
Abstract
Background
Screening for hepatitis C has been found to be beneficial in high-risk individuals and ‘baby boomers’.
Objective
Our aim was to screen for hepatitis C in average and high-risk individuals and compare the disease characteristics and response to treatment among the screened group (SG) and non-screened group (NSG).
Method
Community-based screening for hepatitis C was done in the average and high-risk populations of Qatar. Screening was done using rapid point-of-care testing. All patients with stage 1 fibrosis on liver biopsy were treated with pegylated interferon and ribavirin.
Results
In total, 13,704 people were screened and 272 (2%, 95% CI (1.8–2.2%) had positive antibodies to hepatitis C. During the same period, 237 non-screened patients (NSG) with hepatitis C were referred for treatment. Alanine and aspartate aminotransferases (ALT, AST) and overall fibrosis were significantly lower in the SG as compared with the NSG (p = 0.04, 0.04 and 0.01, respectively). The response to treatment was similar in the SG as compared with the NSG (sustained viral response 61.7 % versus 69.1%, p = 0.55). Average-risk patients had significantly lower ALT levels (p = 0.04) but had similar response to treatment as the high-risk individuals (sustained viral response 63.2 % versus 61%, p = 0.87).
Conclusion
Screening detects hepatitis C with lesser fibrosis but does not result in better response to pegylated interferon and ribavirin as compared with non-screened patients.
Introduction
Despite its discovery more than two decades ago, chronic hepatitis C (CHC) remains a major cause of infectious disease and a leading cause of chronic liver disease throughout the world. 1 The current global prevalence of hepatitis C worldwide is around 3%, corresponding to 130–210 million cases.2–5 Among the Gulf Cooperation Council (GCC) members, the prevalence of CHC ranges between 0.06 and 3.1%.6--9 In North Africa, the highest prevalence is reported from Egypt. 10 It has been suggested that the proportion of those with hepatic decompensation and liver cancer will increase in next 20 years if appropriate treatment is not initiated in a timely manner. 11 A recent report from Centers for Disease Control and Prevention in the United States has revealed that during the period 2002–2007, mortality due to hepatitis C increased by 26%. 12 Recent data from the United States have revealed that more than half of Americans are unaware of having hepatitis C, and only a small proportion of them are actually treated. 13 Also, among those adults who are eligible to be tested for hepatitis C, only 1–12% are actually tested. 14 At present, the United States Preventive Services Task Force recent guidelines do not support screening asymptomatic healthy individuals in the USA but recommends screening only high-risk individuals and single-time screening for adults born between 1945 and 1965—so called ‘baby boomers’. 15 The addition of baby boomers to the screening ambit is a new approach to detect a large number of patients with hepatitis C without screening the entire population. 16 It has been also postulated that since risk-based screening is not implemented rigorously in real-life scenarios, screening the entire population in a birth cohort is more reasonable and cost effective. 17 Other organizations, namely the American Association for Liver Diseases (AASLD), the Infectious Disease Society of America (IDSA) and recently the World Health Organization (WHO), have recommended screening high-risk individuals. 18 Nonetheless, few authors have argued for screening asymptomatic people with CHC and treating them. This helps to eradicate the virus early, reduces hepatic inflammation and ultimately reduces fibrosis. 19 These patients can then be advised to abstain from alcohol and make sure they are immunized against hepatitis A and B, both of which have proven to facilitate fibrosis in patients with CHC. Screening not only helps in preventing the transmission of disease, but also reduces the health care costs of treating decompensated liver cirrhosis and liver cancer. A survey of outpatients visiting various clinics in Seattle revealed that only 15% preferred testing based on clinician judgment (based on guidelines) and wished for universal testing of hepatitis C virus (HCV). 20 A recent study has suggested that if screening is done among a larger cohort of 20–69 year-olds, this might be more cost effective provided that patients are referred early and treated in a timely manner with effective drugs. 21
With this lack of clarity regarding screening of hepatitis C, this study was conducted to ascertain the prevalence of hepatitis C in Qatar, and the effect of screening on treatment outcomes.
