
Abstract
Background
Device-assisted enteroscopies (DAEs) are recent endoscopic techniques that enable direct endoscopic small-bowel evaluation.
Objective
The objective of this article is to evaluate the implementation of DAEs in Portugal and assess the main indications, diagnoses, diagnostic yield, therapeutic yield and complication rate.
Methods
We conducted a multicenter retrospective series using a national Web-based survey on behalf of the Portuguese Small-Bowel Study Group. Participants were asked to fill out two online databases regarding procedural data, indications, diagnoses, endoscopic therapy and complications using prospectively collected institutional data records.
Results
A total of eight centers were enrolled in the survey, corresponding to 1411 DAEs. The most frequent indications were obscure gastrointestinal bleeding (OGIB), inflammatory bowel disease and small-bowel tumors. The pooled diagnostic yield was 63%. A relation between the diagnostic yield and the indications was clear, with a diagnostic yield for OGIB of 69% (p = 0.02) with a 52% therapeutic yield. Complications occurred in 1.2%, with a major complication rate of 0.57%. Perforations occurred in four patients (0.28%).
Conclusion
DAEs are safe and effective procedures, with complication rates of 1.2%, the most serious of which is perforation. Most procedures are performed in the setting of OGIB. Diagnostic and therapeutic yields are dependent on the indication, hence appropriate patient selection is crucial.
Keywords
Introduction
In recent years, two major innovations revolutionized small-bowel endoscopic exploration: capsule endoscopy (CE) and deep enteroscopy. CE was developed in 2001 1 and rapidly evolved as the ideal technique for the endoscopic evaluation of small-bowel pathology, as it is a safe, easy and noninvasive technique that enables complete small-bowel visualization. However, it has some major limitations, mostly lack of movement control and therapeutic capabilities. Deep enteroscopy, on the other hand, allows direct endoscopic visualization and control, as well as most diagnostic and therapeutic endoscopic techniques. The concept of deep enteroscopy was introduced with the development of double-balloon enteroscopy (DBE) in 2003 by Yamamoto et al. 2 Soon, single-balloon enteroscopy 3 (SBE) and spiral enteroscopy 4 (SE) were also introduced. These techniques are grouped under the designation of device-assisted enteroscopy (DAE).
The experience with DAE mostly relies on single-center series from experienced referral centers, and on multicenter studies also usually from referral centers focusing on specific pathologies or technical comparisons. There is limited evidence on the national use of DAEs in the community, particularly in Portugal.
Hence, the authors aimed to evaluate the Portuguese experience with DAEs, focusing on two different aspects: technical ones, related to the equipment, logistics and training capabilities; and clinical ones such as indications, diagnoses, therapeutic procedures, diagnostic and therapeutic yield and complications.
Methods
We conducted a multicenter retrospective descriptive study of medical centers performing DAEs in Portugal. A national survey of centers performing DAEs was performed, on behalf of the Portuguese Small-Bowel Study Group (GEPID—“Grupo de Estudos Português do Intestino Delgado”), a section of the Portuguese Society of Gastroenterology (SPG—“Sociedade Portuguesa de Gastrenterologia”). A formal invitation letter to participate in the study was sent from the SPG to all Portuguese gastroenterology departments. This invitation letter explained the nature of the multicenter survey and the purpose of data collection. The invitation letter also contained links to two online questionnaires for data collection.
Questionnaires
Centers enrolled in the survey were asked to fill out two online questionnaires. The links sent in the invitation letter gave access to online forms for which only data entry was possible. The deadline for data entry was set to May 7, 2014. Participants were not able to see the questionnaires from other centers. Patients were inserted anonymously by the participants entering data. Access to the database was granted only to investigators directly involved in data analysis.
