
Abstract
Aim
To describe a poorly known endoscopic entity associated with portal hypertension, characterized by polypoid lesions either in the stomach or small intestine of patients with cirrhosis.
Methods
Between 2003 and 2012, patients with cirrhosis and portal hypertension underwent endoscopic workup of portal hypertension in our endoscopy unit. The clinical expression, endoscopic features of these lesions, and their pathological characteristics are described.
Results
A total of 1538 patients were included, among which 14 (0.9%) presented polypoid lesions; these patients had evidence of portal hypertension and had dilated capillaries in the lamina propria. Four patients presented with severe anaemia or melaena and required treatment. Propranolol was administered to three patients, and one patient needed a transjugular intrahepatic portosystemic shunt in order to control bleeding. For asymptomatic patients in whom polypoid lesions were resected, no recurrence of lesions was observed during follow-up gastroscopy (median 36 months, range 7–85 months).
Conclusion
Portal hypertension-associated gastric or small intestine polypoid lesions may be associated with a significant risk of bleeding and are responsive to adequate treatment of portal hypertension.
Introduction
Cirrhosis and portal hypertension are associated with recognized gastric, small bowel, and colonic mucosal abnormalities that include portal hypertensive gastropathy, enteropathy, and colopathy, characterized by mucosal vascular lesions such as spider angiomata and inflammatory-like abnormalities such as hyperaemia and oedema. These lesions are flat or slightly protruding in the lumen during diagnostic endoscopy. Recently, protruding red bumps were described in the small bowel of a cirrhotic patient. 1 The present study extends this report and describes a poorly known endoscopic entity, characterized by polypoid lesions in the stomach and small bowel, in a series of patients with cirrhosis. It also assesses the impact of therapeutic procedures on these lesions.
Patients and methods
During the study period from May 2003 to September 2012 in our endoscopy unit, 1538 patients with cirrhosis and portal hypertension underwent upper and lower gastrointestinal (GI) endoscopy (GIF-Q160, GIF-H180, GIF-1T140, GIF-1TQ160, CF-Q160AI; Olympus, Hamburg, Germany) for either a work up of portal hypertension, anaemia, or blood exteriorization. Capsule endoscopy (Pillcam SB1 or SB2 video capsule endoscope; Given Imaging, Yoqneam, Israël; or M2A Olympus video capsule endoscope) was done in case of severe anaemia or bleeding with inconclusive findings at oesogastroduodenoscopy and colonoscopy. Cirrhosis with portal hypertension was diagnosed clinically and with liver imaging and confirmed by the measurement of the hepatic venous pressure gradient (HVPG) in 11/14 patients. In the case of protruding lesions, depending on the endoscopic appearance, polypectomy (n = 5), mucosectomy (n = 2), or biopsies (n = 5) were performed. Other mucosal lesions associated with portal hypertension, including gastropathy, varices, enteropathy, and colonopathy, were described according to their respective classifications.2–7
Data collection for these patients included clinical examination, biochemical tests, HVPG measurements, and follow up. All patients gave informed consent for diagnosis and therapeutic procedures performed for the evaluation and treatment of their disease.
Data were expressed as median and range calculated using statistical software (SPSS version 20.0; SPSS, Chicago, IL, USA).
Results
Patients
Among the 1538 patients examined during the study period, 14 (0.9%) disclosed polypoid lesions histologically proven to be related to portal hypertension in the stomach or small bowel. Clinico-biological and usual endoscopic characteristics of these 14 patients are shown in Supplementary Tables S1 and S2. Patients were predominantly male (11/14) with a median age of 66 years (range 42–82 years). Cirrhosis was caused by alcohol in seven patients, viral hepatitis in three, non-alcoholic fatty liver disease in one, and was cryptogenic in three. Median Child–Pugh and Model for End-stage Liver Disease scores were 5 (range 5–11) and 12 (range 6–18), respectively. All 11 patients who had measurement of HVPG exhibited sinusoidal portal hypertension (median 16 mmHg, range 8–25), had oesophageal varices (median grade 2, range 1–3), and portal hypertensive gastropathy (mild in 11, severe in three). Three patients had a history of oesophageal variceal bleeding treated by band ligation (14, 3, and 2 months before entering the study, respectively). No patient had previous upper GI endoscopic mucosal treatment (coagulation or resection) for any reason.
Clinical presentation
Presentation consisted of active melaena with severe anaemia in three patients (patients 1, 2, 12), severe anaemia without blood exteriorization in two (patients 3, 14), and no symptoms nor an acute drop in hemoglobin values in the remaining nine (patients 4–11, 13). Cirrhosis was clinically compensated in all patients except patients 2 and 12, whose Child–Pugh scores were 11. All patients underwent follow-up upper GI endoscopy and ileo-colonoscopy when indicated. Video-capsule endoscopy was complementarily performed on patients presenting haemoglobin levels <8.5 g/dl with no significant lesions at upper or lower GI endoscopy (patients 1–3, 11, 12).
