
Abstract
Background
Eosinophilic esophagitis (EoE) affects health-related quality of life (HRQoL). Data on determinant factors and the influence of dietary interventions are scarce.
Objective
The objective of this article is to evaluate factors influencing HRQoL in adult EoE patients.
Methods
We conducted a multicenter observational, cross-sectional study. A validated Spanish version of the self-administered Adult Eosinophilic Esophagitis Quality of Life (EoE-QoL-A) questionnaire and specific surveys were used. Multiple linear regression was used to identify and quantify determinant factors of HRQoL.
Results
Responses provided by 170 patients were assessed (73.5% male; mean age 33.5 ± 11.4 years). Overall mean score for the EoE-QoL-A index was 1.4 ± 0.8, with no differences between patients on dietary or pharmacological therapy (1.82 ± 0.8 vs. 1.62 ± 0.8; p = 0.132). Disease anxiety showed the highest mean score (2.13 ± 0.9 points), followed by choking anxiety (1.97 ± 1.1); social impact (1.77 ± 1.1), and diet/eating impact (1.68 ± 0.9). Emotional impact had the lowest rating (1.15 ± 0.9), and only with a significantly worse score in patients under dietary restrictions. Recurrent food impaction, a higher educational level, dietary interventions and symptom duration were all independent determinant factors significantly impairing HRQoL. Female gender and empiric elimination diets negatively influenced on diet/eating impact.
Conclusion
Recurrent food impaction, dietary interventions and symptom duration are the most important factors influencing the perception of HRQoL in adults with EoE.
Introduction
Eosinophilic esophagitis (EoE) is a chronic esophageal inflammatory disease, characterized clinically by symptoms related to esophageal dysfunction, and histologically by eosinophil-predominant inflammation.1,2 EoE affects children and young adults 3 and has rapidly grown over the past decade, especially in developed countries. 4 Presently, it represents the second leading cause of chronic esophagitis after gastroesophageal reflux disease (GERD) 5 and the main cause of dysphagia in children and young adults. 6
From a clinical point of view, predominant clinical manifestations in EoE are chronic dysphagia and food impaction in adult patients, whereas children usually present with food refusal, vomiting, GERD-like symptoms, abdominal pain and even failure to thrive. 1 Consequently, EoE may negatively affect the health-related quality of life (HRQoL) of patients and their families by causing emotional distress, limiting normal feeding and restricting social activities.7–9 Disease activity, as determined by the severity of symptoms and biological markers,10,11 as well as disease duration 8 have been demonstrated to affect patients HRQoL. Adult patients with dysphagia develop adaptive strategies to cope with chronic symptoms, including selective food avoidance, slow-paced eating and increased water drinking. 12 The frequent diagnostic delay in most EoE patients, usually of several years after the onset of initial symptoms, 13 also aggravates the disease. The duration of the untreated disease directly correlates with the presence of fibrostricturing findings in the esophageal lumen, including narrow-caliber esophagus and strictures.14,15
Currently, EoE is recognized as a particular form of food allergy, in which esophageal inflammation and symptoms remit after avoidance of exposure to potential food triggers.16,17 Dietary therapy constitutes a main pillar in the management of EoE patients, which is able to achieve and maintain remission in a high proportion of patients. 17 Like in other food allergies, long-term management of EoE may rely on avoidance of food triggers. As such, dietary restrictions may result in psychological burden for patients and their relatives that can result in stress, anxiety, and impairment of socialization, with a negative impact on their daily life. 18 However, the impact of food avoidance on QoL of patients with EoE has not been evaluated.
HRQoL constitutes one of the most important primary patient-reported outcome (PRO) measures for assessing an individual’s burden of any given chronic condition, and provides valuable information for developing interventions to promote the greatest possible well-being as well as a better optimization of health care resources. 19 Identifying the aspects that influence HRQoL in EoE might allow implementation of strategies to reduce the impact of the disease.
