
Abstract
Background
Barrett’s esophagus (BE) is rare in African Americans (AA). However, the risk difference magnitude in histologic BE prevalence between AA and non-Hispanic whites (nHw) has not been quantified to date.
Objective
The objective of this article is to determine the degree of histologic BE risk difference between AA and nHw.
Methods
PubMed, Web of Science and EMBASE were searched for studies reporting histologic BE in AA/nHw for inclusion. Pooled odds ratios (ORs) with risk estimates of histologic BE occurrence between AA/nHw were calculated along with 95% confidence intervals (CIs). Forest plots were used to quantify heterogeneity. Funnel plots and the Cochrane Collaboration Risk of Bias tool were used to assess bias risk.
Results
Eight studies reported BE histologic confirmation in AA/nHw. Analysis demonstrated a nearly 400% increased histologic BE risk in nHw patients compared to AA (OR 3.949, 95% CI 3.069–5.082). In the model without the case-control study, histologic BE risk remained elevated at approximately 360% in nHw compared to AA (OR 3.618, 95% CI 2.769–4.726). Heterogeneity was not present in either model. Risk of bias was significant.
Conclusions
Histologic BE risk is elevated in nHw by 3.6–4 times compared to AA. Investigation into understanding any clinical, molecular or genetic mechanisms underlying this risk disparity is warranted.
Key summary
Summarize the established knowledge on this subject:
Barrett’s esophagus (BE) is associated with progression to esophageal adenocarcinoma (EAC). Risk factors for BE include duration of gastroesophageal reflux disease (GERD), male sex, obesity, and cigarette smoking. Helicobacter pylori colonization, regular aspirin, proton pump inhibitor or nonsteroidal anti-inflammatory use and African American (AA) ethnicity are associated with decreased risk. Limited data exist regarding degree of risk difference by ethnicity of histologically confirmed BE. What are the significant and/or new findings of this study?
Non-Hispanic whites (nHw) have a 3.6–4 fold increased risk of histologically confirmed BE compared to AA. These findings quantify the observation of increased BE in nHw and can be used to further enhance cost-effectiveness studies in BE screening. Continued exploration to determine factors explaining the disparity in BE formation and/or presence seen between United States ethnic groups is required.
Introduction
Barrett’s esophagus (BE) is a metaplastic alteration of the distal esophageal epithelium, following injury caused by reflux of acid and bile, in which one kind of fully differentiated cell replaces another. 1 This change, called specialized intestinal epithelium (SIM), is present in up to 1.6% of the general population and 5%–13% of patients having endoscopy for reflux symptoms.2,3 BE is associated with a 0.12%–0.5% yearly risk of progression to esophageal adenocarcinoma (EAC), which is an aggressive cancer whose incidence has increased eight-fold in the United States (US) over the past several decades.4–9 Risk factors for BE include non-Hispanic white race (nHw), male sex, obesity, and gastroesophageal reflux disease (GERD) while Helicobacter pylori colonization and regular aspirin or nonsteroidal anti-inflammatory drugs reduce risk.2,10–21
Although investigators have recently increased their focus on BE in US multiethnic populations, the studies published to date have not featured large samples. In addition, the difference in degree of histologic BE prevalence risk between African Americans (AA) and nHw has not been determined to date. To quantify and confirm the magnitude of difference in histologic BE prevalence between AA and nHw, we conducted a meta-analysis combining the results of published studies reporting the prevalence of histologically proven BE in AA and nHw, thus providing a quantitative estimate of the risk reduction for histologically proven BE associated with AA race/ethnicity.
