
Abstract
Background
The median age of diagnosis of primary sclerosing cholangitis (PSC) is ∼30–40 years.
Objective
We aimed to analyse disease progression and liver-dependent survival in patients diagnosed with PSC after 50 years of age.
Methods
Patients with PSC were analysed with regard to their age at diagnosis. Patients with a first diagnosis of PSC after the age of 50 years were considered as the late-onset group.
Results
A total of 32/215 (14.9%) patients were diagnosed with PSC after 50 years of age. The proportion of females was significantly higher among patients with late-onset PSC (48.4 vs. 27.3%; p = 0.02). Patients with later diagnosis required dilatation therapy more often due to dominant stenosis (84.2 vs. 53.1%; p = 0.01) and suffered from recurrent cholangitis more often (48.3 vs. 21.0%; p = 0.003). Patients with late-onset PSC had reduced transplantation-free survival (10.5 ± 0.6 years vs. 20.8 ± 1.7 years, p < 0.0001), with progredient liver failure and cholangiocarcinoma as the leading causes of death.
Conclusions
Patients with later age at diagnosis of PSC displayed a different clinical phenotype with a different sex ratio, immune status and an increased risk for progressive liver failure and biliary malignancies.
Keywords
Key summary
Patients with later age at diagnosis of PSC display a different clinical phenotype with a significantly higher proportion of females. Patients with later diagnosis require biliary dilatation therapy more often due to dominant stenosis and re-stenosis and suffer from recurrent cholangitis more often. Patients with late-onset PSC had reduced transplantation-free survival with progredient liver failure and cholangiocarcinoma as the leading causes of death.
Introduction
Primary sclerosing cholangitis (PSC) is a chronic cholestatic liver disease characterised by inflammation and stricture formation in the biliary system, progressing to liver cirrhosis in the majority of cases.1-3 The aetiology is still not resolved, but many studies suggest an immunological context.4,5 Besides the frequent association with inflammatory bowel disease (IBD) and other immune-mediated diseases,6–8 there is a clear male predominance. The median age at onset of the disease varies between different ethnic groups, but is generally between 30 and 40 years.9–11 In many cases, time of onset of disease until clinical obvious symptoms is unknown. A recent study found a high prevalence of subclinical PSC in patients with IBD, detected by magnetic resonance cholangiography. 12
In Japan, a second peak in age distribution was reported, with an onset occurring over 50 years of age. PSC occurring after 50 years of age shows distinct clinical features, such as a weaker association with ulcerative colitis (UC) and lower IgM serum levels. 13 In many immune-mediated diseases, late onset is associated with a different clinical phenotype. 14 In myasthenia gravis, early onset shows female preponderance, while late-onset patients have a male predominance, and both groups develop different alterations in the thymus tissue. 15 Furthermore, in systemic lupus erythematosus, the sex ratio varies between early- and late-onset cohorts, with a higher mortality in patients with disease onset in childhood. 16 In UC, late-onset disease is associated with higher rates of proctitis and left-sided colitis and an increased risk for cytomegalovirus and herpes virus infections. 17 Changes in immune cell function may explain characteristics of patients with late onset of different immune-mediated diseases.
In this study, we analysed the prevalence of patients with late-onset PSC, defined as a first diagnosis after the age of 50 years, and evaluated their clinical characteristics and immunological activity markers in serum and bile fluids and its impact on liver-dependent survival in a well-characterised cohort of 215 patients that has been prospectively followed for up to 25 years.
Patients and methods
Patients/study design
Clinical characteristics of patients with earlier- and later-onset primary sclerosing cholangitis.