Endoscopic and histological features
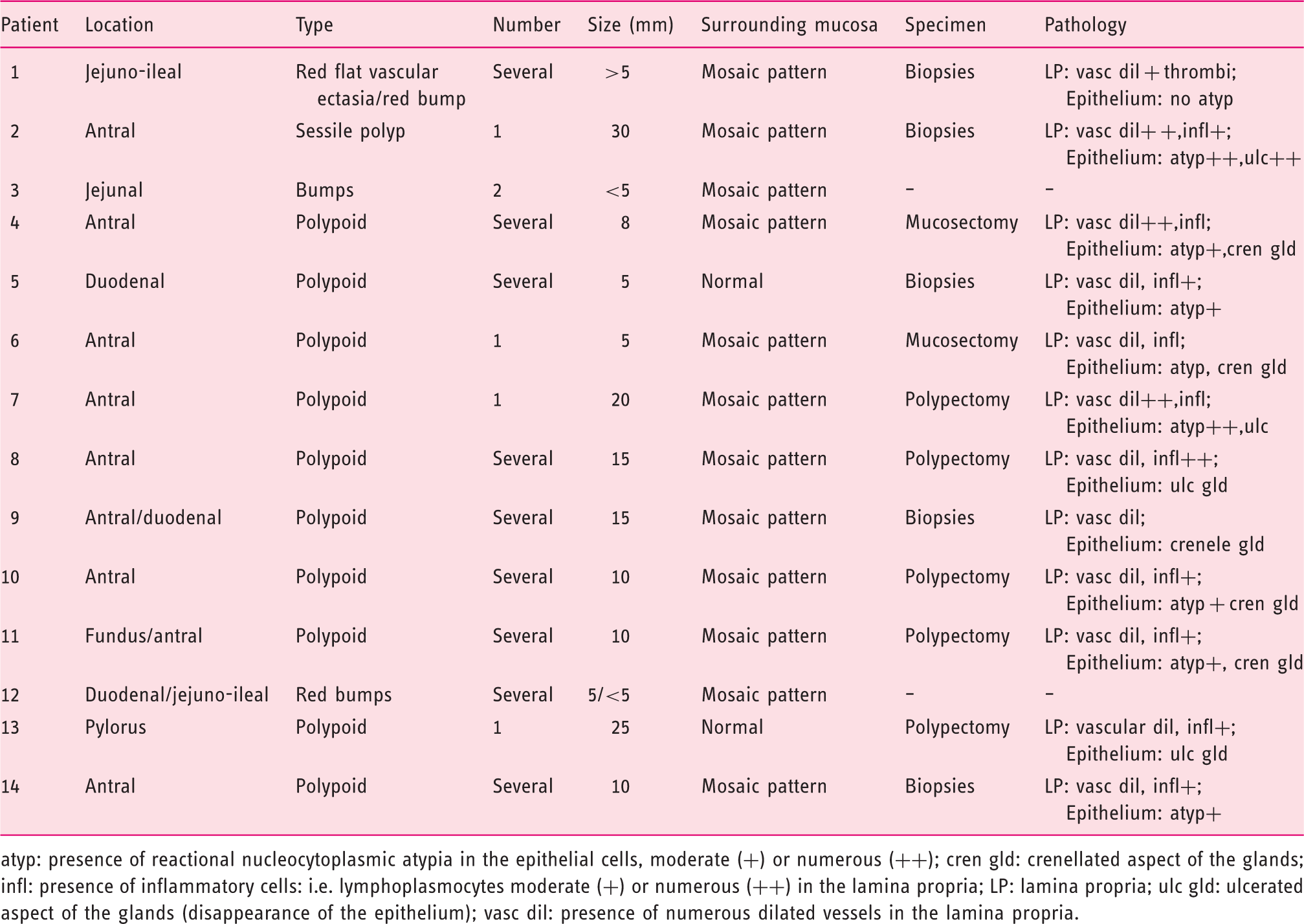
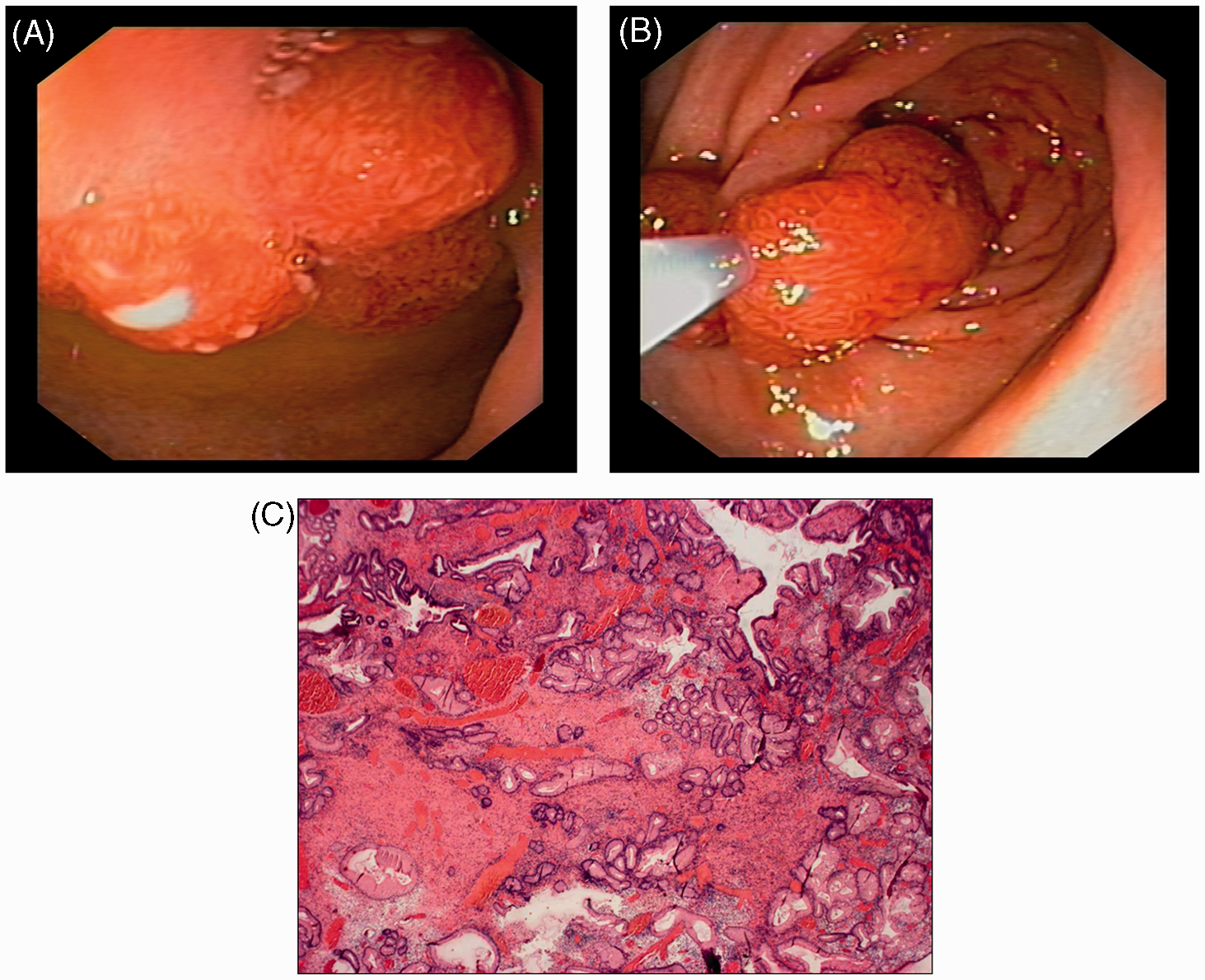
Endoscopic findings and pathological descriptions are summarized in Table 1. Protruding bumps with a mosaic surrounding mucosa were present in the jejuno-ileum of three patients (patients 1, 3, 12; Figures 1 and 2 and Supplementary Figure S1, available online). In patient 1, they were multiple, hyperaemic, and disseminated in the jejunum and ileum (the largest was 7 mm), while in patient 3 there were less numerous and smaller. Biopsies of ileal red bumps in patient 1 revealed numerous dilated capillaries in the lamina propria, with fibrin thrombi in some of them (Figure 1E).
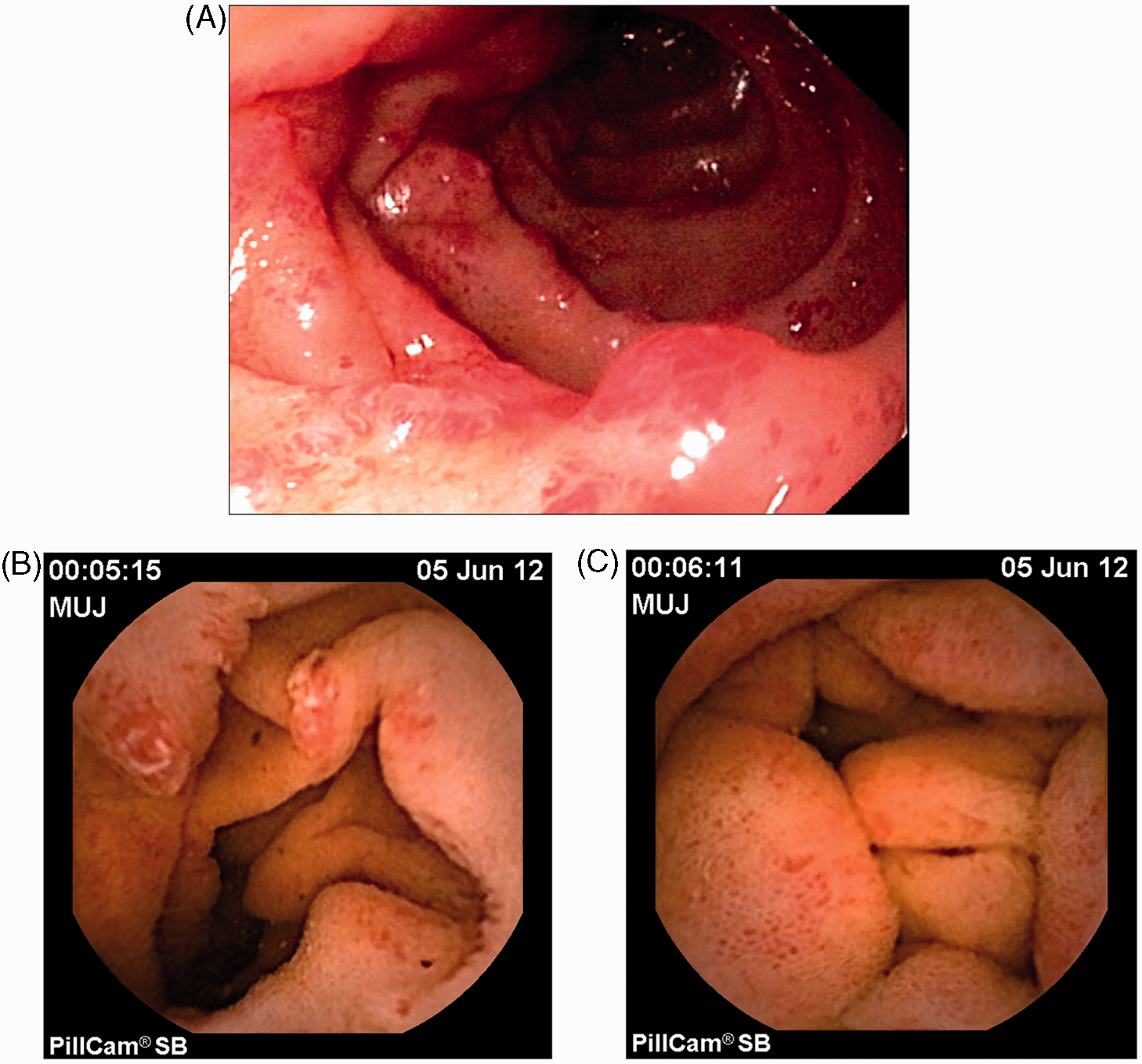
Patient 1: severe anaemia and recurrent episodes of melaena. (A) Terminal ileoscopy revealed one polypoid lesion with a mosaic pattern of mucosa