
Abstract
Introduction
The ideal way of preparing patients for small-bowel capsule endoscopy has been controversial. Previous studies have shown that ingestion of 2 l of polyethylenglycol (PEG) 12 hours prior to capsule ingestion leads to improved visibility in comparison to no preparation at all. We speculated that using a post-ingestion (PI), booster-based cleansing protocol might provide an alternative to the PEG cleansing protocol.
Methods
This randomized, blinded, prospective study enrolled 45 individuals. Patients were allocated to either of two groups. The PEG group ingested 2 l PEG 12 hours prior to the exam (n = 22) and the PI group ingested one sachet of Picolax® dissolved in 250 ml of water one hour after swallowing the capsule with 500 ml of water (n = 18). Primary endpoints were overall small bowel and distal third of small bowel cleansing levels. Secondary endpoints were average gastric and small-bowel transit time.
Results
Forty-five patients participated in this study. Five individuals were excluded because of incomplete study. Percentage of patients with adequate visibility in the distal third of the small bowel in the PEG group was 9% vs 72% in the PI group (p < 0.0001). Average gastric time and total transit time were shorter in the PI group vs the PEG group (p = 0.0065).
Conclusion
Timing of ingestion of the Picolax® purgative 60 minutes after swallowing the capsule endoscopy delivers better visibility in the distal third of the small bowel than the accepted cleansing protocol of ingesting 2 l PEG 12 hours prior to the capsule endoscopy procedure.
Introduction
Capsule endoscopy of the small bowel arrived in 2001 and has revolutionized the inspection of the small bowel. The most common indications for capsule endoscopy are obscure gastrointestinal bleeding and suspected Crohn’s disease. The ideal way to prepare the patient for capsule endoscopy has been controversial. Given Imaging, the first producer of capsule endoscopes, recommends that physicians have no need to give their patients purgatives prior to capsule endoscopy. A special diet the day prior to the procedure and an overnight fast (8–12 hours) is sufficient. Indeed, this protocol was used in the controlled studies of obscure gastrointestinal bleeding and of suspected or established Crohn’s disease. In 2007 the first consensus paper on capsule endoscopy produced by experts reviewing the literature discussed the value of bowel lavage prior to capsule endoscopy. They reached the following conclusion: “The current evidence mainly from fully published papers suggests the PEG lavage and simethicone both positively affect mucosal visibility and perhaps also diagnostic yield.” 1 In the meanwhile, seven randomized, controlled studies have addressed the question whether a purgative improves bowel visibility, diagnostic yield and completion rate.2–8 At this point three meta-analyses conclude that the ingestion of 2 liters of polyethylenglycol (PEG) 12 hours prior to capsule ingestion leads to improved visibility of the small-bowel mucosa, although it does not affect completion rate and in reference to diagnostic yield the jury is still out.9–11 Our experience with colon capsule endoscopy provided us with unmatched quality of visibility of the small bowel, especially the distal small bowel, which often suffers from compromised visibility. 3 In colon capsule endoscopy, participants ingested 4 liters of PEG in divided doses. More important, though, these patients were required to ingest a booster (Na phosphate, Suprep®) to propel PillCam Colon® through the intestinal tract and clear the bowels of accumulated debris.12,13 We speculated that the improved visibility of the small-bowel mucosa was due to the booster effect. We gave 16 consecutive patients enrolled for small-bowel capsule endoscopy Picolax® dissolved in 250 cc of water followed by an additional 500 cc of water one hour after ingestion (post-ingestion purge) of the small-bowel capsule and compared the quality of visibility to that of 10 consecutive historical controls. Our results indicated that the visibility of the distal ileum was indeed improved. To test our hypothesis we proposed to use a post-ingestion purge in small-bowel capsule endoscopy and compare its performance to that of established 2 liter PEG bowel preparation (pre-ingestion purge) in a randomized, controlled trial with blinded investigators and readers. Our primary endpoints were quality of overall small-bowel visibility (entire small bowel), quality of visibility in the distal third of the small bowel and small-bowel transit time.