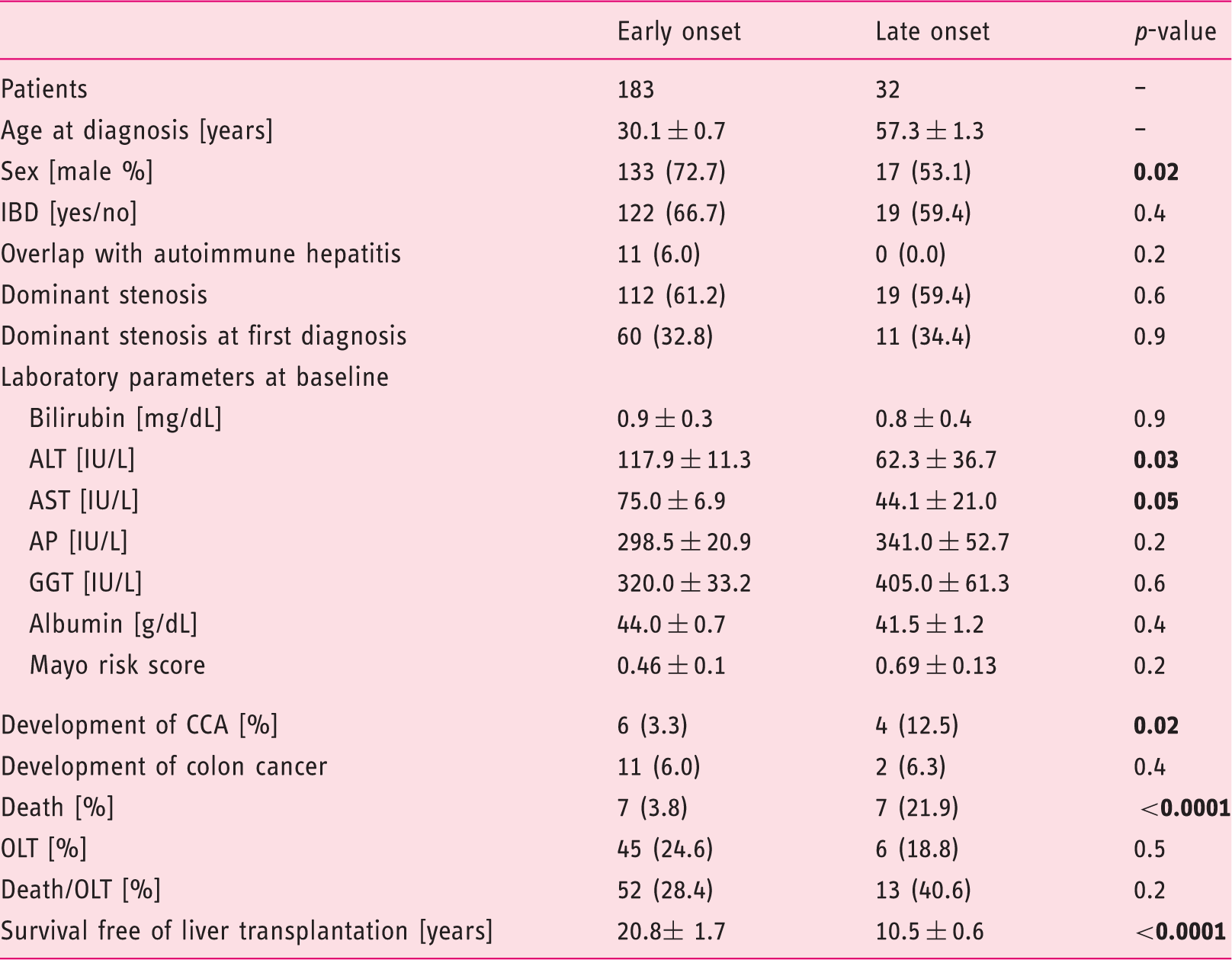
Data are presented as n (%) or as means ± standard deviations.
IBD: inflammatory bowel disease; ALT: alanine aminotransferase; AST: aspartate aminotransferase; AP: alkaline phosphatase; GGT: gamma-glutamyl transferase; CCA: cholangiocarcinoma; OLT: orthotopic liver transplantation
Measurement of serum sCD30 and cytokines in bile fluid
Serum sCD30 at time-point of first diagnosis was quantitated in 50 patients (early-onset = 40, late-onset = 10) by Human sCD30 Instant ELISA (Bender MedSystems, Vienna, Austria) according to the manufacturer’s instructions.
In 27 patients (early-onset = 19, late-onset = 8) bile samples from first ERC were available for cytokine analysis. Cytokine levels were measured by mouse cytometric bead array (CBA) Kit (BD Biosciences). Briefly, 50 μl of bile fluid or known concentrations of standard samples (0–5000 pg/ml) were added to a mixture of 50 μl each of capture antibody bead reagent and phycoerythrin (PE)-conjugated detection antibody. The mixture was incubated at room temperature in the dark for 2 h and then washed to remove unbound detection antibody. Data were acquired using a FACS AriaII flow cytometer and analysed using CBA software 1.1 (BD Biosciences).
