Moreover, scarce data regarding both risk factors for the development of colorectal adenomas and the risk of metachronous colorectal adenomas in UC patients are available. Significant and/or new findings of this study: Although all the endoscopies in the present study were performed with white light endoscopes and we did not have a control group (patients without UC) to help clarify the difference in the prevalence of colorectal adenomas between patients with UC and patients without UC, we found a low prevalence of colorectal adenomas in patients with UC. However, the observed prevalence is higher than previously reported. No colorectal cancer was found in patients with colorectal adenomas and UC once these lesions were removed. No effect on the development of colorectal adenomas regarding UC-related therapies was found. The risk of metachronous colorectal adenomas in UC patients seems to be similar to that of the background population.
Introduction
Although a decrease in the risk of colorectal cancer (CRC) in patients with ulcerative colitis (UC) has been reported recently, these patients are still at an increased risk of developing this complication when compared to the general population. 1 Extensive disease, longer UC duration and primary sclerosing cholangitis are the most relevant risk factors for the development of UC-related CRC,4–7 whereas more accurate control of the inflammatory activity of UC seems to reduce this risk.5–7 Flat dysplasia is considered to be the best surrogate marker of CRC risk in patients with inflammatory bowel disease (IBD), and is believed to develop through an inflammation-dysplasia-carcinoma sequence. 8 A surveillance colonoscopy program is recommended for patients with long-standing colonic IBD in order to prevent CRC development by detecting neoplasia at early stages. 9 In recent years, the widespread use of new technologies for the screening of dysplasia has increased the number of dysplastic lesions among UC patients, 10 though the prevalence of CRC remains practically unchanged. 11
On the other hand, because of pathogenic concerns, until recently, adenomatous polyps in UC were usually grouped together as adenoma-like dysplasia when they were located within colitic segments (as opposed to raised dysplasia with a gross appearance like a plaque, mass or stricture, and, in turn, classified as non-adenoma-like dysplasia or dysplasia-associated lesion or mass (DALM)), and sporadic adenoma when located in those colonic segments not involved in UC.8,12 It has been recommended that both adenoma-like dysplasia and sporadic adenoma should be removed endoscopically whenever possible and followed up in a similar way to sporadic adenoma in non-IBD patients.9,13–15 A recent consensus statement proposed a new terminology in an attempt to establish a more uniform classification of endoscopic findings in IBD surveillance. It has been proposed that the phenomena referred to using the older nomenclature described above should be reclassified as visible dysplastic lesions encompassing polypoid and non-polypoid dysplasia (regardless of their location with respect to colitic mucosa), and invisible dysplasia when identified by random biopsies of colon mucosa without a visible lesion. 16 However, this new nomenclature does not take into account the natural history of polypoid dysplasia resembling a sporadic adenoma as compared to raised lesions that do not resemble an adenoma. This is an important issue, since the risk of CRC development once those lesions are detected is not necessarily the same. 10
Although an occurrence rate of colorectal adenomas of up to 7.5% has been reported among UC patients,15,17–22 scarce data are available regarding the prevalence of these lesions in patients with UC. The lack of consistent definitions for raised dysplasia forms in IBD may have had an influence on the paucity of such information.
The aims of the present study were to assess the prevalence both of sporadic adenoma and adenoma-like dysplasia, grouped as colorectal adenomas, in patients with UC, and to identify associated risk factors, outcomes and recurrence.
Materials and methods
This was a retrospective study performed in two tertiary referral centers in Catalonia (Hospital de Sant Pau, Barcelona; Hospital Germans Trias i Pujol, Badalona). Patients were identified from the respective local data of the ENEIDA database (Estudio Nacional en Enfermedad Inflamatoria Intestinal sobre Determinantes genéticos y Ambientales), a nationwide database by the Spanish Working Group in IBD (GETECCU). The Ethics Committee of both centers approved the ENEIDA Registry on April 27, 2006 (reference EO-06-031). All patients provided their informed written consent for participation. The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a prior approval by the institution’s human research committee.
