
Abstract
Introduction
Small bowel angiodysplasias account for over 50% of causes of small bowel bleeding and carry a worse prognosis than lesions located elsewhere in the gastrointestinal tract. Re-bleeding rates are high even after first-line endoscopic therapy and are associated with high levels of morbidity for affected patients. Small trials of long-acting somatostatin analogues have shown promising results but have not yet been assessed in patients with refractory small bowel disease.
Aim
The purpose of this study was to assess the effect of long-acting somatostatin analogues in reducing re-bleeding rates and transfusion requirements, and improving haemoglobin levels in patients with refractory small bowel angiodysplasia.
Methods
Patients with refractory small bowel angiodysplasia were treated with 20 mg of long-acting octreotide for a minimum of three months. Response was assessed according to: rates of re-bleeding, haemoglobin levels, transfusion requirements, and side effects.
Results
A total of 24 patients were initially treated and 20 received at least three doses. Rates of complete, partial and non-response were 70%, 20% and 10% respectively. Average haemoglobin rates increased from 9.19 g/dl to 11.35 g/dl (p = 0.0027, 95% confidence interval (CI) −3.5 to −1.1) in the group overall and 70% remained transfusion-free after a mean treatment duration of 8.8 months. The rate of adverse events was higher than previously reported at 30%.
Conclusion
Long-acting somatostatin analogues offer a therapeutic advantage in a significant proportion of patients with small bowel angiodysplasia. With careful patient selection and close observation, a long-acting somatostatin analogue should be considered in all patients with persistent anaemia attributable to refractory disease in conjunction with other standard treatments.
Introduction
Small bowel angiodysplasias (SBAs) account for up to 60% of cases of obscure gastrointestinal bleeding (OGIB). 1 Angiodysplasias are known to bleed recurrently, with up to 70% re-bleeding within two years of initial presentation. 2 SBA patients are known to be elderly and to have multiple co-morbidities. 3 In addition, lesions in the small bowel are thought to have a worse prognosis than lesions elsewhere. 4
Although small bowel imaging and endoscopic techniques have improved the diagnosis of OGIB, the development of effective treatments for SBA is still lacking, as evidenced by numerous studies reporting high rates of persistent anaemia despite treatment.5–7
Many patients become dependent on empirical iron and red cell transfusions, which are suboptimal at controlling their anaemia, leading to exacerbation of their co-morbidities, an impaired quality of life and a significant burden on hospital resources.8,9
The most effective treatment available is argon plasma coagulation (APC) via double balloon enteroscopy (DBE). 10 However, there are variable reports of efficacy, with re-bleeding rates ranging from 11–57% at one year of follow up.11,12 There are a number of limitations of DBE; the entire small bowel is rarely visualised during a single procedure, leaving the possibility of untreated lesions, and lesions can grow in new sites sporadically, making its use as the sole treatment often futile. 13
Medical treatments have been tried with varying levels of success. Despite initial beneficial reports of oestrogen, a recent randomised controlled study has shown it to be ineffective in angiodysplasia. 14 Thalidomide has shown some effect in small randomised controlled trials but due to its high rates of serious side effects is rarely used as first-line treatment. 15 The development of more specific treatments for SBAs is limited by a lack of understanding of the pathophysiology behind their formation.
Somatostatin is a cyclic peptide secreted by a number of gastrointestinal cells which reduces bleeding by a number of mechanisms: increasing platelet aggregation, reducing splanchnic blood flow, increasing vascular bed resistance and down-regulation of vascular endothelial growth factor. 3 Long-acting somatostatin analogues are used safely as a long-term medication in patients with acromegaly with very few side effects. 16 The use of somatostatin analogues in gastrointestinal angiodysplasias has been reported in a number of small trials and case reports, initially via subcutaneous administration, and more recently via a long-acting monthly intramuscular injection.17–19 Their use specifically in small bowel lesions which are known to be more difficult to treat has not yet been evaluated, but it may offer a synergistic treatment option alongside APC in those with refractory angiodysplasias.
