
Abstract
Background and aim
The impact of 25-OH vitamin D on sustained viral response (SVR) to antiviral therapy and on fibrosis progression in hepatitis C is debated. We assessed the impact of 25-OH vitamin D concentration on the efficacy of antiviral therapy in naïve genotype 1 hepatitis C virus (HCV)-infected patients.
Methods
The study population consisted of treatment-naïve genotype 1 patients enrolled in a randomised controlled trial. A total of 516 patients received peginterferon α-2a 180 µg/week plus ribavirin 800 mg/day for 24 weeks. There were 349 patients with undetectable HCV RNA (<50 IU/ml) at week 24 (W24) who were randomised to continue dual therapy (n = 173) or to continue peginterferon alone (n = 176) until week 48. 25-OH vitamin D concentration was measured at baseline in frozen serum.
Results
A total of 461 patients could be analysed for virologic response at W24, and 285 (119 non-responders at W24 + 166 responders who continued dual therapy until W48) for the impact of SVR. There were 487 patients who could be analysed for fibrosis progression. Metavir fibrosis scores (centralised analysis) were: F1 30%, F2 34%, F3 27% and F4 9%. Median 25-OH vitamin D concentrations were similar in virologic responders (13.5 ng/ml) and in non-responders at W24 (12.6 ng/ml), as well as in patients with SVR (12.8 ng/ml) and without SVR (12.8 ng/ml, 3.99) at W72. Median 25-OH vitamin D concentrations were: F1: 14.30 ng/ml, F2: 13.50 ng/ml, F3: 13.30 ng/ml and F4: 12.80 ng/ml.
Conclusion
In this study, 25-OH vitamin D level has no impact on the efficacy of antiviral therapy in naïve genotype 1 HCV-infected patients.
Introduction
Hepatitis C virus (HCV) infection is one of the main causes of chronic liver disease worldwide. It can lead to extensive fibrosis, cirrhosis and hepatocellular carcinoma. The number of chronically infected patients worldwide is estimated to be about 160 million. Most of them are unaware of their infection.1,2 The prevalence of hepatitis C is highly variable according to geographic area but it seems higher in developing countries. The prevalence rates are as follow: less than 2.5% in North America and Western Europe, around 3.2% in Africa, 1.5% to 5% in Eastern Europe, 2.5% to 4.9% in the Western Pacific region and 1% to more than 12% in the Middle East and Central Asia. 1
Despite recent major therapeutic breakthroughs,3,4 the standard of care remains the combination of pegylated interferon (IFN) alfa plus ribavirin in the majority of countries. Indeed, for most infected patients the direct-acting agents are inaccessible because of their costs. Thus, finding new ways to improve virologic response, at lower cost, is of high interest.
Vitamin D is a fat-soluble secosteroid with pleiotropic effects. Recent molecular genetic techniques including genomics revealed that 25-hydroxy (25-OH) vitamin D controls more than just calcium homeostasis. It has widespread effects on cellular differentiation and proliferation, and plays a role in the immune system. 5 A role for 1,25-OH-vitamin D3 as a mediator of normal function of both the innate and adaptive immune systems has been established. 6 25-OH vitamin D deficiency is very common in chronic hepatitis C.7–9 Recent reports provided conflicting results on the impact on the efficacy of antiviral hepatitis C therapy10–15 and on fibrosis progression.10,16,17
The aim of this study was to assess the impact of 25-OH vitamin D concentration on the virologic response and on fibrosis progression in a post-hoc analysis of a randomised, controlled trial.
Materials and methods
The study population were genotype 1, naïve, mono-infected patients enrolled in a study assessing the effect of ribavirin in genotype 1 patients with chronic hepatitis C initially responding to pegylated IFN alfa 2a plus ribavirin. 18 All patients received pegylated IFN alfa-2a (Pegasys; Roche, Basel, Switzerland), 180 µg once weekly subcutaneously, plus ribavirin (Copegus; Roche) 400 mg twice daily orally, for 24 weeks. At week 24 (W24), HCV RNA was analysed by means of a qualitative polymerase chain reaction (PCR) assay (Cobas Amplicor HCV v2.0; Roche Molecular Systems) with a lower limit of detection of 50 IU/ml. The patients were seen at W26 with the result of their HCV RNA detection. Patients with undetectable HCV RNA at W24 were randomised at W26 to a further 22 weeks of treatment (i.e. until W48) with either pegylated IFN alfa-2a 180 µg once weekly without ribavirin, or continuation of pegylated IFN alfa-2a 180 µg once weekly in combination with ribavirin 400 mg twice daily. The remaining patients who had detectable HCV RNA at W24 stopped therapy because they had a low chance of achieving a sustained viral response (SVR) with continued treatment.