In this study we aimed (1) to determine for the first time the HRQoL in a representative sample of Spanish adults with EoE, and (2) to identity determinants of impaired HRQoL, including the effect of dietary restrictions.
Materials and methods
Study population and procedures
A prospective cross-sectional observational study was conducted in 2014 at eight different tertiary centers located in several regions of Spain. The diagnosis of EoE was based on esophageal dysfunction symptoms in conjunction with characteristic histopathological findings (≥15 eosinophils per high-power field) that persisted after an eight-week trial with proton pump inhibitor (PPI) therapy at double doses. 20 Male and female patients aged 18 years or older and consecutively recruited provided written informed consent to participate in the study. Demographic data including age, gender, education level, residence characteristics, as well as comorbidities, concomitant allergic disorders, EoE symptoms and current therapy, were collected in a standardized fashion.
QoL measures
The EoE-QoL-A is a validated instrument to measure QoL developed by Taft et al. specifically for adult patients with EoE. 21 The initial 37-item symptom inventory was later refined to a 30-item scale subsequently published by the same researchers. 22 A translated and validated Spanish version of this questionnaire 23 was used.
For the purposes of this study, 24 items applicable for all patients were scored, falling into five following subscales: eating/diet impact (four items), social impact (four items), emotional impact (eight items), disease anxiety (five items) and swallowing anxiety (three items). Six additional items were completed by patients undergoing elimination diet only (that were scored within the eating/diet impact subscale). The EoO-QoL-A score ranges from 0 (very good QoL) to 4 (very poor QoL) for every item. The final score was the weighted average of all QoL subscales, following previously used methods. 11
Statistical methods
Results for continuous variables are expressed as the mean and SD or as the median and interquartile range (IQR); qualitative variables are presented as absolute and relative frequencies. The χ2-test (Fisher’s exact test, where appropriate) or Student’s t-test (analysis of variance (ANOVA) test, where appropriate) were used to compare qualitative and quantitative variables, respectively. Spearman test was used for correlation analysis of nonparametric variables and Pearson test for parametric variables