Methods
This is a randomized, blinded, prospective study enrolling 40 evaluable individuals. All patients were referred to our institution for established indications of small-bowel capsule endoscopy (Figure 1). The secretarial staff randomly assigned the patients to either of two groups while the investigators remained blinded. Sample size was not calculated since we related to this study as a preliminary pilot study to verify whether our observation of a post-ingestion purge was effective.
Flow of study participants.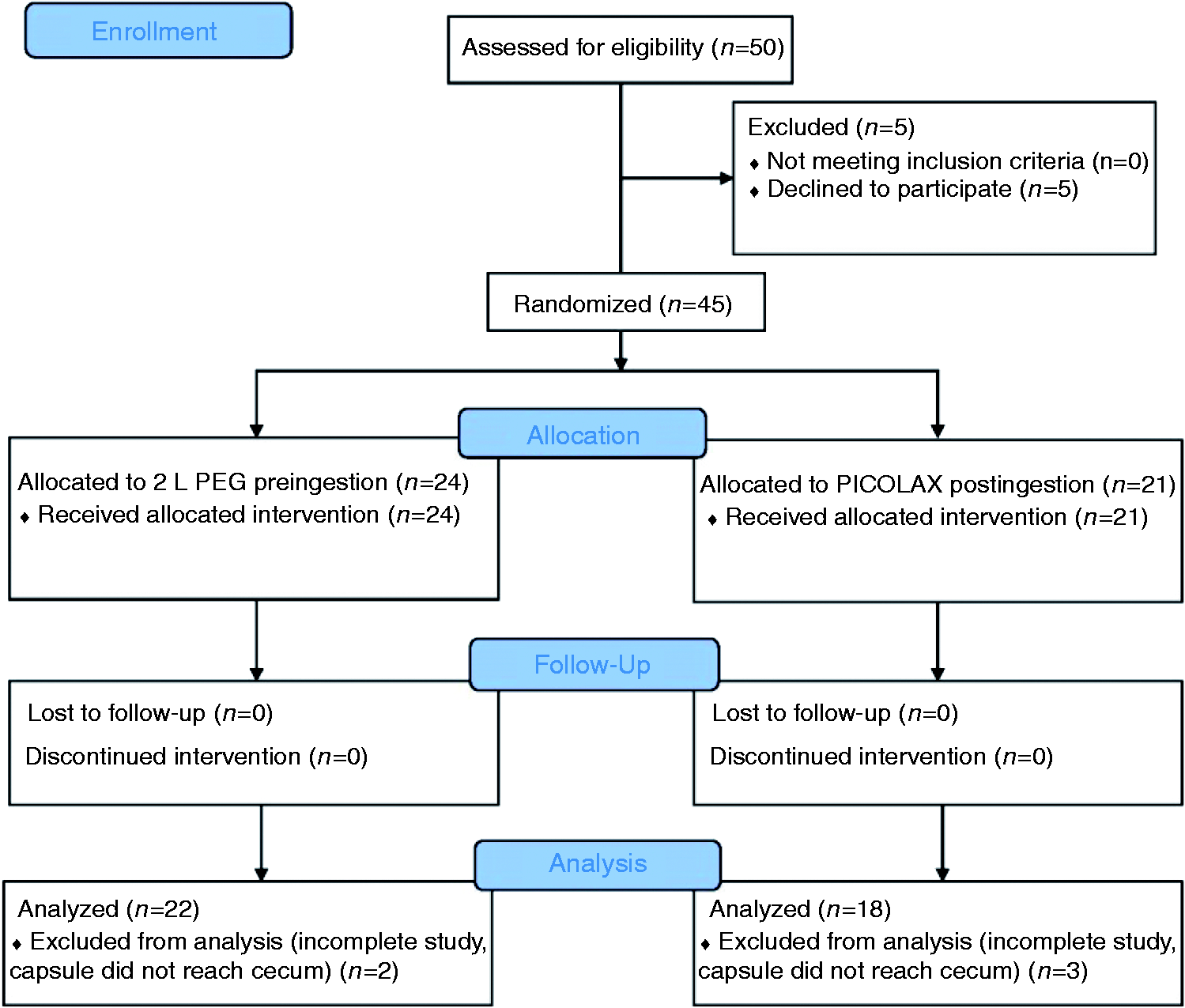
Group 1: PEG (pre-ingestion purge)
These patients received standard small-bowel preparation that included a low-residue diet the day prior to the exam, and from 2 p.m. on the day prior to the exam patients had clear liquids only. The evening prior to the exam (12 hours prior to the test) these patients ingested 2 l of PEG (pre-ingestion purge). On the day of the test, the patient arrived fasting for capsule ingestion.