Methods
Search strategy
A systematic literature search was conducted of PubMed, Web of Science, and EMBASE databases from 1997 to 2014 to identify all relevant articles on histologically proven BE in AA and nHw. Key words used in the search included a combination of “Barrett esophagus,” “ethnicity,” “race,” “African American,” and “non-Hispanic white.” The search was restricted to studies in human participants published in the English language in peer-reviewed journals. Two authors (AA and KJV) independently reviewed the title and abstract of identified studies in the primary search to exclude those that did not address the research question of interest, based on preselected inclusion and exclusion criteria (details below). Full text of remaining articles were then examined to determine if it contained relevant information. Any discrepancy of article selection was resolved by consensus. Finally, bibliographies of selected articles as well as systematic and narrative review articles on the topic were manually searched for additional articles. Each included study was weighted according to its inverse variance.
Study inclusion criteria
All eligible studies had to satisfy the following inclusion criteria: (a) histologic confirmation of BE (presence of intestinal metaplasia either with or without goblet cells), (b) reported AA and nHw ethnicity for patients/participants, (c) adequate data available to provide an estimate of effect measure (odds or risk ratio), (d) was original, and (e) used the individual as the unit of analysis. We excluded studies that: (a) did not have histologic confirmation of BE and (b) consisted of highly selected cohorts (referral to a single individual).
