
Abstract
Background
The natural history of pediatric-onset primary sclerosing cholangitis (PSC) and overlap with autoimmune hepatitis (PSC/AIH) is poorly known.
Objective
The aim of this study was to evaluate the clinical outcome of patients with pediatric-onset disease in a tertiary referral center.
Methods
We traced 33 patients (median age at diagnosis 16 years), with PSC or PSC/AIH in cholangiography and liver histology diagnosed between December 1993 and 2011, at Helsinki University Hospital. Diagnostic procedures and long-term follow-up were reassessed until the end of December 2013.
Results
PSC was confirmed in all 33 patients; 19 of them had an overlap with AIH. At diagnosis, three of 33 had cirrhosis. Inflammatory bowel disease (IBD) was associated in 76% of the patients, mostly ulcerative colitis (70%); treatment of IBD being a minor determinant of the clinical outcome of liver disease. In the last follow-up (median nine years), all patients were alive, and no malignancy occurred. Most patients (91%) were on ursodeoxycholic acid and 12 PSC/AIH patients on immunosuppression. Endoscopic retrograde cholangiography during follow-up showed a progression of intra-hepatic disease in 12 patients (36%). Four patients (12%) had undergone liver transplantation, and one was listed; no recurrence of the disease in the graft was seen.
Conclusion
The clinical course and outcome of pediatric-onset PSC and PSC/AIH seem to be favourable in the majority of patients until early adulthood. In about one-third of patients, however, PSC is progressive, challenging the current treatment guidelines and warranting further studies on disease pathogenesis.
Keywords
Introduction
Primary sclerosing cholangitis (PSC) is a chronic cholestatic liver disease of unknown etiology characterized by inflammation and progressive fibrosis of the intra- and/or extra-hepatic bile ducts.1,2 No effective medical treatment is currently available, and the disease may progressively lead to cirrhosis and end-stage liver disease requiring liver transplantation (LT).1,2 Still, PSC is associated with inflammatory bowel disease (IBD), 3 and it also has a high risk of malignancy (i.e. colon-carcinoma and cholangio-carcinoma). 4 PSC may already occur in children, frequently in association with autoimmune hepatitis (AIH), and it is referred to as a subtype, “autoimmune sclerosing cholangitis” 5 or more commonly “primary sclerosing cholangitis/autoimmune hepatitis overlap syndrome” (PSC/AIH). 1
Pediatric-onset PSC, however, is rare
The aim of this study was to assess the long-term clinical course and prognosis of a cohort of patients with pediatric onset of PSC in Finland who underwent endoscopic retrograde cholangiography (ERC) at diagnosis and during follow-up, in order to contribute to a better definition of the natural history and surveillance of this condition.
Materials and methods
Study design
We conducted a retrospective, observational cohort study.
Study area, period and population
Patients with suspected pediatric-onset PSC, consecutively referred to the Helsinki University Central Hospital (HUCH) between December 1993 and December 2011, were traced by using the 10th revision of the International Statistical Classification of Diseases and Related Health Problems (ICD-10) codes (i.e. AIH K73 and cholangitis K83). HUCH is a tertiary referral center in Finland (5.4 million inhabitants), serving a defined population of about 1,500,000 inhabitants and covering approximately 30% of the total child population in the country (www.stat.fi). Most pediatric and adult patients with PSC are referred from all over the country to this center where ERC still represents the gold standard for the diagnosis and follow-up of this disease
Case-ascertainment
Diagnosis of PSC was based on unequivocally typical cholangiographic features of the disease (i.e. ERC) in a patient with elevated gamma glutamyltranspeptidase (GGT) and/or alanine aminotransferase (ALT) and/or alkaline phosphatase (ALP). Histologic features in the liver biopsy compatible with PSC and/or other imaging technique
All the patients’ medical records were reviewed (A.T. and T.J.) to ensure the correct diagnosis. Data regarding clinical history (i.e. symptoms and signs, associated IBD, associated autoimmune diseases) were collected. Laboratory tests including biochemical parameters (i.e. total bilirubin, ALT, aspartate aminotransferase; AST, GGT, ALP) and serologic parameters (i.e. immunoglobulin M [IgM], immunoglobulin G [IgG], antinuclear antibody [ANA], anti-smooth muscle antibody; [ASMA], antimitochondrial antibody [AMA], anti-antibody to the liver/kidney microsome type 1 [anti-LKM1], and perinuclear antineutrophil cytoplasmic antibody [pANCA]) were collected. Medical treatment during the follow-up time (i.e. ursodeoxycholic acid (UDCA), corticosteroids, immunosuppressive) was recorded. Finally, the need for and timing of LT, as well as the occurrence of complications associated with PSC (i.e. cholangiocarcinoma, colorectal carcinoma), was registered.
