
Abstract
Background
Evaluation of factors correlating with the quality of bowel preparation (QBP) is critical to ensure high-quality colonoscopy.
Objectives
We sought to determine whether the time interval between the start of conventional polyethylene glycol (PEG) ingestion and the onset of bowel activity is predictive of QBP.
Methods
Consecutive adult outpatients attending colonoscopy were prospectively assessed. Data including demographics, medical history, time of starting/completion of PEG and time when bowel activity started were recorded. The QBP was assessed according to the Ottawa bowel preparation score (OBPS); inadequate QBP was OBPS ≥7.
Results
A total of 171 patients (92 males, mean age: 60.5 years) complying with preparation instructions were included. The median OBPS was 5 (range: 1–13) and 57 (33.3%) had inadequate QBP. The median interval between the initiation of PEG and the onset of bowel activity was 60 min (range: 9–300 min). Patients (n = 52, 30.4%) with a delayed (>90 min) onset of bowel activity had poorer QBP (p = 0.0001). In multivariate analysis, male gender (OR: 2.38, p = 0.03), the interval between the end of preparation and the start of colonoscopy (OR: 1.94, p = 0.02) and time to onset of bowel activity >90 min (OR: 3.38, p = 0.004) were predictive of inadequate QBP.
Conclusion
The time interval between the initiation of PEG ingestion and the onset of bowel activity is predictive of the QBP. Our data support “on demand” intensification of bowel preparation in patients with a delayed onset of purgative response to PEG.
Introduction
Colonoscopy is the gold standard for the evaluation of the colon and a valuable preventive tool with proven efficacy in lowering the burden of colorectal cancer.1,2 However, the diagnostic and therapeutic yield of colonoscopy is critically dependent on the quality of bowel preparation. Cecal intubation rate and polyp detection rate, key quality indicators in colonoscopy, are adversely affected by poor bowel preparation.3–5 Moreover, poor preparation is associated with increased technical difficulty, enhanced risk of complications, and further costs as repeated or alternative investigations have to be organized.6,7
A split regimen of 4 L of polyethylene glycol (PEG) solution (or a same-day regimen for afternoon colonoscopies) is widely recommended for routine bowel preparation due to its good efficacy, tolerability and favourable safety profile. 8 However, despite continuous efforts for improved laxative agents, at least 20% of all colonoscopies have inadequate preparation.5,9,10 Satisfactory bowel preparation is a complex and hard to predict outcome, as it depends not only on the regimen used, but requires a close adherence to preparation instructions and a precise timing.11,12 Moreover, bowel preparation is heavily affected by patient-related factors, thus ideally it should be tailored according to individual needs and personal characteristics.13,14 Although different predictors correlating with cleansing efficacy have been put forward, none has allowed as yet for wide implementation of individualized bowel preparation protocols. In this setting, the predictive relevance of factors reflecting the magnitude of the purgative response to PEG, such as the onset, timing or frequency of defecation, remains unknown.
Herein, we aimed to prospectively identify factors associated with an inadequate level of bowel preparation. In particular, we sought to determine the predictive ability of the interval between the start of PEG intake and the time when the first bowel movement occurred during bowel preparation. This was prompted by the observation that patients with poor bowel preparation frequently described a delayed onset of bowel activity in response to PEG.
Materials and methods
Subjects
In this prospective observational study we included consecutive adult outpatients attending colonoscopy at the endoscopy unit of the Konstantopoulion General Hospital of Athens between 1 June and 31 July 2012. The unit offers open-access colonoscopy service by direct referral from either primary or secondary care physicians. Both morning (starting time between 8 AM and 11:59 AM) and afternoon (12 PM and thereafter) colonoscopies were eligible for inclusion. Age <18 years, history of colon surgery and/or inflammatory bowel disease, incomplete colonoscopy unrelated to the quality of bowel cleansing, bowel preparation different than 4 L-PEG, and non-adherence to bowel preparation instructions were exclusion criteria. The study protocol was approved by the local ethics committee and informed written consent was obtained from all participating subjects.
