
Abstract
Background
The ability to predict the severity of disease is important to reduce morbidity and mortality in patients with acute pancreatitis (AP). Vitamin D deficiency has been associated with severity in various diseases.
Objective
This study was conducted to assess vitamin D as a predictor of disease severity in patients with AP.
Methods
Patients with AP were prospectively enrolled at Yonsei University Wonju College of Medicine from March 2015 to September 2017. Serum vitamin D was analyzed as soon as AP was diagnosed. The level of vitamin D was classified as normal (>20 ng/ml), insufficient (>10 and ≤20 ng/ml) or deficient (≤10 ng/ml).
Results
Among 242 patients with AP, the prevalence of vitamin D deficiency was 56.2%, and 28.5% of patients had vitamin D insufficiency. Serum vitamin D level was negatively correlated with severity indexes, such as the Atlanta classification, Computed Tomography Severity Index, Bedside Index for Severity of Acute Pancreatitis, and Ranson score. The prevalence of vitamin D deficiency increased with severity of AP according to the Atlanta classification. Vitamin D deficiency was the independent factor for predicting severe AP (OR 5.37, 95% CI 1.13–25.57, p = 0.015) and intensive care unit admission (OR 3.09, 95% CI 1.24–7.69, p = 0.035).
Conclusion
Vitamin D deficiency is associated with increased severity of AP and is a predictor for intensive care unit admission.
Key summary
There is no study investigating the relationship between vitamin D deficiency and severity of acute pancreatitis (AP). This is the first study to reveal an independent association between vitamin D status and severity of AP. This study showed lower blood vitamin D is a risk factor for intensive care unit admission and severity of disease in patients with AP.
Introduction
Acute pancreatitis (AP) is an inflammatory process that causes local and systemic inflammatory response syndrome. The incidence of AP is increasing worldwide, and the disease is associated with high morbidity and mortality.1,2 Most patients with AP experience a mild disease course, but 20% of patients develop moderately severe or severe AP (SAP).1,3 The mortality due to AP is approximately 13% in patients with sterile necrosis and 15% to 35% in patients with infected necrosis. 3 Therefore, early recognition of the severity of AP is very important to optimize intensive therapy and improve outcomes. 4
Several scoring systems such as Ranson score, Acute Physiology and Chronic Health Examination II (APACHE II) score, computed tomography severity index (CTSI), and Bedside Index for Severity in Acute pancreatitis (BISAP) have been developed to identify the severity of AP.5–8 The Atlanta classification was revised in 2012 (Atlanta 2012). 9 In addition, individual underlying comorbidities such as metabolic syndrome and diabetes mellitus were related to the severity of disease.10,11 Recent studies have shown that inflammatory markers such as apolipoprotein B/A-I ratio, neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio were related to AP severity.12,13
Vitamin D3 (cholecalciferol) is a secosteroid hormone that affects bone metabolism and also has immunologic properties. Vitamin D insufficiency is common worldwide, and the prevalence of vitamin D insufficiency has been reported to be 47.3% in males and 64.5% in females in Korea.14,15 The presence of vitamin D receptors in other tissues and organs suggests that vitamin D physiology extends well beyond bone homeostasis. 16 Vitamin D seems to play a role in chronic inflammatory disease, including cardiovascular diseases, diabetes mellitus, cancer, infections and autoimmune diseases. 17 A few studies have reported the possible role of vitamin D deficiency in chronic and acute pancreatitis. 18 However, there has been no study investigating the relationship between vitamin D deficiency and severity of AP.
In this study, we aimed to determine the prevalence of vitamin D deficiency in patients admitted to a tertiary care center with AP and to assess the severity of AP according to vitamin D level.