Patient selection and data collection
For the purpose of our study, a cohort of UC patients prior to the implementation of chromoendoscopy and narrow band imaging (NBI) endoscopy for surveillance of dysplasia and CRC in IBD was identified from our IBD databases. Medical records and endoscopic and histopathology reports of all these patients were carefully reviewed from UC diagnosis to October 2009. Taking into account that most scientific societies recommend beginning CRC screening at age 50 in the average risk population as the preferred screening strategy, with a more intensive screening in first-degree relatives patients with CRC, starting at a younger age than the average-risk population (usually beginning screening at age 40),23,24 we decided to exclude those UC patients in whom all the available colonoscopies were performed under 40 years of age. Patients with a previous diagnosis of CRC or colorectal adenoma were also excluded and those colonoscopies not reaching at least the ascending colon were excluded from the analysis.
Therefore, all patients over 40 years of age diagnosed with UC for whom at least one colonoscopy report was available, regardless of age at UC diagnosis and indication for colonoscopy, were included. Demographic data (date of birth, gender), epidemiological data (smoking history, personal history of malignancies, familial history of IBD or CRC), clinical data regarding UC (date of UC diagnosis, maximal disease extent defined as the maximal macroscopic involvement of disease at colonoscopy at any time, 25 extraintestinal manifestations) and UC-related drug therapies (prescription of systemic corticosteroids, oral aminosalicylates, thiopurines, or biological therapies whenever used), as well as date, indication, and type of surgery (when performed), were collected.
Both the total duration and dosage of oral aminosalicylates, thiopurines and biological agents were registered. Aminosalicylate exposure was considered to exist when the drug was taken at a dosage of ≥1.2 g per day for at least six months; 7 thiopurine exposure was considered to exist when it was used for at least four months. 5
End of follow-up was defined as the date of diagnosis of the first colorectal adenoma or the time of CRC diagnosis, death or colectomy if no colorectal adenoma had been diagnosed previously, or the date of the last colonoscopy performed if none of these events occurred. Time of follow-up was defined as the time from UC diagnosis to the end of follow-up. In addition, we evaluated the development of metachronous adenomatous lesions in those patients in whom a colorectal adenoma was diagnosed. In this context, we considered a new follow-up period to begin from the detection of the first adenomatous lesion to the diagnosis of further colorectal adenoma, CRC, death or colectomy or the date of the last colonoscopy when none of those events occurred.
Endoscopic and histological procedure
Date, age, UC duration, and indication for colonoscopy were recorded. Colonoscopies were performed at both centers by experienced endoscopists. At the time our data were extracted, colonoscopies were performed with white light following the standard procedure (i.e. random biopsies and targeted biopsies of any visible lesion). The colonoscopy surveillance program followed the current European recommendations for dysplasia surveillance in IBD patients 9 at any given time, though it varied depending both on the physicians’ discretion and patients’ decisions. Polypoid mucosal lesions were removed when found.
The histopathology reports of all the available raised lesions detected and removed in each colonoscopy were reviewed. A colorectal adenoma was defined as an endoscopically resectable lesion with a histological diagnosis of adenoma, whether it was located within or outside the colitic mucosa.8,9,12,22,26 A second review by another pathologist was performed when a diagnosis of neoplasia was given. A one-year interval definition to define a metachronous adenoma was used to minimize the possibility of previously missed synchronous adenomas. 27 An advanced adenoma was defined as a colorectal adenoma ≥10 mm in size, or one containing a villous component or high-grade dysplasia. 28 Additionally, we also recorded the finding of post-inflammatory polyps.