Statistical analysis
Calculations were carried out using PASW Statistics 20. Frequencies were compared using a chi-squared test or the Fisher’s exact test where appropriate. Continuous data were compared using the nonparametric Wilcoxon rank-sum test. Actuarial transplantation-free survival was estimated using a Kaplan–Meier product limit estimator. Differences between the actuarial estimates were tested using the log rank test. Factors that independently affected the risk of reduced transplantation-free survival were determined using Cox proportional hazard ratio models with simultaneous adjustment for Mayo risk score (MRS), sex, late-onset disease, presence of IBD, and presence of DS. Statistical significance was set at p < 0.05.
Consent
Written, informed consent was obtained from each patient included in the study. The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a prior approval by the institution’s human research committee. The study was approved by the local ethics committee of Heidelberg University (S-043/2011; approval granted 19.04.2011).
Results
Clinical and laboratory characteristics and first diagnosis of PSC
A cohort of 215 patients with PSC was analysed in this study. Of these, 150 (69.8%) patients were male and 65 (30.2%) were female; 145 (67.4%) patients had concomitant IBD, of which 129 (60.0%) were UC, 13 (6.0%) were Crohn’s disease, and three (1.4%) were Colitis indeterminata. The median age at first diagnosis was 34.4 years. The clinical and laboratory baseline characteristics are depicted in Table 1. The age at PSC diagnosis was analysed and is shown in Figure 1 (a–c). Patients with first diagnosis of PSC above the age of 50 were considered as the late-onset group. The late-onset group comprised 32 patients with a median onset of PSC of 58.3 (range: 50–68) years, compared with 30.0 (range: 13–49) years in the early-onset group.