Bowel preparation and colonoscopy procedures
A standard 4 L-PEG solution (Fortrans®, Ipsen EPE, Athens, Greece) was used in the study, consisting of PEG 4000 plus electrolytes (potassium chloride, sodium chloride, sodium bicarbonate, sodium sulphate anhydrous). Dietary instructions were given as follows: consume a low-residue diet for 2 days before starting the bowel preparation; on the day before colonoscopy have a light breakfast, a light lunch scheduled before 13:00 PM, but only a clear-liquid diet thereafter. All patients were thoroughly instructed to take the preparation diluted into 4 l of plain water at a quantity per interval of one glass (8 oz) every 15 minutes. Additional intake of at least 1 l of clear fluid was recommended. Choice of the bowel preparation schedule was not standardized. However, according to the local protocol, administration of the bowel preparation entirely the day before colonoscopy (i.e. a 4 L/0 L PM/AM dosing schedule) was recommended for procedures scheduled early in the morning (before 10 AM) and a split-dosing schedule (either 3 L/1 L or 2 L/2 L) was used for “late” morning procedures, whereas a 0 L/4 L “same-day” dosing schedule was preferred for afternoon sessions. Adherence to bowel preparation instructions, including administration of the entire volume of the solution and proper quantity per interval intake, were checked by an endoscopic nurse upon arrival of all patients at the endoscopy unit.
All colonoscopies were performed by three experienced endoscopists (KDP, AG and NM; range of experience: 15–20 years) contributing equally to morning and afternoon sessions. A standard video endoscope (CF-Q165L, Olympus, Tokyo, Japan) was used for all procedures. Colonoscopies were performed under conscious sedation using midazolam 1–5 mg alone or in combination with fentanyl 25–50 mcg.
Data collection
At the time of colonoscopy booking all patients were provided with take-home diaries to record the amount and timing of PEG and additional fluids taken, time of start/completion of bowel preparation and time when the first bowel movement occurred after the start of PEG. A pre-endoscopic evaluation, performed by a physician other than the endoscopist, included the following variables: gender, age, body mass index (BMI), previous abdominal surgery, previous colonoscopy, constipation (<3 bowel movements/week), family history of colon cancer and presence of comorbidities. The indication for colonoscopy as well as the time interval between the end of bowel preparation and the start of colonoscopy were also noted.
Assessment of bowel preparation quality
Colonic cleanliness was graded according to the Ottawa Bowel Preparation Scale (OBPS). The OBPS assigns a 5-point score to each colonic segment (right, mid and rectosigmoid colon): 0 = excellent, 1 = good, 2 = fair, 3 = poor and 4 = inadequate. In addition, the overall colonic fluid is rated according to a 3-point score (0 = small, 1 = moderate, 2 = large). A summary score is then obtained, ranging from 0 to 14 (higher is worse). Before initiation of the study, all participating endoscopists were trained in the use of OBPS, including repeated calibration exercises until achievement of an excellent inter-rater agreement (intraclass correlation coefficient >0.8). To assess the quality of bowel preparation as a categorical outcome we have dichotomized the OBPS score values assuming a score of 7 or higher as indicative of inadequate bowel preparation.
Statistical analysis
The statistical analyses were performed using SPSS statistics version 22 (SPSS, IBM, Chicago, IL, USA). Categorical variables are expressed as percentage. Continuous data are reported as means with standard deviation for variables with a normal distribution and median with range for those with a non-normal distribution. Categorical variables were compared using χ 2 or Fisher’s exact test. The Student t-test was used to compare continuous variables with normal distribution and the Mann Whitney U test and Kruskal–Wallis test for variables with a non-normal distribution, as appropriate. Univariate analysis was evaluated to identify associations with inadequate bowel preparation (OBPS score ≥7) and factors with significance of <0.1 were entered into multivariate logistic regression model. All analyses were two-sided and p-values <0.05 were considered statistically significant.