Liver biopsies were reviewed by an experienced pathologist (J.A.) blinded to the patients’ clinical history. The pathologist looked for the following features: the number of portal spaces included in the samples, peri-cholangiolar fibrosis, fibrosis (staging), inflammation (grading), portal inflammation, interface inflammation, lobular inflammation, rosette formation, plasma cells, eosinophil, granuloma, cholangitis, peri-cholangitis, necrosis, macro- and micro-steatosis, copper, diastase periodic acid-Schiff stain (PAS)-positive globules, hepatocellular cytokeratin 7 positivity, loss of bile ducts, acute cholestasis, and PSC alteration (0–3; 0 = no features of PSC, 1 = unspecific features of PSC, 2 = features suggestive of PSC and 3 = diagnostic features of PSC).
The modified Amsterdam PSC score at the time of diagnosis of the PSC pediatric patients (n = 33).
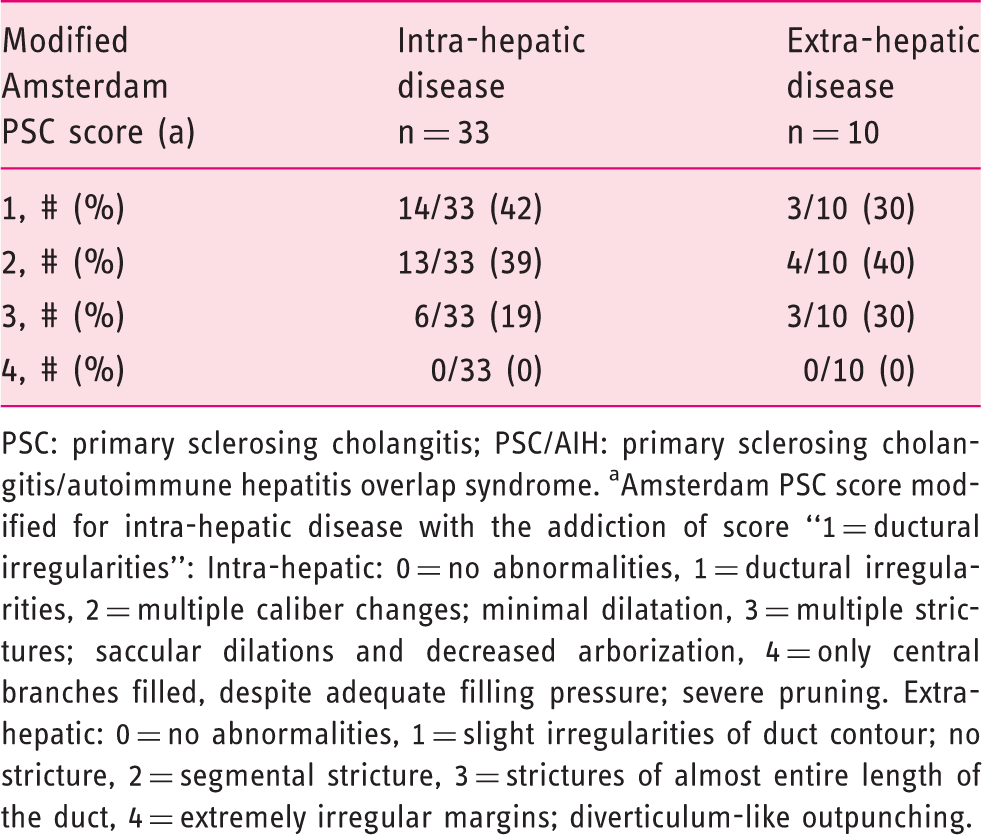
PSC: primary sclerosing cholangitis; PSC/AIH: primary sclerosing cholangitis/autoimmune hepatitis overlap syndrome. aAmsterdam PSC score modified for intra-hepatic disease with the addiction of score “1 = ductural irregularities”: Intra-hepatic: 0 = no abnormalities, 1 = ductural irregularities, 2 = multiple caliber changes; minimal dilatation, 3 = multiple strictures; saccular dilations and decreased arborization, 4 = only central branches filled, despite adequate filling pressure; severe pruning. Extra-hepatic: 0 = no abnormalities, 1 = slight irregularities of duct contour; no stricture, 2 = segmental stricture, 3 = strictures of almost entire length of the duct, 4 = extremely irregular margins; diverticulum-like outpunching.
For the study purpose, follow-up was considered to start when the patient was referred to HUCH for suspected PSC (outpatient clinic and/or liver biopsy and/or ERC) and ended at the time of the last consultation by the end of December 2013.
Statistical analysis
Data are presented as median and range when continuous. Categorical variables were compared by using Fisher’s exact test (small number of participants). Continuous variables were compared by using the Mann-Whitney test or the Wilcoxon test. The p-value < 0.05 was considered statistically significant.