The aims of this study were to evaluate the effect of a once monthly intramuscular injection of a long-acting somatostatin analogue on; haemoglobin levels, re-bleeding and transfusion requirements in patients with refractory SBA.
Methods
Patient group
Ethical approval was obtained from the ethics committee of our institution. All patients with a diagnosis of SBA, attending our gastroenterology department, over the age of 18 years, and capable of providing written informed consent were considered for inclusion. SBA was diagnosed by small bowel capsule endoscopy (SBCE) or DBE. At SBCE, lesions were assigned a P value. 20 Only patients with definite (P2) lesions, who had undergone a negative workup for anaemia, including upper and lower endoscopy were included. Further to this, patients had to have refractory disease; defined as persistent anaemia for greater than 12 months despite iron replacement with or without RCC (red cell concentrate) transfusions.
Study design
This was an open label uncontrolled proof of concept study. Suitable patients were provided with information on the medication and informed consent was obtained. All patients were prescribed 20 mg of long-acting octreotide intramuscularly on a monthly basis, which was obtained by the patient from their community pharmacy. Patients who had lesions amenable to treatment with APC via DBE, who were fit to undergo the procedure did so prior to commencing octreotide. No alterations were made to any other medications and patients continued to receive iron and red cell transfusions as required.
Patient follow-up
Patients were assessed on a monthly basis where a record was made of any adverse effects, overt bleeding episodes, transfusion requirements, and follow-up haemoglobin levels were checked. A re-bleeding episode was defined as either an overt episode of melaena or haematochezia, or a decrease in haemoglobin of >2 g/dl. RCC transfusions were prescribed when haemoglobin levels fell <8 g/dl in general, and <10 g/dl in patients with cardiopulmonary compromise. A decision was made to discontinue the medication in any patient who suffered what was deemed a serious side effect by the clinical team, or in patients who had undergone more than six months of treatment without a beneficial effect.
Statistical analysis
Response to treatment was defined as complete: no re-bleeding episodes or transfusion requirements; partial: a reduction in re-bleeding frequency or transfusion requirements; or non-response. Statistical analysis was performed using SPSS version 20 (Chicago, Illinois, USA). Results were compared between groups using a one-sided students t-test or Mann Whitney U test with a p value of <0.05 considered significant. Prediction of response over time was assessed using Spearman’s rho test, with a p value of <0.01 considered significant.
Results
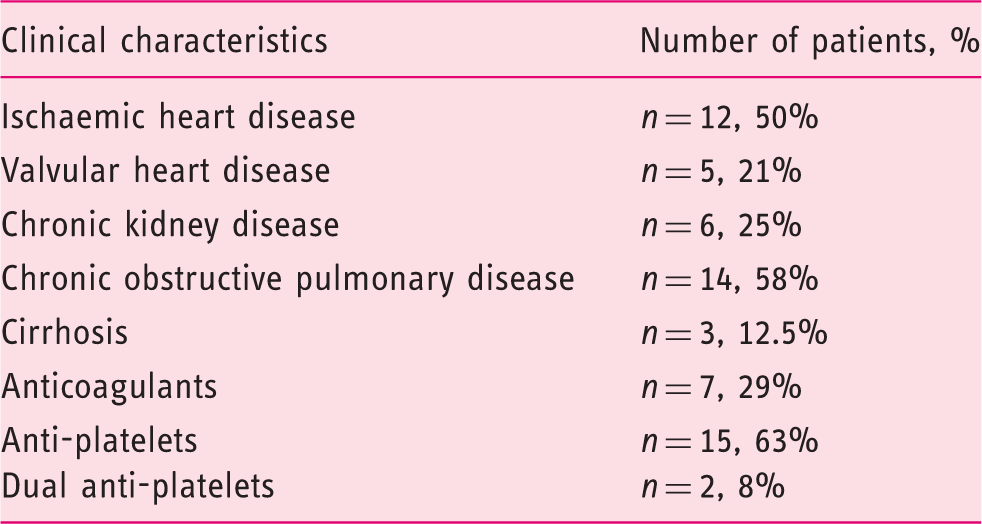
Demographics
Clinical characteristics of the 24 patients commenced on octreotide
Treatment effects
A total of 83% (n = 20) of patients received at least three doses of long-acting octreotide and were included in the analysis. In the group overall the mean treatment duration was 8.8 months (range 3–17). In all, 70% (n = 14) were complete responders, 20% (n = 4) were partial responders and 10% (n = 2) were non-responders (Figure 1).