Questionnaires sent to gastroenterology departments performing device-assisted enteroscopy in Portugal
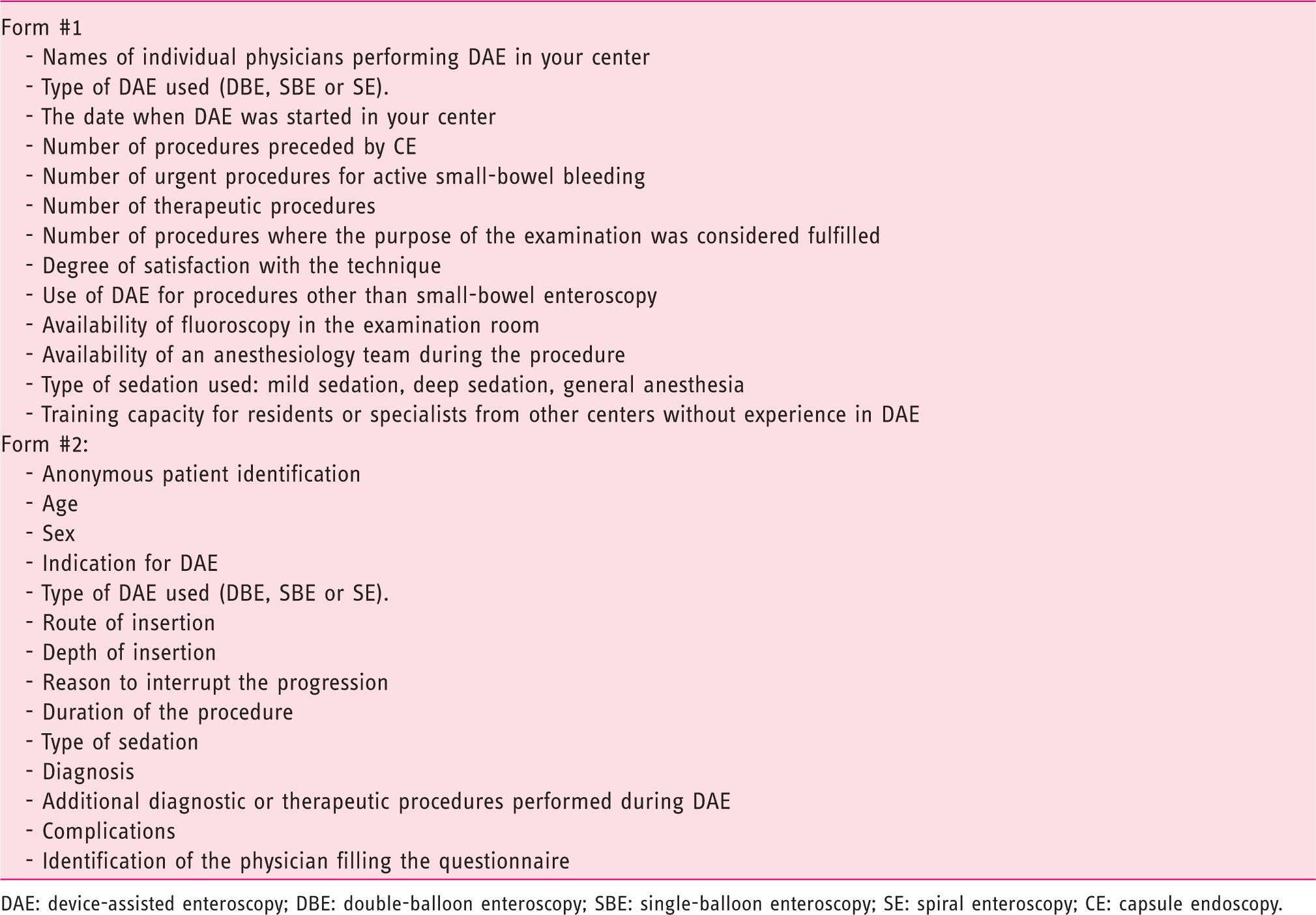
DAE: device-assisted enteroscopy; DBE: double-balloon enteroscopy; SBE: single-balloon enteroscopy; SE: spiral enteroscopy; CE: capsule endoscopy.
DAE procedures
Participants were invited to include all procedures performed until the deadline for data inclusion. All DAE procedures were performed according to each institution’s individual protocol, reflecting standard community practice. Each patient gave informed consent for DAE, complementary diagnostic and therapeutic procedures and sedation. The survey was approved by the ethics committees and both the SPG and GEPID boards.
Statistical analysis
Data from the online forms were exported as an “.xls”-file spreadsheet and imported to SPSS v19.0 for data analysis. Data were reviewed for homogeneity, and inconsistencies and some answers were grouped into different categories when appropriate.
Descriptive statistics were used to summarize data: Fisher’s exact test to compare discrete variables (diagnostic yield, complications); Spearman’s correlation coefficient to correlate the satisfaction score with the total number of procedures; and the Mann-Whitney test was used to compare the satisfaction score with the type of enteroscope.