All patients had a liver biopsy finding consistent with chronic hepatitis C obtained within 18 months before therapy (Metavir scores of at least A1 and F1, as assessed by a single pathologist).
25-OH vitamin D concentration was measured at baseline in serum, frozen at −80℃ with a chemiluminescent immunoassay which quantified 25-OH vitamin D and other hydroxylated vitamin D metabolites. The assay was used according to the manufacturer’s recommendation (LIAISON® 25 OH Vitamin D TOTAL Assay DiaSorin, Antony, France). Concentrations < 4 ng/ml were given as 3.99 ng/ml. Patients lacking a 25-OH vitamin D serum concentration before initiation of the treatment were excluded from the correlation analysis.
Correlation between the baseline 25-OH vitamin D concentration and virologic response at W24 and the fibrosis score respectively were analysed in the whole population whereas the correlation with SVR was assessed only in the non-responders at W24 and the responders at W24 randomised in the dual-therapy continuation arm.
The protocol was approved by the local ethics committee (Comité Consultatif de Protection des Personnes dans la Recherche Biomédicale) of the University Hospital of Nancy on 24 October 2000. All patients provided written informed consent. The study was conducted according to the guidelines of the Declaration of Helsinki, under provisions of Good Clinical Practices, or both. Data were collected by the study group and analysed by the authors with the help of the sponsor. The authors had unlimited access to the data and no limitation on publication was imposed by any party.
Statistical analyses
Continuous variables were described as medians, means, interquartiles and range, and categorical variables were reported as frequency and percentages. Differences between groups were assessed using the Kruskal-Wallis test or the Wilcoxon test for non-normally distributed variables. Differences between groups were assessed using the Chi 2 test or Fisher’s exact test for categorical data. Receiver operating characteristic (ROC) curves were applied to find the best cut-off values of 25-OH vitamin D in order to distinguish virologic responders from non-responders.
A p value < 0.05 was considered statistically significant. All calculations were performed using SAS V9.1.3 software (SAS Institute Inc, Cary, NC, USA).
Results
Baseline characteristics of patients and 25-OH vitamin D concentration
Patient characteristics at baseline
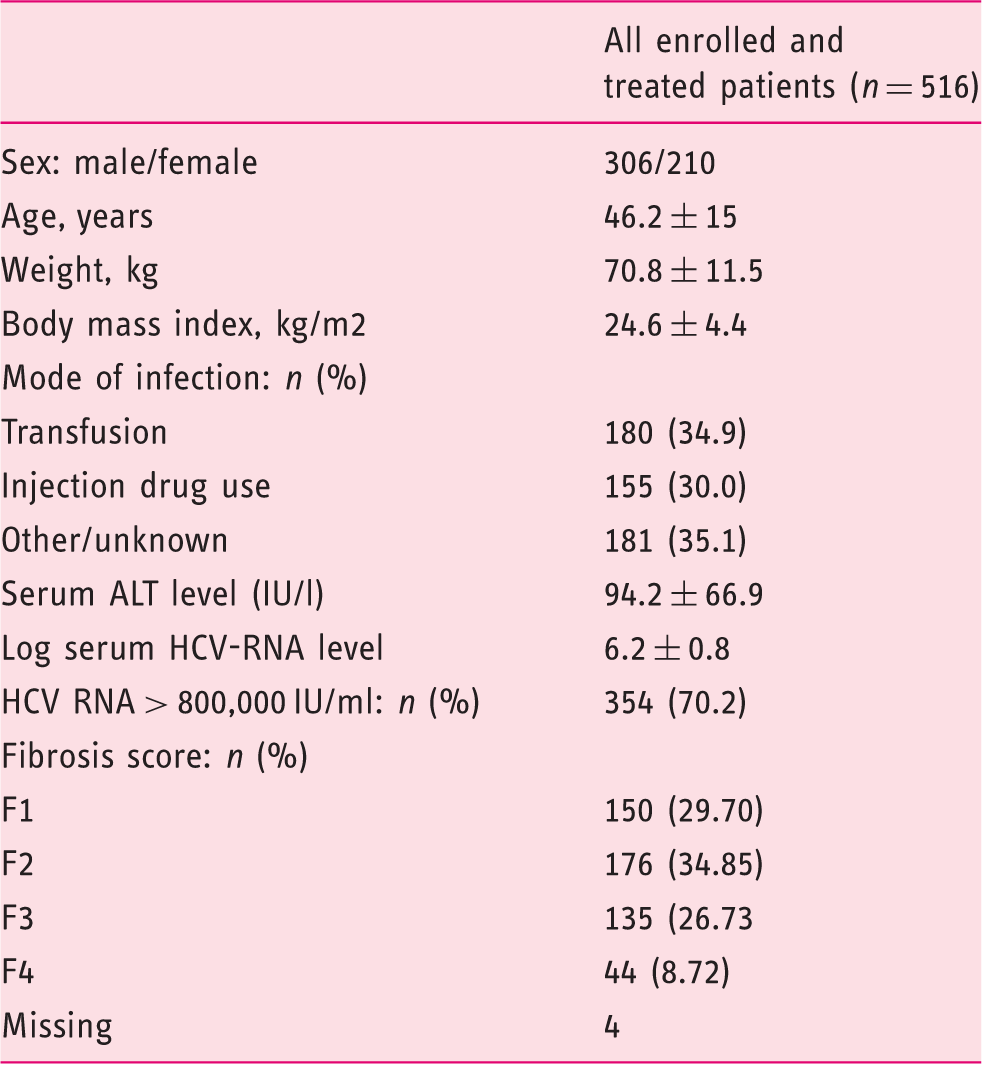
ALT: alanine aminotransferase; HCV: hepatitis C virus.
