
Abstract
Background
The most concerning complication of video capsule endoscopy (VCE) is capsule retention (CR) in the gastrointestinal (GI) tract although clinical outcome and management of patients with CR are still uncertain in a large single center material.
Objectives
The aim of this retrospective study was to investigate incidence, causes, risk factors, management and clinical outcomes of CR in a large single center between 2001 and 2011.
Results
2401 consecutive small-bowel (SB) VCEs were performed. CR was detected in 25 cases (1%). CR in patients with suspected and known Crohn’s disease (CD) undergoing VCE occurred in 14/1370 (1%) including known CD 9/390 (2.3%) and suspected CD 5/980 (0.5%). CR in patients with obscure GI bleeding was observed in 11/816 (1.3%) cases. The SB was the most common site of CR with 17 cases followed by the esophagus (4 cases), colon (2 cases), and stomach (2 cases). Emergency endoscopic intervention (3 cases) and surgery (2 cases) was needed in 5 cases of CR. Elective capsule removal was performed by surgery in 6 cases and endoscopically in 8 cases. Three retained capsules dislodged after steroid treatment and another 3 cases of CR resolved without any intervention.
Conclusion
This large clinical material demonstrates that CR is a rare complication with a favorable clinical outcome. Most patients with CR can be electively managed with non-surgical intervention.
Introduction
Video capsule endoscopy (VCE) has been established as the method of choice for visualizing the small-bowel (SB) mucosa. 1 VCE is particularly useful in the work-up of obscure gastrointestinal (GI) bleeding and in the evaluation of intestinal lesions related to non-steroidal anti-inflammatory drugs, celiac, and Crohn’s disease (CD).2–7 Although VCE is a non-invasive method and generally considered to be safe, capsule retention (CR) is a concerning complication, which can lead to acute bowel obstruction and necessitate emergency surgery.8,9 Significant narrowing of the bowel lumen by tumors or strictures increases the risk of CR.10,11 Thus, suspected SB stenosis is a contraindication for performing VCE. Bowel patency can be evaluated by use of radiological SB imaging (enteroclysis or barium SB follow-through) or by administration of a self-dissolving patency capsule (PC).12–17 The incidence of CR varies widely in the literature from 0 to 21%, which might be related to the characteristics of the examined populations or the relatively small groups of patients used in most studies.18–20 Surgical intervention was the most common approach for removal of retained capsules in earlier studies, 21 although more recent reports indicate the possibility of endoscopic treatment methods.22,23
The aim of this of study was to define the incidence, causes, risk factors, management, and clinical outcomes of CR in a large number of patients from one tertiary referral center for SB VCE.
Materials and methods
Patients
This investigation was a retrospective evaluation of all consecutive patients undergoing VCE from April 2001 to April 2011 at Skåne University Hospital in Malmö, Sweden. All patients gave written informed consent prior to the examinations. The study was conducted in accordance with the ethical principles of the Declaration of Helsinki, in compliance with good clinical practice and local regulations and the study was approved by the Ethical Committee of Lund University, Sweden. All patients referred for VCE had their medical records reviewed by an experienced gastroenterologist prior to VCE in order to identify patients with potential VCE contraindications, including suspected SB obstruction, known SB stricture, pregnancy or dysphagia. Patients with suspected SB obstruction underwent radiological SB imaging or PC examination. All cases with SB patency proceeded with VCE.
Video capsule endoscopy
The PillCam SB capsule endoscope (Given Imaging Ltd, Yokneam, Israel) was used in 2293 (95.5%) of all VCE cases. The Endocapsule (Olympus, Tokyo, Japan) was used in 98 cases (4.1%) and 10 examinations (0.4%) were performed using the Mirocam (Intromedic, Seoul, South Korea). Patient preparation included nothing by mouth 8 h before VCE. After swallowing the capsule, patients were allowed clear liquids after 2 h and solid food after 4 h. In patients with dysphagia the capsule was placed endoscopically in the duodenum by use of a polypectomy snare, Roth Net retrieval device (US Endoscopy, Mentor, OH, USA) or AdvanCE system (US Endoscopy). In patients with suspected slow gastric transit time, such as diabetic patients, and patients with previous slow gastric transit time on VCE, the real time viewer was used 1 h after swallowing the capsule. If the capsule remained in the stomach, gastroscopy was performed to move the capsule into the duodenum by use a polypectomy snare. At the end of the investigation day, patients returned the data recorder. All VCE studies were evaluated by one of four gastroenterologists experienced in VCE. No further controls were done if the video showed capsule passage to the colon. An abdominal X-ray film was recommended 2 weeks after the examination if the video did not show capsule passage to the colon or if the patient did not observe natural passage of the capsule.