Objective of the study
The primary aim of this study was to screen average-risk and high-risk asymptomatic individuals for evidence of hepatitis C infection in a community-based setting.
Secondary aims included comparing the disease characteristics and response to treatment among screened and non-screened hepatitis C patients.
Methods
A community-based survey was conducted to screen for hepatitis C antibodies in the average- and high-risk populations over a 16-month period from December 2008 through June 2010 in Doha, the capital city, Qatar. Ethical approval for conducting the study was taken from Institute Review Board (IRB) of the Medical Research Centre. The high-risk group was defined as per the American Gastroenterology Association Technical committee report
22
as subjects who are either:
– Injection drug abusers – Received a blood transfusion before 1992 – Diagnosed with hemophilia and received clotting factors before 1987 – Persons with frequent percutaneous exposures, including those on hemodialysis, or had inadvertent single needle-stick injury, such as health care workers – Immigrants from countries with a high prevalence of HCV infection – Spouses of persons with CHC infection – Persons infected with human immunodeficiency virus (HIV)
The patients were screened using a visual qualitative kit to detect antibodies against hepatitis C. The Rapid Anti-HCV Test (Health-Chem Diagnostics LLC, FL, USA) used in this study is a colloidal gold enhanced rapid immunochromatographic assay for the qualitative detection of antibodies to HCV in human serum or plasma. It has a sensitivity and specificity of 97–99% and 99%, respectively, for detecting antibodies to hepatitis C as per the manufacturer product claims.
Work-up and management of chronic hepatitis C
All patients detected to have hepatitis C antibodies based on the kit underwent confirmation of the infection using third-generation enzyme-linked immunosorbent assay (ELISA) and quantitative polymerase chain reaction (PCR) testing. Once confirmed, further work-up was done including liver function tests, coagulation profile, viral load, HCV genotype and ultrasound of abdomen. Serum HCV-RNA was detected by reverse transcriptase PCR (RT-PCR-Amplicor Molecular System, Hoffmann-La-Roche) and HCV genotyping was carried out using a line probe assay (Inno-LiPA HCV II, Immunogenetics). All patients who gave written consent underwent percutaneous blind liver biopsy (except for patients with vascular lesions in the liver and morbid obesity, who underwent guided liver biopsy) prior to treatment. Necro-inflammation (grade) and fibrosis scoring (stage) on the liver biopsy was determined using the classification devised by Scheuer. 23 All patients detected to have at least stage 1 disease on the liver biopsy were offered treatment with pegylated interferon and ribavirin. The patients were treated with either Peg-IFN alpha 2 a 180 µg/week (Pegasys, Hoffmann-La Roche) or Peg-IFN alpha 2 b (Pegintron, MSD) 1.5 µg/kg/week, plus weight-based ribavirin daily. Patients infected with HCV genotypes 1 and 4 were treated for 48 weeks with ribavirin, 1000 mg daily in patients with weight of ≤75 kg or ribavirin 1200 mg daily if weight >75 kg, while patients infected with HCV genotypes 2 or 3 were treated for 24 weeks with ribavirin 800 mg daily and Peg-IFN, as per AASLD guidelines. 24 Patients with decompensated cirrhosis, pre-existing autoimmune disorders, history of active alcohol intake, known psychiatric disorders or focal lesions on abdominal imaging suggestive of hepatocellular carcinoma, were excluded from treatment.
Another study was undertaken to assess the safety and adequacy of liver biopsy over a 1-year period during the course of this study. 25 All liver biopsies were reviewed by an experienced hepatopathologist to adequately judge the number of portal tracts as suggested by Farrell et al. 26
Assessment of efficacy
The measures of efficacy were defined as: rapid virological response (Negative HCV PCR at week 4 of treatment), early virological response (absence of HCV-RNA at the end of 12 weeks of treatment), end-of-treatment virological response (undetectable HCV-RNA by quantitative PCR at the end of treatment) and sustained viral response (SVR) (undetectable HCV-RNA by qualitative PCR, 24 weeks after completing treatment).