Results
Study population
A total of 232 patients were assessed for eligibility. In all, 61 (26.3%) patients were excluded: six had a history of colon surgery, five had inflammatory bowel disease, four received bowel preparation different than PEG, eight had incomplete colonoscopy irrespective to the quality of bowel preparation and 38 were non-compliant with the bowel preparation instructions (non-adherence to dietary instructions: 11, incomplete volume: 12, inappropriate interval within which the bowel preparation was taken: 15). Therefore, 171 patients (92 males, 53.8%; mean age: 60.5 ± 11.3 years, range: 28–85 years) finally comprised the study population. Of these, 68 (39.8%) had a previous colonoscopy, 26 (15.2%) reported history of abdominal surgery and 31 (18.1%) reported constipation, whereas a family history of colon cancer was noted in 17 (9.9%). The mean BMI was 26.6 ± 3.7 kg/m2, with 28 (16.4%) patients having a BMI ≥30. A total of 78 (45.6%) patients reported a history of at least one comorbid condition; 29 (17%) reported diabetes, 35 (20.5%) arterial hypertension, seven (4.1%) cerebral vascular disease, 19 (11.1%) thyroid disease, 10 (5.9%) ischemic heart disease and three (1.8%) patients reported liver cirrhosis. The vast majority (142, 83%) underwent colonoscopy in the morning session. Screening/surveillance for colorectal cancer prevention was the most common indication for colonoscopy (77.8%), followed by anaemia (5.9%), rectal bleeding (5.9%), abdominal pain (4.7%) and diarrhoea (1.8%), whereas other indications comprised 4.1%.
Bowel preparation
Some 65 (39.2%) patients drunk the whole volume of bowel preparation on the day before colonoscopy (i.e. a 4 L/0 L PM/AM dosing schedule), whereas 106 (60.8%) had at least one dose of bowel preparation on the same day of the procedure according to a 3 L/1 L (n = 62, 36.3%), 2 L/2 L (n = 27, 15.8%) or 0 L/4 L (n = 15, 8.8%) PM/AM schedule. The median volume of additional fluids administered during bowel preparation was 0.5 L (range: 0–3 L), with 76 (44.4%) of patients taking at least 1 L of additional fluid. The time interval between the completion of PEG intake and the start of colonoscopy was 2–4 h in 32 (18.7%), 4–6 h in 60 (35.1%), 6–8 h in 11 (6.4%), 8–10 h in five (2.9%) and >10 h in 63 (36.8%) patients.