Patency capsule
PC examinations were performed using a first or a second generation PC (Given Imaging Ltd.). A PC test was considered negative if the capsule was eliminated from the GI tract within 40 (first generation PC) or 30 (second generation PC) hours from ingestion according to the manufacturer’s instruction. Elimination of the PC was confirmed by use of a hand-held scanner.
Capsule retention
CR was defined as the presence of the capsule in the GI tract for at least 2 weeks after ingestion, or when it is indefinitely retained unless directed medical, endoscopic or surgical intervention is initiated. 24 Patients with Kock’s reservoir had their capsule removed endoscopically and these cases were not defined as CR. Patients with confirmed CR underwent further radiological examinations to identify the precise location of the retention or to detect spontaneous but delayed passage of the capsule. Depending on the position of the capsule and the cause of the retention, medical, endoscopic or surgical intervention was performed. We analyzed indications for the procedure, causes for the retention, management, and clinical outcomes in patients with CR.
Statistical analysis
To identify possible association between CR and a number of risk factors we used simple logistic regression analysis. Odds ratios (ORs) and 95% confidence intervals (CIs) are presented for dichotomous categorical variables; p-values below 0.05 were considered to be significant. Given the exploratory nature of the study, no correction of significance levels for multiple testing was done. All analyses were carried out using IBM SPSS (Version 20.0; IBM Corp., Armonk, New York, USA).
Results
Univariate analysis for development of capsule retention (CR).