Statistical analysis
Results are expressed as frequencies, mean and standard deviation (SD) or median and range, as required. For the univariate analysis, categorical variables were analyzed using Pearson’s χ2 or Fisher’s exact test, as required, and continuous variables were compared using Student’s t test. For the multivariate analysis, those variables with a p value < 0.1 in the univariate analysis were included in a stepwise multiple logistic regression analysis. The adjusted odds ratio (OR) of colorectal adenomas and its 95% confidence intervals (CI) were calculated for each independent predictor included in the final model. Prevalence of adenomas was defined as the proportion of patients with at least one adenoma in any of the performed colonoscopies. The cumulative risk of colorectal adenoma was evaluated by the Kaplan-Meier (KM) method. Statistical analyses were performed using the SPSS 18.0 package for Windows (SPSS Inc, Chicago, IL, USA).
Results
Baseline characteristics
Of the 906 UC patients identified from the databases of both centers, a total of 403 patients met the inclusion/exclusion criteria and were available for the analysis. Median follow-up was 6.3 years (range, 0–32.6 years) for a total of 2966 person-years.
Patient demographics (n = 403). Expressed in absolute numbers (frequencies) or median ± standard deviation.
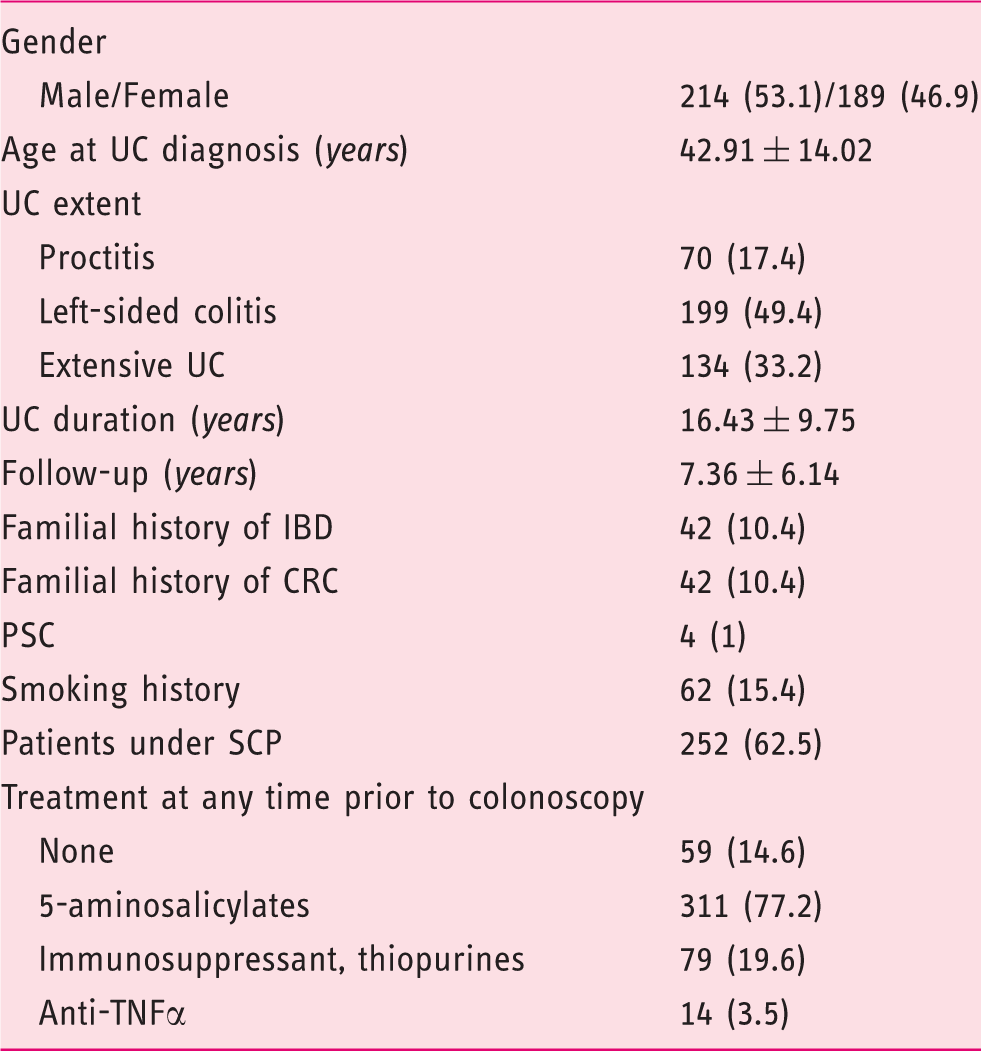
CRC: colorectal cancer; IBD: inflammatory bowel disease; PSC: primary sclerosing cholangitis; SCP: surveillance colonoscopy program; TNFα: tumor necrosis factor alpha; UC: ulcerative colitis.