Statistical analysis
Data were expressed as mean with standard deviation (SD) for interval variables and frequency with percentages for categorical variables. Prevalence and 95% confidence interval (CI) was calculated. Student t-test was used to study the significance of difference between mean values of continuous variables among the screened group (SG) and non-screened group (NSG) group. The chi-square test was used to detect any association between SG and NSG groups for categorical variables. Univariate logistic regression analysis was performed to detect associated factors for response in hepatitis C cases; p ≤ 0.05 (two tailed) was considered a statistically significant level. Data were analyzed with a statistical software SPSS, version 21.
Results
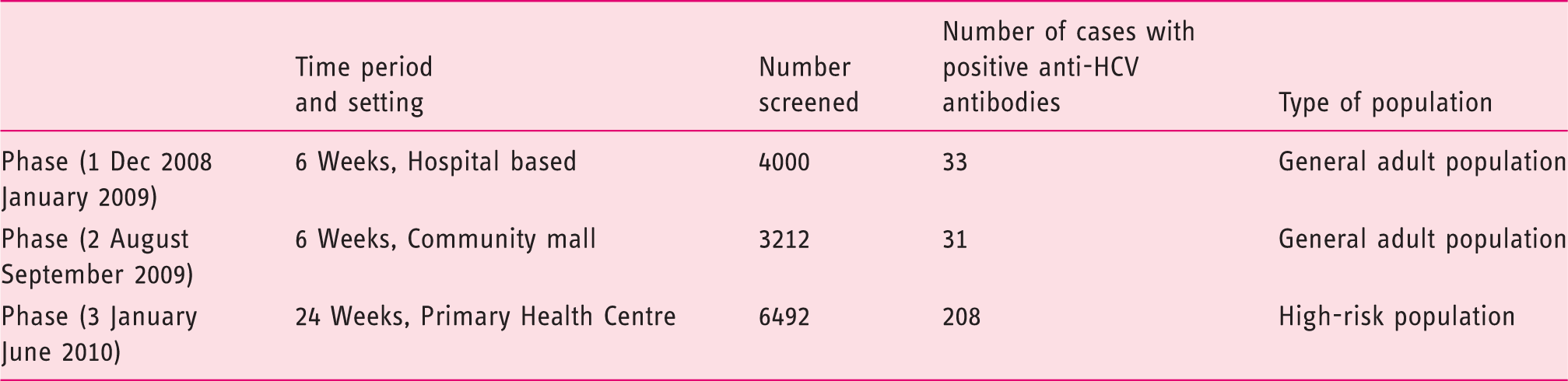
A total of 13,704 people (0.94 % of the population, average population of Qatar in 2008 1,448,479) in the age group of 18–65 years were screened. This comprised both high-risk (6492 people) and average-risk individuals (7212 people). In total, 272 subjects (∼2%) were detected to have antibodies to hepatitis C in the screening survey with 95% CI (1.8–2.2%). The survey was carried out in three phases, in different community settings and in three different time periods (Table 1). Of the 272 people detected to have antibodies, 148 people consented for confirmation and comprised the SG. In the same time period, 237 patients with CHC were referred to our liver clinics for further management and comprised the NSG. Of the NSG, 236 (97%) patients consented for further evaluation and treatment. The entire pathway of screening is shown in Figure 1.