Distribution of age at first diagnosis of PSC.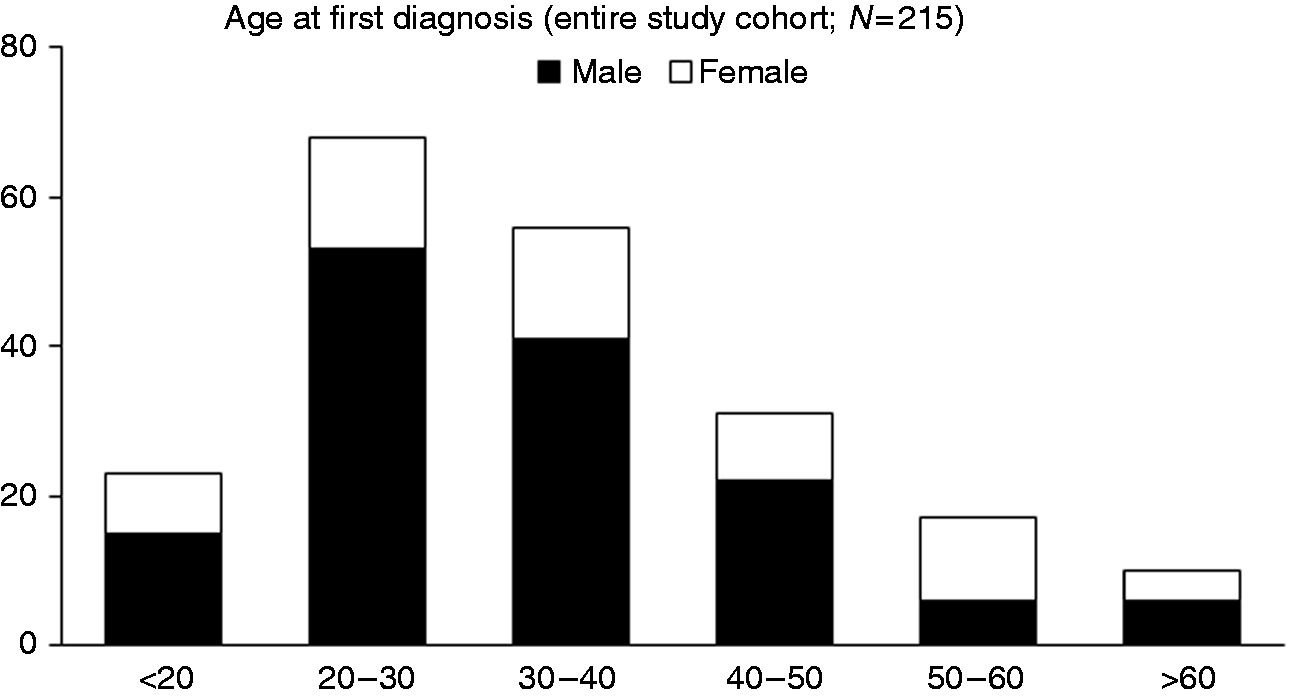
Clinical characterisation of patients with diagnosis of PSC after the age of 50
The two groups of PSC patients with earlier or later diagnosis of PSC were compared with regard to their clinical and laboratory parameters at entry into the study. We found marginally lower alanine aminotransferase (ALT) and aspartate aminotransferase (AST) levels in the late-onset group (p = 0.03 and p = 0.05, respectively), whereas the other cholestatic and liver parameters, including INR and serum albumin, showed no statistically significant difference. The prevalence of DS did not differ significantly between the two groups (112/183 (61.2%) vs. 19/32 (59.4%)), nor did we find a statistically significant difference in prevalence of DS at first diagnosis (60/183 (32.8%) vs. 11/32 (34.4%)). However, patients from the late-onset group more often developed re-stenosis, requiring repeated endoscopic dilatation (56/112 (50.0%) vs. 15/19 (78.9%); p = 0.02). In 52/215 patients, episodes of recurrent cholangitis requiring hospitalisation and/or antibiotic treatment were reported. Fourteen of 32 (43.8%) belonged to the late-onset group and 38/183 (20.8%) to the earlier-onset group (p = 0.002). Numbers of collected bile samples were comparable between both groups. Furthermore, the proportion of females was significantly higher in the late-onset group compared with the earlier-onset group (50/183 (27.3%) vs. 15/32 (46.9%); p = 0.02).
Immunological serum markers
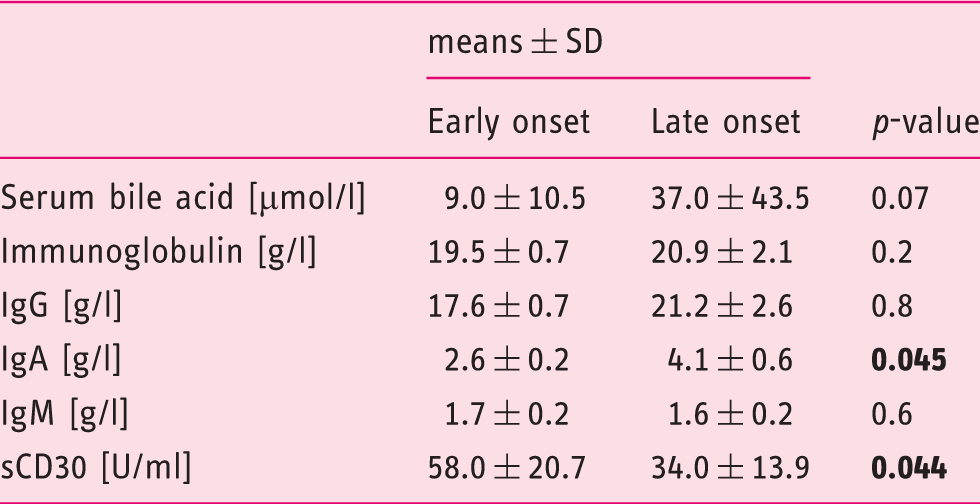
Immunological serum markers in patients with younger and late-onset primary sclerosing cholangitis.
Cytokines secreted into bile fluid
Cytokine profile secreted into bile fluid.