Fifteen patients (3.9%) underwent colectomy during follow-up. None of them had a past history of colorectal adenoma. Ten patients underwent colectomy for refractory UC and two patients for non-malignant colonic stenosis. No flat dysplasia, colorectal adenoma or CRC was found in either the pre-surgical biopsies or the surgical specimen of these patients. Three patients underwent colectomy because of CRC (further details below).
Five patients died during follow-up, with a median UC duration of 16 years (range 5–37 years) and at a median age of 75 years (range 43–78 years). One patient died of lung cancer, two of pancreatic cancer, one of unknown non-colorectal metastatic cancer and one after a total colectomy due to a severe, refractory UC flare-up.
Endoscopic findings
Features of study colonoscopies and endoscopic findings.

IQR: interquartile range; SCP: surveillance colonoscopy program; UC: ulcerative colitis.
There were three cases of CRC (0.7%, all in male patients). Two had extensive UC and one left-sided UC. All CRC were located within involved segments of UC (one in the rectum, one in the sigmoid colon and one in the hepatic flexure). None of these patients had a previous diagnosis of either flat dysplasia or colorectal polyps, and all underwent proctocolectomy following CRC diagnosis.
Colorectal adenomas
Features of adenomas within and outside colitic mucosa. Univariate Analysis.
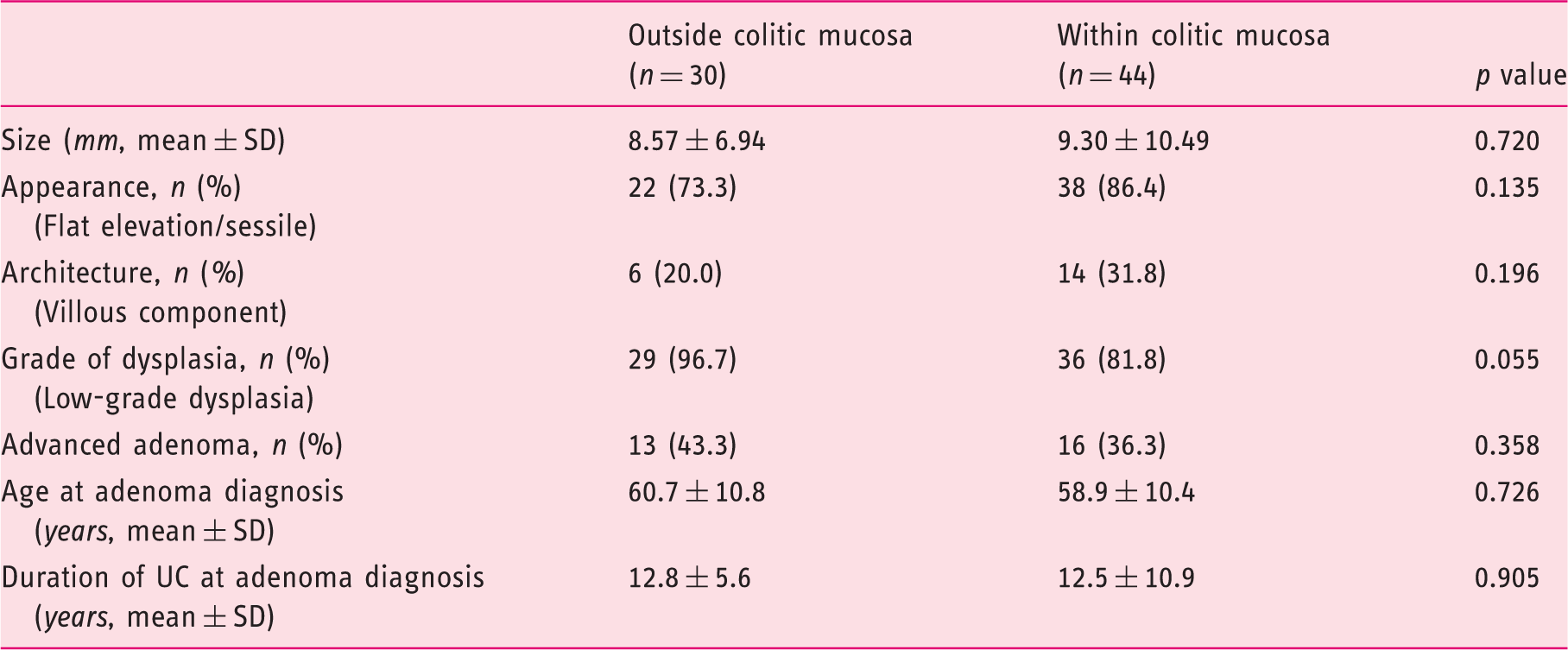
SD: standard deviation; UC: ulcerative colitis.
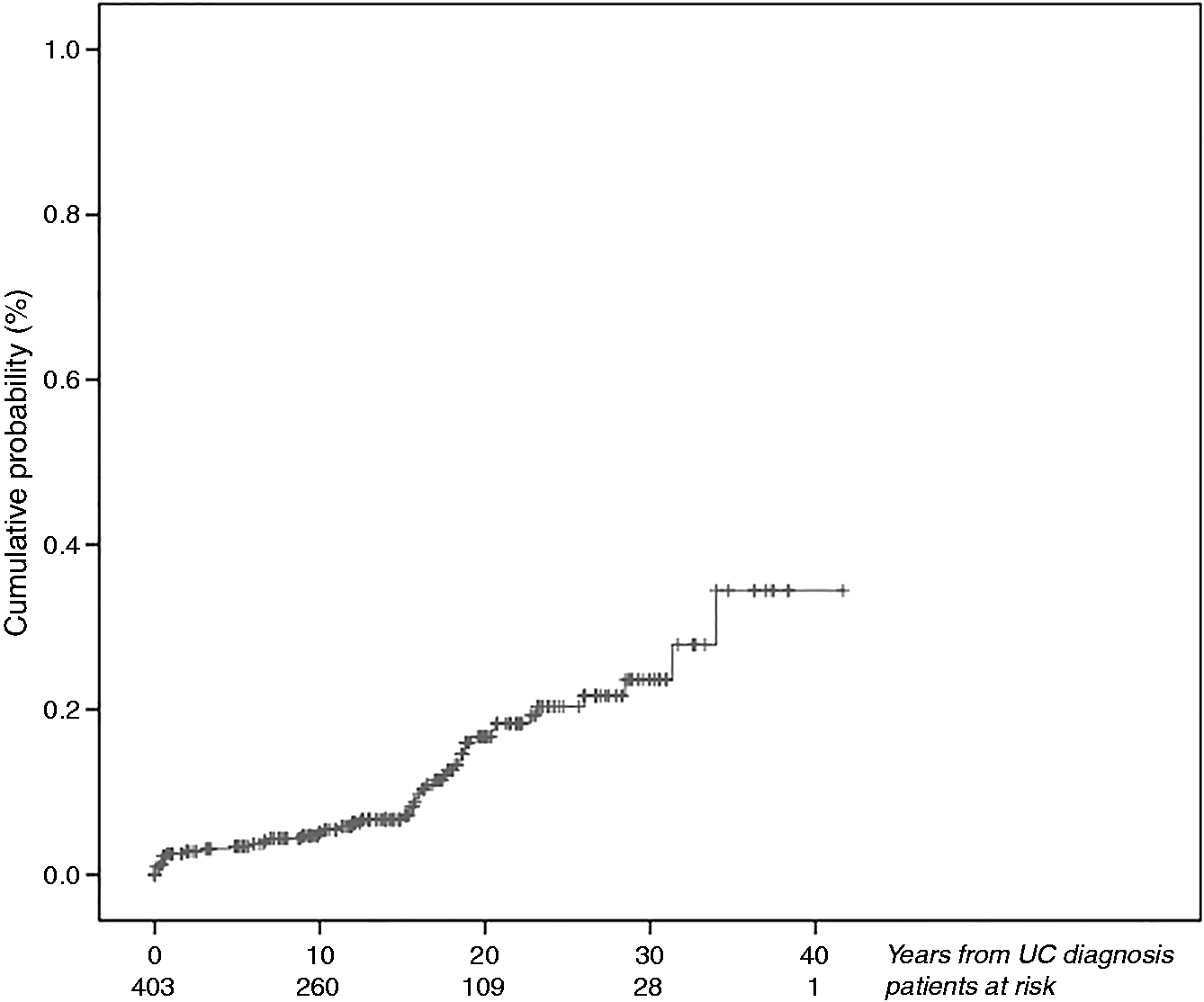
Cumulative risk of developing colorectal adenoma (n = 403).
Factors associated with colorectal adenoma in UC patients.
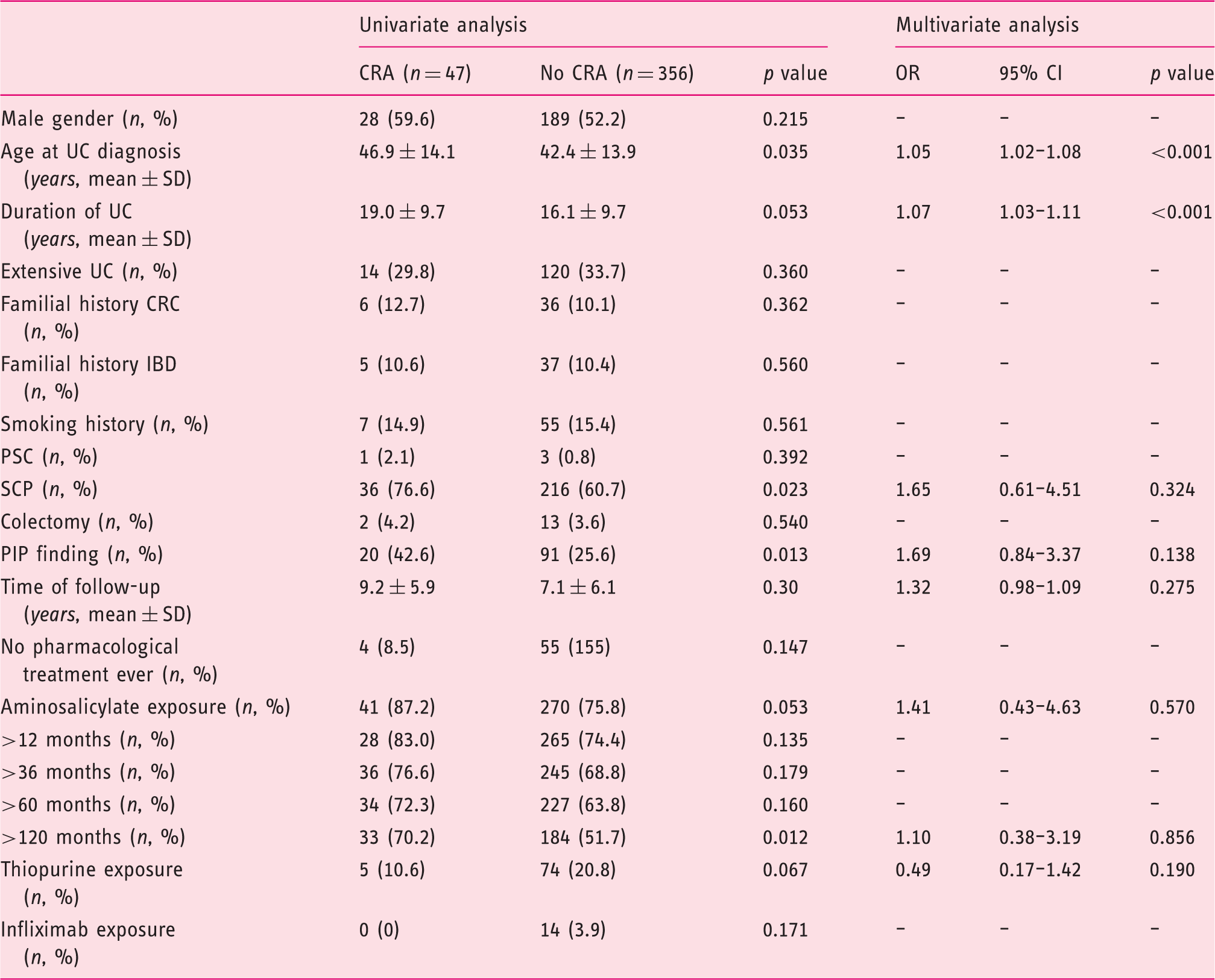
CRA: colorectal adenoma; CRC: colorectal cancer; CI: confidence interval; IBD: inflammatory bowel disease; OR: odds ratio; PIP: post-inflammatory polyps; PSC: primary sclerosing cholangitis; SCP: surveillance colonoscopy program; SD: standard deviation; UC: ulcerative colitis.
Thirty-three of those patients with colorectal adenomas (70.2%) underwent at least one further colonoscopy after the first one was detected. Of these, 13 patients (39.4%) developed at least one metachronous colorectal adenoma (median, 1, range 1–5) within a median of 61 months (range 12–259 months). The cumulative risk of developing metachronous colorectal adenomas was 67%, 88%, and 91% at 5, 10, and 15 years from first adenoma detection, respectively.