Schematic diagram of the screening survey and comparison of the screening group with the non-screened group. Phases of screening for hepatitis C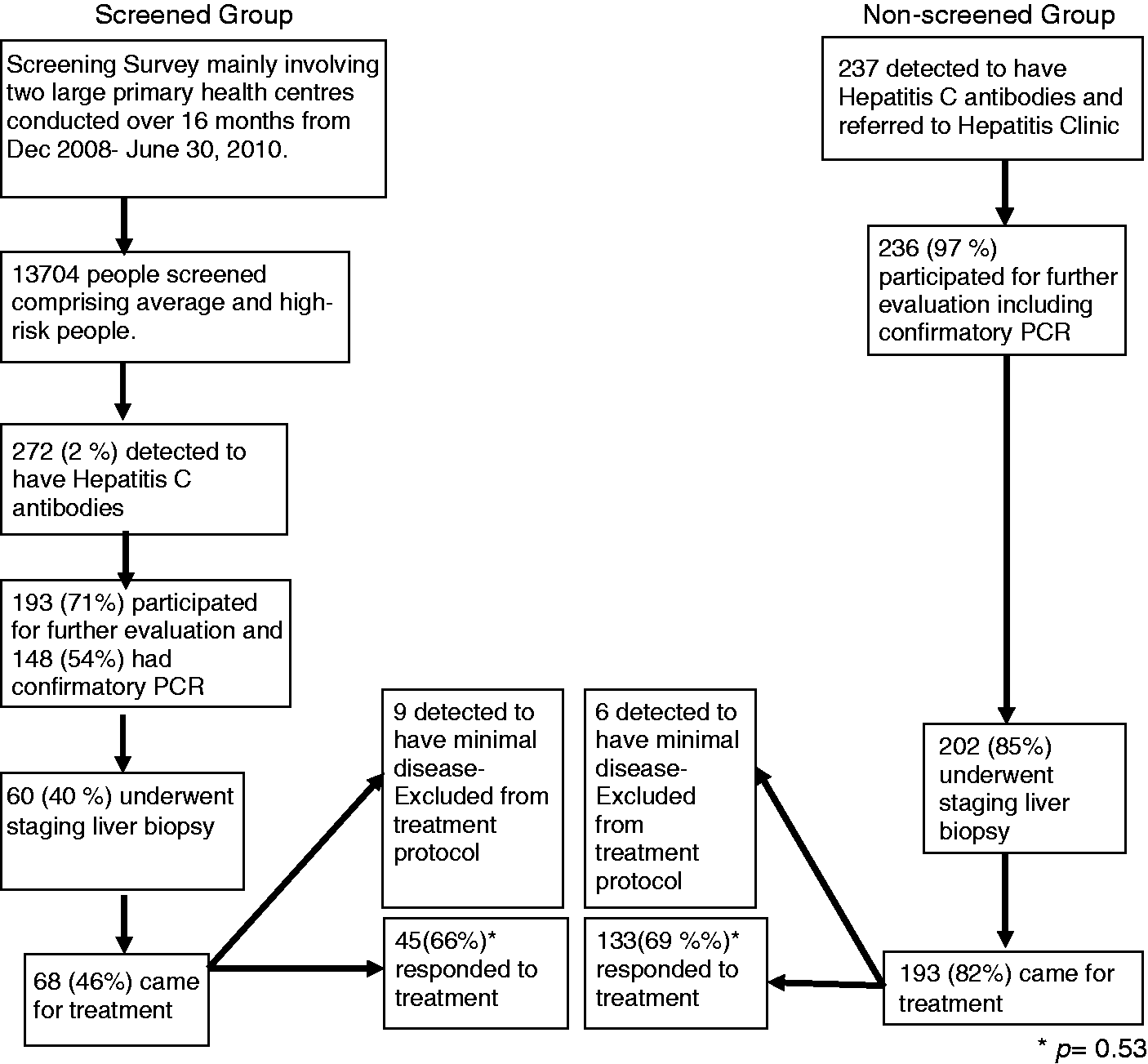