around the base and multiple red bump lesions. (B–D) Videocapsule endoscopy performed in the same patient showed diffuse small intestinal involvement by sparse red bump lesions (B) and confirmed the presence of the polypoid lesion in the terminal ileum (C, D). (E) Biopsy specimen of the ileal polyp; numerous vascular dilations in the lamina propria are suggestive of hypertensive enteropathy; some capillaries presented intravascular fibrin thrombi, a feature well described in gastric antral vascular ectasia. (F) Terminal ileoscopy performed 5 months after treatment with β-blockers revealed significant regression of the red bumps and polypoid lesions previously described in the terminal ileum whereas the patient no longer exhibited melaena or anaemia. Patient 12: chronic melaena and severe anaemia requiring multiple transfusions. (A) EGD revealed multiple red bumps in the duodenum. (B, C) Videocapsule endoscopy demonstrated multiple red bumps also present in the jejunum (B) and ileum, with a mosaic-like pattern in the surrounding mucosa (C). Endoscopic and histological characteristics of the lesions atyp: presence of reactional nucleocytoplasmic atypia in the epithelial cells, moderate (+) or numerous (++); cren gld: crenellated aspect of the glands; infl: presence of inflammatory cells: i.e. lymphoplasmocytes moderate (+) or numerous (++) in the lamina propria; LP: lamina propria; ulc gld: ulcerated aspect of the glands (disappearance of the epithelium); vasc dil: presence of numerous dilated vessels in the lamina propria.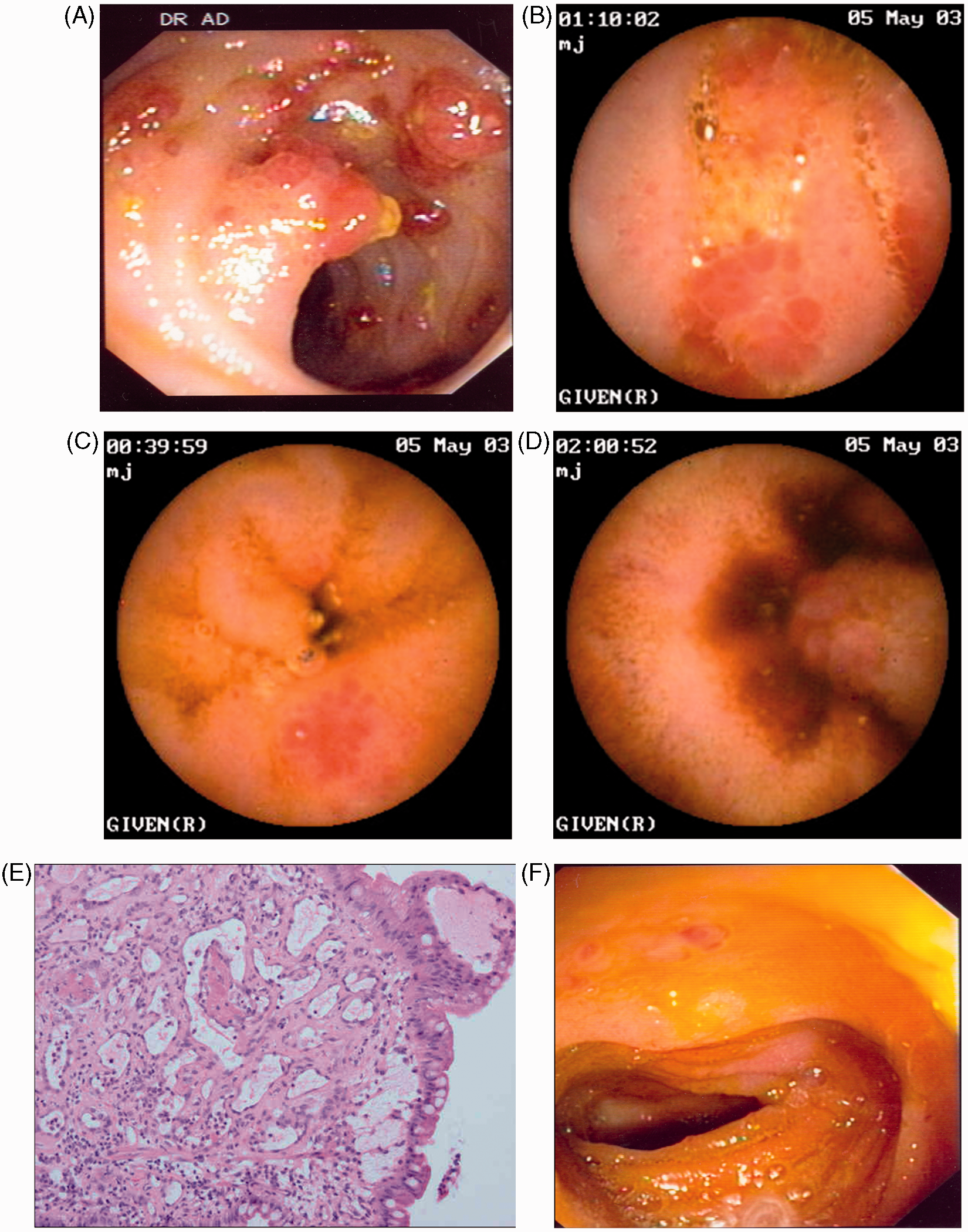
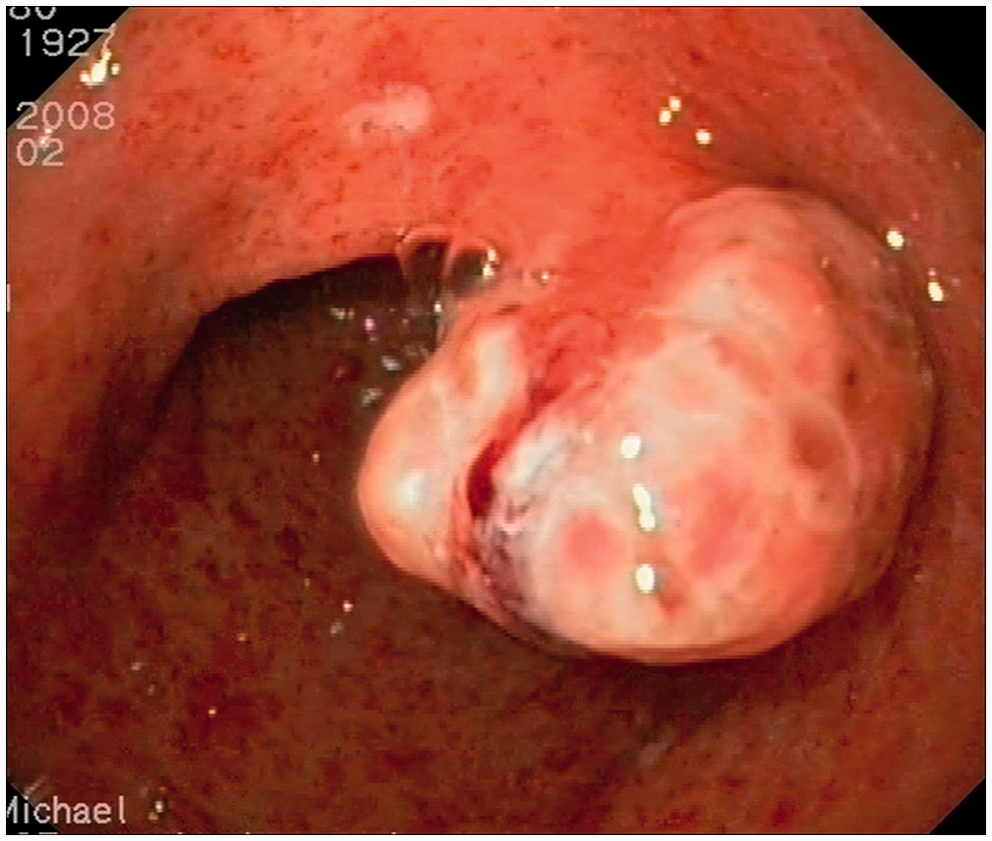
Patient 2 exhibited a huge 30-mm sessile polyp in the antrum, with a profound crater in the centre (Supplementary Figure S2). Biopsies were performed and showed numerous dilated capillaries and numerous inflammatory lymphoplasmatocytes in the lamina propria, while the epithelium focally presented an ulcerated aspect with regenerative nucleocytoplasmic atypia.
The other 10 patients (patients 4–11, 13, 14) exhibited protruding polyps, either pedunculated or sessile, single or numerous, small (from 3 mm) to voluminous (up to 20 mm diameter), with whitish exudates at their top (Figure 3A, B) mimicking adenomatous polyps, and were localized in the antrum (Figure 4), the pylorus (Figure 5), and/or the first duodenum (Figure 3C). In all cases, histological analysis of polypectomy and mucosectomy pieces revealed numerous dilated capillaries in the lamina propria, with a variable contingent of inflammatory lymphoplasmatocytic cells, while the epithelium presented a crenulated glandular aspect and nuclear regenerative atypias (Figure 3D).