The cecum was reached in all patient procedures. The median OBPS score was 5 points (range: 1–13). The right colon was rated higher (median: 2, range 0–4) as compared with the mid and rectosigmoid colon (each with median score 1, range 0–4), whereas the median OBPS rate for fluid volume was 1 (range 0–2). Of the patients, 57 (33.3%) had an inadequate (total OBPS score ≥7) level of bowel preparation. No difference in median OBPS scores was shown based on the physician who performed the colonoscopy (p = 0.76). The OBPS scoring values with respect to bowel preparation adequacy are shown in Figure 1. Patients with inadequate bowel preparation had significantly higher median OBPS scores on each colon segment and fluid amount (p = 0.0001 in all comparisons).
Total OBPS score and individual scoring values for each colon segment and fluid amount with respect to the level of bowel preparation adequacy. Error bars represent 95% confidence intervals.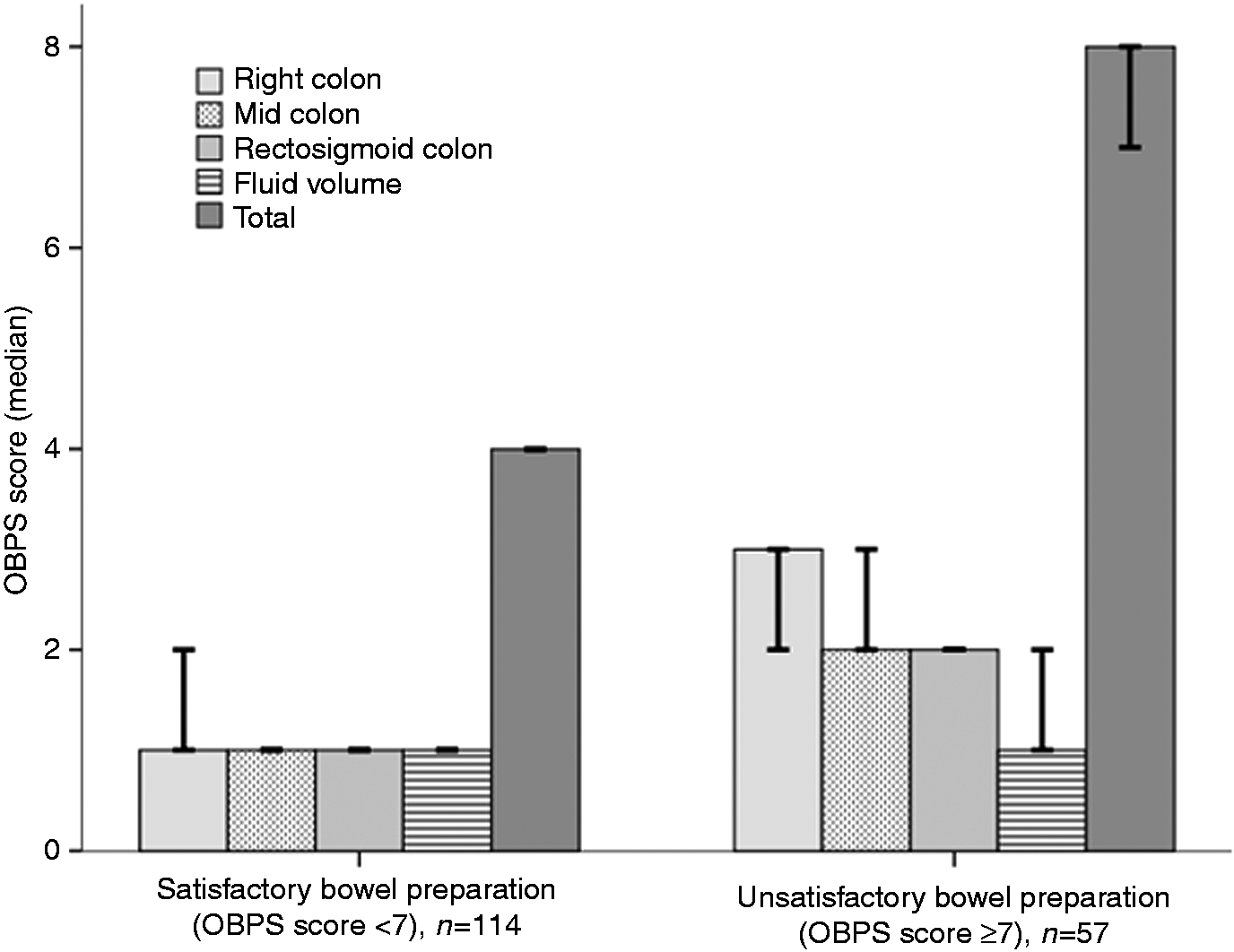
Interval between the start of PEG intake and the onset of bowel activity: relationship with bowel preparation quality
The median interval between the start of bowel preparation and the time when the first bowel movement occurred was 60 min (range: 9–300 min). Some 37 (21.6%) patients had the first bowel movement occurring within 30 min, 94 (54.9%) within 60 min and 119 (69.6%) within 90 min from the start of PEG. The relationship between the timing of onset of bowel activity after the start of PEG and the quality of colonic cleanliness according to OBPS is shown in Figure 2. Overall, the total OBPS score was significantly higher in patients in whom bowel activity occurred >90 min from the start of PEG (n = 52, 30.4%; median OBPS = 7, range: 1–13) as compared with those with a more rapid onset of bowel movements (median OBPS: 4, range: 1–12; p = 0.0001). The difference was statistically significant on right colon (p = 0.0001) and fluid amount (p = 0.03), whereas statistical significance was not reached for mid (p = 0.06) and rectosigmoid (p = 0.16) colon.