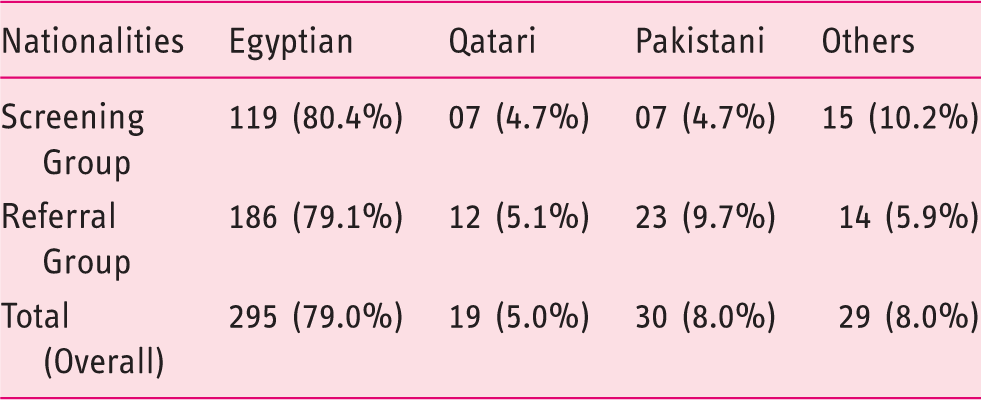
Nationality data of patients and their percentages detected with hepatitis C
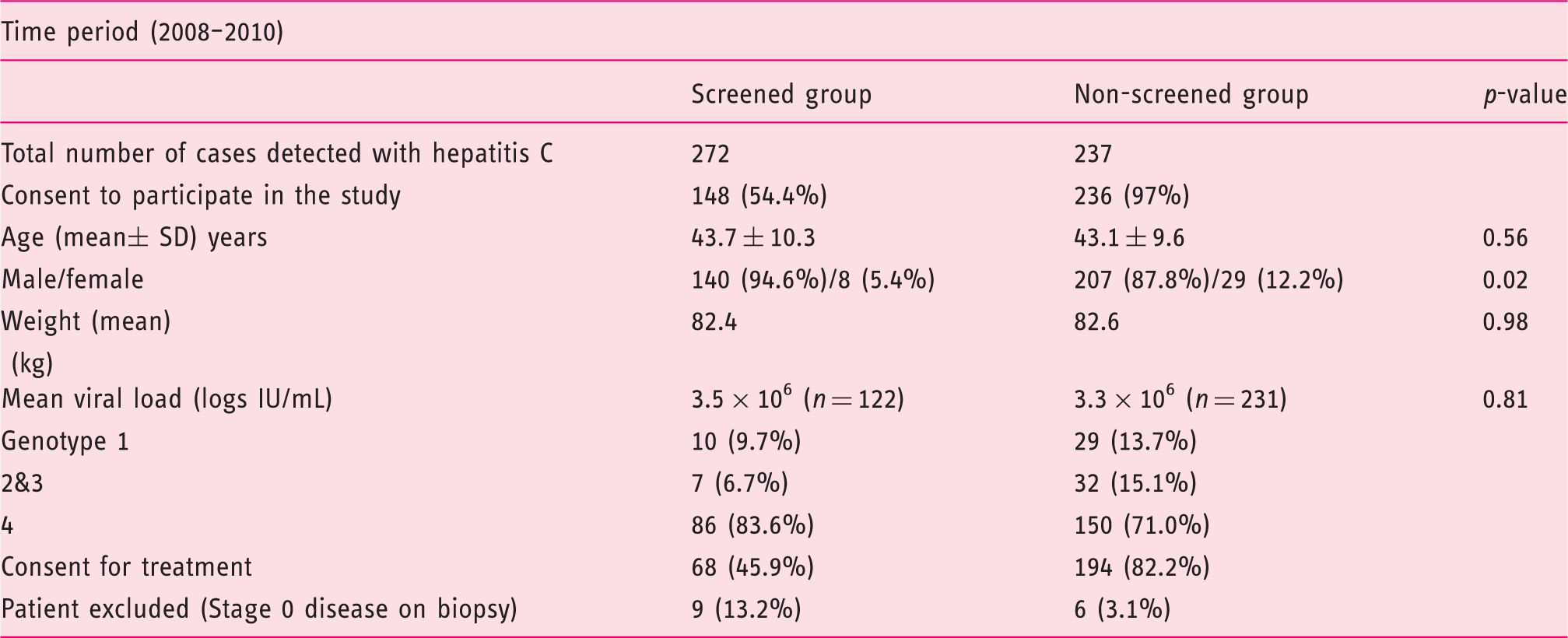
Baseline demographic data of screened and