Group 2: Picolax® (post-ingestion purge preparation)
These patients participated in the new post-ingestion purge preparation. All patients kept to a low-residue diet on the day prior to the exam and from 2 p.m. on the day prior to the exam had clear liquids only. No purgatives were taken the evening before. On the day of exam, the patient arrived fasting for capsule ingestion. One hour after ingestion of the capsule the patients drank one sachet of Picolax® dissolved in 250 ml of water followed by another 500 cc of water.
We used PillCam® SB3 in this study, with Sensor Belt and Data Recorder3 (DR3) recorder (Given Imaging, Yokneam, Israel). This capsule transmits varying frames per second (2–5 fps) to the DR3 recorder; while stationary, the capsule transmits 2 fps, while in motion 5 fps. 14 Our technicians downloaded all completed studies to a computer with Rapid8® software.
An experienced capsule endoscopist (more than 2000 capsule studies) graded the cleansing quality of the small-bowel preparation. We used a grading scale of 1 to 4 that was used in previous studies.15,16 Four was excellent (no more than small bits of residue), 3 was good (some residue, not enough to interfere with the examination), 2 was fair (enough residue to preclude a completely reliable examination) and 1 was poor (large amount of residue). Patients with good and excellent preparation (grade 3 and 4) were defined as adequate and patients with fair and poor preparation (grade 1 and 2) were defined as inadequate. The blinded reviewer assessed the cleansing quality of the entire small bowel as well as the distal third of the small bowel. Small-bowel transit time was divided by three. The final third of the small-bowel transit time was defined as the distal third of the small bowel.
For the evaluation of the association between study groups and categorical variables, we used the Chi-square test (or Fisher’s exact test). We used the Wilcoxon two-sample test for evaluation of continuous variables. The statistical analysis was performed with SAA 9.4 software. A value smaller than p = 0.05 was considered statistically significant.
The institutional review board of Shaare Zedek Medical Center, Jerusalem, approved our study on January 7, 2015. All patients signed informed consent prior to participation in this study.
Results
Demographics and indication for capsule study.
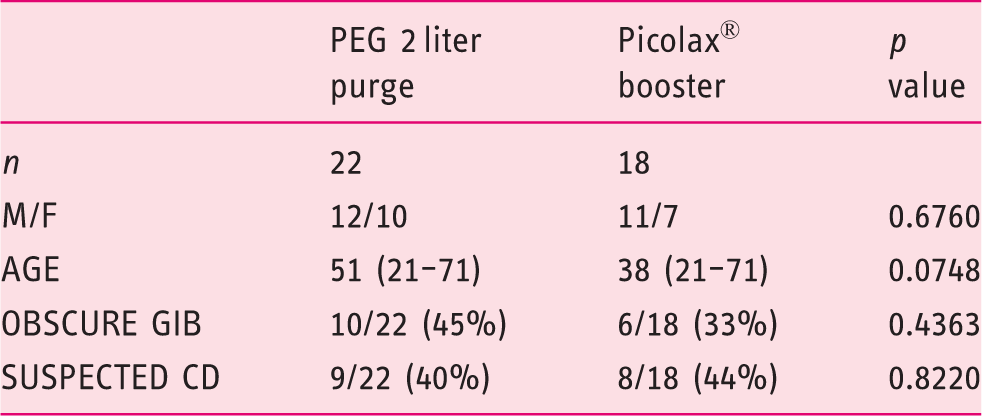
PEG: polyethylenglycol; M: male; F: female; GIB: gastrointestinal bleeding; CD: Crohn’s disease.