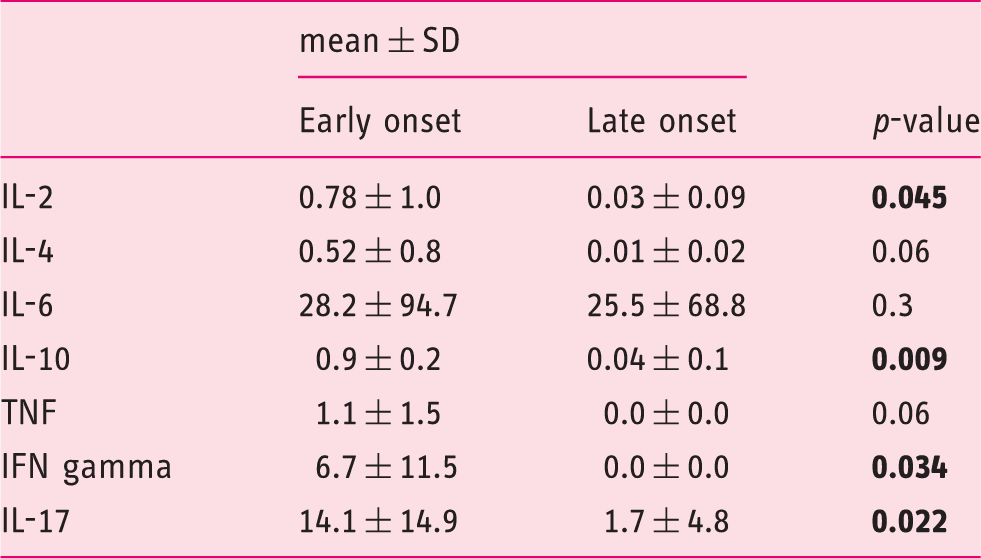
IL, interleukin; TNF, tumour necrosis factor; IFN, interferon
Disease progression and survival analysis
Clinical end points among patients with early- and late-onset primary sclerosing cholangitis.
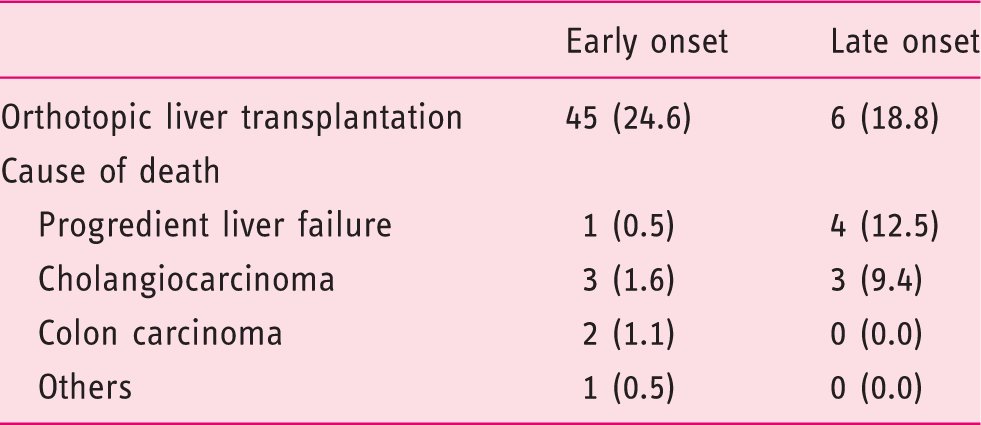
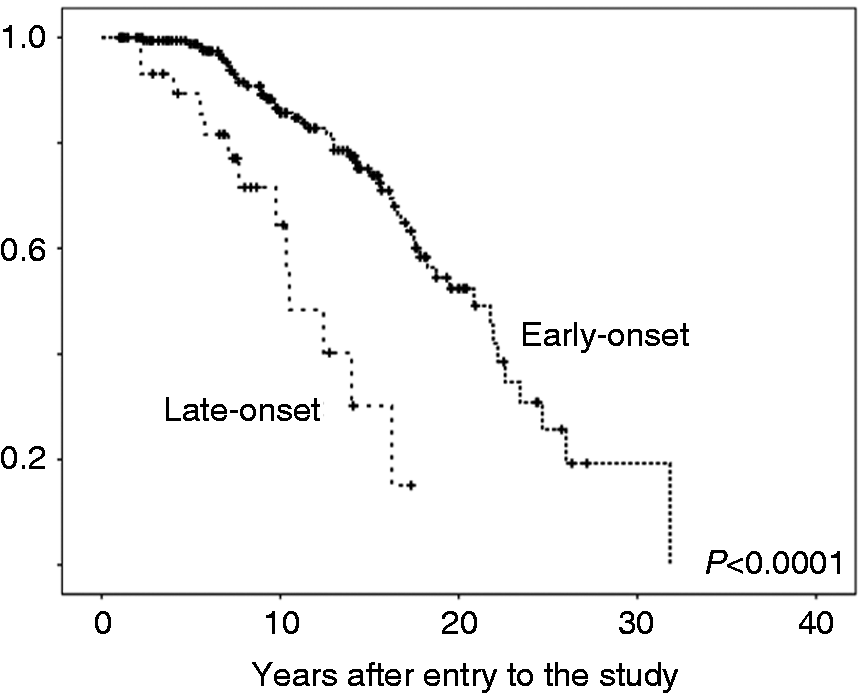
Transplantation-free survival in patients with early- and late-onset PSC.