Finally, there were no differences in colectomy rates between patients who developed colorectal adenoma and those who did not (2 vs. 14 patients, respectively, p = 0.562).
Discussion
Patients with UC are at risk of developing CRC1,2,9,12 and also run the same potential risk of developing CRC as the background population.13–21 Data regarding the real magnitude of the latter are scarce. Changes in the definition of raised dysplasia and CRC in IBD patients in recent years may have influenced the reported occurrence of these lesions.12,29 There is some evidence that the risk of CRC development in the presence of raised dysplasia may be different, with a lower risk in those lesions appearing as raised, dysplastic lesions with distinct borders.9,12,29
During a total follow-up of 2966 person-years, we found a prevalence of 11.7% for colorectal adenomas, which is higher than the 3–7.5% previously reported.15,17–22 This difference might be related to the baseline characteristics of the studied UC population. Kitiyakara et al. 17 found six out of 115 UC patients (4%) with colorectal adenomas, though patients with a familial history of CRC were excluded. Dixon et al. 19 reported a prevalence of colorectal adenoma of 3.7%, but this study evaluated a subgroup of patients aged 55 to 64 years. Finally, in a recent case-control study, adenomatous polyps were detected in 6.3% of UC patients, although this study included only patients over 50 years of age. 22 The design features of our study may also explain some of the differences in the frequency of colorectal adenoma. Firstly, in line with the recommendations by scientific societies for the beginning of CRC screening in the general population,21,24 we included all those patients over 40 years of age at colonoscopic examination. Considering that the physiopathology of adenomas in IBD patients seems not to differ from that of the background population, 10 we thought that this would be the best approach to the background population at risk of colorectal adenoma and CRC. In addition, we did not exclude patients according to UC extent or duration, giving a more accurate picture of adenoma risk in the whole UC population.
