
Abstract
Background
The association between diverticulosis and colonic neoplastic lesions has been suggested, but data in literature are conflicting. This study aimed to investigate such a relationship in patients participating in a colorectal cancer screening program who underwent high-quality colonoscopy.
Methods
Data from consecutive individuals 50–75 years of age with a positive faecal immunological test were considered. Diverticulosis was categorised as present or absent. The prevalence of neoplastic lesions (adenoma, advanced adenoma, and cancer) between individuals with and those without diverticula was compared. A multivariate analysis was performed.
Results
Overall, data from 970 consecutive individuals were evaluated, and diverticulosis was detected in 354 (36.5%) cases. At least one adenoma was detected in 490 (50.5%) people, at least one advanced adenoma in 264 (27.2%), multiple adenoma in 71 (7.3%), whilst a cancer was diagnosed in 48 (4.9%) cases. At univariate analysis, the adenoma detection rate in patients with diverticula was significantly higher than in controls (55.9% vs 47.4%; p = 0.011). At multivariate analysis, presence of diverticulosis was an independent risk factor for both adenoma detection rate (OR = 1.58; 95% CI = 1.14–2.18; p = 0.006) and advanced adenoma (OR = 1.57; 95% CI = 1.10–2.24; p = 0.013), but not for colorectal cancer.
Conclusions
In a colorectal screening setting, the adenoma detection rate was significantly higher in individuals with diverticulosis than in controls.
Introduction
Diverticulosis and colonic neoplastic lesions are both highly prevalent in Western countries, and their incidence tend to increase with advancing age, so that an association has been hypothesised. 1 Indeed, age and some common lifestyle factors such as diet – low in fibre and rich in fat content – body mass index, metabolic-related factors, and microbiota changes may play a role in the development of both conditions.2–7 This has triggered several studies investigating the possible relationship between diverticulosis and colonic neoplastic lesions in the last decades, but conflicting results emerged. Despite some evidence suggesting an association, a systematic review concluded that the available data are not yet consistent, prospecting the necessity of further studies. 1 The inconsistency could be due, at least in part, to several reasons, including a diverse study design (retrospective, prospective), the setting (endoscopic, radiological, surgical), ethnicity (Caucasian, Asiatic) and diverticular disease (DD) phenotype (diverticulosis, diverticulitis) or neoplastic finding (adenoma, cancer) considered in different studies. Based on these considerations, we hypothesised that the screening for colorectal cancer would be a more appropriate setting to investigate the potential association between diverticulosis and neoplastic lesions of the colon. In fact, in an organised screening program, a high-quality colonoscopy according to key quality indicators is performed in asymptomatic individuals within a fixed range of age. 8 Moreover, these people have increased prevalence of neoplastic lesions due to the positive result of faecal immunological test (FIT). 9 Therefore, the primary aim of this study was to investigate the potential association between diverticulosis and colonic neoplastic lesions in a colorectal cancer screening setting. A secondary end-point was to assess diverticulosis prevalence in asymptomatic individuals with positive FIT who undergo colorectal cancer screening due to scanty research in such a setting. 10
Methods
Patients
Data from all individuals 50–75 years of age with positive FIT (cut-off: 100 ng/ml) who underwent colonoscopy in a single endoscopic unit, as a part of regional screening program (first round), were considered. Colonoscopy was performed under conscious sedation with intravenous (i.v.) midazolam 3–5 mg. Split bowel cleansing with polyethylene glycol (PEG) 3 plus 1 l for the early morning session or 2 plus 2 litres for the afternoon session was usually adopted. For the purpose of the study, incomplete examinations, for any reason, were excluded. For those patients with unsatisfactory bowel cleansing, a colonoscopy was rescheduled the day after following a further tailored bowel preparation, as routinely performed in our colorectal cancer screening program. All the endoscopic reports of individuals with a complete colonoscopy observed between July 2011 and January 2015 were singularly reviewed. Four experienced (>10 years) endoscopists, who previously completed a specific re-training for screening colonoscopy, performed the endoscopic examinations. The prevalence of different neoplastic lesions (cancer, advanced adenoma, and adenoma) was independently quoted. Advanced adenoma was defined as an adenoma with high-grade dysplasia and/or villous component >30%, and/or size >1 cm. Adenoma dimension was evaluated at endoscopy. Multiple adenoma was defined as a presence of >3 adenomas. Hyperplastic polyps were not considered. Diverticulosis was categorised as present (at least one or more diverticula present through the colon, regardless of the site, extent and severity) or absent.
Statistical analysis
Comparison of data between DD and control groups was performed at univariate analysis by using the Chi-squared test, whilst a multiple logistic regression was used to assess the relationship between neoplastic lesions detected and the age and gender of patients as well as the endoscopist involved. Odds ratio (OR) and 95% confidence intervals (CIs) were calculated. A p level less than 0.05 was considered significant. A standard statistical package was used for statistical computation (SPSS, version 19.0; Chicago, IL, USA).