Baseline 25-OH vitamin D concentration and the virologic response at W24 and with SVR
Among the 489 patients with available baseline 25-OH vitamin D concentration, the virologic response at W24 was missing in 28 patients. Thus, 461 patients were eligible for the correlation study with the virologic response at W24. A total of 342 of the 461 patients (74%) were HCV RNA negative at W24 of combination therapy. They were randomised into two arms, one continuing combination therapy (n = 173), the second arm treated with peginterferon only (n = 169). Patients included in the second arm were excluded from the correlation analysis with SVR. Among the 173 patients continuing combination therapy for a total of 48 weeks, 118 achieved an SVR, and 55 patients failed to achieve SVR. 25-OH vitamin D was missing in three of the 118 patients achieving SVR and in four of the 55 patients failing to achieve SVR. The patients’ disposition is summarised in Figure 1.
Flowchart.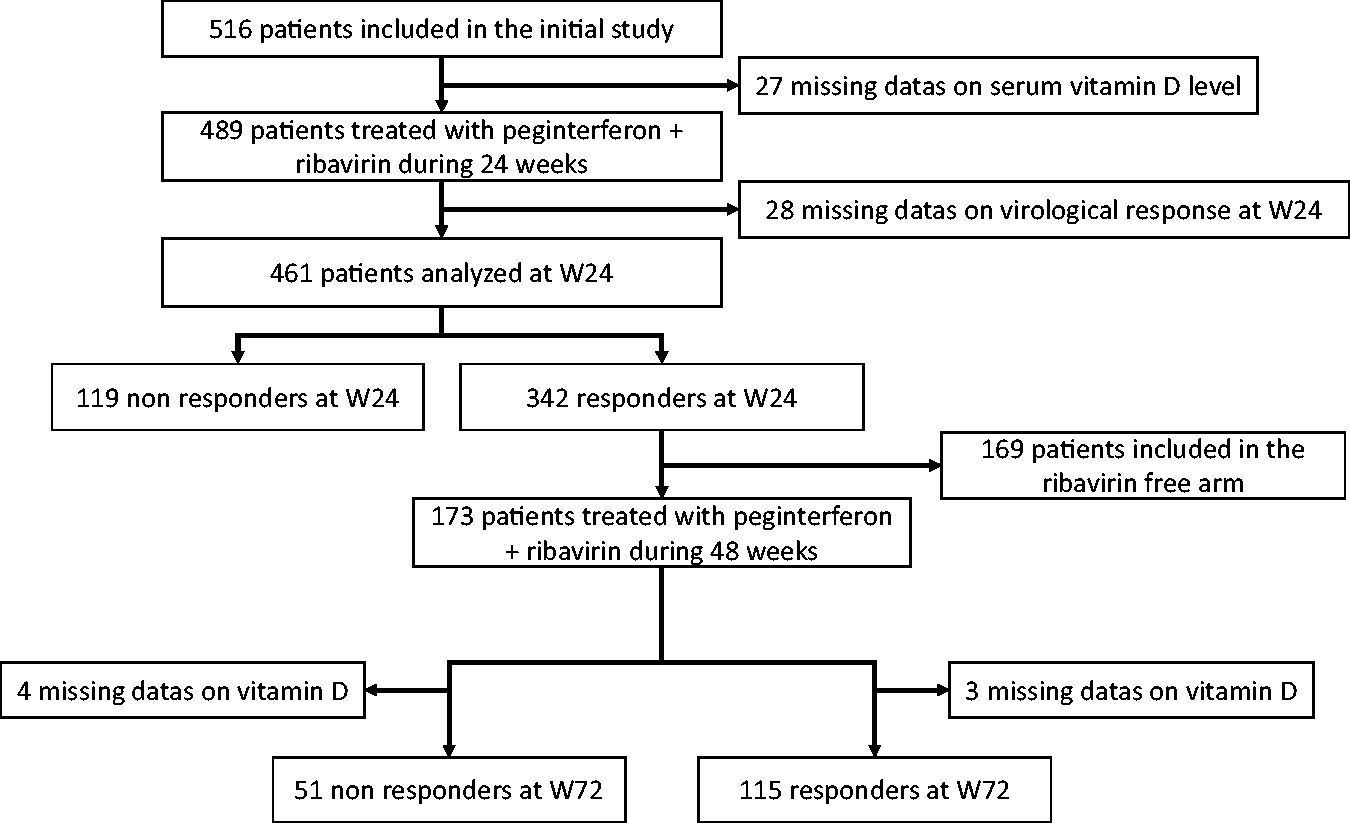
Baseline 25-OH vitamin D level and virologic response at W24

25-OH: 25-hydroxy; W24: week 24.
Virologic response at W24 according to the quartiles of 25-OH vitamin D concentration
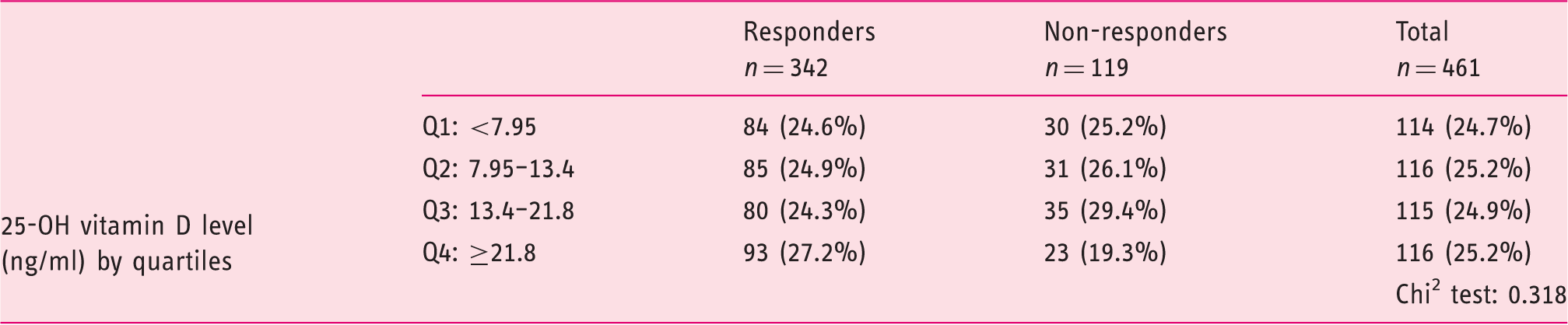
W24: week 24; 25-OH: 25-hydroxy.