Data extraction/statistical analysis
Data were extracted from the relevant studies specifically looking at histologic diagnosis of BE among nHw and AA. Each study was weighted according to its inverse variance. The distribution of effect measures was examined using visual and tabular displays as well as tests of homogeneity to reveal variation in the risk estimates of histologic BE occurrence between AA and nHw using a DerSimonian-Laird random-effects method. Odds ratio (OR) was calculated along with 95% confidence interval (CI) estimates. Forest plots were created and summary OR with 95% CI of histologic BE was reported. Heterogeneity was quantified using the I2 statistic. A sensitivity analysis was performed comparing results with and without case-control studies. Software used to conduct the meta-analysis was the open source OpenMetaAnalyst platform. We used Excel to create a funnel plot according to number of patients and risk estimate for each study. Funnel plots are reported according to sample size and relative risk estimate. Funnel plots according to standard error and relative risk estimate were also created, yielding similar results. The Cochrane Collaboration Risk of Bias Tool was used to assess the quality of the studies. 22
Results
Search results
Our search strategy in PubMed, Web of Science, and EMBASE identified a total of 129 unique articles. On the basis of pre-specified inclusion and exclusion criteria, a total of eight studies were selected for review (Figure 1 and Table 1). These studies had a total of 76,574 patients for analysis.