Materials and methods
Patients
This was a prospective study of patients with AP in Yonsei University Wonju College of Medicine from March 2015 to September 2017. AP was diagnosed based on the presence of two of the following three features: 9 (1) typical abdominal pain, (2) serum amylase and/or lipase ≥ 3 times the upper normal limit and (3) radiologic findings. Peripheral blood samples were obtained on admission. Hemoglobin, hematocrit, white blood cell count, calcium, phosphorus, blood urea nitrogen, creatinine, lactate dehydrogenase, aspartate aminotransferase, C-reactive protein (CRP) and arterial blood gas analysis were measured at the time of admission. Hypertension and diabetes mellitus were checked by medical examination and body mass index (BMI) was calculated. Abdominal computed tomography (CT) scan was performed in all patients upon admission to differentiate AP from other diseases. Once AP was diagnosed, scoring systems, such as the Ranson score, CTSI and BISAP, were applied. Vitamin D level was measured within 24 hours of admission as serum 25-hydroxyvitamin D3 (25-(OH)D3) using a radioimmunoassay kit (DiaSorin, Stillwater, MN, USA). Vitamin D deficiency was defined as a 25-(OH)D3 level less than 10 ng/ml. A 25-(OH)D3 level of 10 to 19 ng/ml was defined as vitamin D insufficiency, and a level ≥20 ng/ml was considered to indicate a sufficient level of vitamin D. 19 The severity of AP was assessed according to the Atlanta 2012 criteria and classified as mild, moderately severe or severe. 9 Mild AP is defined by the absence of organ failure (OF) and local or systemic complications. Moderately severe AP is described as transient OF that resolves within 48 hours and is accompanied by local or systemic complications. SAP is described as persistent OF. Endoscopic retrograde cholangiopancreatography was performed when gallstone pancreatitis was diagnosed. The study protocol was approved by the international review board for human research (CR315005-002) of Yonsei University Wonju College of Medicine on June 18, 2015. Formal consent was obtained from all patients.
Statistical analysis
Categorical variables were presented as the frequency and percentage. Continuous variables were presented as the mean ( ± SD) or median with range. One-way analysis of variance (ANOVA) or chi-squared test was used to compare the scoring systems and number of intensive care unit (ICU) admissions according to serum vitamin D level. The Pearson rank method was used to evaluate the correlation