Results
Individual centers and DAE techniques
Summary of the characteristics of individual centers
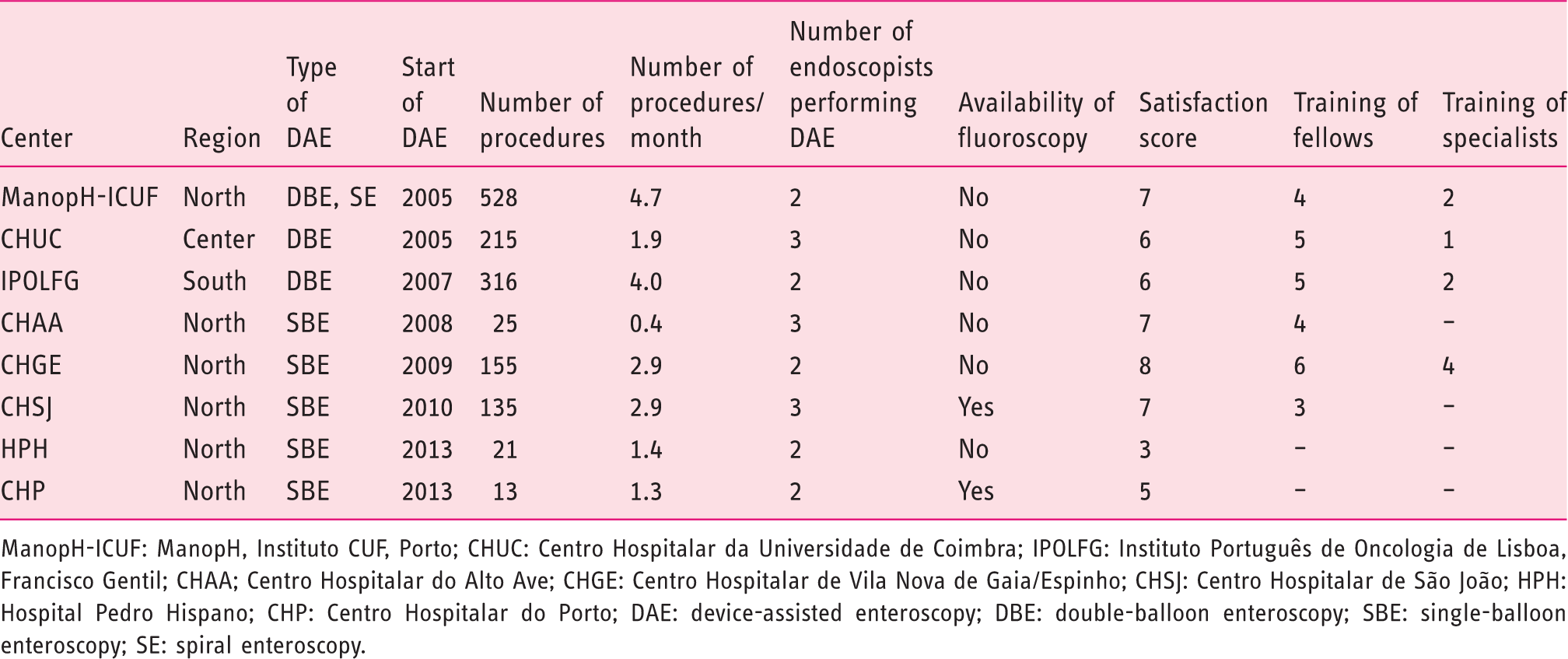
ManopH-ICUF: ManopH, Instituto CUF, Porto; CHUC: Centro Hospitalar da Universidade de Coimbra; IPOLFG: Instituto Português de Oncologia de Lisboa, Francisco Gentil; CHAA; Centro Hospitalar do Alto Ave; CHGE: Centro Hospitalar de Vila Nova de Gaia/Espinho; CHSJ: Centro Hospitalar de São João; HPH: Hospital Pedro Hispano; CHP: Centro Hospitalar do Porto; DAE: device-assisted enteroscopy; DBE: double-balloon enteroscopy; SBE: single-balloon enteroscopy; SE: spiral enteroscopy.
Two of these centers started DAEs in 2005, one in 2007, 2008, 2009, 2010 and two in 2013. The first three centers implementing DAEs adopted DBE and all the remaining centers from 2008 onward selected SBE.
A total of 23 endoscopists have performed DAEs in these eight centers. Currently, 20 of them routinely perform DAEs, ranging from two to three in each center.
Use of DAE
Only three of the eight centers declared using DAE in the emergency setting for active OGIB.
Half (n = 4) of the centers reported using the enteroscope for other purposes than small-bowel enteroscopy (ManopH-ICUF, CHGE, CHUC and HPH), mainly to perform difficult colonoscopies and push enteroscopies. Only two centers (CHGE and HPH) reported its use to perform endoscopic retrograde colangiopancreatography (ERCP) in patients with surgically altered anatomy.
Satisfaction with DAE was evaluated on a subjective analog scale ranging from 0 (no satisfaction) to 10 (complete satisfaction). The median satisfaction score was 6.5 ranging from 3 to 8 and was not correlated with the total number of procedures (p = 0.3) or the type of enteroscope used (p = 0.9).
Only two centers (CHSJ and CHP) have fluoroscopy available in the examination room used to perform DAEs, although all centers (except ManopH-ICUF) have fluoroscopy available in other locations on request.
All participating centers declared having an anesthesiologist during the procedure. In all centers, most cases were performed under deep sedation with propofol without orotracheal intubation. In three centers, 24 (1.7%) patients were examined under general anesthesia and in one center, 55 (3.9%) patients were examined under mild midazolam sedation.
Regarding the capacity to train gastroenterology fellows and specialists from other centers without experience in DAE, six centers reported training capacity. The two centers whose activity started only in 2013 declared no training capacity at their current stage. A total of 27 gastroenterology fellows have already been trained in DAE in the six centers with training capacity. A total of five centers have already trained nine gastroenterology specialists from other centers (CHGE: four, ManopH-ICUF: two, IPOLFG: two and CHUC: one).
Case series
A total of 1411 cases were recorded in the online Form #2, from the eight participating centers. From these, 1054 were DBE, 351 SBE and six SE.
The mean age was 57.6 years (SD 18.3), ranging from 9 to 98 years old. Males accounted for 53.3% of patients. Of the 1411 procedures, 16 (1.1%) were pediatric patients (<18 years old) and 567 (40.2%) were elderly patients (≥ 65 years old).