Subgroup analysis according to geographic origin (North vs South of France) did not reveal an influence of 25-OH vitamin D concentration on SVR in either of the two regions.
Baseline 25-OH vitamin D concentration and fibrosis score
Baseline 25-OH vitamin D level and fibrosis score

25-OH: 25-hydroxy.
Discussion
Our study is the largest study performed in genotype 1 naïve patients assessing the impact on 25-OH vitamin D of virologic response and fibrosis progression. In our study, 25-OH vitamin D level before antiviral treatment has no impact on the efficacy of antiviral therapy in naïve genotype 1 HCV-infected patients. Moreover, no significant association was found with the fibrosis progression.
25-OH-vitamin D has pleiotropic effects. 5 It is an innate antiviral agent and has anti-fibrotic effects.16,19,20 Several studies assessed the relationship between vitamin D concentration and achievement of SVR in patients with genotype 1 chronic hepatitis C. A total of 274 naïve genotype 1 patients, from the Cognitive Health in Ageing Register: Investigational, Observational, and Trial Studies in Dementia Research (CHARIOT) cohort study, were included in the Kitson et al. study. 15 Baseline 25-OH vitamin D level was not independently associated with achievement of SVR. 15 Moreover, 25-OH-vitamin D level did not show any significant association with treatment outcome among 391 genotype 1 patients followed prospectively. 21 On the other hand, six studies found a correlation between vitamin D level and achievement of SVR.8–11,13,22,23 The largest is a retrospective study including 468 patients living in Germany, infected with all genotypes. 8 Reduced 25-OH-vitamin D levels were associated with failure to achieve SVR in HCV genotype 1-, 2- and 3-infected patients. 8 In 117 naïve genotype 1 chronic hepatitis C patients followed prospectively, 25-OH vitamin D levels were independently associated with the likelihood to achieve SVR. 22 In recurrent hepatitis C, after liver transplantation, 25-OH vitamin D deficiency predicted an unfavourable response to antiviral treatment. 11 A meta-analysis by García-Alvarez et al. retrieved 14 studies evaluating relationship of vitamin D status with advanced liver fibrosis in chronic hepatitis C treatment-naïve patients and sustained virologic response in patients under pegylated IFN alfa plus ribavirin therapy. 24 They retrieved 11 studies that evaluated relationship with SVR, representing a total of 2672 patients. They noted a significant heterogeneity among studies, and only found a significant association with SVR for a vitamin D cut-off of 20 ng/ml (odds ratio (OR) = 0.53 (95% confidence interval (CI) = 0.31–0.91). 24 After excluding the outliers, they found significant pooled ORs, for all patients and for genotype 1 and 4 patients, for vitamin D cut-off of 10 ng/ml and 20 ng/ml. More recently another meta-analysis concluded that baseline 25-OH vitamin D level was not associated with SVR to pegylated-IFN plus ribavirin therapy in chronic HCV infection, regardless of genotype. 25
Our study did not find a correlation between 25-OH vitamin D level and fibrosis stage. Results previously published are contradictory.10,15,26–29 In the CHARIOT study, 25-OH vitamin D level was not independently associated with fibrosis stage, in 274 naïve genotype 1 patients, but a correlation was found with the histological activity. 15 On the other hand, lower 25-OH vitamin D levels were independently associated with the severity of liver fibrosis in 197 Italian naïve genotype 1 patients. 10 It is worthy to note that genetic variants involved in cholesterol synthesis, vitamin D hydroxylation and vitamin D transport were also associated with the severity of fibrosis. 26 Three more studies assessed a correlation between 25-OH vitamin D status and fibrosis in chronic hepatitis C patients10,28,29 and one study in HCV/human immunodeficiency virus (HIV) co-infected patients. 27 In the García-Alvarez et al. meta-analysis, seven studies were selected which evaluated the relationship of vitamin D status with advanced liver fibrosis in chronic hepatitis C treatment-naïve patients. Low vitamin D status was related to a diagnosis of advanced liver fibrosis, with the cut-offs of 10 ng/ml (OR = 2.37 (95% CI = 1.20–4.72)) and 30 ng/ml (OR = 2.22 (95% CI = 1.24–3.97)) being significant. 24