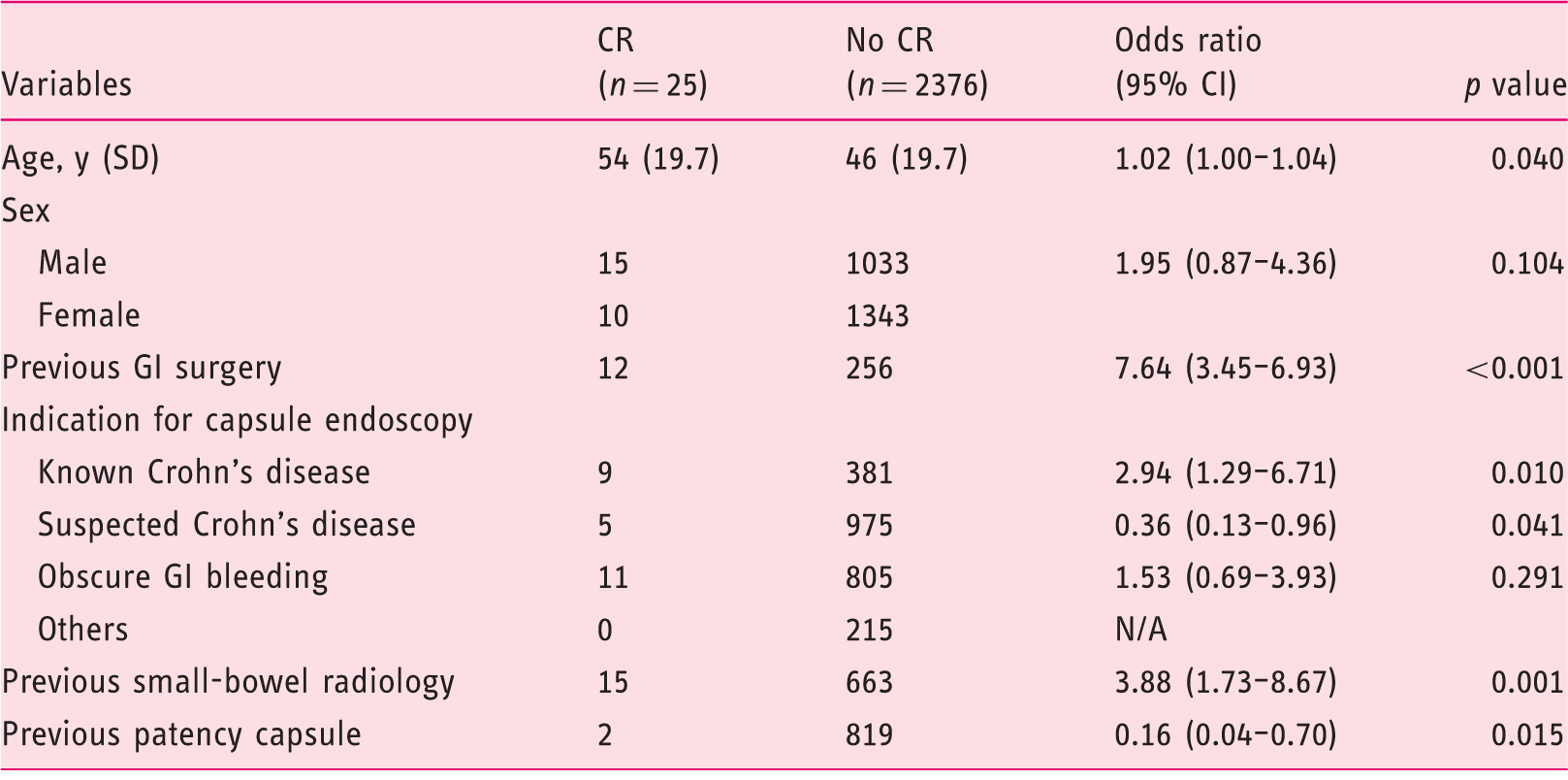
CI, confidence interval; N/A, not applicable since the logistic regression procedure could not perform the computation.
Patients with capsule retention.

F, Female; M, Male; CD, Crohn’s disease; OGIB, obscure gastrointestinal bleeding; SBFT, small-bowel follow-through; CTE, computed tomographic enterography; MRE, magnetic resonance enterography; y, year; m, month; DBE, double-balloon enteroscopy; PE, push enteroscopy; EBD, endoscopic balloon dilatation; APC, argon plasma coagulation; CE, capsule endoscopy; SB, small-bowel; AD, angiodysplasia.
The risk of CR was significantly increased in patients with known CD (9/390 patients, OR 2.94; 95% CI 1.29–6.71; p = 0.01) while suspected CD was associated with a significantly decreased risk (5/980 patients, OR 0.36; 95% CI 0.13–0.96; p = 0.04) of CR. No CR was observed in patients with miscellaneous indications. Obscure GI bleeding was not associated with a significant higher risk of CR (11/816 patients, p = 0.29).
The SB was the most common site of CR with 17 cases (13 ileal, 2 duodenal, and 2 jejunal stenosis) followed by the esophagus, colon, and stomach (Figure 1). The most frequent cause of CR was Crohn’s stenosis in the SB, which occurred in 12 (48%) cases. Additional causes of CR were NSAID-induced webs in the SB (3 cases), peptic stricture in the esophagus (2 cases), and pyloric stenosis (2 cases). Rare causes of CR were esophageal diverticulum, postoperative stenosis in the duodenum, duplication cyst in the SB and metal stent in the colon, which occurred in one case each. One case of CR in the esophagus occurred without any macroscopic pathology and one capsule was retained in a normal colon for 37 days.