Indications for DAE, according to the type of DAE and route of insertion
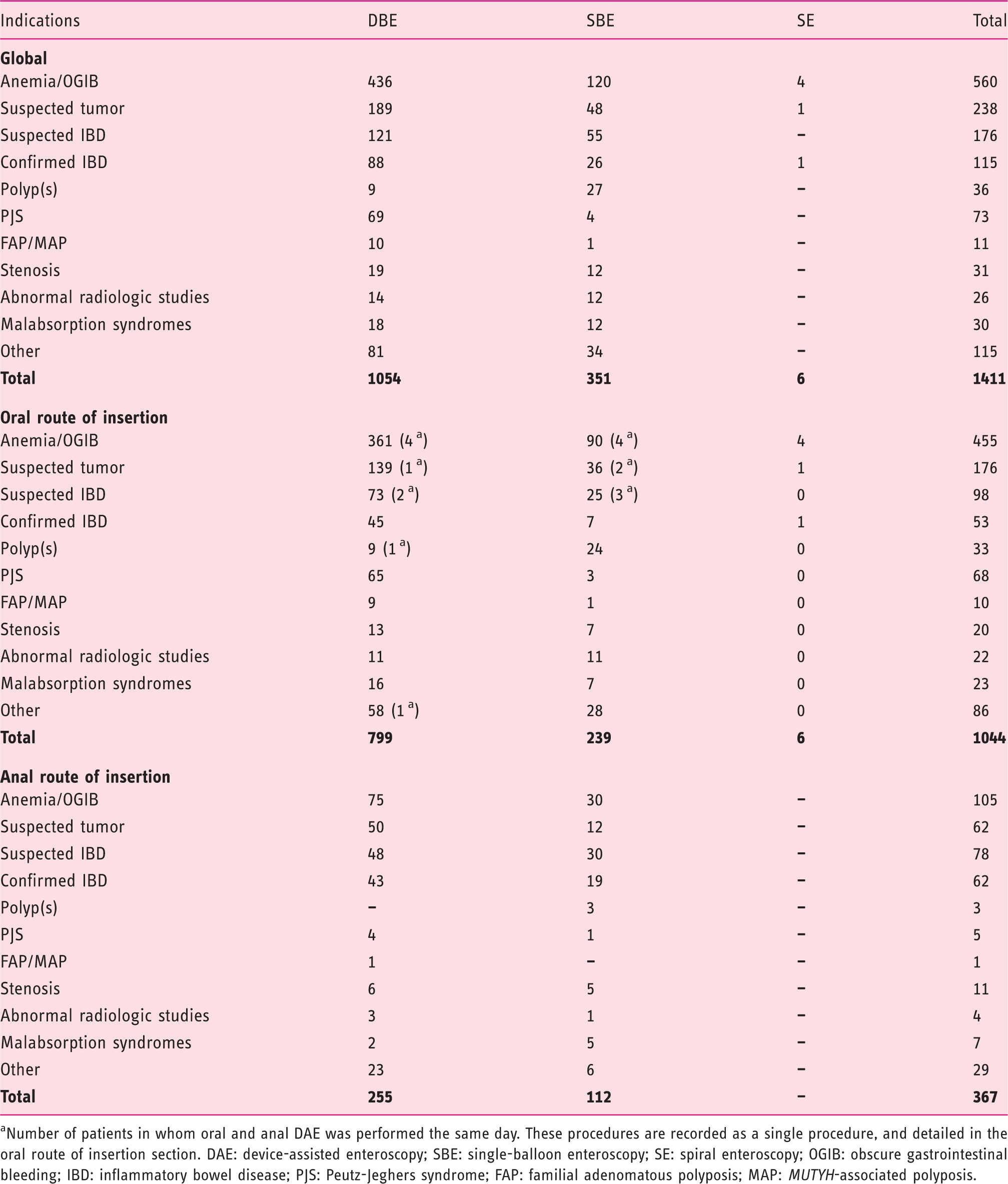
Number of patients in whom oral and anal DAE was performed the same day. These procedures are recorded as a single procedure, and detailed in the oral route of insertion section. DAE: device-assisted enteroscopy; SBE: single-balloon enteroscopy; SE: spiral enteroscopy; OGIB: obscure gastrointestinal bleeding; IBD: inflammatory bowel disease; PJS: Peutz-Jeghers syndrome; FAP: familial adenomatous polyposis; MAP: MUTYH-associated polyposis.
The route of insertion according to the different types of DAE and indications is detailed in Table 3. Predictably, the oral route of insertion was more frequently used with all DAE techniques.
Total enteroscopy was rarely attempted as the goal of most procedures was dictated by the findings of a previous examination, mostly CE (n = 1033, 73.2%). The rate of total enteroscopy could not be determined as the database was not designed to evaluate the limit of insertion in the uncommon procedures in which it was attempted. However, total enteroscopy was reported in 22 procedures (DBE: 19, SBE: two, SE: one).