Haemoglobin levels pre and during treatment according to response classification.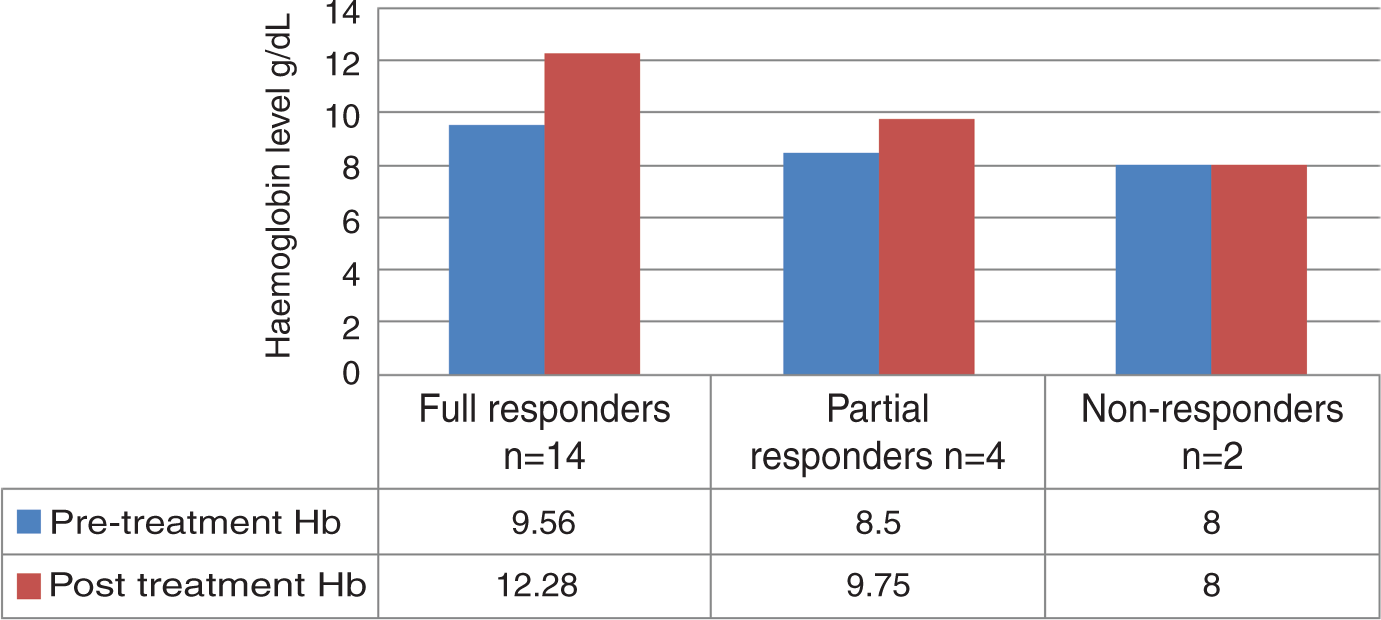
There was a significant increase in haemoglobin levels overall in patients pre- and post-treatment, with median levels rising from 9.19 g/dl to 11.35 g/dl (p = 0.0027, 95% confidence interval (CI) −3.5 to −1.1), and from 8.96 g/dl to 11.57 g/dl, and 9.13 g/dl to 11.1 g/dl in females and males respectively. Three-month and six-month haemoglobin levels were predictive of overall response with correlation coefficients of 0.84 and 0.87 respectively, p < 0.01 (Figure 2).