non-screened patients with hepatitis C
Biochemical and histological characteristics of screened and non-screened group
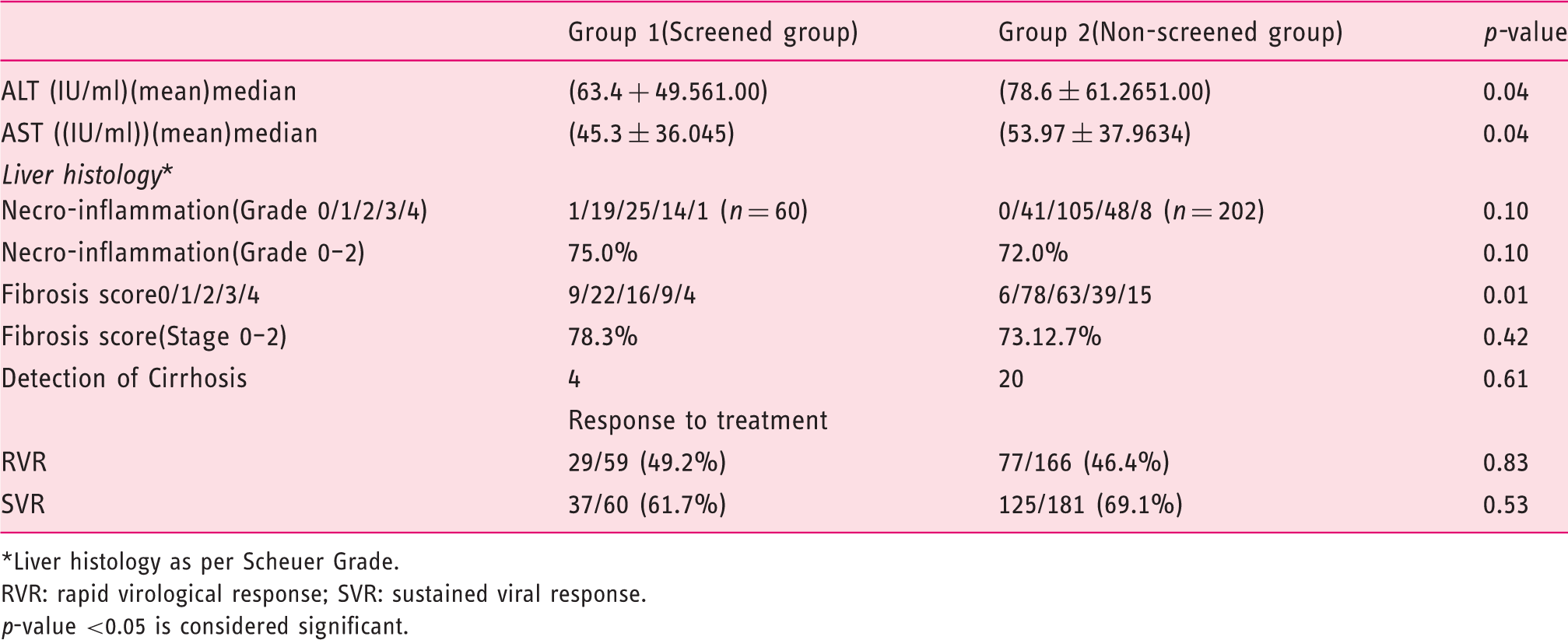
Liver histology as per Scheuer Grade.