between serum vitamin D level and scoring system. We calculated the odds ratios (ORs) and confidence intervals (CIs) for having SAP and ICU admission using a multivariable logistic regression analysis after adjustment for confounding variables. A p < 0.05 was considered statistically significant. All statistical analysis was performed using SPSS version 21.0 for Windows (SPSS Inc, Chicago, IL, USA).
Results
Study population
Baseline characteristics of all patients.
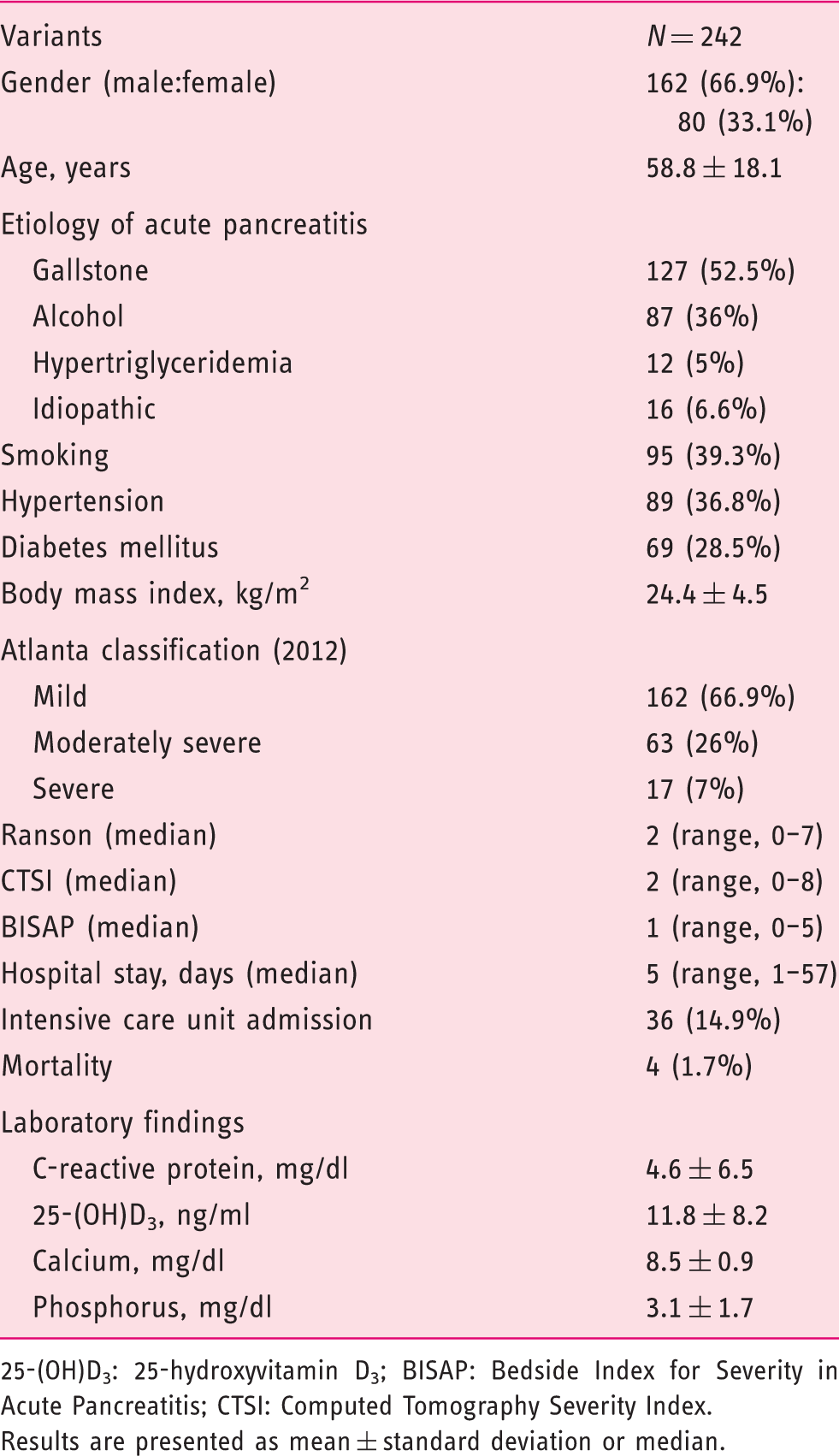
25-(OH)D3: 25-hydroxyvitamin D3; BISAP: Bedside Index for Severity in Acute Pancreatitis; CTSI: Computed Tomography Severity Index.
Results are presented as mean ± standard deviation or median.
Vitamin D level and severity of pancreatitis
Scoring systems and severity of acute pancreatitis according to vitamin D level.
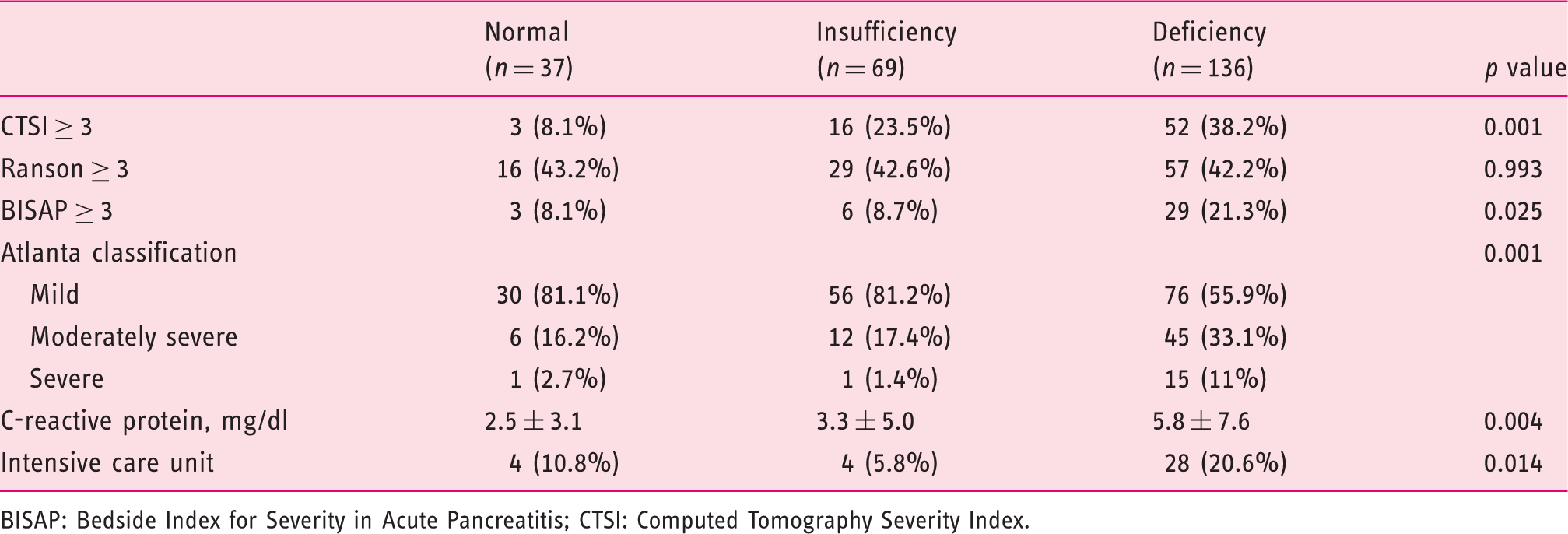
BISAP: Bedside Index for Severity in Acute Pancreatitis; CTSI: Computed Tomography Severity Index.
Correlation between serum vitamin D and scoring systems.
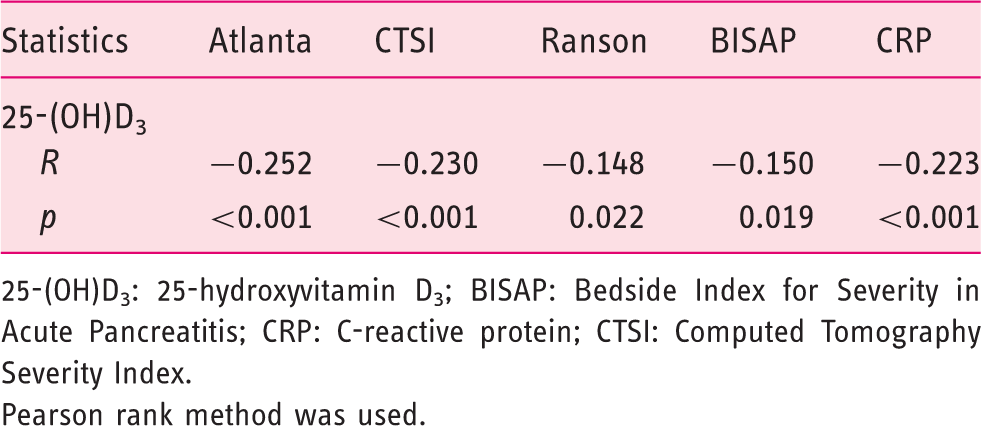
25-(OH)D3: 25-hydroxyvitamin D3; BISAP: Bedside Index for Severity in Acute Pancreatitis; CRP: C-reactive protein; CTSI: Computed Tomography Severity Index.
Pearson rank method was used.