Prognosis factors in late-onset PSC
Cox regression analysis.
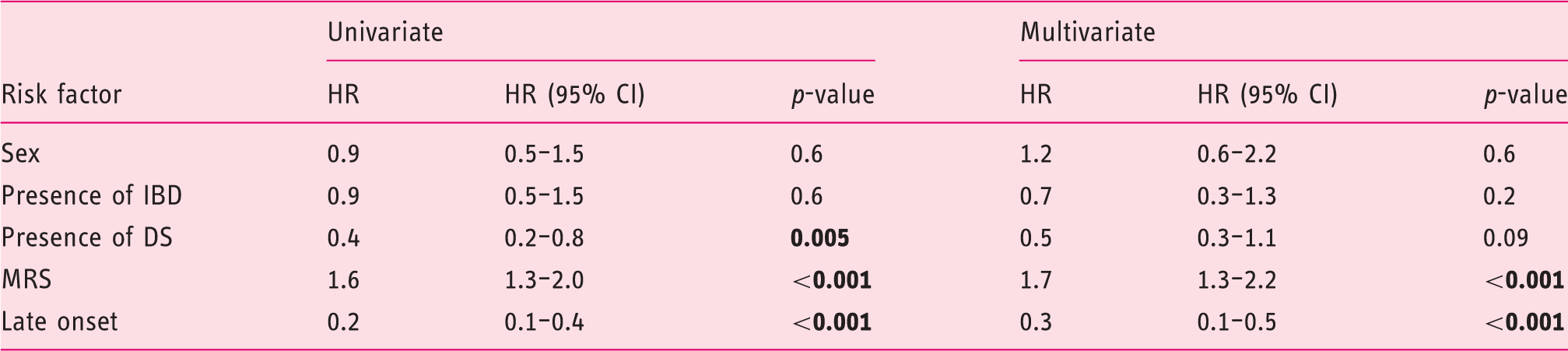
HR: hazard ratio; CI: confidence interval; IBD: inflammatory bowel disease; DS: dominant stenosis; MRS: Mayo risk score
Data show prospective factors for longer survival until liver transplantation or death. In univariate analysis presence of dominant stenosis, MRS and late-onset disease were associated with reduced actuarial survival. In multivariate analysis only MRS and late-onset disease reached significance (p < 0.05).
Discussion
In this large cohort study, we describe the clinical features of patients first diagnosed with PSC after the age of 50. We found these patients to be at increased risk of developing cholangiocarcinoma and suffer from progredient liver failure. Although these patients are reaching clinical end points at older age, compared with patients with earlier diagnosis of PSC, transplantation-free survival from first diagnosis is markedly reduced. Interestingly, the sex ratio was significantly different in the late-onset group, with a higher rate of female patients. Frequency and manifestation of IBD were not different between groups. Frequency of DS was equal between earlier and late-onset patients. However, late-onset patients developed re-stenosis requiring repeated endoscopic therapy more often, and suffered more often from recurrent episodes of cholangitis.