The mean overall quality of visibility in the PEG group was 2.77, and 2.83 for the Picolax® post-ingestion group. This difference is statistically not significant (p = 0.687).
The mean visibility score in the distal third of the small bowel in the PEG group was 2.04 and for the Picolax® post-ingestion group 2.83. This difference is statistically significant (p < 0.0001). The percentage of patients with adequate visibility in the distal third of the small bowel in the PEG group was only 9% vs 72% in the Picolax® post-ingestion group (p < 0.0001) (see Figure 2).
Quality of visibility in the distal third of the small bowel (%).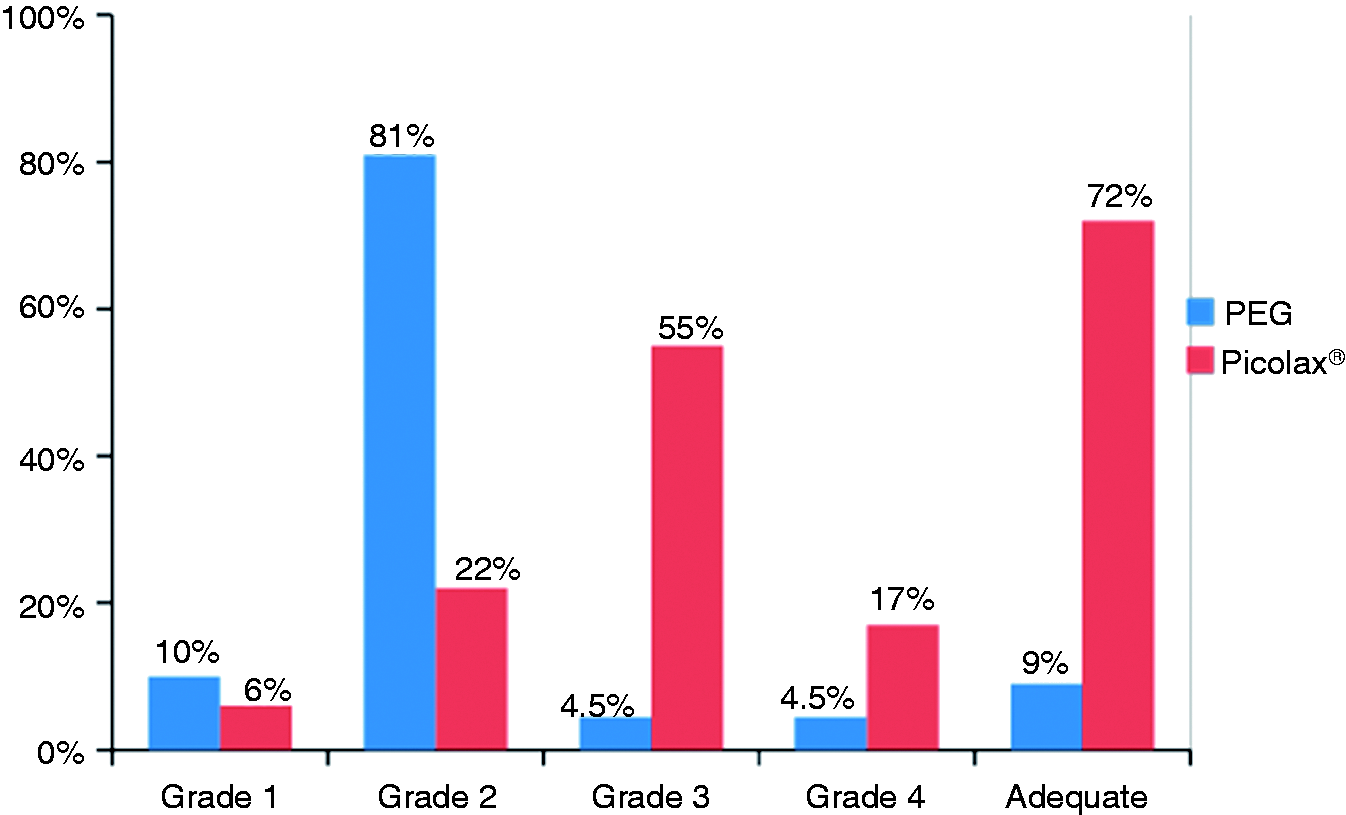
Findings and diagnostic findings at capsule endoscopy.