Variables with a p value <0.1 in the univariable analysis were selected for the multivariable analysis. Variables were selected by backward selection. Multiple linear regression analysis with backward selection was used to model the relationship between the factors analyzed and QoL in EoE patients. Multiple lineal regression was performed for the overall series of patients for the EoE-QoL-A questionnaire score overall and within each subscale of it. The selection criterion of p < 0.1 was used for elimination of a variable. Analyses and summaries were carried out with the PASW statistical program (version 18.0; SPSS Inc, Chicago, IL, USA). A significance level of 0.05 was used throughout.
Results
Study participants
Demographic and clinical characteristics of adult patients with eosinophilic esophagitis.
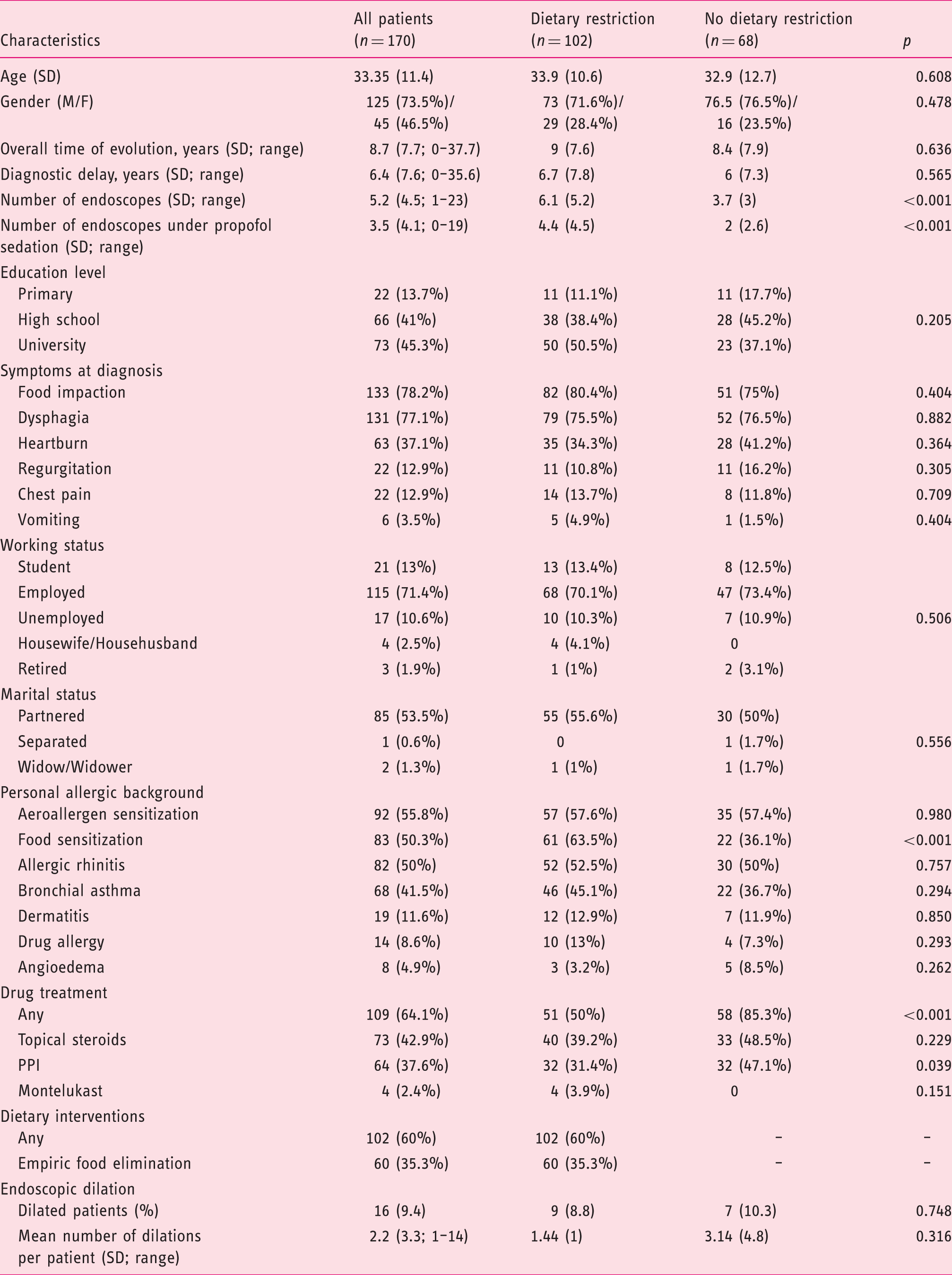
SD: standard deviation; M/F: male/female; PPI: proton pump inhibitors.
Regarding EoE treatment, 102 patients (60%) had been prescribed some kind of dietary restriction. No differences were observed in the demographic data (including educational level, employment or marital status, or size of the residence) between patients with or without dietary-based therapeutic interventions, despite a trend toward a lower QoL overall among patients under food restriction. Family and self-reported personal allergic background were similar in patients with and without dietary restrictions, except for the presence of associated food sensitizations that were more frequent in patients under food restriction-based treatment. Patients receiving dietary interventions underwent a significantly higher number of endoscopies, due to individual food reintroduction followed by endoscopy in responders to diet.
HRQoL levels
Mean quality of life score ± standard deviation (rank) in our series of 170 adult patients with eosinophilic esophagitis, determined by the Adult Eosinophilic Esophagitis Quality of Life (EoE-QOL-A) instrument, and differential impact in patients undergoing some kind of dietary restriction compared with those who were not.