Main diagnostic finding established in all enteroscopies according to the route of insertion and type of enteroscope used

Number of patients in which oral and anal DAE was performed the same day. These procedures are recorded as a single procedure, and detailed in the oral route of insertion section. DAE: device-assisted enteroscopy; SBE: single-balloon enteroscopy; SE: spiral enteroscopy; NSAIDs: nonsteroidal anti-inflammatory drugs; PJS: Peutz-Jeghers syndrome; FAP: familial adenomatous polyposis; MAP. MUTYH-associated polyposis.
Diagnostic and therapeutic procedures performed during DAE. Only one technique is reported per procedure. In some cases, more than one technique has been used – for instance, in procedures where polypectomy has been performed, injection and tattooing could also have been used
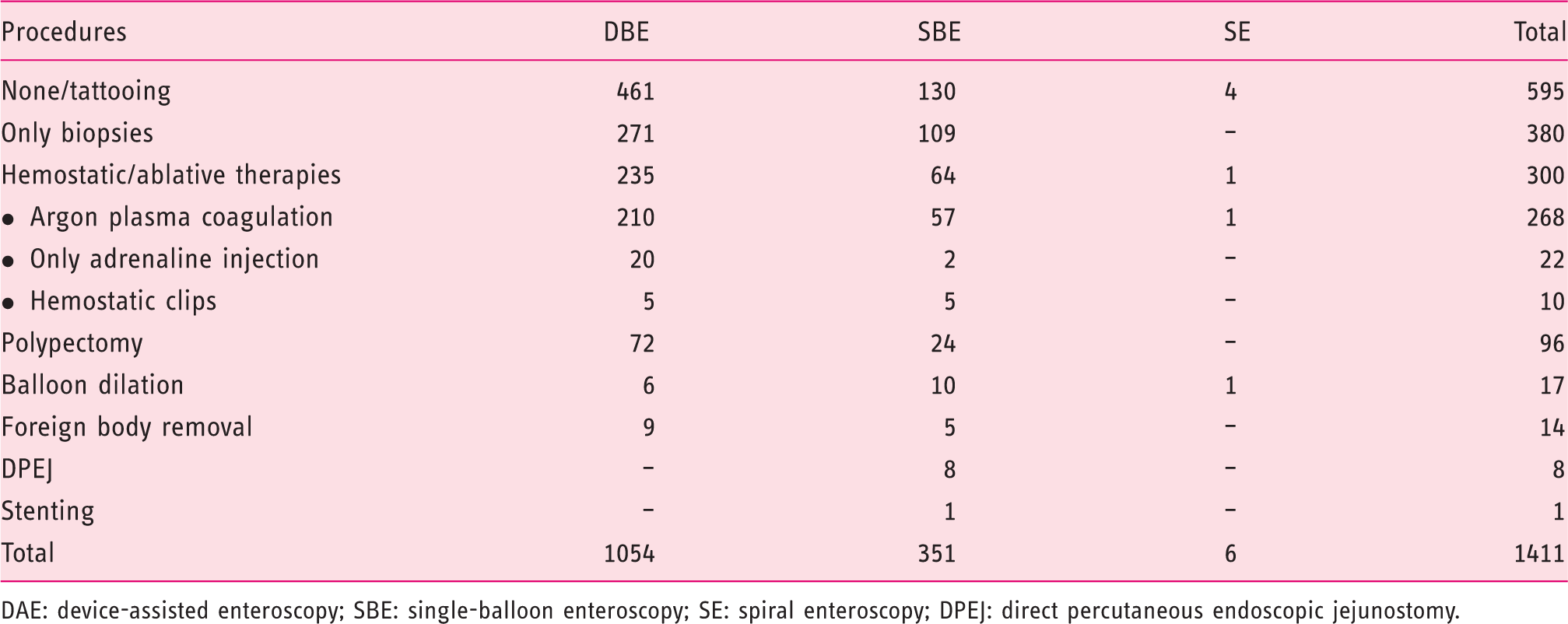
DAE: device-assisted enteroscopy; SBE: single-balloon enteroscopy; SE: spiral enteroscopy; DPEJ: direct percutaneous endoscopic jejunostomy.