Relationship between the timing of onset of bowel activity after the start of polyethlylene glycol (PEG) intake and the quality of bowel preparation according to the Ottawa Bowel Preparation Scale (OBPS). Error bars represent 95% confidence intervals. p-values regard comparisons between total OBPS scores.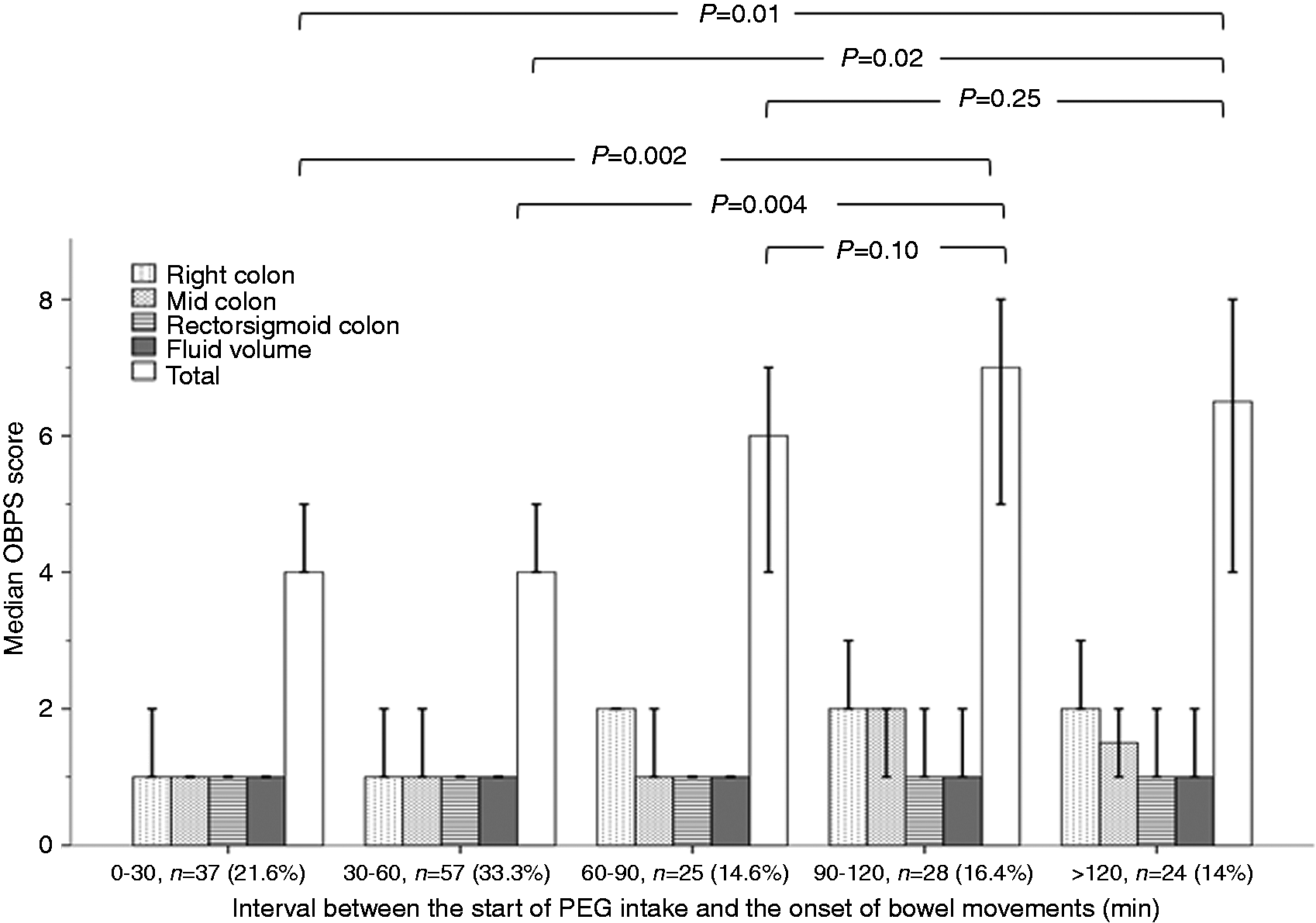
Factors correlating with inadequate bowel preparation
Univariate analysis of factors correlating with the adequacy of bowel preparation