Site of capsule retention.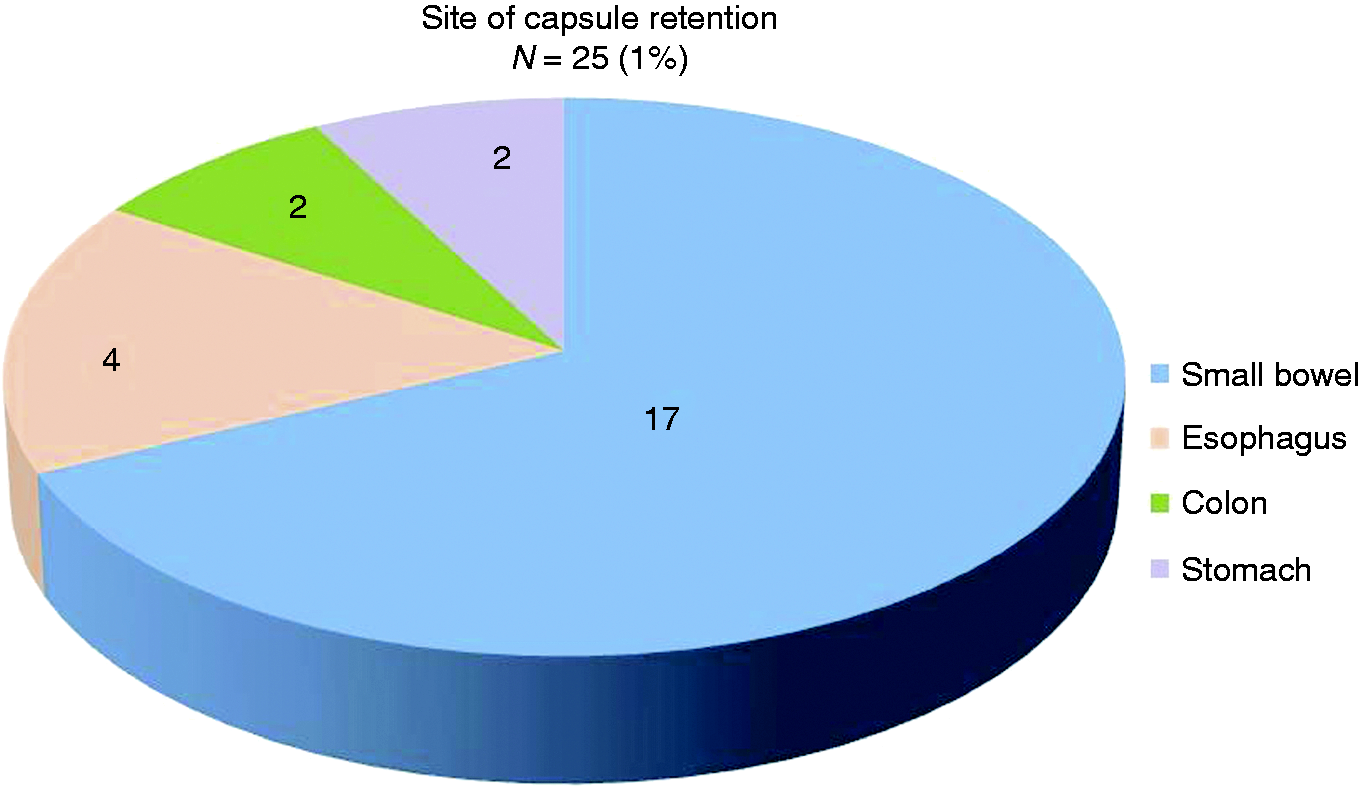
The risk of CR was significantly increased in patients who had undergone SB radiology before VCE (OR 3.88; 95% CI 1.73–8.67; p = 0.001, Table 1). In contrast, utility of PC prior to VCE decreased risk of CR (OR 0.16; 95% CI 0.04–0.70; p = 0.015, Table 1). Notably, we found that 14 of 17 (82%) patients in the group with SB CR had previously undergone a negative work-up for SB stricture (12 SB imaging and 2 patency tests). In one of the two patients who underwent a positive patency test before CR the following radiological examination incorrectly located the PC in the rectum. VCE was then performed and the video capsule was retained in the SB. In the other case of CR after PC test, excretion of the PC was considered complete after 60 hours instead of the manufacturer’s recommendation being 40 hours. Only 7 patients (28%) with CR had symptoms of obstruction (dysphagia in 3 cases and abdominal obstructive symptoms in 4 cases).