Diagnostic and therapeutic yield according to the indication
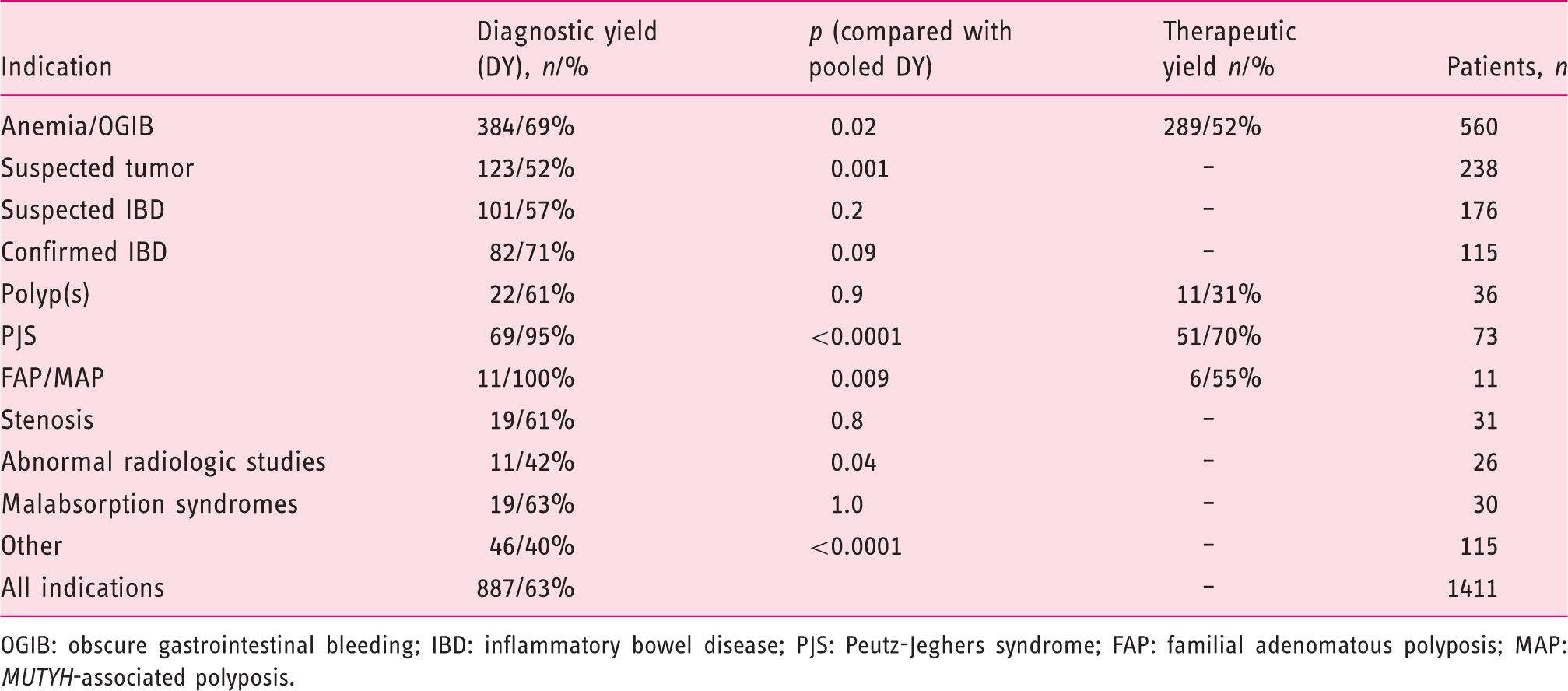
OGIB: obscure gastrointestinal bleeding; IBD: inflammatory bowel disease; PJS: Peutz-Jeghers syndrome; FAP: familial adenomatous polyposis; MAP: MUTYH-associated polyposis.
Complications of device-assisted enteroscopy
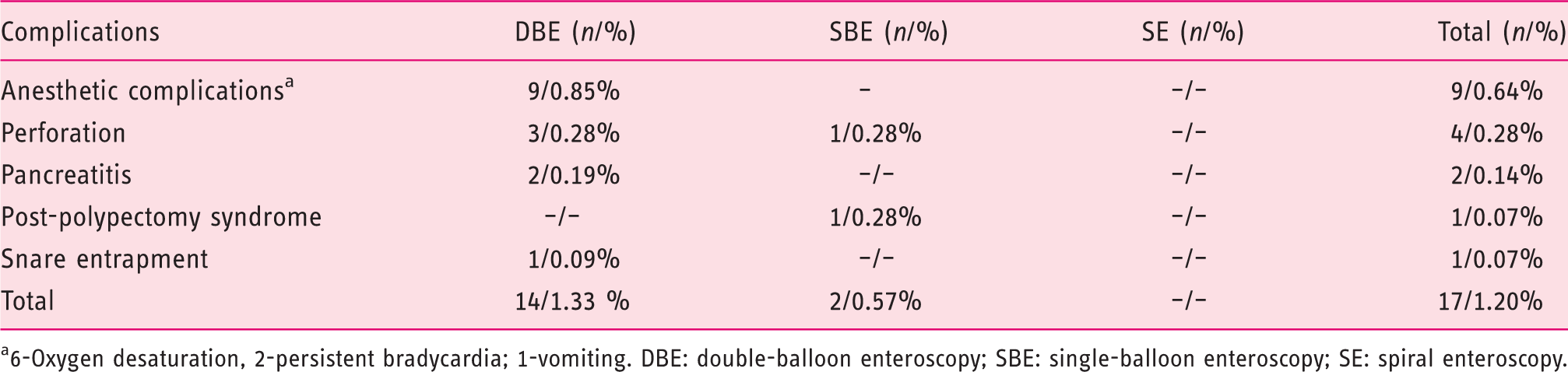
6-Oxygen desaturation, 2-persistent bradycardia; 1-vomiting. DBE: double-balloon enteroscopy; SBE: single-balloon enteroscopy; SE: spiral enteroscopy.