Ethics consideration
The study protocol has been approved by the ethics committees of HUCH (Diary number: 64/13/03/03/12).
Results
Patient population
In the final analysis, 33 patients (median age at diagnosis 16 years: range 5–19; male: 21) were included (Figure 1). Six patients (median age 13.5 years: range 7–17; male: 1) were excluded because of misclassified diagnosis on the ICD-10 score. One PSC patient (10-year-old boy) lost to follow-up and one PSC/AIH patient (10-year-old boy) with missing data were also excluded.
Patients included in the study.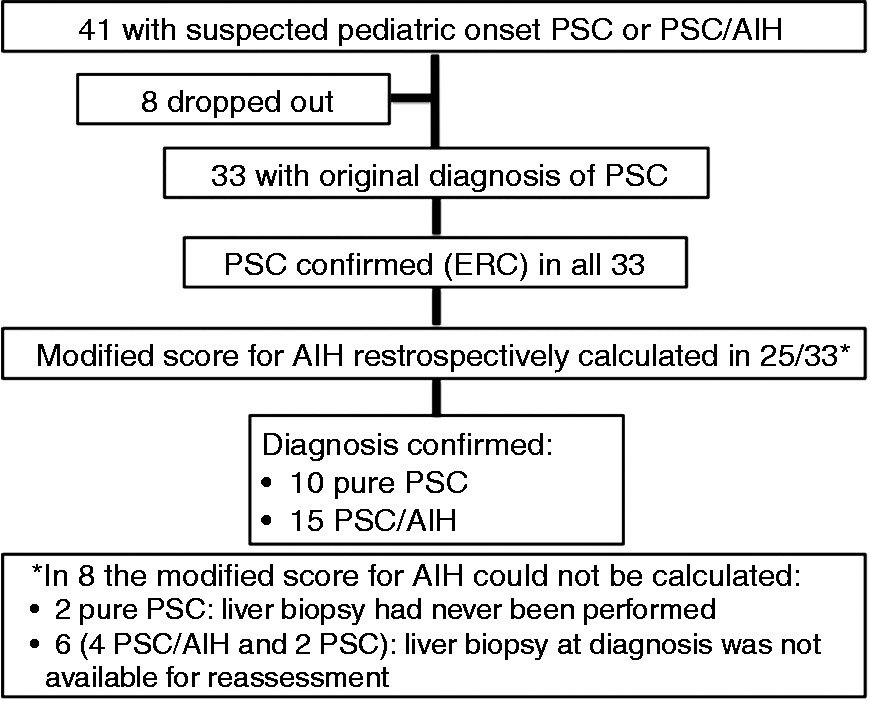
The diagnosis of PSC was confirmed in all 33 patients in the review of the ERC images at the time of diagnosis. The modified score for AIH was retrospectively calculated in 25 patients (76%) with biopsies available for review: pure PSC was confirmed in 10 and PSC/AIH in 15, the latter group including seven patients with AIH originally overlooked.
Clinical presentation and lab tests at the time of diagnosis
Background characteristics and clinical presentation at the time of diagnosis of the PSC pediatric patients (n = 33).
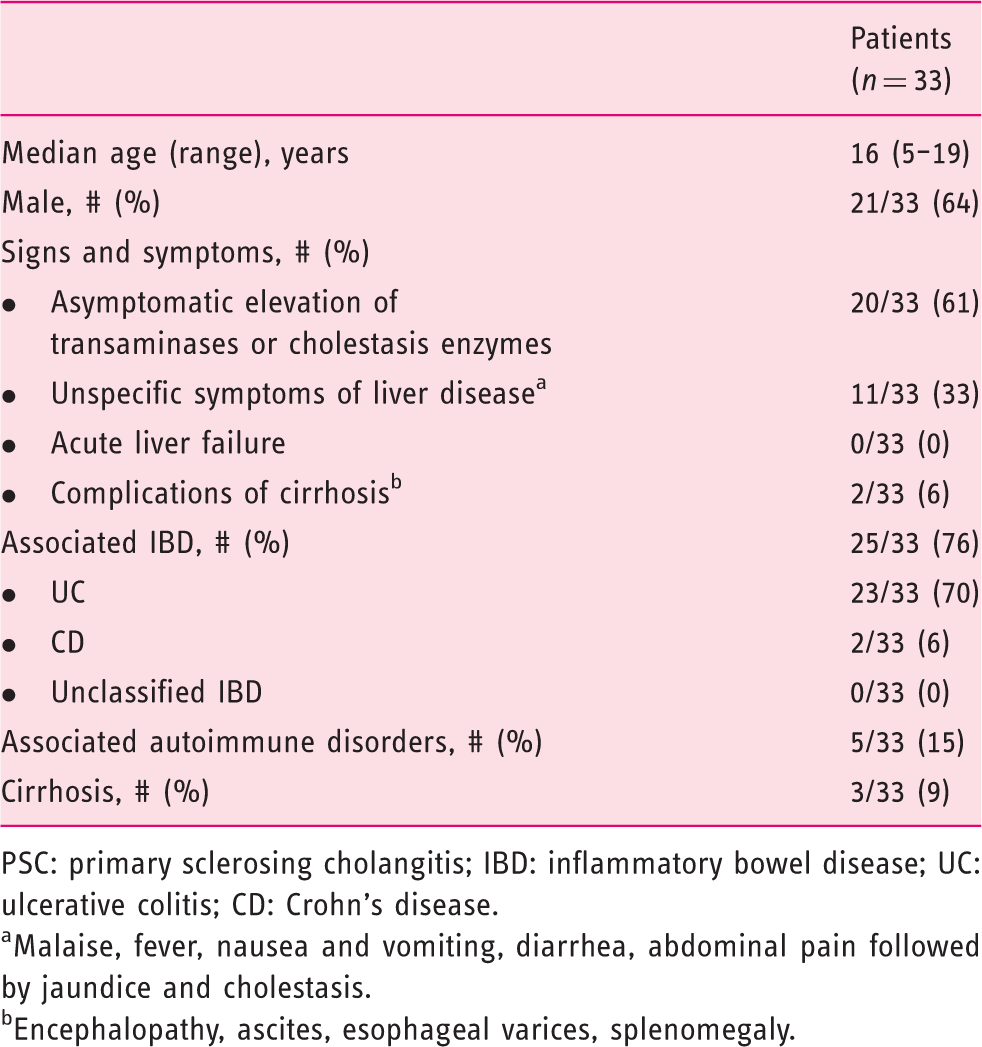
PSC: primary sclerosing cholangitis; IBD: inflammatory bowel disease; UC: ulcerative colitis; CD: Crohn’s disease.
Malaise, fever, nausea and vomiting, diarrhea, abdominal pain followed by jaundice and cholestasis.