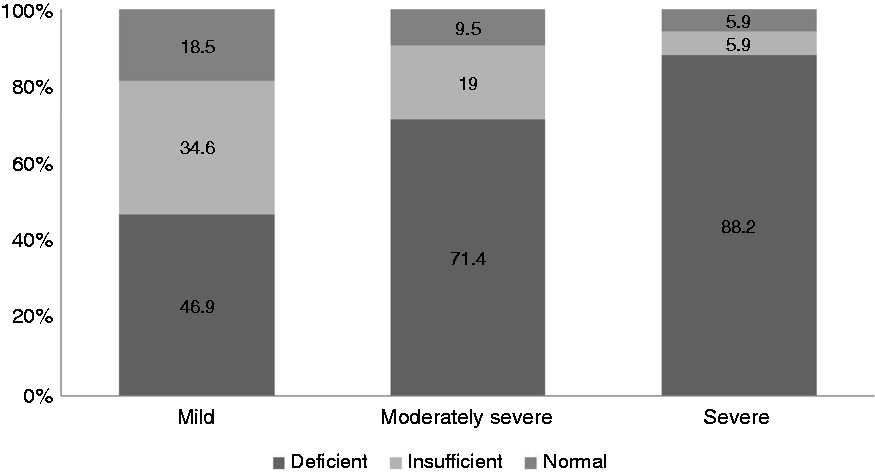
The prevalence of vitamin D deficiency in acute pancreatitis according to the Atlanta classification.
Predictive factors affecting ICU admission and SAP
Association between vitamin D deficiency and intensive care unit admission.
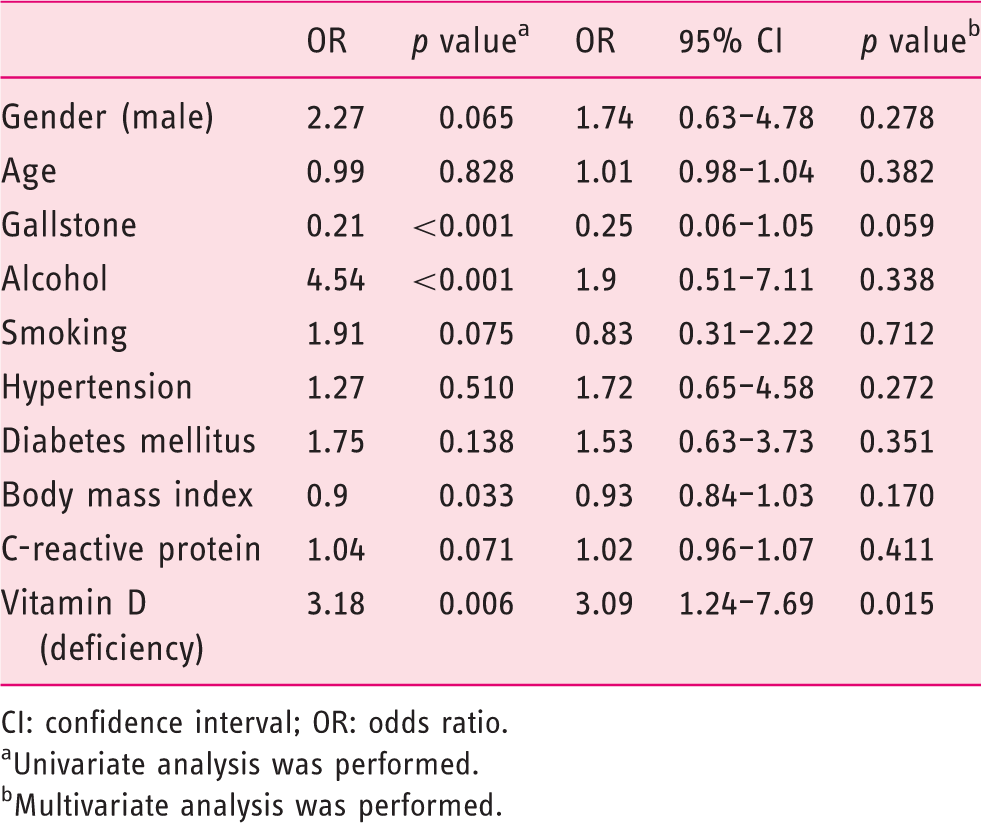
CI: confidence interval; OR: odds ratio.
Univariate analysis was performed.
Multivariate analysis was performed.
Association between vitamin D deficiency and severe acute pancreatitis.