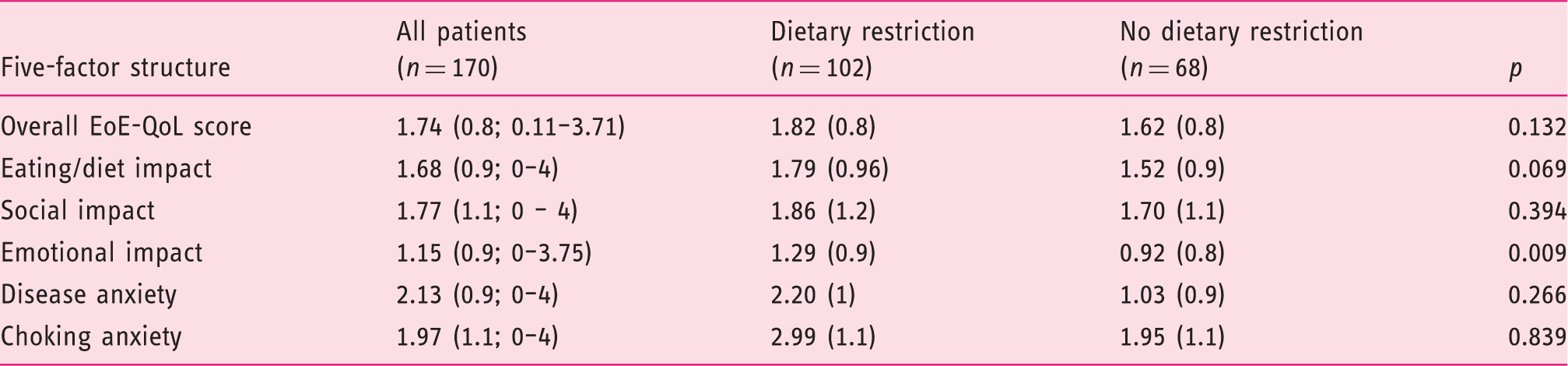
Likewise, no differences in HRQoL were observed between men and women (1.73 ± 0.8 vs. 1.8 ± 0.9, respectively; p = 0.617) nor among age groups in our sample.
As for the five dimensions included in EoE-QoL-A scale, Disease anxiety showed the highest mean score (2.13 ± 0.9), followed by choking anxiety (1.97 ± 1.1), social impact (1.77 ± 1.1) and diet/eating impact (1.68 ± 0.9). Emotional impact had the lowest rating, namely 1.15 ± 0.9. This was the only dimension that obtained a significantly higher impact in patients with dietary restrictions compared to those without (1.29 ± 0.9 vs. 0.92 ± 0.8, p = 0.09) (Table 2).
With regards to individual items, numbers 1 (“I have to be cautious about eating because I have EoE”), 15 (“I worry that EoE will get worse or turn into something else”), and 12 (“I worry about never identifying the cause of my EoE”) received the greater scores. In contrast, items 23 (“I feel isolated from others because of my EoE”) and 9 (“I find it embarrassing when I have to make special requests at restaurants”) received the lowest mean scores, as shown in Supplementary Table 1).
HRQoL determinants
Multivariate analysis by means of multiple linear regression between quality of life assessed by the Adult Eosinophilic Esophagitis Quality of Life (EoE-QoL-A) instrument and its five dimensions, with regard to all determinant factors.

CI: confidence interval. Boldface values denote the variables that reached statistical significance in the mutivariate analysis.
Regarding the Eating/diet impact dimension, female gender and a higher education level directly determined an impaired HRQoL. Having presented symptoms of food impaction and being under an empiric elimination diet were additional independent variables that were significantly associated with worse QoL perception.
The Social impact dimension of EoE was significantly determined by food impaction symptoms, drug treatment and length of disease evolution (all with p < 0.05). An increased Emotional impact of EoE was strongly determined by a higher educational level, EoE symptoms (including both food impaction and regurgitation) and the need of therapy for EoE (including food restriction, drug therapy and esophageal dilation, the first two reaching statistical significance).
Disease anxiety was significantly worse among patients with symptoms of food impaction and regurgitation, drug treatment and dietary restriction, and length of disease evolution. Finally, having experienced food impaction was the only independent factor that determined choking anxiety.