Mean haemoglobin levels (g/dl) of patients before and during treatment.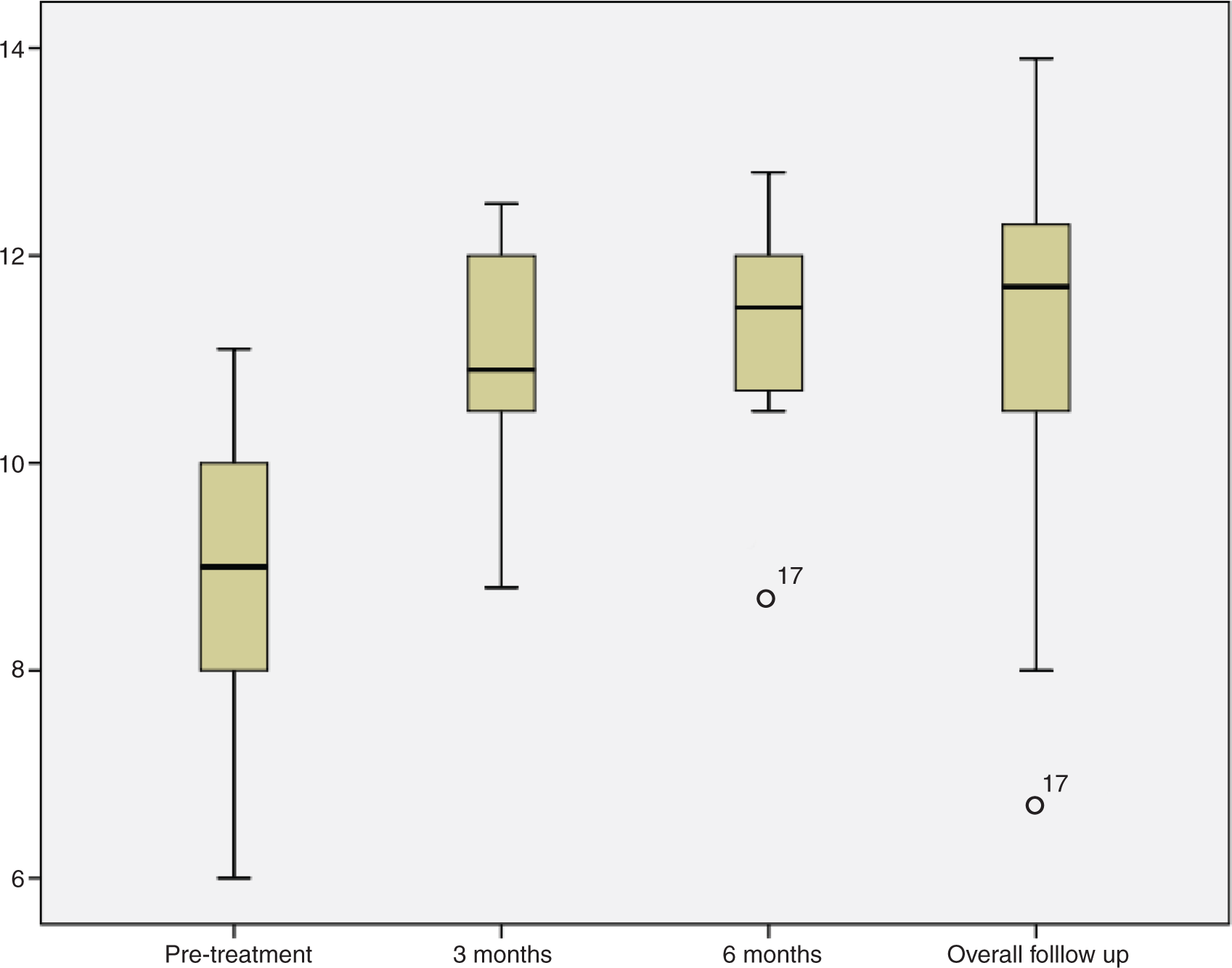
Re-bleeding episodes occurred in 30% of patients (n = 6), with overt bleeding in four patients. In one patient this occurred after missing two consecutive doses, a further patient required surgery for uncontrolled bleeding from a caecal angiodysplasia. Of the re-bleeders, octreotide was discontinued in 33% (n = 2). Only one patient with re-bleeding was on warfarin therapy, the remaining five patients were on anti-platelet therapy; however these factors were not statistically significant.