(A) Patient 4: multiple pediculated polyps in the antrum presenting whitish exudates at their top; several of these polyps were safely removed by snare polypectomy using endocut current. (B) Patient 6: one isolated sessile polyp in the antrum, with a discrete whitish exudate at its top. (C) Patient 5: upper GIE revealed multiple polypoid lesions in the duodenum. (D) Patient 7: histological examination of antral polyp; numerous vascular dilations in the lamina propria, suggesting portal hypertensive enteropathy. Patient 8: one large pediculated polyp in the antrum diffusely covered by a whitish exudate; this large polyp was safely removed by polypectomy after leaving an endoloop around its base. Patient 13: A NAFLD cirrhotic patient underwent a gastroscopy for portal hypertension work-up. (A,B) A polypoid lesion in the pylorus observed during gastroscopy (A) was resected with a snare and endocut current (B); the endoscopic pattern of the polyp was that of an orange-coloured lesion with slightly whitish exudates at the top. (C) Histological examination of this polyp; numerous vascular dilations in the stroma separated by inflammatory infiltrates comprising neutrophils and eosinophils.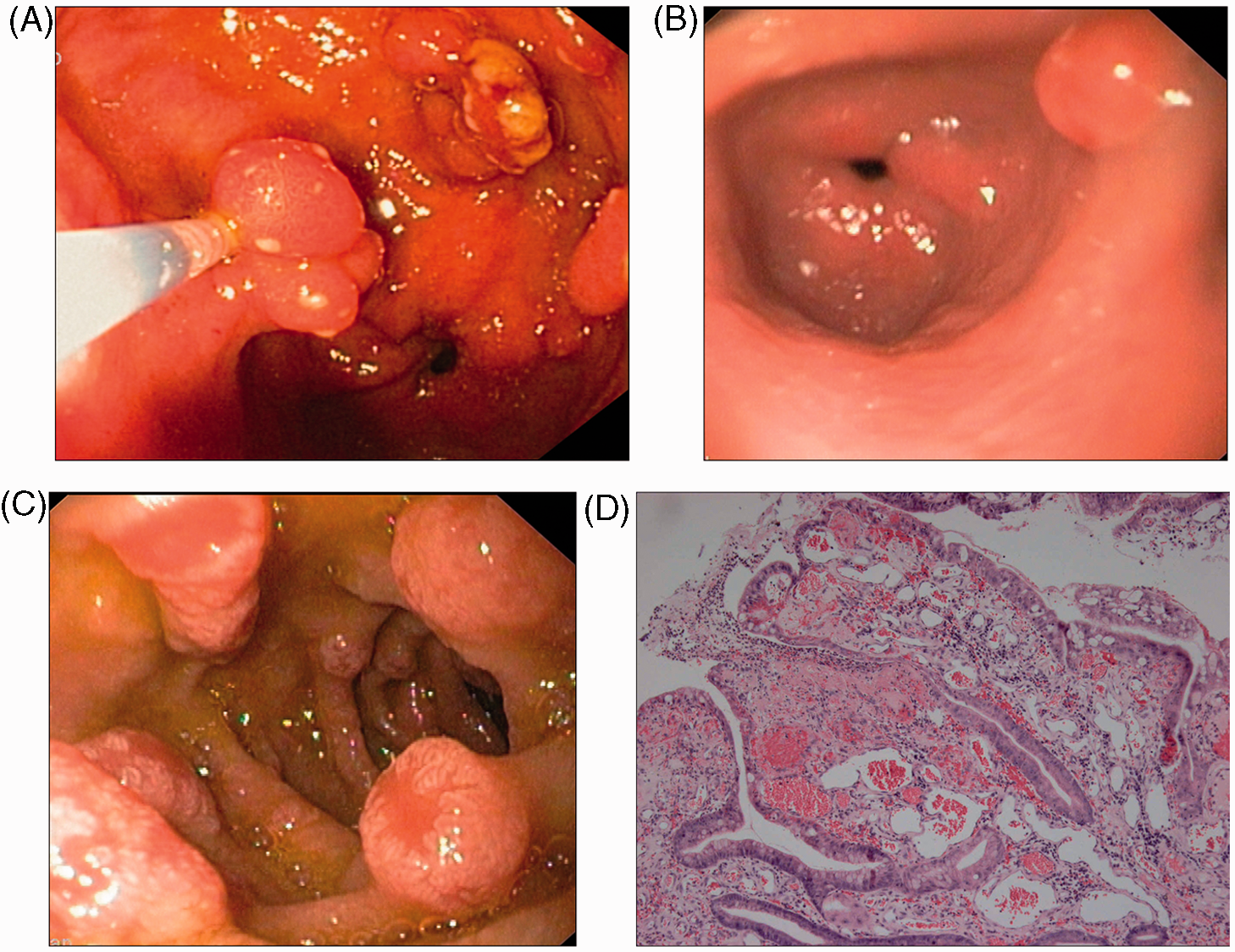
None of the patients had associated portal hypertensive colopathy. Finally, none of the endoscopic procedures (biopsy, polypectomy, mucosectomy) were associated with immediate or delayed clinically significant bleeding.