Results
We analysed data from 970 patients who underwent total colonoscopy, including 458 males and 512 females, with a mean age of 63.7 years (range: 50–75). Diverticula were found in 354 (36.5%) individuals. Diverticulosis involved the sigmoid tract in all cases, extending also to the descending colon in 23% of cases, and as far as the right colon in 14% of patients. No cases of diverticula confined in the right colon were observed in our series. Sex distribution did not differ between the patients with diverticula and controls (males/females: 171/183 vs 287/329, p = 0.6), but those with diverticulosis were significantly older than controls (mean age: 65.3 ± 7.1 vs 62.8 ± 7.2 years; p < 0.001). Overall, at least one adenoma was detected in 490 (50.5%) patients, at least one advanced adenoma in 264 (27.2%), multiple adenoma in 71 (7.3%), and a cancer was diagnosed in 48 (4.9%) cases.
Distribution of neoplastic lesions according to diverticular disease (DD) status
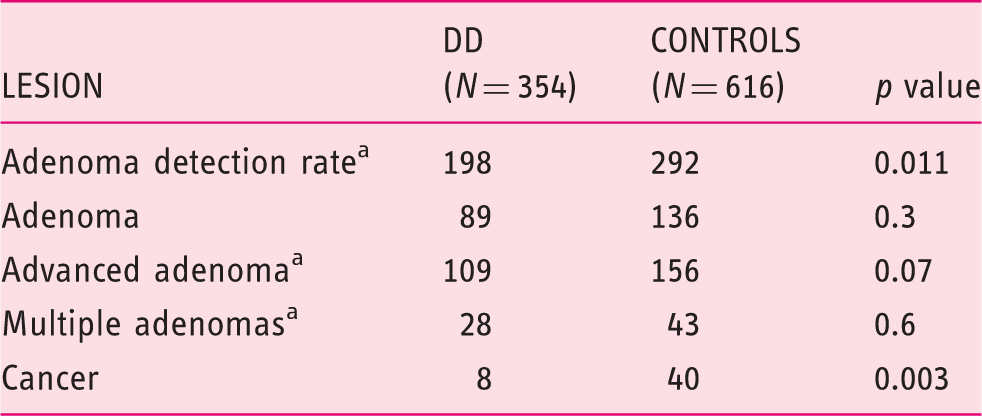
ADR: at least one adenoma, including adenoma and advanced adenoma; Advanced adenoma: adenoma with high-grade dysplasia and/or villous component >30%, and/or size >10 mm; Multiple adenomas: >3 adenomas.
At multivariate analysis, male sex (OR = 1.90; 95% CI = 1.44–2.40; p < 0.001), presence of DD (OR = 1.58; 95% CI = 1.14–2.18; p = 0.006), and age (OR = 1.04; 95% CI = 1.01–1.06; p = 0.001) were independently associated with the adenoma detection rate. Moreover, male sex (OR = 1.72; 95% CI = 1.30–2.30; p = 0.001) and diverticulosis (OR = 1.57; 95% CI = 1.10–2.24; p = 0.013) were the only statistically significant factors associated with the increased risk of advanced adenomas. Conversely, sex (OR = 0.96; 95% CI = 0.53–1.72; p = 0.9), diverticulosis (OR = 0.44; 95% CI = 0.18–1.05; p = 0.063), and patients’ age (OR = 1.01; 95% CI = 0.961–1.07; p = 0.6) were not independent risk factors for colorectal cancer. The endoscopist was not associated with adenoma or advanced adenoma detection (OR = 1.14; 95% CI = 0.95–1.38; p = 0.2).
Characteristics of advanced adenomas in diverticular disease (DD) individuals and controls
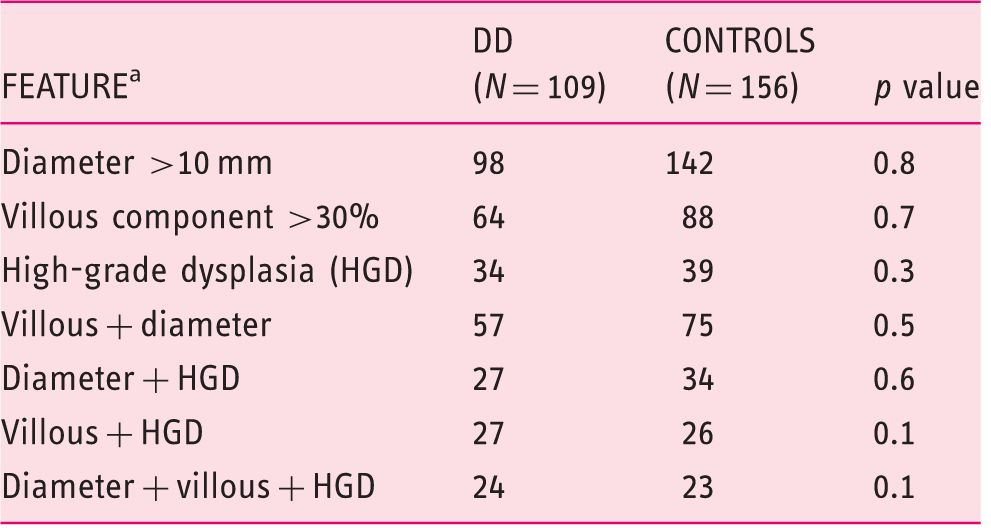
Each advanced adenoma feature was computed independently.