Worse prognosis in the late-onset cohort may be in part explained by an increased frequency of infectious complications that could aggravate disease progression. 20 This may be explained by mechanisms of immunosenescence and a subsequently impaired immune response. 21 Although an immunological basis of PSC is obvious 22 and, in many immunological diseases, a late onset is associated with slower disease progression, in late-onset PSC, the course of the disease may be driven more rapidly by repeated or chronic biliary infections. The increased frequency of episodes of cholangitis in the late-onset group may support this hypothesis. Notably, the number of bile samples were not different between patients with earlier or later diagnosis, as routinely bile samples were collected during endoscopic intervention. One possible explanation for the increased frequency of infectious complications in the late-onset group might be a reduced immune competence. To test this hypothesis, we analysed serum levels of immunoglobulins, showing a marginal elevation of serum IgA in the late-onset group. Elevated IgA has been linked to increased risk for infections in patients with liver cirrhosis, which may reflect a sustained exposure to bacterial pathogens derived from the gut. 23 Furthermore, elevated IgA seems to be associated with progressive liver fibrosis 24 as well as immunological diseases like coeliac disease. 25 In addition, we analysed serum levels of soluble CD30, a well-established marker of T-cell immunity, in our cohort. Increased serum levels of soluble CD30 are associated with disease activity in IBD. 26 Furthermore, soluble CD30 participates in the immune response against viral infectious diseases 27 and is a reliable marker for immune monitoring after solid organ transplantation. 28 CD30 knockout mice display increased susceptibility to bacterial infections due to an impaired innate function of memory phenotype CD44+, CD4+, and T cells. 29 An age-dependent decrease of soluble CD30 has already been demonstrated in paediatric patients. 30 In line with this, we found a marked decrease in soluble CD30 in the late-onset cohort. Furthermore, we found an altered biliary cytokine composition in the late-onset cohort. However, as differences in biliary cytokines were only marginal in a small subset of patients these findings need confirmation by larger studies.
The increased frequency of CC among patients with later diagnosis of PSC accounts for a higher percentage of deaths. It is worth noting that most CC developed within the first 5 years after diagnosis of PSC in these patients. We have to emphasise that patients developing malignancies within the first 3 months after the first diagnosis were excluded according to the study protocol. Of the 10 patients excluded due to development of CC, six were older than 50 years. PSC had not been previously diagnosed in any of these patients, further supporting that late-onset disease in PSC is not an innocent diagnosis. A large multicentre cohort study also found significantly higher incidence of CC in PSC patients with advanced age at first diagnosis. 31
Poorer outcome in late-onset patients may be explained by the later detection of a lengthy, pre-existing disease with a subclinical course. 12 The short timeframe between the first diagnosis of PSC followed by CC may point towards this explanation. To rule out this possibility, we performed extensive comparisons of laboratory and clinical parameters at first diagnosis. There were no significant differences in baseline laboratory parameters. Liver function, expressed by INR and serum albumin level, were comparable between both groups at the time of first diagnosis.
The reliability of the date of first diagnosis is a limitation of this study. A subclinical course of the disease without significant symptoms may differ between patients and hamper interpretation of the results. However, our well-characterised cohort of PSC patients with a standardised diagnostic, screening and therapy protocol, including UDCA and endoscopic treatment, should prevent this concern. Comparable baseline characteristics between both groups at entry into the study argue against a systematically missed onset of the disease. 32 Importantly, there were no patients with biliary cirrhosis at first diagnosis, arguing against delayed diagnosed end-stage patients with later PSC diagnosis. Finally, age at first diagnosis is a continuous variable and the age discriminator at the age of 50 seems arbitrary. Nevertheless, we decided for this age because it has been used in other immunological diseases, and previously in a PSC cohort from Japan. Furthermore, we found the age of 50 to be the best discriminator between both groups, although the basic results (transplantation-free survival, frequency of CC) remains equal if the discrimination is varied between the ages of 45 to 55 years.
In conclusion, we found an altered sex ratio and an increased frequency of biliary infectious complications in line with an altered immune status in late-onset PSC patients, subsequently leading to reduced transplantation-free survival with CC and progressive liver failure as leading causes of death. Patients with late-onset PSC display a different clinical phenotype, requiring adapted screening and surveillance strategies. As treatment options are often limited in elderly patients due to comorbidities and increased risk for general anaesthesia, PSC patients have to be evaluated carefully and well in advance for liver transplantation.
Footnotes
Acknowledgements
The authors would like to thank Petra Klöters-Plachky and Yvonne Schäfer for technical assistance.
Conflict of interest
The authors declare that they have no competing interests.
Financial support
DNG and PSa were supported by “Stiftung Elementarteilchen”, Hamburg, Germany. CR was supported by Deutsche Forschungsgemeinschaft (DFG).
Ethics approval
The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a prior approval by the institution s human research committee. The study was approved by the local ethics committee of Heidelberg University (S-043/2011; approval granted 19.04.2011).
Informed consent
Written, informed consent was obtained from each patient included in the study.