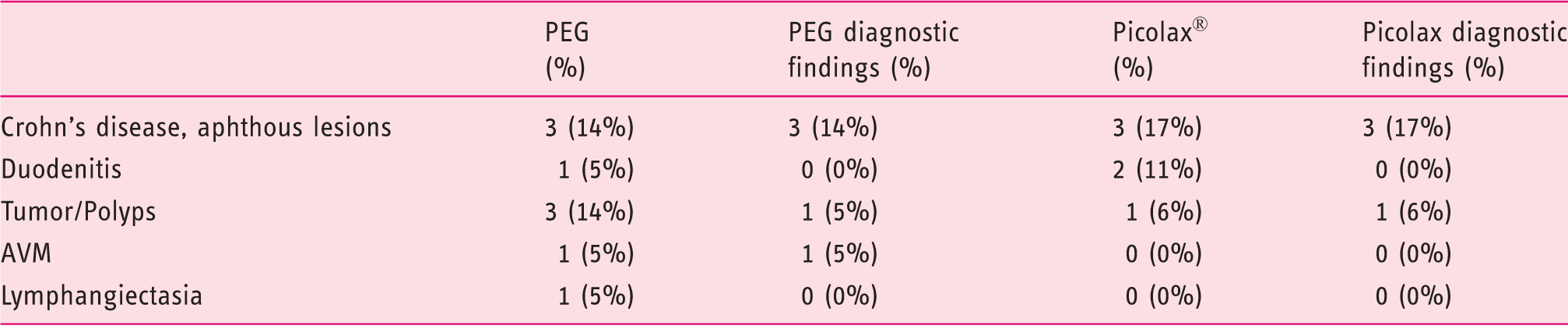
PEG: polyethylenglycol; AVM: arteriovenous malformation.
Gastric and small bowel transit times.

PEG: polyethylenglycol; h: hour; m: minutes; s: seconds.
The investigators recorded reading time. The average reading time for pre-ingestion PEG purge was 15.7 minutes and the average reading time for post-ingestion Picolax® purge was 13.7. The sample size was too small to reach statistical significance (p = 0.49).