Of the 20 patients, transfusion requirements were significantly reduced in the group overall, with 70% (n = 14) remaining free of transfusions while on treatment, and mean requirements falling from 1.35 units/month pre-treatment to 0.31 units/month during treatment (p < 0.001, 95% CI 0.92–1.71). Of those requiring RCC transfusions, the number of transfusions decreased significantly from a mean of 2.25 units/month to 1.07 units/month during treatment (p = 0.002, 95% CI 1.33–3.17).
With regard to patients treated with APC: all patients underwent a single DBE and APC attempt prior to commencement of octreotide. there was a significantly higher haemoglobin level at three months with mean levels of 11.69 g/dl compared to 9.55 g/dl in those without APC (p = 0.011, 95% CI 0.54–3.73). However, by six months and at overall follow up, this trend was no longer significant, with levels of 11.53 g/dl vs 10.97 g/dl (p = 0.457), and 11.74 g/dl and 9.78 g/dl (p = 0.87).
A total of four patients died during the study, with SBA a direct cause of mortality in two (8.3%) cases. The remaining two deaths were secondary to metastatic lung cancer.
Treatment safety
Treatment was discontinued in eight patients (30%); five due to adverse events, one underwent a hemicolectomy for a bleeding caecal lesion and did not resume treatment, one as no beneficial effect was observed after at least 12 months, and a further patient was lost to follow up. There were five adverse events which led to treatment discontinuation. These included; an acute blistering skin reaction, thrombocytopenia with platelets falling from 357 × 109/l to 22 × 109/l, choledocholithiasis and biliary sepsis, severe generalised joint pains, and severe pain around the injection site. All adverse events resolved with conservative management on withdrawal of octreotide. In addition, two patients reported mild diarrhoea and nausea within 48 h of their first dose which did not recur on subsequent doses. There was only one diabetic patient in the study who did not experience any changes in blood sugar control or insulin requirements.
Discussion
This study shows a clear benefit of long-acting somatostatin analogues in refractory SBA. This is in keeping with previous studies by Bon et al.,19 and Molina et al.,21 and a number of case reports using short-acting somatostatin analogues in gastrointestinal angiodysplasias. In our study, 90% (n = 18) had a beneficial clinical response, with mean haemoglobin levels in the group overall increasing by >2 g/dl, and transfusion requirements falling from 100% to only 30% at follow-up. For a group of patients with refractory disease who were anaemic for a minimum of 12 months, this represents a major therapeutic advantage.
Although octreotide undoubtedly had positive effects on haemoglobin levels, there are a number of difficulties in quantifying its exact clinical benefit. A recognised obstacle in assessing the benefit of any treatment in SBA is the poorly defined natural history of the condition, and the ethical arguments against enrolling a control group. 21 As the timing of re-bleeding is so unpredictable, it is difficult to differentiate whether the outcome is due to the effect of the medication or the likelihood of a natural bleeding free interval. As there are currently no specific guidelines for the treatment of SBA available, treatment decisions within each institution are made on an ad-hoc basis, guided by the availability of small bowel endoscopy. Where this resource is not available, patients are often managed conservatively with RCC and iron transfusions, however; if DBE is available it is generally used which makes comparison of control and treatment groups between different institutions difficult. In our study, as with previous studies, there was no control group. However, all of our patients had required transfusions at least three months prior to commencing the study and all had been persistently anaemic for at least 12 months. So, in effect, a patient’s own pre-treatment history could be considered their control, with 100% (n = 20) re-bleeding rates, reducing to only 25% (n = 6) during treatment.