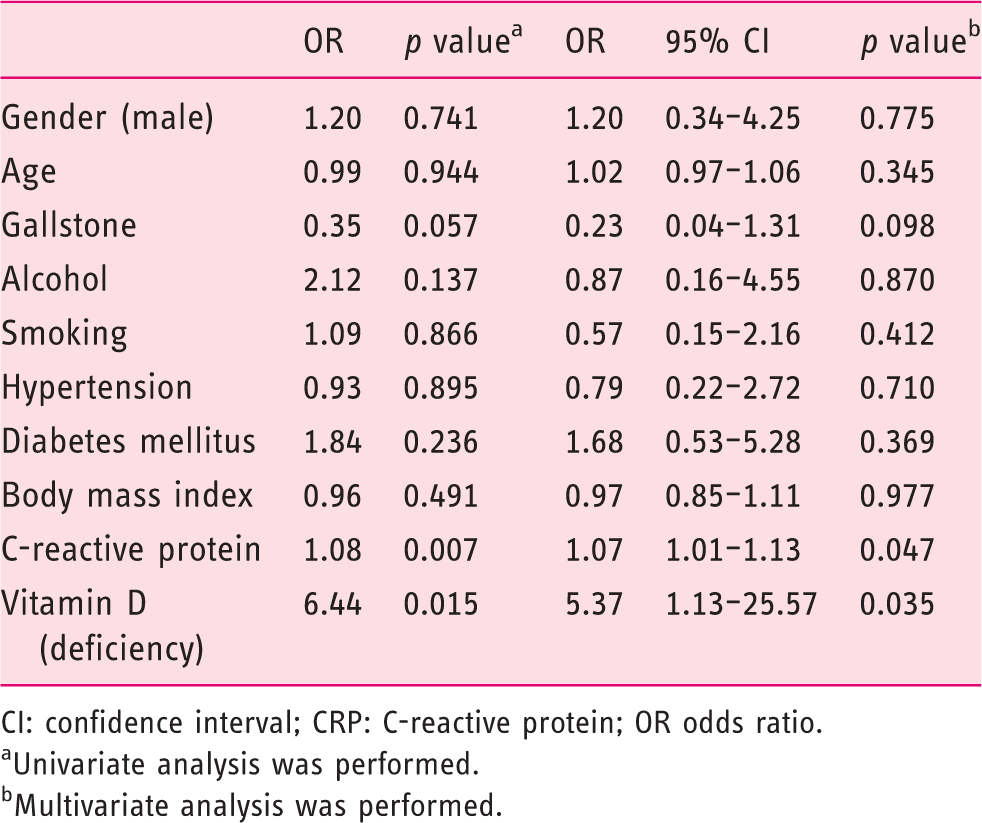
CI: confidence interval; CRP: C-reactive protein; OR odds ratio.
Univariate analysis was performed.
Multivariate analysis was performed.
Discussion
In this study, we evaluated the correlation between 25-(OH)D3 level and AP severity. Serum 25-(OH)D3 level was inversely related with the severity of AP as well as inflammatory markers (e.g. CRP). Moreover, we found that lower serum 25-(OH)D3 level is a predictor for ICU admission and SAP independent of traditional risk factors for SAP. To our knowledge, this is the first study to reveal an independent association between vitamin D status and severity of AP.
AP involves an initial inflammatory reaction within the pancreas. Subsequently, inflammatory cytokines induce hepatic synthesis of acute-phase proteins and mediate distant OF in the setting of SAP. Considering the known relationship between 25-(OH)D3 and acute inflammation, 20 several recent studies have demonstrated that serum vitamin D levels were low in acute pancreatitis. Parrish et al. showed that up to 74.4% of their patients had blood 25-(OH)D3 level less than 20 ng/ml, and approximately 34% of their patients had severe vitamin D deficiency with blood 25-(OH)D3 levels less than 10 ng/ml. 21 Similarly, Bang et al. found that up to 40% of patients with AP had severe vitamin D deficiency at the time of admission. 18 However, these previous studies did not investigate the association between vitamin D deficiency and prognosis of AP. Although the independent role of vitamin D in the immunologic and inflammatory processes is well known, there have been few studies to investigate the association between vitamin D deficiency and prognosis of AP.