Clinical management
Treatment and follow up
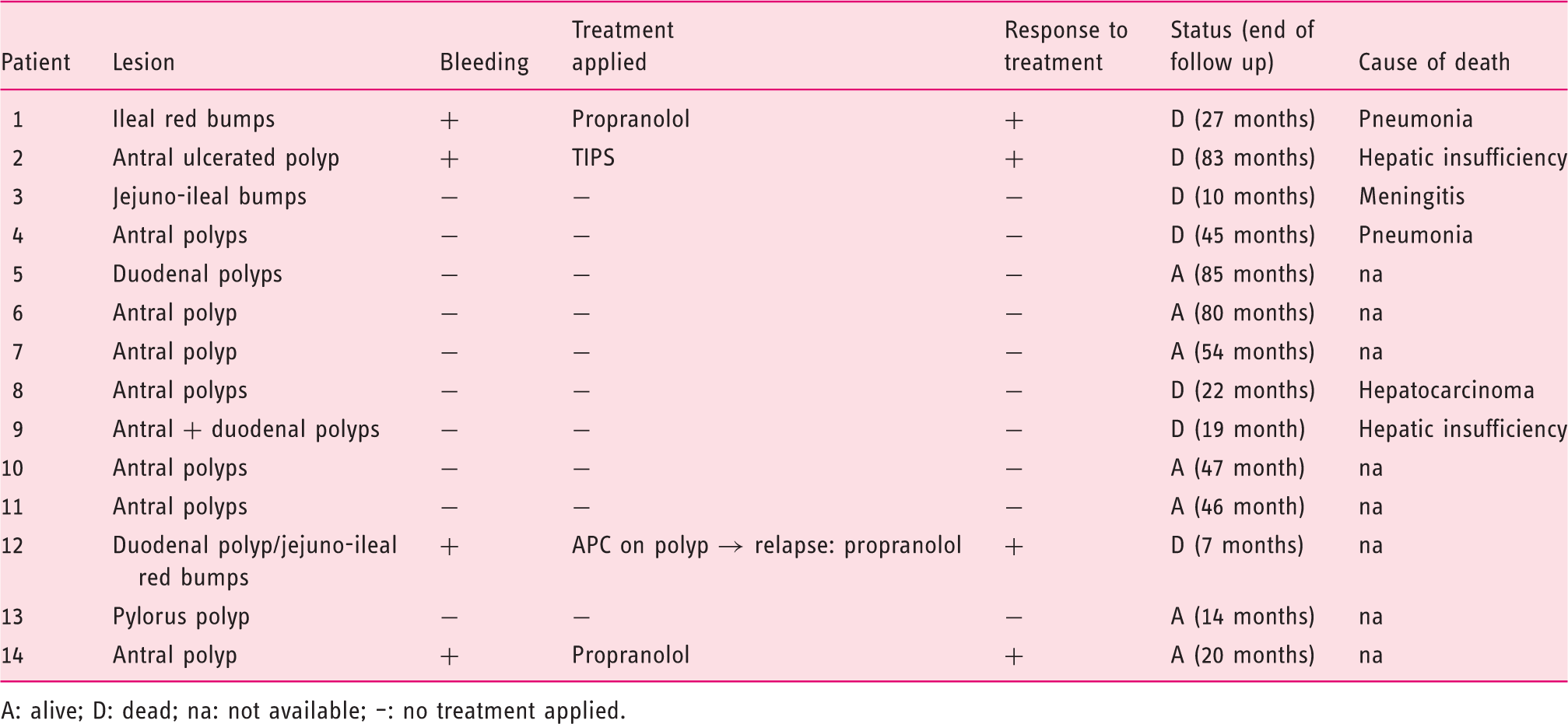
A: alive; D: dead; na: not available; –: no treatment applied.
Patient 1, with melaena and severe anaemia probably related to multiple jejuno-ileal red bumps, was treated with propranolol 160 mg/day. This treatment led to resolution of melaena and stopped the need for red blood cell transfusion after 1 month. Spectacular regression of protruding bumps was observed during follow-up ileoscopy performed 5 months later (Figure 1F).
Patient 2 presented with recurrent melaena and severe anaemia requiring iterative transfusions, probably related to a voluminous antral crateriform polyp. β-blockers did not induce an adequate decrease in HVPG (drop of ≥20% from baseline or under 12 mmHg). 8 Therefore, a transjugular intrahepatic portosystemic shunt (TIPS) was inserted, and 1 month later the patient was free of melaena and no longer required blood transfusion.
Patient 12 presented with chronic melaena and severe anaemia requiring multiple transfusions. He was listed for liver transplantation because of refractory ascites and continuing bleeding after placement of a TIPS, which was unable to decrease the HVPG to less than 15 mmHg. During an episode of clinical bleeding, gastroscopy disclosed active bleeding from two of the multiple red bumps in the duodenum, treated by argon plasma coagulation. Propranolol was introduced after another episode of recurrent bleeding, with subsequent disappearance of melaena and no further need for transfusion during follow up.
Patient 14 presented with severe chronic anaemia. Gastroscopy disclosed multiple polypoid lesions with whitish exudates at their top in the antrum and propranolol was introduced at 160 mg/day. Three months later, anaemia was resolved.
Polypoid lesions observed in the digestive tract of the other 10 patients were not associated with clinical or biological bleeding, but five of them were already being treated with propranolol for variceal-bleeding prophylaxis. Among the remaining five patients, only one received β-blockers after a work up disclosing grade-2 oesophageal varices. No specific therapeutic option was proposed to the other four patients.
At the end of follow up (median 36 months, range 7–85 months), seven patients were alive. Seven patients had died from causes unrelated to polypoid lesions (pneumonia, meningitis, liver failure, hepatocarcinoma). Among the four patients presenting with clinical bleeding, none had recurrent bleeding during follow up. Follow-up gastroscopy was obtained in three of the seven remaining patients disclosing no recurrence of the previously resected polypoid lesions, with no specific treatment and regression of the lesions in patient five, who was treated by TIPS for refractory ascites in the meantime.