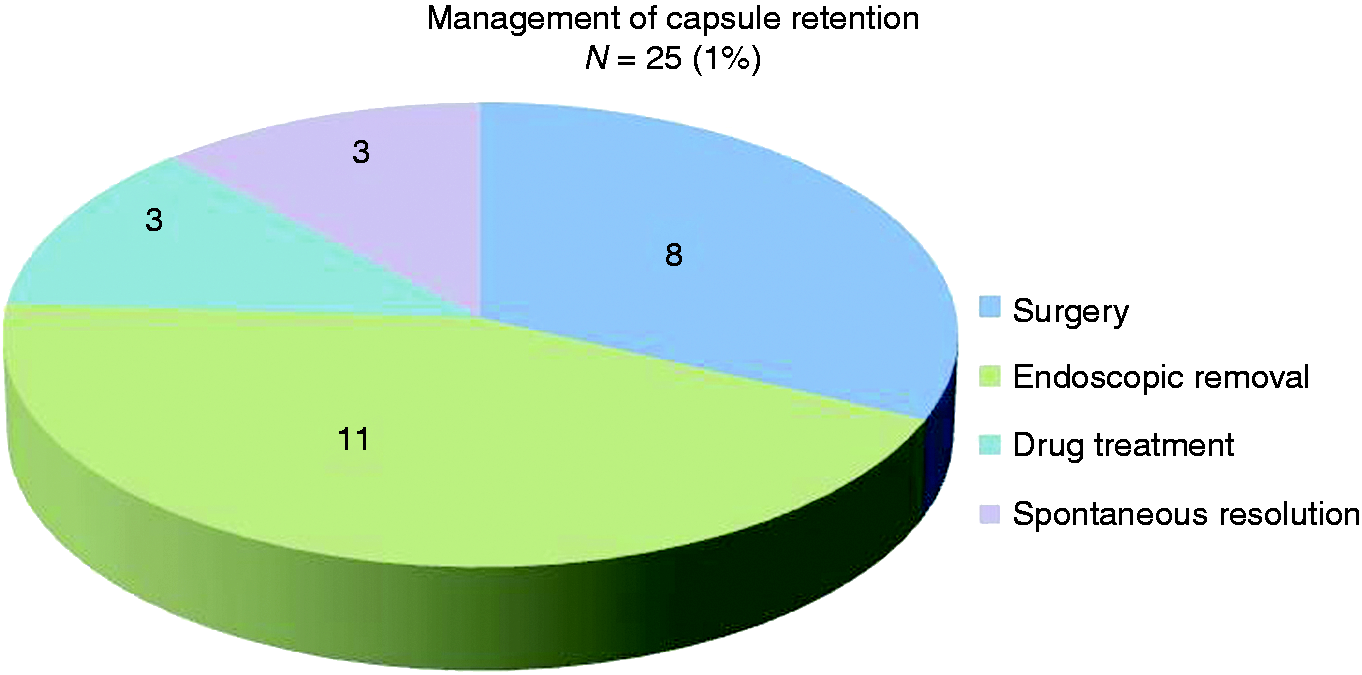
Endoscopic capsule extraction was performed in 11 (44%) cases and 8 (32%) patients underwent laparotomy with segmental bowel resection (Figure 2). Three (12%) capsules dislodged after steroid treatment and 3 (12%) cases of CR resolved without any intervention (Figure 3). Endoscopic interventions involved gastroscopic removal in 8 cases and the use of double-balloon endoscope in 3 cases (Figure 4). Emergency intervention was needed in 5 (20%) cases, of which 3 cases were managed by gastroscopy and 2 had surgery. No CR-related deaths occurred during one-year of follow up.
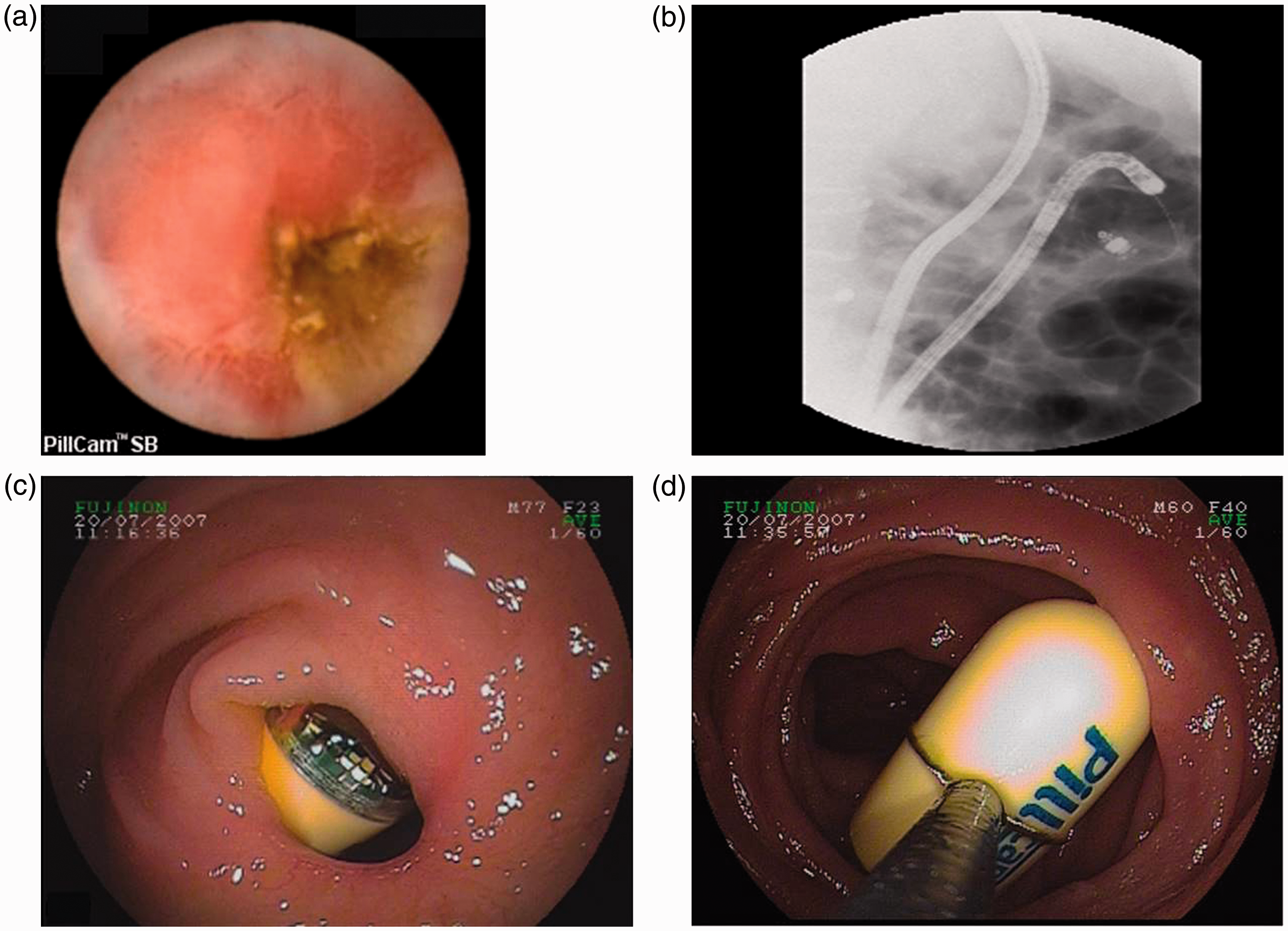
A 44-year-old man with known Crohn's disease who had undergone ileocecal resection presented with suspected disease activity (patient Nr 1). The patient underwent colonoscopy and SB radiology showing normal results. A: VCE image shows an ulcerated SB stricture. B: Plain abdominal x-ray reveals the retained capsule. C and D: Images showing 4 strictures which were treated by surgery. Management of capsule retention. A 73-year-old man with chronic NSAID medication presented with obscure GI bleeding (patient Nr 13). A: VCE image shows a stricture in the proximal part of jejunum causing capsule retention. B: Plain abdominal x-ray image during DBE shows the endoscope and the retained capsule in the proximal jejunum. C: DBE image shows the capsule between two SB strictures. D: DBE image shows the capsule being retrieved using a snare after balloon dilation of the strictures.