Encephalopathy, ascites, esophageal varices, splenomegaly.
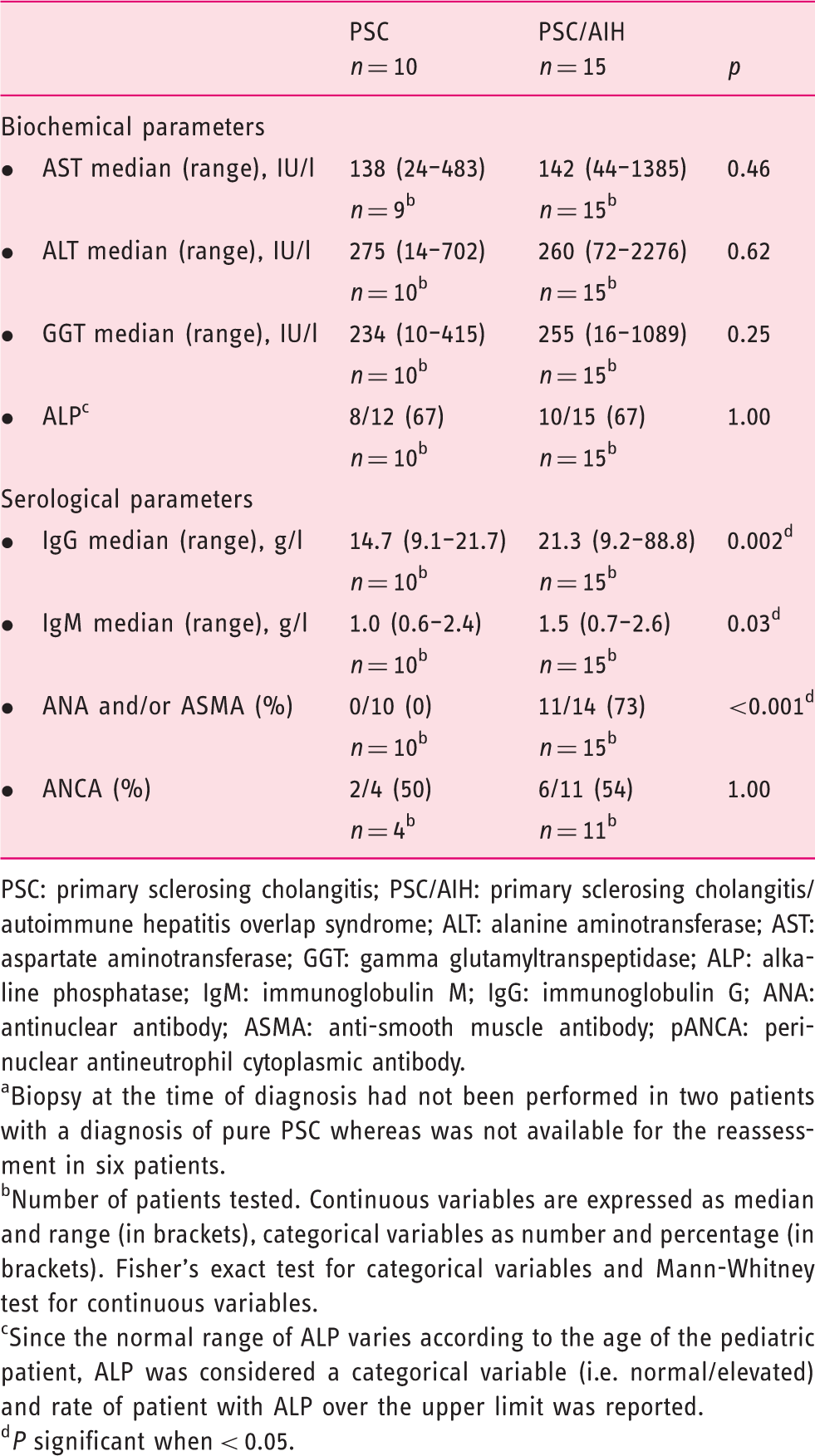
The biochemical and serological parameters at the time of diagnosis of PSC and PSC/AIH pediatric patients after the disease reassessment (n = 25 a ).
PSC: primary sclerosing cholangitis; PSC/AIH: primary sclerosing cholangitis/autoimmune hepatitis overlap syndrome; ALT: alanine aminotransferase; AST: aspartate aminotransferase; GGT: gamma glutamyltranspeptidase; ALP: alkaline phosphatase; IgM: immunoglobulin M; IgG: immunoglobulin G; ANA: antinuclear antibody; ASMA: anti-smooth muscle antibody; pANCA: perinuclear antineutrophil cytoplasmic antibody.
Biopsy at the time of diagnosis had not been performed in two patients with a diagnosis of pure PSC whereas was not available for the reassessment in six patients.
Number of patients tested. Continuous variables are expressed as median and range (in brackets), categorical variables as number and percentage (in brackets). Fisher’s exact test for categorical variables and Mann-Whitney test for continuous variables.
Since the normal range of ALP varies according to the age of the pediatric patient, ALP was considered a categorical variable (i.e. normal/elevated) and rate of patient with ALP over the upper limit was reported.
P significant when < 0.05.
Liver histology at the time of diagnosis