RVR: rapid virological response; SVR: sustained viral response.
p-value <0.05 is considered significant.
Comparison of average and high-risk patients among the screened population
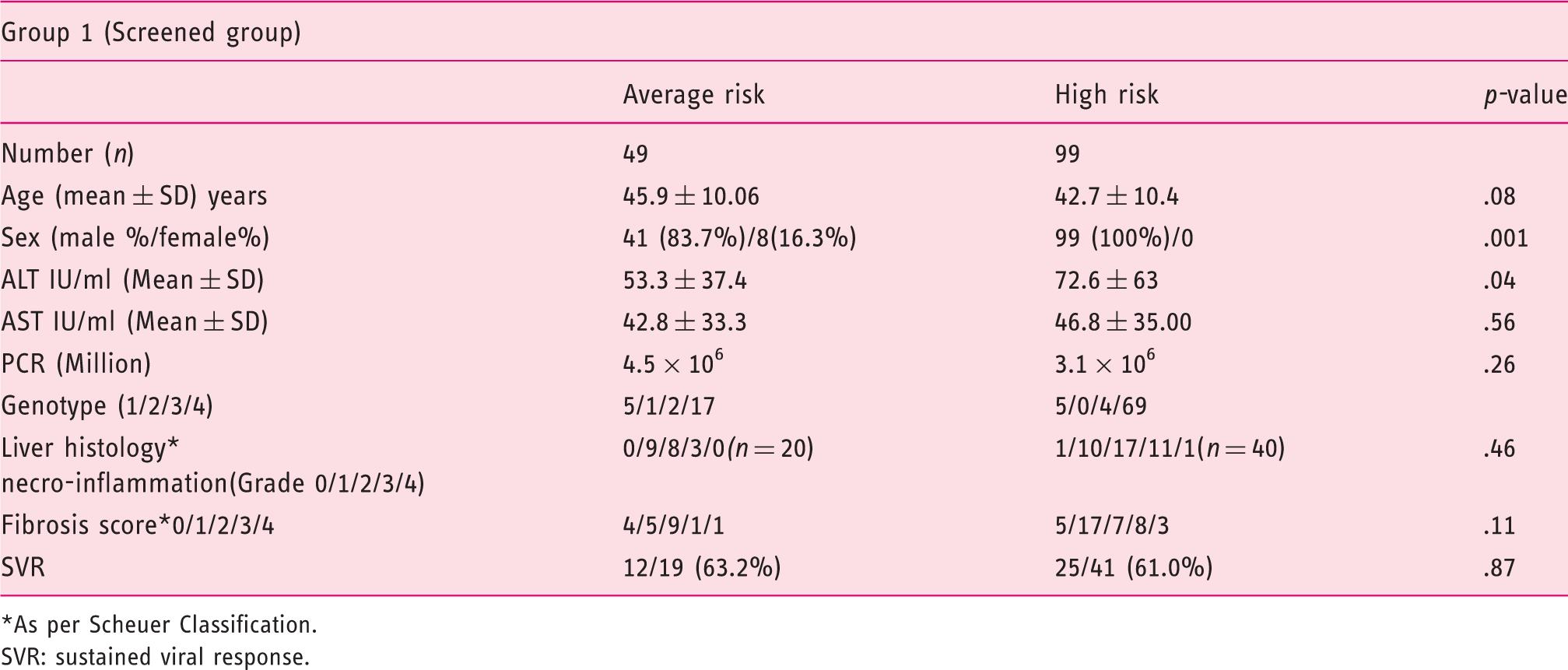
As per Scheuer Classification.
SVR: sustained viral response.