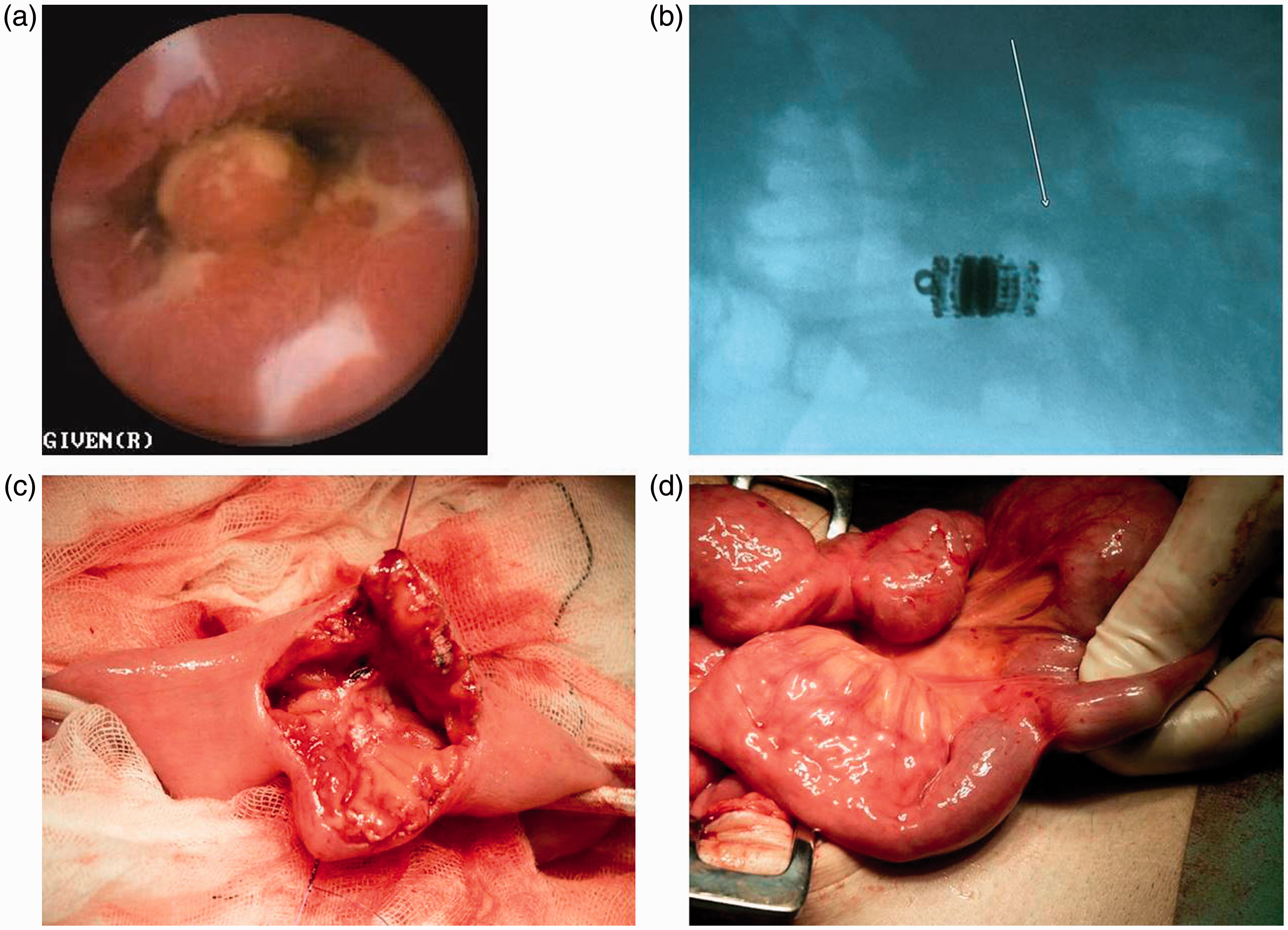
Discussion
VCE has emerged as the leading methodology to examine the mucosa in the SB. The most concerned complication of VCE is retention of the capsule in the digestive tract, which might cause symptomatic intestinal obstruction. This study demonstrates in a large material from a single-center that CR is a rare complication in patients undergoing VCE. The published data on CR in patients undergoing VCE varies between 0 and 21%,18–20 which might be related to the type of the examined populations or the relatively small groups of patients used in most studies. In the present investigation, we observed that the incidence of CR was 1.0%. Our findings represent one of the few investigations on CR with large numbers of patients undergoing VCE in the literature. The CR rate has been reported to range between 0.9% and 1.4% in previous single center studies.21,22 A systematic review on VCE including 227 original papers reported a pooled retention rate of 1.4%. 25 More recently, a large multicenter investigation including 2300 patients reported a CR rate of 1.3%. 26 The low incidence of CR in patients with suspected CD (0.5%) and in patients with obscure GI bleeding (1.3%) is comparable with previous literature.21,22 Recently in a study with a tertiary care population without obstructive symptoms, capsule retention occurred in only 0.3% of cases, 27 whereas a previous investigation reported a CR rate of 2% in more than 5000 patients recruited from 12 centers. 28
The risk of retention in established CD can limit the use of VCE. CR rate in known CD was initially reported to be as high as 13%, 29 but the risk was much lower (2.1–7.8%) in later studies,30–32 especially when a PC was used. Although the use of PC has been demonstrated to significantly decrease the rate of retention, 33 it does not eliminate the risk completely. 32 In our material, the CR rate was 2.3% in patients with known CD, which is lower than that observed in most other studies.29–31 Our relatively low CR rate in patients with CD can be explained by careful patient selection and frequent use of PC or SB imaging. This is in concordance with a recently published report comparing two different strategies for the use of PC in known CD. 34
Strictures caused by surgical anastomosis are also known reasons for CR;27,35 however, in an earlier study no cases of CR were reported in patients with partial SB resection. 36 Herein we found that pervious GI surgery significantly increases the risk of CR.