Discussion
The present study assessing HRQoL in adult EoE patients shows that EoE symptoms at diagnosis (specially food impaction), length of disease evolution, therapies for EoE and patients’ characteristics are the major determinants for this PRO measure. They all contribute in a different way to each one of the five dimensions resulting in the overall EoE-QoL-A score. Although recurrent food impaction significantly affected most of the EoE-QoL-A dimensions, female gender exclusively affected the eating/diet impact dimension.
Our research reinforces symptoms as a strong determinant for disease-specific HRQoL, as previously shown in a recent research, 11 that assessed overall EoE symptoms by measured with the Eosinophilic Esophagitis Activity Index (EEsAI) symptoms score. The EEsAI score is a seven-item instrument that derives five components of the overall score (frequency of trouble swallowing, duration of trouble swallowing, swallowing-associated pain, the visual dysphagia question score and the avoidance, modification and slow eating score), providing a total score ranging from 0 (inactive EoE) to 100 points (very active EoE). 12 Because the EEsAI does not assess the specific symptoms referred to by patients, our research adds to the current knowledge that certain specific symptoms at diagnosis, including food impaction and regurgitation, significantly contributed to the perception of HRQoL by adult EoE patients. Additionally, a long-standing duration of symptoms, defined as the length of time from the onset of initial symptoms of EoE to the moment of answering the questionnaire, even before the effective diagnosis of the disease, was significantly associated with worse HRQoL scores, significantly affecting disease anxiety, social impact and overall EoE-QoL-A score. A similar association has also been shown in patients with celiac disease, for which long-standing symptoms and a previous diagnosis of functional disorders were associated with worse HRQoL.24,25 In fact, a diagnostic delay of up to six years from the onset of symptoms is commonly recognized in EoE, both in children and adults.13,15 Based on these results, early diagnosis of the disease may help in resolving long-lasting QoL impairments in EoE.
Adult patients on a dietary-based therapy for EoE did not exhibit worse EoE-QoL-A overall scores compared to those who were receiving drugs for EoE. These data are conflicting with recent results in children with EoE who were assessed with the PedsQL™ EoE module: Children under diet-elimination therapy exhibited worse QoL scores, compared to those with no restrictions, reaching statistical significances both in child self-reported and parent proxy-reported subscales. 26 Differences in the capacity of adapting or even accepting food restriction as a relevant measure to improve EoE may explain these differences between children and adults. However, our findings show that dietary restrictions led to a significantly worse emotional impact as compared to nondietary exclusions (p = 0.009), but this fact seemed not to contribute to the overall HRQoL perception. Previous studies have demonstrated that patients under dietary restriction usually exhibit an impaired QoL compared to healthy controls, as documented in several disorders, including immunoglobulin (Ig)E-mediated food allergy27–29 and celiac disease. 30 In addition, numerous studies in pediatric and adult celiac patients have repeatedly shown that a gluten-free diet achieves not only symptom relief, but also improvements in HRQoL.30–33 We did not evaluate the efficacy of dietary intervention in every patient who participated in our survey, and studies evaluating this issue are currently lacking. It is tempting to speculate whether identification and long-term exclusion of individual food triggers could also lead to improvements in HRQoL, as suggested in a recent study that assessed EoE with a nonspecific instrument. 9
Our study analyzed all determinant factors for each of the scores constituting the five subscales that integrate the EoE-QoL-A questionnaire. Among them, food impaction was the most relevant, significantly influencing the five subscales. In fact, it was the only one that significantly determined Choking anxiety. An additional symptom, regurgitation, was a significant determinant of both Emotional impact and Disease anxiety. Interestingly, no additional symptom at diagnosis had a significant role in determining HRQoL of adult EoE patients. Unfortunately, our research did not assess the influence of current symptoms manifested by our EoE patients on the EoE-QoL-A overall score, because at the moment no validated instrument to assess esophageal symptoms is available in the Spanish language (e.g. a Spanish version of the EEsAI score). However, our research poses the hypothesis that some specific EoE symptoms at the time of disease onset may determine the emotional impact on QoL of EoE patients and generate disease anxiety, even