Regarding the safety data of liver biopsy as reported in an associated study by us, 25 none of our patients had any serious adverse event. Some 5% reported minor symptoms, with the predominant one being pain at the biopsy site.
Discussion
This study evaluated nearly 1% of the entire population of Qatar, comprising average and high-risk individuals. The prevalence rate of hepatitis C in Qatar was determined to be 0.8% in average-risk and 3.2% in high-risk individuals (overall ∼2%). These results are similar to previous studies from neighboring Gulf countries. This study is unique in that it is first community-based study to assess the prevalence of hepatitis C among various GCC countries. Previous studies from GCC countries have calculated data from blood banks or hemodialysis registries, which may not be representative of the entire population. The prevalence rate of 2% was higher than previously reported from our centre based on blood bank data. 4 The main reason for the higher prevalence rate has been due to the nature of population studies (blood bank versus community based) and the different time periods (2002–06 and 2008–10). Qatar, at present, is going through a massive infrastructure build-up, resulting in a large influx of expatriates, who comprised approximately 80% of subjects in our study. Another highlight of this study was to evaluate the benefits of screening for hepatitis C in both average and high-risk populations as compared with current strategy of evaluating high-risk patients only. Though the persons detected to have hepatitis C on screening had significantly lower levels of liver enzymes and lesser degree of severe fibrosis, compared with the non-screened patients, they did not show higher SVR to dual anti-viral therapy. The main reasons for this could be (a) the smaller number of patients in the SG; (b) similar demographic profile; and (c) similar viral load (and genotype) in both groups.
This study revealed that the prevalence of hepatitis C among the average-risk citizens of Qatar is low. Nevertheless, it proves that average-risk patients can harbor HCV for a long time. Also, the response to treatment was similar to the high-risk group. It thus becomes important to understand that differentiating patients by risk profile is not pragmatic. Previous experience from the United States has revealed that risk-based screening only detects 25% of HCV-infected people, and a large gap exists between practical and theoretical implementation. 27 To obviate this bias, a recent study has recommended screening all healthy adults between the ages of 45 and 65 years, rather than by their individual risk profile. This was amply reflected in our study also, where the mean age of patients in either of the groups was 44 years.
Our study has many distinct features. It has been demonstrated for the first time there are some direct advantages in screening average and high-risk people in a community. Screening helped in the detection of a large number of “hidden” patients with hepatitis C (236 new cases) using simple, cheap and sensitive point-of-care testing. Early detection led to detection of lower levels of liver enzymes and lesser grade of overall fibrosis. 15% were detected to have histological and biochemical evidence of liver cirrhosis. These patients benefitted from close monitoring for development of decompensation and surveillance for liver cancer. The study also helped us to identify the population with a greater need for screening. This will help our policy planners to identify the gaps in the current process of identification of patients with such diseases. Through an associated study, it was also revealed that there is no serious harm due to liver biopsy in such subjects when it is used as a tool to assess liver fibrosis.
The study has multiple limitations. First, the two groups were not homogenous in terms of duration of infection. Second, there was a high dropout rate among the screened population. This was mainly due to the study group being expatriates—their presence is often transient in nature, with the fear of losing their job or deportation—and long duration of treatment. Third, an interleukin 28 B gene analysis was not done in this study as it was not available in our hospital at that time.
In summary, the prevalence of hepatitis C is low in Qatar. Screening for hepatitis C resulted in the detection of milder disease, but did not result in higher SVR to standard anti-viral treatment over those who are not screened and treated at our hospital. Keeping in view the results of this study and the availability of higher cure rates with the newer oral drugs, larger screening studies are required for complete global eradication of hepatitis C.
Footnotes
Acknowledgement
We acknowledge the help of Roche Pharmaceuticals for providing us the kits for detection of anti-HCV antibodies.
Funding
This study was supported by the Medical Research Centre of the Hamad Medical Corporation (grant MRC 10125/10)
Declaration of competing interest
None declared.