CR can occur at all levels of the GI tract; 35 however, earlier large studies have not reported cases of capsule impaction outside of the SB.21,22 Some studies defined CR only inside the SB.21,22 We found several capsules retained in the esophagus and in the stomach despite of earlier negative gastroscopies in other centers. Although 9 of 25 retentions seem to be avoidable by proper flexible endoscopy our policy was to accept patients for VCE with a previous negative gastroscopy and colonoscopy performed within 3 months at other institutions. Nonetheless, our results indicate that repeated high-quality endoscopy, including biopsies for excluding eosinophil esophagitis, prior to VCE should be considered in spite of previous negative endoscopies in order to reduce the risk of CR.
Some cases of esophageal CR could have been avoided by consequent use of real-time viewer, but this helpful device was not available in the beginning of this study. For example, the case with CR due to esophageal diverticulum might have been detected using real-time viewer, and the entrapped capsule could be placed endoscopically in the duodenum at the beginning of examination.
The CR rate in the SB was only 0.7% which is lower than in the most previous studies.21,22 The most common cause of CR was Crohn’s stenosis in the SB, which is related to the fact that a high proportion of the indications were CD in this study. We found a few NSAID-induced rings as the cause of CR, which was the most frequent finding in the report of Li et al. 21 In our material, tumors were not a risk factor for CR, which is in contrast to a previous large multicenter study. 10
Management of CR includes medical, endoscopic, or surgical treatment. 37 In the early years, CR was largely managed by surgical interventions; 21 however, later studies have reported a more favorable clinical outcome using endoscopic methods. 22 In our material, only eight patients (32%) needed surgery for capsule retrieval. Seven of these eight patients underwent VCE between 2001 and 2006. We have mainly performed double-balloon enteroscopy for capsule retrieval since 2007. Between 2007 and 2011, a majority (9/13, 69%) of retained capsules were removed endoscopically and only one patient underwent surgical removal. This endoscopic management trend of CR has also been forwarded in a report by Van Weyenberg et al. 22
In cases of suspected SB stenosis we prefer PC over radiological examinations. Herein PC indicated SB patency in 99% of cases undergoing CE. The two false negative cases were a result of non-conclusive PC examinations. Several studies have shown that use of PC can minimize risk of CR in patients with suspected SB strictures. 38 According to current recommendations, one should consider CR to be unlikely if the PC is excreted in due time, radiologically located in the colon or excreted in an undamaged state. 33 The presence/absence of PC can easily be demonstrated by a hand-held scanner, however, in some cases use of hand-held scanners result in false positive results when the capsule remains in the GI tract but with unclear localization. Indeed, there is still uncertainty regarding optimal technique to localize the PC in the GI tract. 37 If patients have not excreted the PC in due time or if the PC is detected by a hand-held scanner use of plain abdominal film is advocated whereas abdominal radiography is frequently inaccurate in locating the PC as demonstrated in our material. A more recent study emphasized also the inaccuracy of the plain abdominal film for this purpose and forwarded a dedicated low-radiation CT protocol for localization of the PC in the GI tract. 39
Negative radiological examinations like MRE did not exclude SB stenosis in our study. We observed that only seven patients with CR presented with clinical symptoms of intestinal obstruction. These cases of obstruction could be managed endoscopically in three cases and by elective surgery in two cases. Two acute surgical interventions were performed several weeks after capsule ingestion. All patients who underwent surgery had complete resolution of symptoms during the postoperative follow-up period of 1 year.
Conclusions
In conclusion, this large single-center study demonstrates that CR is a rare complication of VCE. Our data suggest that careful patient selection in combination with adequate use of PC decreases the risk of CR. Moreover, a majority of patients with CR can be safely and effectively managed with endoscopic intervention instead of surgery.
Footnotes
Acknowledgement
The authors would like to acknowledge Håkan Lövkvist for statistical analysis.
Declaration of conflicting interests
GW Johansson and E Toth received lecture fees from Given Imaging/Medtronic.
Funding
A Nemeth received grant for PhD students from Region Skåne.