Study flow and selection. Studies included in the analysis. BE: Barrett’s esophagus; AA: African American; nHw: non-Hispanic white; US: United States.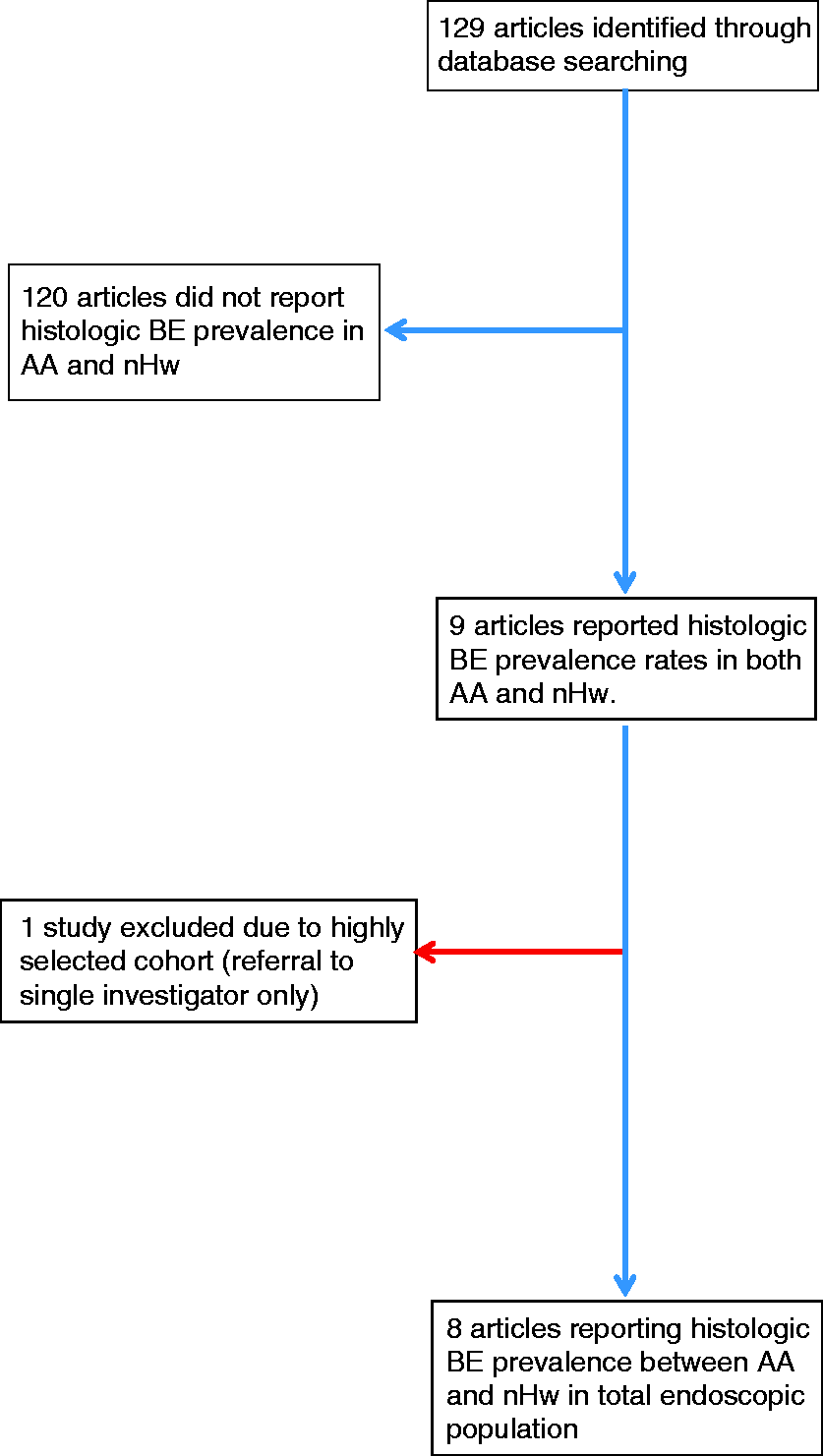
Overview of the included studies
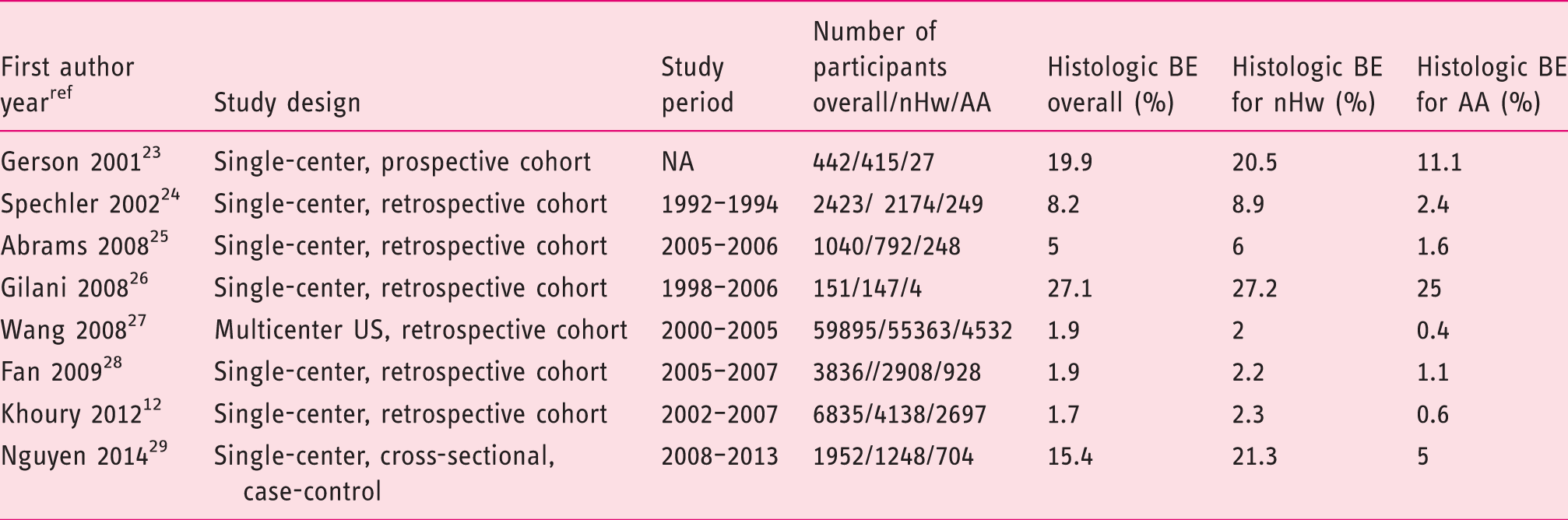
The number of individuals evaluated in each investigation ranged from 151 to 59,895 (Table 1).12,23–29 AA comprised 12.3% (N = 9389) of the overall patient population. Seven of eight studies reported the study period.12,24–29 The oldest was conducted in 1992–1994 and published in 2002. 24 One study was from the national endoscopic database, comprising a combination of academic, community and Veterans Affairs (VA)/military centers. 27 Of the remaining seven reports, four were from academic medical centers in Massachusetts, New York, Florida and Texas, two from VA centers in Texas and Arizona with the final study a combination of an academic medical center and VA in California.12,23–26,28,29 The largest study overall was from the national endoscopy database and the largest single-center report had 6835 participants.12,27
Prevalence of histologic BE
Overall prevalence of histologic BE was 2.6% in the eight studies analyzed. The lowest overall study prevalence was 1.7% (115 of 6835 12 ) while the highest was 27.1% (41 of 151 26 ). For nHw, the overall study prevalence histologically confirmed BE was 2.9% (1924 of 67,185) while this was 1% for AA (95 of 9389). The lowest study prevalence for nHw was 2% (1132 of 55,363 27 ) and the highest 27.2% (41 of 147 26 ). For AA, the lowest study prevalence was 0.4% (20 of 4532 27 ) and highest was 25% (one of four 26 ).