In the current study, we observed that vitamin D deficiency is closely associated with ICU admission and SAP. This association was independent of other traditional factors for SAP. This finding suggests that serum 25-(OH)D3 level at admission may be a useful marker for predicting the severity of AP. Possible mechanisms underlying the association between lower 25-(OH)D3 level and SAP may be explained as follows. Activated macrophages in the inflamed pancreas may convert 25-(OH)D3 to 1,25-(OH)2D3 through a 25-hydroxyvitamin D-1α-hydroxylase (CYP27B1)-catalyzed reaction. Subsequently, 1,25-(OH)2D3 stimulates the activation of the nuclear vitamin D receptor, resulting in the expression of CYP24A1. Hummel et al. showed that the expressions of vitamin D receptor and CYP24A1 increased in diseased pancreatic tissue. 22 CYP24A1 causes the degradation of 25-(OH)D3 and 1,25-(OH)2D3 in the inflamed pancreas to inhibit an increase in the blood level of 1,25-(OH)2D3 to prevent the development of hypercalcemia, which would exacerbate the inflammatory condition. 23 Bang et al. found that the blood level of 25-(OH)D3 significantly and progressively decreased in a linear fashion from day 0 to day 2 in patients with AP. This decrease was associated with increasing CRP concentration in the blood. 18 Similarly, our study also demonstrated that CRP was negatively associated with serum 25-(OH)D3 level, indicating that the AP inflammatory condition is intimately associated with a significant reduction in the serum 25-(OH)D3 level. Therefore, it is reasonable to consider both 25-(OH)D3 and 1,25-(OH)2D3 as negative acute-phase reactants, specifically in the context of AP of various etiologies. In addition, a decrease of ionized calcium in patients with SAP increases the secretion of parathyroid hormone, which increases the nephrogenic metabolism of 25-(OH)D3 24 .
The current study has several limitations, the first of which is the study design. Although this study had a prospective design, there is a possibility of selection bias. All study participants were identified from one hospital, and most patients were older adults. Therefore, the individuals included in our study may have been more likely to be vitamin D deficient. In addition, the more severe patients were transferred to our university hospital, and patients with a higher risk for SAP were included in our study group. Another limitation was that serum 25-(OH)D3 levels were measured only one time during various seasons. Furthermore, we did not collect data on sunlight exposure and types of food intake, which can affect serum 25-(OH)D3 levels. Third, given the cross-sectional study design, a causal relationship of vitamin D in AP could not be disclosed. Lastly, the long-term outcomes of AP were not evaluated according to the serum 25-(OH)D3 levels. Nevertheless, the results of our study have useful clinical implications in suggesting that, in addition to other known predictive factors such as CRP, diabetes and BMI, vitamin D deficiency might be considered as an independent risk factor for predicting the outcome of SAP. In addition, vitamin D is a convenient and simple biomarker for predicting SAP. Furthermore, this is the first study to extensively investigate the potential impact of vitamin D on the clinical outcomes of AP.
In conclusion, we demonstrated that lower blood vitamin D is a risk factor for ICU admission and severity of disease in patients with AP. This finding suggests that vitamin D status in individuals might be helpful to predict the prognosis of AP. Further prospective cohort or randomized trials are warranted to confirm our findings and to gain in-depth insight into the role of vitamin D in AP prognosis.
Footnotes
Declaration of conflicting interests
None declared.
Funding
This work was supported by a National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIP) (No. NRF-2016R1C1B1007909) and a grant from the Kangwon branch of the Korean Society of Gastrointestinal Endoscopy.
Ethics approval
The study protocol was based on the Declaration of Helsinki and approved by the international review board for human research (CR315005-002) of Yonsei University Wonju College of Medicine on June 18, 2015.
Informed consent
Formal consent was obtained from all patients.