Discussion
This is the first audit ever performed to evaluate the practice of DAE in Portugal. Although the study was extended to all Portuguese centers, a small fraction declined to participate. However, all centers with the most experience and greater casuistic were enrolled, allowing the results to be representative of the national experience.
DAE was introduced early in Portugal, shortly after the description of the procedure. In 2005, two centers were already performing the technique and, a few years later, DAE was introduced in a larger number of centers. The later widespread dissemination consisted mostly of SBE, as in Portugal a greater proportion of endoscopy centers use Olympus equipment, hence limiting acquisition costs to the enteroscope itself. According to the organization of the Portuguese national health system, most enteroscopy centers are public inpatient facilities. In each center, two or three endoscopists are dedicated to performing DAEs. The rate of complete enteroscopy, diagnostic and therapeutic yields and the complication rate of DBE and SBE were compared in two recent meta-analyses.6,7 They were found to be comparable regarding all aspects except the rate of complete enteroscopy, which was found to be slightly higher with DBE. This is, however, of arguable clinical significance as the goal of each examination can usually be reached using both techniques, as expected by their similar diagnostic and therapeutic yields.
The use of DAE in the emergency setting is still uncommon. This may result from organizational difficulties, as the two or three endoscopists experienced in DAEs in each center may not be assigned to emergency procedures at that time; and logistical obstacles, since the procedure is time and resource consuming requiring a long allotment of time and significant staff including an anesthesiologist, for the entire duration of the procedure. Furthermore, in some centers CE is not routinely performed in the emergency setting to guide the use of DAE. This has important clinical implications since the use of CE and DAE 8 early in the presentation of overt OGIB improves both the diagnostic and therapeutic yields.
Only half the centers involved reported the use of DAE for purposes other than small-bowel evaluation and only 25% reported its use for ERCP (DAE-ERCP) in patients with surgically modified anatomy. This may be explained in part by the different areas of expertise of endoscopists performing DAE, as most of them may not be proficient in other techniques such as ERCP. DAE-ERCP enables access to the biliary system and most conventional biliary therapeutics in the great majority of this subset of patients.9–11 Nevertheless, it is very demanding, time consuming, and limited by the availability of specific accessories, 12 which also adds technical and logistic difficulties to its widespread implementation.
Only two centers rated the subjective satisfaction with DAE with a score equal to or below 5 (0–10). In these two centers the technique was introduced in the year previous to the survey, hence these centers had performed a limited number of procedures (13 and 21). The remaining centers rated the satisfaction between 6 and 8, probably reflecting greater experience, although a correlation between the satisfaction score and the total number of procedures was not found.
Significant findings were found in 63% of patients, a diagnostic yield similar to a recent systematic review 13 of 12,823 DBEs in which a pooled diagnostic yield of 68.1% was found. In this review, the most frequent findings were inflammatory lesions (either Crohn’s disease or non-specific inflammatory lesions), vascular lesions and tumoral lesions (either benign or malignant). In our series these were also the most frequent findings, accounting for 84% (745/887) of all positive findings and 52.8% of all diagnoses (745/1411). This high rate of positive findings is derived from the fact that DAE is considered a secondary procedure after an initial positive diagnostic test, as recommended by current European guidelines. 14
Small-bowel polyposis syndromes accounted for 6% (84/1411) of the examinations. Most (86.9%; 73/84) consisted of PJS referred for endoscopic polypectomy of polyps larger than 10 mm detected in surveillance CE. Snare entrapment in a large polyp was reported in one procedure (1.4%), requiring surgical intervention to remove the snare and resect the polyp. No perforations were recorded after polypectomy in contrast to high rates of post-polypectomy perforations previously reported in PJS.15,16 A multicenter series of 46 procedures comprising a survey wherein polypectomy was performed was recently published, 17 in which 214 polyps with a median size of 30 mm were removed. In six of these 46 procedures, surgical intervention was required (jejunal neoplasia: one case, polyps locally concentrated in large numbers: two cases, bulky polyps: two cases with a size up to 60 mm and invaginated polyp: one case). All remaining polyps were managed endoscopically.
DAE is frequently used for therapy of small-bowel lesions detected in other procedures.14,18–20 This is reflected in a high percentage of therapeutic procedures (30.9%). As expected from the main indications and other series,13,15,18,21 hemostatic therapies, namely argon-plasma coagulation, were the most frequently employed endoscopic therapies. Polypectomy, frequently in the setting of PJS, was also commonly performed.