Quantitative/qualitative data analysis
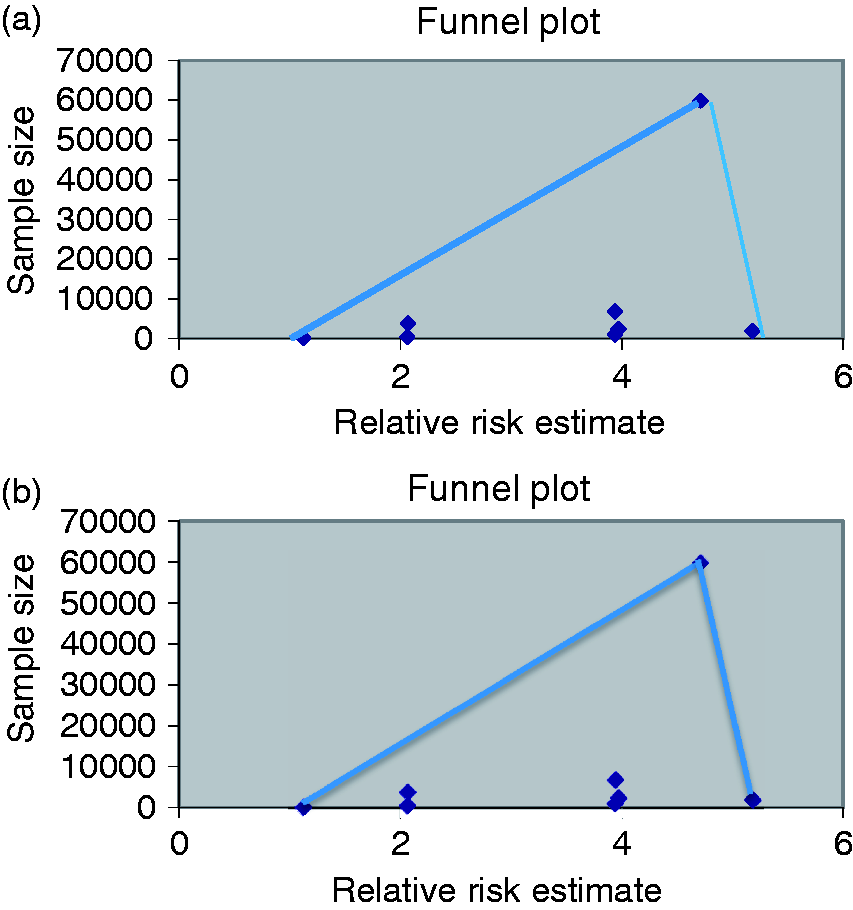
Analysis including the Nguyen study demonstrated a nearly 400% increased risk for nHw patients having histologic BE compared to AA (OR 3.995, 95% CI 3.031–5.266, Figure 2(a)). In the random-effects model without the case-control study, the risk of histologic BE remained elevated at approximately 360% in nHw compared to AA (OR 3.618, 95% CI 2.769–4.726, Figure 2(b)). Heterogeneity was not present in either model (case control included I2 = 17%, p = 0.296, Figure 2(a); without case control I2 = 0%, p = 0.42, Figure 2(b)). Funnel plots (Figure 3(a) and (b)) were constructed and asymmetry around the reported point estimates was noted. This suggests significant publication bias. In assessing the risk of bias using the Cochrane Collaboration Risk of Bias Tool, the currently available studies lacked a randomized, blinded design.
Pooled odds ratios for histologic Barrett’s esophagus between non-Hispanic whites and African Americans. (a) all studies; (b) excluding Nguyen study.
29
Funnel plots corresponding to Figures 2(a) and 2(b), respectively.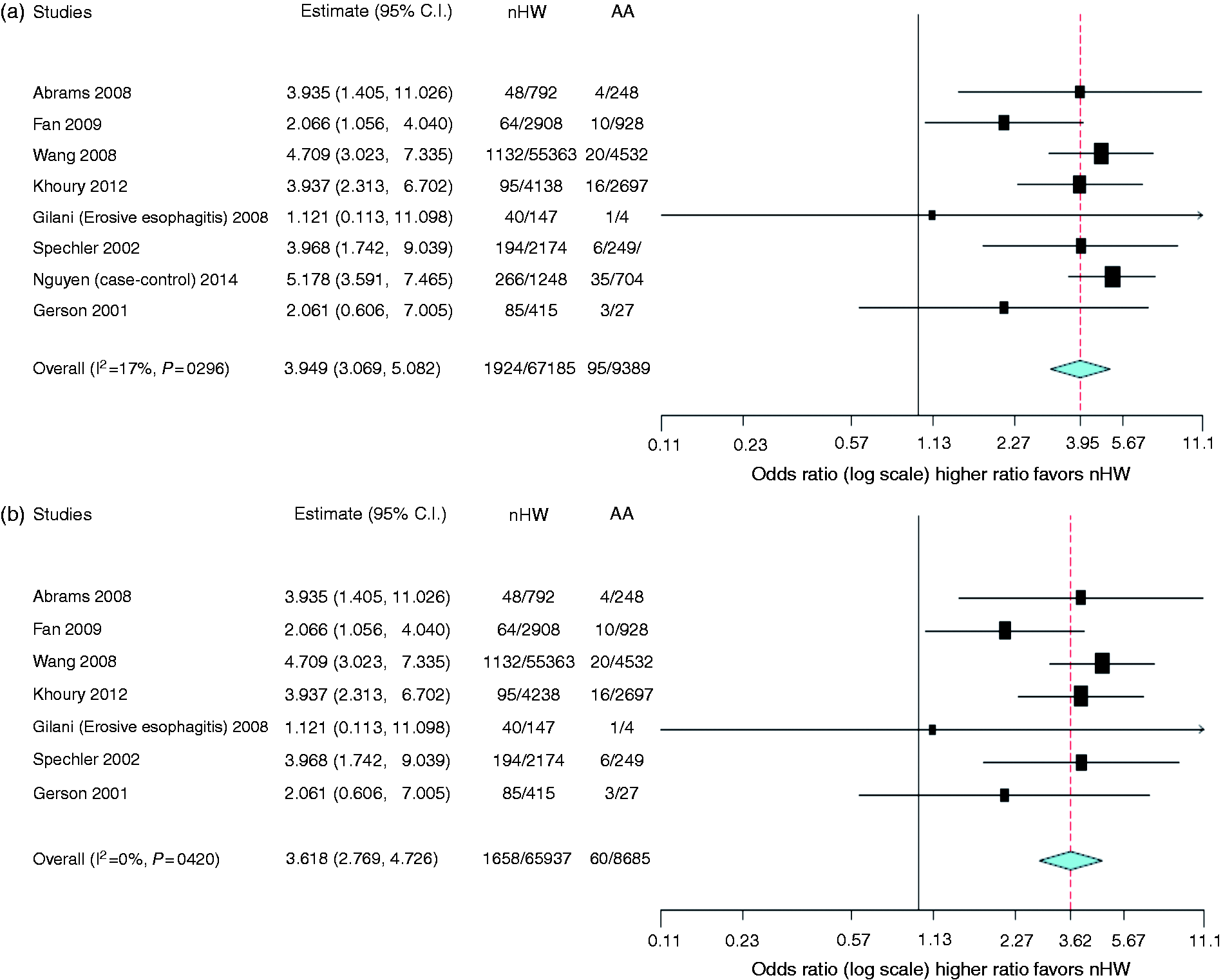
BE length, sex distribution, and age
Assessment of differences in length as well as age and sex distribution of AA and nHw BE patients was attempted. Unfortunately, these items were inconsistently reported in the included studies, preventing any opportunity to perform meta-analysis. Length of BE both in AA and nHw was reported in three included studies.12,25,29 However, in two investigations, BE length