Discussion
This study describes a series of 14 cirrhotic patients with a poorly known endoscopic presentation of portal hypertension characterized by polypoid lesions in the stomach and/or small bowel. We suggest that this endoscopic feature, together with the pathological demonstration of dilated vessels, corresponds to rare (<1%) vascular lesions related to portal hypertension in cirrhosis. These lesions may be associated with clinically significant bleeding in otherwise well-compensated cirrhosis (28% of patients). To our knowledge, such a cohort, with polypoid lesions associated with portal hypertension, has not been previously reported in the upper GI tract of cirrhotic patients, except for few case reports: one reported red bump lesions in the ileum; 1 another reported an isolated duodenal polyp; 9 two reported the histological description of hyperplastic gastric polyps;10,11 and three described nodular gastric antral vascular ectasia lesions. 12 For the colon, some authors have already reported polypoid lesions due to portal hypertensive colopathy. 13 Eventually, we showed that adequate control of portal hypertension was able to stop bleeding from these lesions and that either systemic or local treatment was associated with a reduction in size or long-term disappearance of these lesions
Three questions arise from this series. First, are these lesions related to portal hypertension? Second, are these lesions responsible for bleeding? Third, how do we treat such lesions?
To establish the portal hypertensive origin of the lesions, pathological analysis was provided in all patients except two (patients 3 and 12), in whom polypoid lesions were not endoscopically accessible or were not obtained. The endoscopic presentation of polypoid lesions in the small bowel raises the question of differential diagnosis with intestinal tumoral or inflammatory lesions (patient 1; Figure 1) and, in the stomach and/or duodenum, with malignant gastric ulcer (patient 2; Supplementary Fig S2) or adenomatous polyps (patients 4–11, 13; Figures 3–5). To define the nature of these polyps, biopsy or polypectomy (in the stomach) were performed.
In all cases, numerous vascular dilations were observed in the lamina propria, establishing their portal hypertensive nature and distinguishing them from inflammatory polyps. In the stomach, different degrees of lymphoplasmatocytic inflammation were found in the lamina propria, but these were consistently less severe than vascular changes. The whitish exudates frequently observed at the top of the antral polyps during endoscopy were in accordance with focally crenulated or ulcerated aspects of the glands in the epithelium. In these cases, the epithelium frequently presented nucleocytoplasmic atypia (due to regenerative changes); however, no dysplasia was observed, thereby excluding an adenomatous nature for these polyps.
In patient 1, biopsy specimens of ileal red bumps revealed numerous vascular dilations in the lamina propria specific to portal hypertensive enteropathy. Moreover, some capillaries presented intravascular deposits of fibrin thrombi (Figure 1E); the latter feature has not been previously described in the small intestine, but has been reported in the antrum of patients with portal hypertension, where it appears to be a specific feature distinguishing gastric antral vascular ectasia from portal hypertensive gastropathy. 14 Concerning the protruding bumps observed during videocapsule endoscopy in the distal jejunum of patient 3 (Supplementary Figure S1A, B), which were not accessible for biopsy, their similarity to the other polypoid lesions, together with underlying cirrhosis in the patient, renders a link to portal hypertension highly probable. The same is true for the intestinal red bumps reported by Tang et al. in 2002, 15 which were not accessible for biopsy but which were very likely a manifestation of portal hypertension.
All together, these data strongly suggest the relationship of these lesions with portal hypertension. However, this study was undertaken with a descriptive aim and does not enable us to establish a strong relationship between these polypoid lesions and other parameters such as clinical, biochemical, or endoscopic findings in cirrhotic patients. Among the 14 patients in this series, four presented active bleeding while 10 were asymptomatic. All patients had portal hypertensive gastropathy (mild in 11/14 patients), oesophageal varices, non severe cirrhosis, and clinically significant portal hypertension. We did not find a correlation between severity of clinical manifestations (i.e. anaemia and/or melaena) and HVPG or endoscopic presentation.
In four patients, lesions discovered in the small intestine and stomach were presumed to be responsible for intermittent melaena and severe anaemia after exclusion of other causes, and prompted us to propose therapeutic options. Propranolol was administered to the four patients, and a TIPS was further implanted in one patient who was a nonresponder to β-blockers. Both clinical (anaemia and need for transfusions) and endoscopic features improved by lowering portal pressure, again underscoring the role of portal hypertension in the pathogenesis of these lesions. Similarly, the patient with multiple intestinal red bump lesions described by Tang et al. 15 presented no further GI bleeding after 80 mg/d propranolol administration, and the disappearance of small bowel lesions after orthotopic liver transplantation. The effect of TIPS on small bowel varices, oedema, and red spots related to portal hypertension was recently reported, 16 but its efficacy toward polypoid lesions has not been reported. In the 10 other patients who were asymptomatic, no specific treatment was proposed except for endoscopic polypectomy for diagnostic purposes. Interestingly, long-term follow up gastroscopy did not show any recurrence of these lesions.
In conclusion, this series reports a poorly known and rare endoscopic entity associated with portal hypertension, characterized by polypoid lesions either in the stomach or small intestine. These may be associated with significant bleeding and seem responsive to adequate treatment of portal hypertension. Further large, multicentre, prospective studies are required to confirm their response to the treatment of portal hypertension.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there is no conflict of interest.