Furthermore, only 0.7% of patients developed CRC in our cohort, in concordance with recent data of a current lower CRC risk in UC patients. 1
Despite the higher frequency of colorectal adenomas found in our cohort, it is still lower than the 32% observed in a middle-aged non-IBD Spanish adult population. 30 The reasons why colorectal adenomas are less common in IBD patients are not fully understood. It has been suggested that the use of oral aminosalicylates may have a potential chemopreventive effect on the development of these lesions,19,31 with conflicting results on the effect on the development of CRC in IBD.7,32,33 Moreover, a possible protective effect of thiopurine use in the development of CRC in IBD has been reported.5,7 Nonetheless, we did not observe any association between either aminosalicylate or thiopurine use and colorectal adenoma in our cohort. Furthermore, it has been suggested that the activation of the immune system and the increased presence of intraepithelial lymphocytes that occurs in the colon in UC may allow for the recognition and elimination of the neoplastic cells that could play an important role as adenoma precursor cells.22,34 In this sense, the proportion of patients in our cohort that were exposed to immunosuppressive therapy, and therefore had a more aggressive form of disease and a greater burden of inflammation, was 20%, which is in consonance with what has been described in patients with UC. 35
We also found that those patients developing colorectal adenomas seem to be at the same risk as the background population of developing metachronous adenomas. The fact that we used a one-year interval to define a metachronous adenoma strengthens our results. Similar recurrence rates have been reported previously in IBD 13 and UC. 14 Furthermore, these rates are very close to the 30–50% reported in the general population. 16 These data highlight the importance of carrying out endoscopic follow-up surveillance with these patients once a colorectal adenoma is detected.
A different pathogenesis of colorectal adenomas in UC patients has been suggested depending on their location (colitic or normal mucosa). 29 We did not find differences between patients with adenomas arising within or outside colitic mucosa regarding UC extent, disease duration, and age at UC diagnosis. Moreover, as observed in previous studies,14,15 we found no differences in recurrence rates between adenomas arising within or outside colitic mucosa. These findings support the hypothesis that dysplastic raised lesions in UC patients with an endoscopic and histologic adenoma appearance may have a similar natural history to adenomas in non-IBD patients and should be managed similarly whether they arise within or outside colitic mucosa. 9 This may also explain why age at UC diagnosis and time of UC evolution were the only independent risk factors for colorectal adenomas in our population. This may reflect the fact that, as in the background population, age but not UC itself is the main risk factor for colorectal adenomas in UC patients. 24
Our study has several limitations. We did not have a control group (patients without IBD) to help clarify the difference in the prevalence of colorectal adenomas between patients with UC and patients without UC. Notwithstanding, we did have a very good quality reference as to the real prevalence of colorectal adenomas in the non-IBD population in Spain. 30 Moreover, all of the colonoscopies were performed with white light endoscopes, and this might have led us to underestimate the frequency of colorectal adenomas. However, although recent studies suggest an increased detection of dysplastic lesions with advanced endoscopic techniques as compared with white light endoscopy in dysplasia surveillance in IBD, 10 other studies have not demonstrated an increased neoplasia detection rate. 11
In summary, patients with UC seem to be at a lower risk of developing colorectal adenomas than the background population. UC patients who develop colorectal adenomas are at a high risk for metachronous lesions, indicating the need for regular follow-up examinations.
Footnotes
Acknowledgments
Jordi Gordillo collected the data, designed the study, performed the statistical analysis and drafted the article. Esther Garcia-Planella, Eduard Cabré and Eugeni Domènech designed the study, interpreted the results and drafted the article. Xavier Bessa and Ignasi Gich helped in the statistical analysis and the interpretation of the results and drafted the article. All the remaining authors collected data, reviewed and approved the article.
Eugeni Domènech is the guarantor of this article.
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethics approval
The Ethics Committee of both centers approved the ENEIDA Registry on April 27th, 2006 (reference EO-06-031).
Informed consent
All patients provided their informed written consent for participation.