was missing in 13 AA and three nHw patients, respectively.25,29 Despite these missing data from the reports above, long-segment BE (LSBE) was present more frequently in nHw than AA (nHw 35.1% vs AA 14.5%, p < 0.002) while AA had short-segment BE (SSBE) more frequently that nHw (AA 85.5% vs nHw 64.9%, p < 0.002). Three studies reported sex distribution of BE cases.12,26,29 However, two of these investigations were from VA centers limiting assessment by sex.26,29 The single community-based report revealed more males then females with BE both in AA and nHw. 12 Interestingly, a trend was seen between AA and nHw regarding the degree of male predominance in histologic BE, with nHw have a greater male percentage than AA (p < 0.08). Finally, mean age of AA and nHw BE patients was reported by only two groups.12,29 No difference in age between AA and nHw BE patients was observed in either investigation.
Discussion
It is well recognized that nHw ethnicity is a risk factor for histologically established BE compared to AA.12,23–29 However, the degree of risk difference between AA and nHw has not been determined to date. The aim of the present investigation was to provide a quantitative estimate of the risk variation between these two racial/ethnic groups for histologically proven BE. The results indicate that histologically confirmed BE among more than 67,000 nHw and 9300 AA patients occurred 3.6 to 4 times more frequently in nHw than AA. This now quantifies the risk difference for histologically confirmed BE between these two ethnic groups as well as enhances future cost-effective analysis in screening for BE.