Concerning the impact of vitamin D supplementation on virologic response, data are scarce. Three studies evaluated the impact of vitamin D supplementation on the virologic response in chronic hepatitis C.11,23,30 The early virologic response was better in a subgroup of patients receiving 1-OH vitamin D3 and having an interleukin (IL)-28B T/T genotype. The study compared 42 patients treated with a combination of peginterferon alfa, ribavirin, and 1-OH vitamin D3 to 42 matched controls treated with peginterferon alfa and ribavirin only. 30 In another study, vitamin D supplementation improved the probability of achieving an SVR in patients with recurrent hepatitis C, and in the presence of a normal or near normal baseline vitamin D concentration. 11 The last study focused on genotype 1 treatment-naïve patients. Adding vitamin D3 to conventional peginterferon alfa 2b/ribavirin therapy significantly improved the virologic response in a population of 72 consecutive patients. 23 In this study 86% of the patients undergoing vitamin D supplementation achieved an SVR, vs 42% of control patients (p < 0.001), which means that vitamin D supplementation could be as effective as the addition of a protease inhibitor to dual therapy.31–34 Another study concluded that vitamin D supplementation has no significant impact on SVR in HCV genotype 4 patients. 35
The mean 25-OH vitamin D concentration in our population was very low (13.4 ng/ml) compared to other studies.10,15 Indeed, mean vitamin D level was 31.6 ng/ml in the Kitson et al study. 15 This may be due to differences in the measurement technique used. The technique used in our study is reliable and is recommended by the French authorities. 36 The proportion of HCV-positive patients with severe deficiency is high in all the published studies regardless of geographic origin. It is not clear if chronic hepatitis C exposes patients to vitamin D deficiency compared to the general population. However, in the Lange et al. study, including 468 patients infected with all genotypes, baseline 25-OH-vitamin D levels were lower in the chronic hepatitis C group compared to a control group. 8
Moreover, there is a higher prevalence of osteoporosis and osteopenia in patients with chronic hepatitis C. Among 43 non-cirrhotic patients, 30 infected with HCV and 13 with hepatitis B virus, there was a significantly reduced bone mineral density. 37 Viral clearance could reduce that risk. In 420 post-menopausal women infected with HCV and treated with IFN monotherapy, virus clearance caused a reduction by two-thirds in the risk of bone fracture after cessation of IFN therapy. 38 Cirrhotic patients secondary to hepatitis C infection have an early increase of bone resorption, leading to osteoporosis. 39 The severity of metabolic osteopathy is related to the alteration in liver function. 39 Treatment of chronic hepatitis C, especially ribavirin, has been reported as inducing bone loss.40,41 In 32 male patients with chronic hepatitis C treated for 12 months with either IFN alone or IFN plus ribavirin, bone mineral density was significantly lower in the dual-therapy group. 40 In vitro, ribavirin, but not IFN alfa-2b, has been associated with impaired osteoblast proliferation and differentiation. 41 But other conflicting results have been reported.41,42 Antiviral therapy with IFN-alfa and ribavirin led to an on-treatment increase of bone mineral density in 30 patients with genotype 1 infection without cirrhosis. 43
Our study strengths are that it is the largest to evaluate a correlation between serum 25-OH vitamin D level and virologic response in naïve genotype 1 patients and that the liver histology was reassessed by a single pathologist. But it also suffers some limits. It is a retrospective study and we were not able to assess the impact of 25-OH vitamin D concentration according to predictors of SVR like insulin resistance 44 and IL-28B polymorphism. 45
In conclusion, in our study, 25-OH vitamin D level before antiviral therapy has no impact on the efficacy of antiviral therapy in naïve genotype 1 HCV-infected patients. Moreover, no significant association could be found with fibrosis progression.
Footnotes
Acknowledgements
Author contributions include: AB and EG, draft of the manuscript; MBA, data collection and critical review of the article; SR, statistical analysis; LPB; drafting of the article and critical review of the article; JMP, GC and AL critical review of the article; and JPB, study design and supervision.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
None declared.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.