Discussion
Our two groups were properly randomized as the demographics show. The indications for capsule endoscopy were similar in both groups. The proximal small bowel is often sufficiently clean by fasting alone. For this reason, it is not surprising that there was no statistical difference for overall quality of visibility between the two groups. Our study results demonstrate that the post-procedure ingestion of Picolax® purge delivers a cleaner distal small bowel than the pre-procedure ingestion of 2 liters of PEG. Post-procedure Picolax® provides adequate bowel preparation in 72% of patients vs 9% in the PEG group (see Figure 2). It is the distal part of the small bowel that is often affected by debris and dark intestinal fluid. Van Tuyl et al. report in their prospective, controlled, randomized study that the quality of visibility in the terminal ileum was good in only 25% of that group that received no purgatives prior to capsule endoscopy. 3 Whether improved visibility leads to improved diagnostic findings remains controversial. 11 In this study, we recorded diagnostic findings, which showed no significant difference between the two groups (Table 2). This first pilot study was underpowered for demonstrating increased diagnostic yield between the two groups. The fact that small-bowel transit time of the capsule is reduced by post-procedure ingestion of Picolax® is not surprising. Picolax® acts not only as a purgative but also as a propellant. There is concern that the faster transit may prevent the capsule from photographing the relevant findings and curtail diagnostic sensitivity. One needs to keep in mind, though, that the SB3 capsule has an adjustable frame rate transmission. While in motion the capsule increases the transmission rate from two images per second to five images per second.14,17 The shorter small bowel transit time is welcome for patient and reader. Average reading time was shorter in the post-ingestion Picolax® purge group; however, our sample size was too small to deliver a statistically significant result. Our results are in agreement with the experience of others. Endo et al. report that in a prospective blinded study the ingestion of 500 cc of PEG 30 minutes after capsule ingestion led to statistically significant improvement of visibility, especially in the distal ileum. 18 In a randomized, controlled trial, Ito et al. gave 500 cc of PEG post-capsule ingestion and compared the quality of visibility to those patients who received no purgatives. Here, as well, improved visibility was noticed along the entire small bowel, especially in the distal ileum (p = 0.00004). 19 In a prospective study, Hosono et al., using real-time reading, gave patients whose capsule reached the small bowel one hour after capsule ingestion 500 ml of PEG. Here too, the ingestion of 500 ml of PEG after the capsule entered the small bowel improved the quality of visibility in the distal small bowel (image quality score 1.6 vs 3.0). 20 Our experience, the experience of our Japanese colleagues and the experience with colon capsule endoscopy purges raises the question whether our approach to small-bowel capsule endoscopy purges is flawed. The initial recommendations for small-bowel purges relied on our experience of purging the colon for colonoscopy. Hence the recommendation to take 2 to 4 l of PEG prior to capsule ingestion, the same way we recommend the ingestion of PEG prior to colonoscopy. Yet the conditions in the colon are fundamentally different from those in the small bowel. While the proximal small bowel is as a rule clean in the fasting state, the colon is laden with fecal debris. The distal small bowel accumulates debris and dark bile. After washing this accumulated debris with PEG the evening before, there is ample time for debris to accumulate again. For this reason, the timing of purgative ingestion is the key factor for obtaining a clean distal small bowel. In the future, better timing for purgative ingestion can be obtained. We chose the one-hour mark, since by experience more than 90% of capsules will have left the stomach at that time. The ideal time for ingestion of the purgative theoretically would be precisely once the capsule leaves the stomach and enters the small bowel. The technology to determine this event already exists. The DR3 can recognize the presence of the capsule in the small bowel. 21 Future studies will verify if this assumption is correct. Finally, we should not forget two considerations, one is convenience for the patient and the other is cost. There is no question that ingesting Picolax® during the procedure is preferable over drinking 2 l of PEG the evening before. In Israel a 3 liter canister of PEG sells for US $33 whereas an original package of Picolax® sells for US $16.
In conclusion: The timing of ingestion of Picolax® purgative 60 minutes after swallowing the capsule endoscope delivers better visibility in the distal third of the small bowel than the accepted cleansing protocol of ingesting 2 l PEG 12 hours prior to the capsule endoscopy procedure.
Footnotes
Acknowledgment
The authors would like to acknowledge the contribution of Dr Naama Schwartz, PhD, for her assistance in this research and biostatistics.
Declaration of conflicting interests
The capsules for this study were donated by Covidien; the company had no access to the patient data during the entire study or thereafter. SNA was a consultant for Covidien in the past. SF is an employee of the Covidien R&D Department.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.