Reasons for such a risk variance between nHw and AA observed in the meta-analysis remain unclear at present. Clinical risk factors assessment between AA and nHw with BE was reported in two of the eight studies included in the analysis.12,29 In one, from a multiethnic histologic BE cohort, only age, sex, and hiatal hernia were assessed between ethnic groups. 12 No difference was observed in any of those parameters between AA and nHw. Nguyen and colleagues evaluated clinical factors for BE at a Texas VA facility and reported that nHw with histologic BE had a higher waist-to-hip ratio than AA BE cases. 29 However, no difference was seen between AA and nHw histologic BE groups in age, sex, GERD symptoms, hiatus hernia, proton pump inhibitor (PPI)/nonsteroidal anti-inflammatory drug (NSAID)/aspirin/statin use as well as cigarette and alcohol use. Infection with H. pylori was assessed by only one group at a VA institution, with AA having higher rates of infection compared to nHw. 29 It is well known that H. pylori infection is associated with a decreased risk of BE. 30 The prevalence of H. pylori is higher among AA compared to nHw and this factor could affect differences observed in BE between ethnic groups. 31
However, there are no data evaluating H. pylori prevalence in the overall endoscopic population simultaneously in any histologic BE study included in the meta-analysis.
Evaluations have recently occurred attempting to determine BE predisposition within the genome. At present, eight loci have been identified by genome-wide association studies associated with BE/EAC risk. 32 Unfortunately, assessment by ethnicity has not occurred to date. If ethnic variation of the BE/EAC risk loci is found to exist, then improved BE-preventive and -therapeutic efforts can be targeted to those at greatest risk for development of EAC.
Our meta-analysis had a number of strengths. First, a systematic literature search was performed using well-defined inclusion criteria to eliminate studies that were redundant or had significant referral bias. Second, studies were included in the analysis only if all patients with BE had histologic confirmation, excluding any opportunity for misclassification bias. Third, minimal heterogeneity was observed in either analysis model. This was most evident in the simulation not using the case-control study but even with inclusion of that investigation, heterogeneity remained acceptable (Figure 2).
However, the present study had limitations. First, this meta-analysis, like many performed, is subject to the individual biases of each study included. Second, there was significant variation in the prevalence of histologically confirmed BE among the included studies both in AA and nHw. This occurred among both groups and ranged from 2% to 27.2% in nHw and 0.4% to 25% in AA. Of note, highest prevalence rates were seen in AA and nHw among studies with smaller cohorts and from a VA hospital.23,26,29 Third, clinical (GERD symptom frequency, hiatal hernia and H. pylori infection rates, obesity) and social factors (smoking frequency or alcohol/medication use) known to affect BE prevalence were inconsistently reported, limiting any ability to address the effect from these items individually.33–35 Fourth, items such as BE length, age, and sex distributions were inconsistently reported, limiting any ability to assess via meta-analysis. Finally, the funnel plots (Figure 3(a) and (b)) support the role of publication bias. In assessing the risk of bias using the Cochrane Collaboration’s tool, the studies available tend to be nonrandomized and non-blinded. This makes them subject to reporting bias. Thus, potential under-reporting of negative studies may be possible.
In summary, we have identified a large disparity in histologic BE prevalence between AA and nHw and quantified the risk difference (3.6–4 times higher in nHw than AA) between these ethnic groups. The results should be tempered by the limited number of studies available looking at the dimension of BE according to nHw and AA race. Future investigations should confirm these findings. In addition, continued assessment of clinical factors along with genetic mechanisms underlying this risk disparity are required to improve BE-preventive and -therapeutic efforts for maximization of benefit, reducing EAC incidence.
Footnotes
Acknowledgments
Author contributions are as follows: Ahmad Alkaddour: planning, collecting, and interpreting data and drafting and editing manuscript; Carlos Palacio: study design, interpreting data, statistical analysis, and editing manuscript for intellectual content; and Kenneth J. Vega: planning, collecting, and interpreting data and editing manuscript for intellectual content. All authors approved the final version of the manuscript.
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethics approval
This research did not require institutional review board approval as it was a meta-analysis of existing data in the literature.
Informed consent
Not required for this article.