Discussion
Colorectal cancer is a highly prevalent neoplasia in Western countries. Similarly, diverticulosis is very frequent in the general population, particularly in aged people. It has been suggested that both conditions may share some predisposing risk factors, such as a Western diet, body mass index and metabolic-related factors, smoking, alcohol use, and microbiota changes.1–7 Therefore, a relationship between diverticulosis and colon neoplastic lesions has been proposed. A systematic review of studies published until 2007 showed that the association between diverticulosis and colorectal cancer was controversial, whilst that with either adenomas or advanced adenomas was more consistent. 1 The latter association has been substantially confirmed in different studies published thereafter,10–13 whilst other studies on the diverticulosis and colorectal cancer association still provided conflicting results.14–19 The inconsistency among studies could depend on several factors, 1 including not reporting presence of diverticula when a colonic neoplastic lesion is detected or evaluations performed in non-audited databases.20,21 Consequently, the association could have been overlooked in different studies.
To reduce these limitations, we designed the present study so the potential association was investigated in a well-defined setting – that is, a structured screening program for colorectal cancer. In this setting, asymptomatic individuals within a fixed range of age, all with a positive FIT result, underwent a high-quality colonoscopy (caecal intubation rate ≥95%; withdrawn time >6 minutes, incomplete or unsatisfactory bowel cleansing examinations were immediately re-scheduled, etc.). 22 Of note, it has been found that detection rate of both adenomas and diverticula is significantly associated with the withdrawal time at colonoscopy, 23 although colonoscopy may overlook small diverticula. 24 Moreover, all patients underwent first colonoscopy, so that the potential bias of an increased surveillance in patients with diverticulosis as compared to those in a population-based setting is ruled out in our study. 25
The detection rate of neoplastic lesions (adenoma: 50.5%; advanced adenoma: 27.2%; cancer: 4.9%) we observed is largely consistent with data reported in other colorectal cancer screening studies.26–28 Indeed, a recent nationwide Italian study found that the adenoma detection rate ranged from 13.5% to 75%, with a mean rate of 44.8%. 27 In other studies the advanced adenoma rate was 21.4%, 27 and that of cancers ranged from 3.6% to 6.3%. 29 The prevalence of diverticulosis (36.5%) we detected in the present study would appear higher than the 15.5%–28.4% reported in the English Bowel Cancer Screening Programme.10,29 However, as clearly pointed out by the same authors, under-reporting of non-neoplastic lesions – including diverticulosis – was largely probable in their study, particularly when a neoplastic lesion was detected. 10 To our knowledge, there are no other studies assessing diverticulosis prevalence in a colorectal cancer screening setting.
Of note, the multivariate analysis of our data found a statistically significant increased prevalence of either adenomas or advanced adenomas in patients with diverticulosis as compared to controls. In detail, individuals with diverticula have a near 60% increased risk of any adenoma or advanced adenoma in the colon. Similarly, male sex was found to be another independent risk factor for adenoma and advanced adenoma, with an increased risk of 72%–90%, whilst age increased the risk of any adenoma by only 4% in the considered age range. These results are relevant when considering the widely documented adenoma-carcinoma sequence in the colon. Indeed, the advanced adenoma is considered a surrogate of colorectal cancer in a colonoscopy prevention setting. 8 The multivariate analysis failed to find any independent risk factor for colorectal cancer in the considered series, including diverticulosis. This finding is agreement with data from some recent studies showing no increased risk of colorectal cancer in patients with diverticula,14–18 although data are still conflicting. 19 Potential explanations for the lacking association between diverticulosis and colorectal cancer could include an increased likelihood of positive faecal occult blood in patients with diverticula over controls, 29 the peculiar alterations of extracellular matrix in diverticulosis which are not conducive to colon cancer, 30 under-reporting of diverticula when a cancer is detected, 20 and missed lesions within the diverticular segment. 29 For the latter hypothesis, it is intriguing to note that diverticulosis is an independent predictor (OR: 4.25–6.00) of interval cancer in colorectal screening, as has emerged in recent studies.31,32 Therefore, other prospective studies, with well-collected data and including a large number of patients with colorectal cancer, are needed to unravel this potential association. In addition, the relationship between diverticulosis and neoplastic lesions could be present in only a sub-group of patients, as pointed out in a study showing an increased risk only in females with extensive, left-sided diverticulosis.33,34
In conclusion, our study found that prevalence of colonic adenomas and advanced adenomas, but not carcinoma, is significantly increased in patients with diverticulosis who underwent colonoscopy for a positive FIT result in a colorectal cancer screening program.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.