Histologic features on the liver biopsy at the time of diagnosis of PSC and PSC/AIH pediatric patients after the disease reassessment (n = 25a).
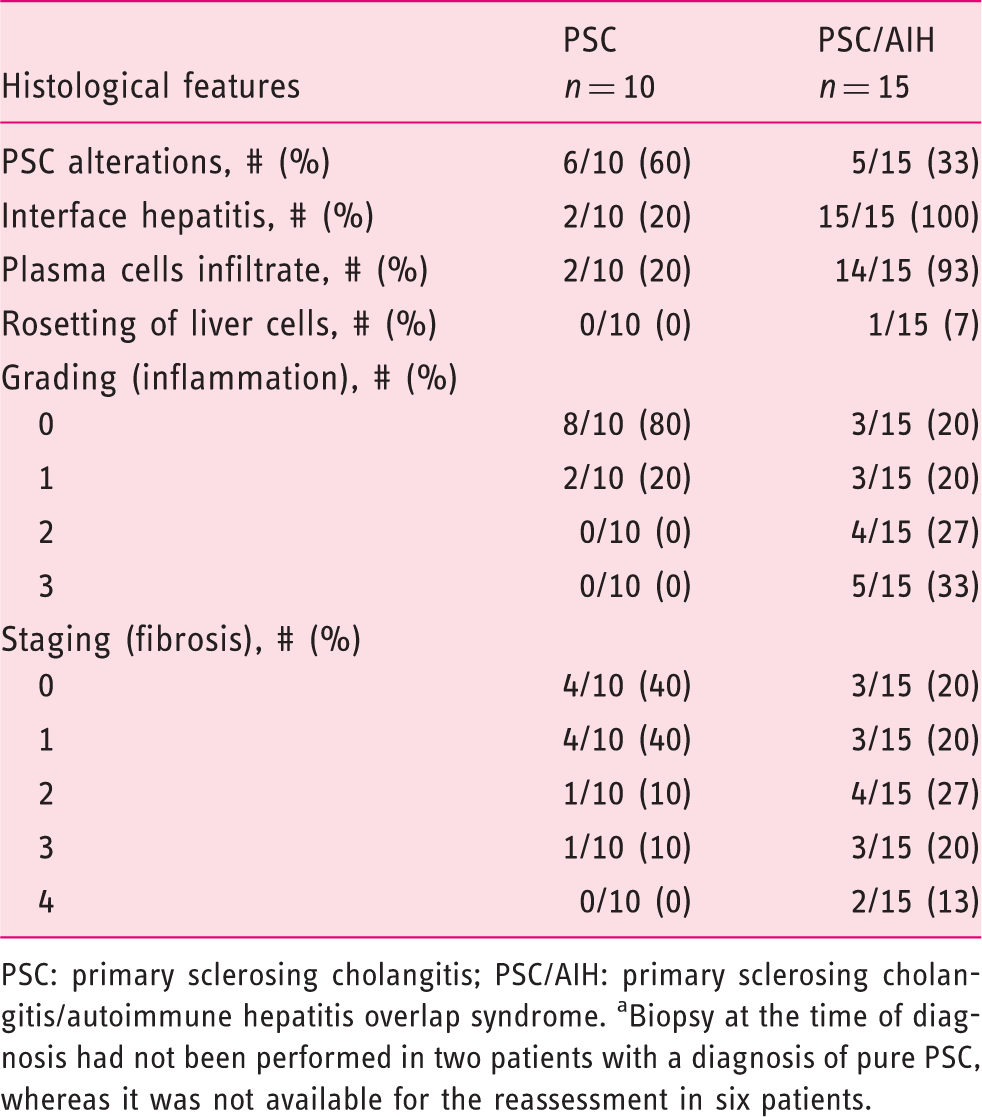
PSC: primary sclerosing cholangitis; PSC/AIH: primary sclerosing cholangitis/autoimmune hepatitis overlap syndrome. aBiopsy at the time of diagnosis had not been performed in two patients with a diagnosis of pure PSC, whereas it was not available for the reassessment in six patients.
ERC findings at the time of diagnosis
At the time of diagnosis, 12 patients (36%) had intra- and extra-hepatic disease, 21 patients (64%) had only intra-hepatic disease; isolated extra-hepatic disease was not present in any patients. No case with small-duct PSC was found. The modified Amsterdam PSC score at the time of diagnosis is shown in Table 1.
Treatment
During the follow-up, 30 out of 33 patients (91%) were on UDCA at a daily dosage of 20 mg/kg. One patient underwent a colectomy one year after the diagnosis of PSC for severe UC. Twelve patients with a diagnosis of PSC/AIH (seven with associated IBD) received corticosteroids and/or azathioprine during the follow-up; in three of them IBD was diagnosed at the same time as PSC/AIH, whereas in four it came before the diagnosis of PSC/AIH (two of them had undergone a colectomy for severe colitis). The seven patients with AIH overlooked at the time of diagnosis were on UDCA, and six of them had associated IBD (four UC and two Crohn’s disease [CD]) diagnosed before (n = 4) or at the same time as liver disease (n = 2). One of these six patients underwent a colectomy, but none of the others received corticosteroid and/or immunosuppression because of a mild clinical course of the intestinal disease.
Clinical course and prognosis
The long-term clinical outcome is shown in Figure 2. The median follow-up was nine years (range: 2–20). At the last follow-up, all the patients were alive. No malignancy was diagnosed during the follow-up period. During follow-up, a repeated ERC was available in 27/33 patients (82%). Initially, a short papillotomy was performed in 15 (42%) procedures. Dilation of the bile ducts was performed in eight (24%): in two with intra-hepatic and in six with extra-hepatic disease. Biliary stenting was not performed in any of the patients. The median number of ERCs per patient performed during the follow-up period was three (range 1–8). The modified Amsterdam PSC score showed a significant progression of intra-hepatic disease in 12 (36%) patients (p = 0.01), but not of extra-hepatic disease (p = 0.85). At the end of the study, 29 patients (88%) were still non-transplanted Long-term clinical outcome of patients with pediatric-onset PSC or PSC/AIH.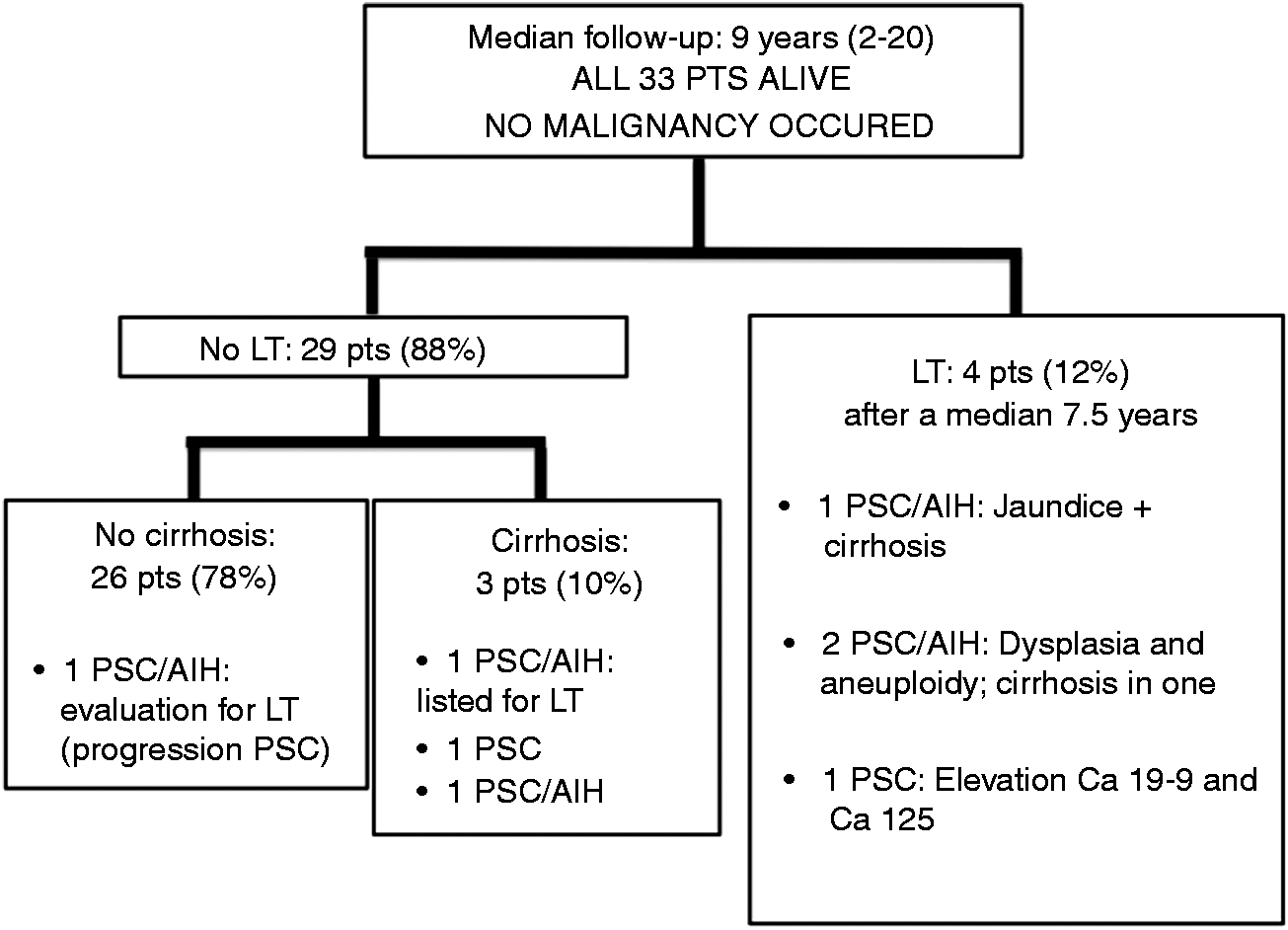
Discussion
Statement of principal findings
To our knowledge, this is one of the longest follow-up studies investigating the clinical course and prognosis of pediatric-onset PSC documented systematically with ERC imaging with brush cytology. The main finding of this study was that both PSC and PSC/AIH with pediatric onset seem to have a relatively good prognosis until early adulthood. In our series, no malignancy occurred
Presentation at the time of diagnosis
PSC affected mostly boys with an onset in the second decade of life, as previously reported in the literature.6,7,12 The asymptomatic elevation of liver enzymes (transaminases and/or cholestasis) was the most common presentation
Similar to three other large series,6–8 most of the children (76%) had associated IBD, UC being the most common (70%). So far, all studies have shown that PSC and IBD do not have a common genetic background,13,14 supporting the paradigm of a unique phenotype of PSC-IBD. 15 As previously reported, the majority of our patients had mild pancolitis, 15 and IBD was diagnosed at the same time as PSC or before the liver disease. 6 The effect of immunosuppressive treatment for IBD on the outcome, especially of PSC/AIH patients, is difficult to study, but it is probably low. Firstly, in about 50% of the patients IBD was diagnosed at the same time as PSC or PSC/AIH. Secondly, most of the patients in the current cohort had only mild intestinal disease without the need of corticosteroids and/or immunosuppression during their follow-up.