The diagnostic yield was high in all indications, reflecting an appropriate patient selection, since in most cases DAE followed a positive CE as in other series. 18 In patients with OGIB, the most frequent indication for CE and DAE,13,16,22,23 the diagnostic yield was 69%, similar to other series,15,21 and the therapeutic yield was also high at 52%. In patients with polyposis syndromes, the diagnostic yield was near 100% (95% and 100% for PJS and FAP/MAP) and the therapeutic yield was also high (70% for PJS and 55% for FAP/MAP). Although not directly evaluated in the present study, since in Portugal the surveillance of these patients is typically performed with CE these data also point to a good accuracy of CE for screening these patients. Although several reports show that CE24,25 and cross-sectional radiological modalities 26 may miss significant mass lesions, both have a role for small-bowel screening.25,27
The diagnostic yield for suspected small-bowel tumors (52%) was below the pooled diagnostic yield (p = 0.001). Although DAE is regarded as the gold standard for the diagnosis of small-bowel tumors, 28 this lower diagnostic yield reflects a significant portion of false-positive tumors in CE, probably resulting from bulges due to compressions from adjacent organs or bowel loops. 29
Most examinations were performed under anesthesiologist-administered propofol sedation, a common practice in deep sedation for endoscopic procedures in Portugal. 30 Anesthetic complications occurred in 0.6% of DAEs and consisted mainly of oxygen-desaturation and less frequently bradycardia and vomiting. All cases were reversed after the interruption of the procedure. Minor oxygen desaturation not requiring the interruption of the procedure was not regarded as a complication. In a recent study, Lara et al. 31 reported anesthetic adverse events in 15 of 432 procedures (3.5%) performed under deep sedation, mostly oxygen desaturation. Based on this high rate of anesthetic adverse events, the authors currently perform endotracheal intubation for antegrade DAEs. However, this sedation-related complication rate is superior to previous reports.15,32 A recent large multicenter study from Germany, a country where non-anesthesiologist propofol-sedation is common practice, reported 11 (0.5%) sedation-related adverse events in 2245 procedures. 15 No more sedation-related adverse events were found in elderly patients, as previously reported. 33
Complications were reported in 1.2% (17/1411), similar to the multicenter German study 15 in which a complication rate of 1.2% (27/2245) was also found. Major complications were reported in 0.57% (eight of 1411), similar to a recent systematic review where major complications where reported in 0.72% of examinations. 13 Only two cases of acute pancreatitis were recorded. However, this complication is probably underreported, as it occurs frequently several hours after the procedure and most centers perform DAEs for patients from other institutions. Perforation occurred in four patients (0.28%), most of them after therapeutic procedures, as previously reported.15,16
The authors acknowledge some limitations. Although all centers enrolled in the survey maintained prospective data records of all procedures, the databases were not designed for this survey. Consequently some minor variations in data collection, registration and follow-up may have occurred. One participant at each institution compiled the database. Although it was a simple database and the required fields were easy to follow, some inconsistencies in the records may have occurred. However, the database was checked for possible inconsistencies by two authors (RP, MMS). Most centers perform procedures for other institutions and the institution with the highest volume is an outpatient center performing procedures exclusively for other institutions. Hence patient follow-up and recording of delayed complications such as acute pancreatitis may be compromised.
Conclusions
This is the first published survey on the use of DAEs in Portugal. It shows that DAE is widely available in Portugal, mostly in Northern centers, with good performance and training capabilities. Earlier centers adopted DBEs whereas the centers that recently introduced DAE elected SBE. The diagnostic and therapeutic yields are high as most procedures were performed to manage abnormalities detected in other examinations, mostly CE. The complication rate is low, mostly anesthetic complications promptly reversed after the interruption of the procedure. Perforations are rare (0.28%) and occur mainly in therapeutic procedures.
Footnotes
Acknowledgments
Mário Dinis-Ribeiro: ManopH, Instituto CUF; Serviço de Gastrenterologia, Instituto Português de Oncologia do Porto
Fernando Castro-Poças: ManopH, Instituto CUF; Serviço de Gastrenterologia, Centro Hospitalar do Porto
Sandra Lopes: Serviço de Gastrenterologia, Centro Hospitalar e Universitário de Coimbra
Carlos Sofia: Serviço de Gastrenterologia, Centro Hospitalar e Universitário de Coimbra
Ana Rita-Lopes: Serviço de Gastrenterologia, Centro Hospitalar e Universitário de Coimbra
Diogo Branquinho: Serviço de Gastrenterologia, Centro Hospitalar e Universitário de Coimbra
Iolanda Ribeiro: Serviço de Gastrenterologia, Centro Hospitalar de Gaia/Espinho
Ana Ponte: Serviço de Gastrenterologia, Centro Hospitalar de Gaia/Espinho
Joana Silva: Serviço de Gastrenterologia, Centro Hospitalar de Gaia/Espinho
Armando Ribeiro: Serviço de Gastrenterologia, Centro Hospitalar de São João
Filipe Vilas-Boas: Serviço de Gastrenterologia, Centro Hospitalar de São João
João Antunes: Serviço de Gastrenterologia, Centro Hospitalar de São João
Maria João Moreira: Serviço de Gastrenterologia, Centro Hospitalar do Alto Ave
José Soares: Serviço de Gastrenterologia, Hospital Pedro Hispano
Ângela Rodrigues: Serviço de Gastrenterologia, Centro Hospitalar do Porto
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicts of interest
None declared.