As with Bon et al., our inclusion criteria were broad and the patient cohort was variable but this reflects clinical practice. A recent retrospective study has recommended a risk stratification policy to identify patients at higher risk of re-bleeding, and less likely to respond to medical therapy. 22 Key at-risk factors included older age, chronic obstructive pulmonary disease (COPD) and anti-platelet therapy, factors almost universally present in our cohort. The treatment effect demonstrated in this cohort was good but there remains the possibility that earlier treatment and selection of a less resistant group could improve outcome even more.
A second difficulty in assessing the efficacy of octreotide is the fact that 83% of patients had treatment with APC which occurred within a week of commencing octreotide therapy. APC is currently the recommended therapy for SBA. However, despite this, studies with prolonged follow up have shown that re-bleeding rates can be up to 57% at one year, similar to the reported natural history of the condition itself. This has led to recent debate that DBE and APC may not be worth the risk of complications for the patient, and the financial burden to institutions. Our study showed that by six months the benefit of APC therapy over octreotide treatment alone was no longer significant, suggesting that the benefit of APC is short-lived, although the number of patients receiving octreotide alone in this study was admittedly small. In addition, due to the retrospective nature of the study it was not possible to determine from the endoscopy reports whether all lesions seen on SBCE were detected and treated during the subsequent DBE, meaning that some lesions may have remained untreated, which may be a confounding factor.
This is the largest published cohort to date of patients treated with long-acting somatostatin analogues; however we have used shorter minimum treatment duration than other studies. The duration of three months can be validated by our results, showing no differences in haemoglobin levels in the group overall after three or six months, or after mean treatment duration of 8.8 months. In the six non- and partial-responders, there was also no difference in haemoglobin level or transfusion requirements at three, six or 12 months of treatment. A similar study by Scaglione et al., treated 13 patients with 10 mg of a long-acting somatostatin analogue, they increased the dose to 20 mg after 12 months in non-responders, and found no additional beneficial response. 17 These findings would suggest that a three-month trial of 20 mg is sufficient to determine patient response, although this theory would need to be tested in a sufficiently powered study prior to being employed in clinical practice.
One of the unexpected findings in this study was the relatively high rate of adverse events compared to other studies. Thrombocytopenia has been reported in case reports in the literature, and although rare, is a particularly unwanted consequence in a patient with gastrointestinal haemorrhage. Fortunately, there was rapid resolution of the platelet count on withdrawal of therapy. Gallstones are a recognised complication of somatostatin analogues, and although not a serious side effect in the majority of patients, can lead to potentially fatal outcomes in frail or immunocompromised patients, and this and the possibility of rarer adverse events, needs to be carefully considered prior to commencing treatment. The milder side effects such as local reactions and joint pains could possibly be dose related, and although not carried out during this study, a reduction to 10 mg per month, or subcutaneous administration may be an option in patients who have exhausted all other treatment options. It must be noted that although the rate of adverse events was high at 30%, it is less than that reported for thalidomide, which has been reported to be as high as 71%. 15
SBA impacts hugely on patient morbidity, and due to poorly specific treatments, results in a huge burden on healthcare resources for admissions for RCC transfusions and repeat endoscopic procedures. Although this study did not formally assess the quality of life or cost-effectiveness of long-acting somatostatin analogues, it can be presumed that by the dramatic reduction in dependency on transfusions, from 100% to only 30% that it would have had a significant impact on both. The mortality of gastrointestinal angiodysplasias overall has been estimated to be 2% per hospital admission. 23 As mentioned earlier, the prognosis for lesions in the small bowel may be worse, as evidenced in this study as 8.3%, however the overall number of patients recruited in this study is small, and further studies on the natural history of SBA would be required to accurately describe SBA mortality rates. As the majority of patients suffer from cardiac and respiratory conditions, both of which are exacerbated by anaemia, any medication which improves their mean haemoglobin level has the potential to dramatically improve both their quality of life and morbidity levels.
Conclusion
Somatostatin analogues show a potential therapeutic advantage in improving haemoglobin levels and reducing transfusion requirements in patients with refractory SBA in conjunction with current standards of treatment. Although careful patient selection and close monitoring for adverse events is required, somatostatin analogues should be considered in all patients with refractory SBA.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.