In the current series, most of the patients (64%) had only intra-hepatic involvement, and no patients presented isolated extra-hepatic disease. Feldstein et al. found only intra-hepatic PSC in about 40% and only extra-hepatic in 2% of the children. 6 In this study, all the patients have been followed up with ERC, which is an invasive procedure associated with complications such as pancreatitis, bleeding, perforation, and cholangitis,16–18 especially after papillotomy. 19 However, the complications rate might be low in a high-volume center. 20 In HUCH, more than 1200 ERCs per year are performed, and in PSC patients only a short papillotomy is usually performed in order to facilitate the following cannulations and reduce the risk of post-ERC pancreatitis. In recent series of our unit consisting of 441 patients with PSC undergoing ERC, 7% had pancreatitis, of whom two patients required hospitalization for two weeks, and six patients developed cholangitis (1.6%). 21 Recently, MRI was reported as an accurate, safe and cost-effective tool in the diagnosis of PSC, although false-negative and/or false-positive cases do occur, 9 and therefore the role of MRI in PSC diagnostics needs further evaluation.
Treatment, clinical course and prognosis
During the follow-up, most of our children received UDCA, and all of those with an original diagnosis of PSC/AIH also immunosuppression. The real impact of the pharmacological therapy on the outcome of PSC and PSC/AIH patients is still debated.5–7 A high dose of UDCA is associated with severe adverse events. 22 In a single study, treatment with UDCA and immunosuppressants had a minor impact on survival in patients with pediatric-onset PSC and PSC/AIH, 6 but in another study such treatment showed a good effect on the clinical course. 7 A few studies have suggested a clinical benefit of treatment with vancomycin in PSC children with IBD, 23 and especially those without cirrhosis. 24 No patients in our series were taking this antibiotic.
Cirrhosis was present in less than 10% of the children at the time of diagnosis
Overall, LT was performed in approximately 12% of the patients after a median time of 7.5 years from the diagnosis of liver disease. Interestingly, in this study the rate of transplanted patients was lower compared to the 17–21% reported in other studies with a similar follow-up, also showing a shorter time free of LT.3,6,7 So far, none of our patients have shown recurrence of PSC and/or AIH in the graft, although this has been reported both in adults 25 and in children. 6
We did not identify cases of cholangiocarcinoma after a median follow-up of nine years. This is in line with two single-center pediatric studies with somewhat shorter follow-up that reported no cholangiocarcinoma.6,7 Conversely, in one population-based study, cholangiocarcinoma was reported in approximately 7% of pediatric cases. 3 We speculate that the follow-up protocol performed in our center—which is based on endoscopic (i.e. ERC), radiologic (i.e. MRI/CT) and pathologic (i.e. cytology and flow-cytometry) findings—might help to select patients for optimal timing for LT. Interestingly, recurrent severe biliary dysplasia with aneuploidy on cytology samples indicated LT, which probably have prevented the occurrence of malignancy. However, American 2 and European 1 guidelines recommend that ERC with brush cytology and/or fluorescence in situ hybridization (FISH) should not be considered as an evidence-based screening method for cholangiocarcinoma in PSC patients. Moreover, specific guidelines on diagnosis and follow-up of PSC and PSC/AIH in the pediatric population are still lacking. Recently, Barr Fritcher et al. reported that FISH might detect patients with polysomic cells in brushing samples before other techniques, identifying those having a higher risk of cholangiocarcinoma. 26 New prospective, multicenter, long-term follow-up studies are warranted in order to establish the best diagnostic approach in these patients.
Strengths and limitations of this study
Strengths of this study are: 1) being the second study conducted in Europe on the clinical outcome of pediatric-onset PSC, 2) the number of patients included, 3) the disease systematically proved in all the patients with ERC and 4) the long follow-up. Limitations are: 1) the retrospective design as in many other studies on pediatric PSC,3,6,7 2) the detection bias (i.e. the number of patients missed) as well as the referral bias (i.e. diseases severity), although these biases should be low as in Finland most pediatric patients with suspected PSC are referred from all over the country to HUCH for diagnosis and follow-up, 3) the reported misclassification bias of overlap with AIH in a few patients without liver biopsy. 6
Conclusions
As in adults, PSC in children is frequently associated with IBD, but the therapy of IBD did not seem to be a major determinant of the clinical course and outcome of the liver disease. Both PSC and PSC/AIH may present with cirrhosis already at the time of diagnosis, highlighting the importance of an earlier diagnosis of the disease. Importantly, both PSC and PSC/AIH seem to have a relatively good prognosis in the majority of pediatric patients until early adulthood. Disease progression is, however, observed in about one-third of patients
Footnotes
Funding
This work was supported by the Sigrid Jusélius Foundation, Pediatric Research Foundation, Helsinki University Central Hospital Research Fund.
Conflict of interest
None declared.