when the disease has been diagnosed and a treatment has been instituted. Disease duration was also a significant determinant for HRQoL in several subscales of the EoE-QoL-A questionnaire. Therapy for EoE, including food restriction, drug therapy and even endoscopic dilation (although this last one did not have statistical significance) influenced Social impact, Emotional impact and Diet/eating impact of EoE; specifically, an empiric food elimination impaired the Diet/eating impact subscale in our patients. Certainly, the empiric six-food elimination diet, which has been demonstrated to be a highly effective and reproducible dietary option for inducing disease remission in EoE patients, 34 had a deleterious effect on HRQoL of our EoE patients; the number of foods excluded in each respondent patient was not recorded, preventing us from evaluating this fact properly. In any case, and despite the fact that scores for Diet/eating impact tended to be worse among EoE patients under food restriction compared to those who were not, the difference was not significant. Finally, a higher education level and female gender determined a worse HRQoL perception. The relationship of HRQoL with education level has shown to behave differently for several diseases; while both positively correlated in bronchial asthma exacerbations,35,36 they did the opposite in inflammatory bowel disease. 37 In our study, patient gender was shown to be an independent factor associated with the perception of HRQoL in EoE that had a significant effect on the Diet/eating impact dimensions of the EoE-QoL-A questionnaire, with women providing worse scores. One speculative explanation for this may be the greater difficulty perceived by the Spanish women in our series in finding substitutions or alternatives for foods when following a food elimination-based therapy in comparison to men, or the greater value placed on the act of eating on the part of women. In the Spanish socio-cultural context, women generally bear greater responsibility for buying and preparing food, perhaps conditioning them more than men in this respect.
Strengths of our study include its sample size, inclusion of patients from different Spanish geographical areas, measurement of HRQoL with a validated instrument previously adapted to the Spanish socio-linguistic environment, 23 the inclusion of patients with different therapeutic modalities for EoE, and control of confounding factors by means of multivariate analysis. Several drawbacks to this study, however, should be acknowledged. Recruited patients may not be representative of the Spanish adult population with EoE or EoE patients from other countries, mostly because of selection bias by including only hospital-controlled patients. Cultural and emotional aspects influencing food restrictions could also affect the generalization of our results. Additional limitations might be using self-reported symptoms, and lacking evaluation of treatment efficacy and the correlation of HRQoL with clinical and histological outcomes after therapy.
In summary, the present study demonstrates that EoE-specific HRQoL in adult patients with EoE is strongly associated with baseline presenting symptoms, especially food impaction, dietary restrictions and long-lasting disease. The type of therapy (drug treatment or dietary therapy) did not significantly affect the perception of HRQoL. Women with a higher educational level showed the highest concerns with dietary therapy.
Footnotes
Acknowledgments
We are grateful to all collaborators who recruited patients to participate in this research: Isabel Pérez-Martínez, Jesús Barrio, Óscar Nantes, Marta Sánchez-Cazalilla, Constanza Ciriza de los Ríos, and Antonia Perelló. We thank all the patients who participated in this study. Author contributions are as follows: AJL and AA designed the study; AJL and JM-I included the patients; AA and LAG managed and performed the statistical analyses and interpretation of the data; AJL wrote the manuscript; LAG, JM-I and AA interpreted the data and review the draft providing with relevant critical comments. All authors read and approved the final manuscript.
Declaration of conflicting interests
None declared.
Funding
This work was funded by the Instituto de Salud Carlos III through the project “PI 14/01417” (co-funded by the European Regional Development Fund, “Investing in your future”).
Ethics approval
This article does not contain any studies with animals performed by any of the authors. The study was carried out in accordance with the Declaration of Helsinki. Ethical approval was granted by the La Mancha Centro General Hospital Ethics Committee.
Informed consent
Informed consent was obtained from all individual participants included in the study. All participants included in the study consented to the publication of the data extracted from the statistical study. No individual patient data are reported.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.