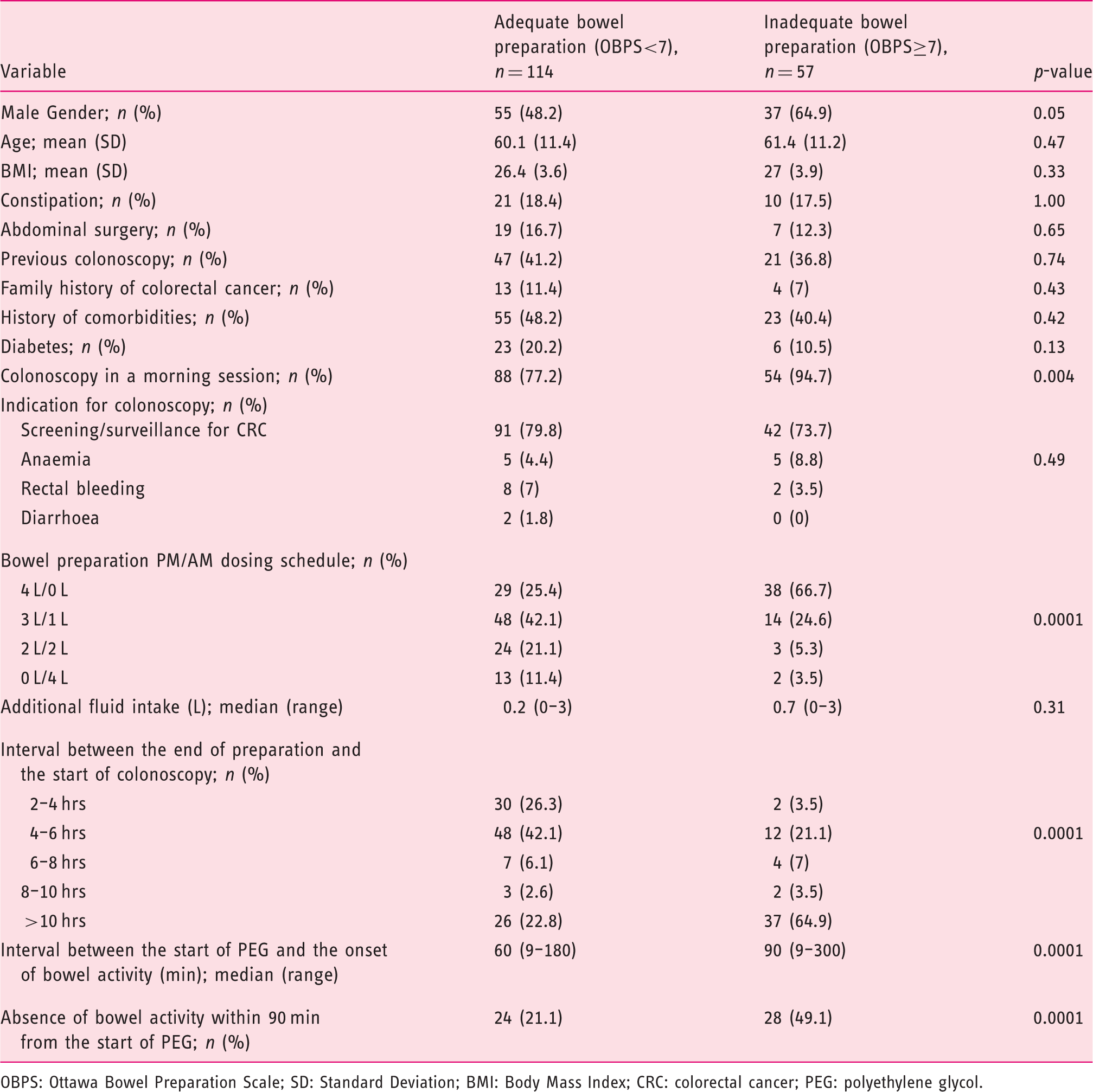
OBPS: Ottawa Bowel Preparation Scale; SD: Standard Deviation; BMI: Body Mass Index; CRC: colorectal cancer; PEG: polyethylene glycol.
Multivariate analysis of factors correlating with inadequate (OBPS score ≥7) bowel preparation. The time interval between the start of PEG and the onset of bowel activity was analysed either as a continuous variable (2(a)) or as a categorical variable using a 90 min time cut-off (2(b))
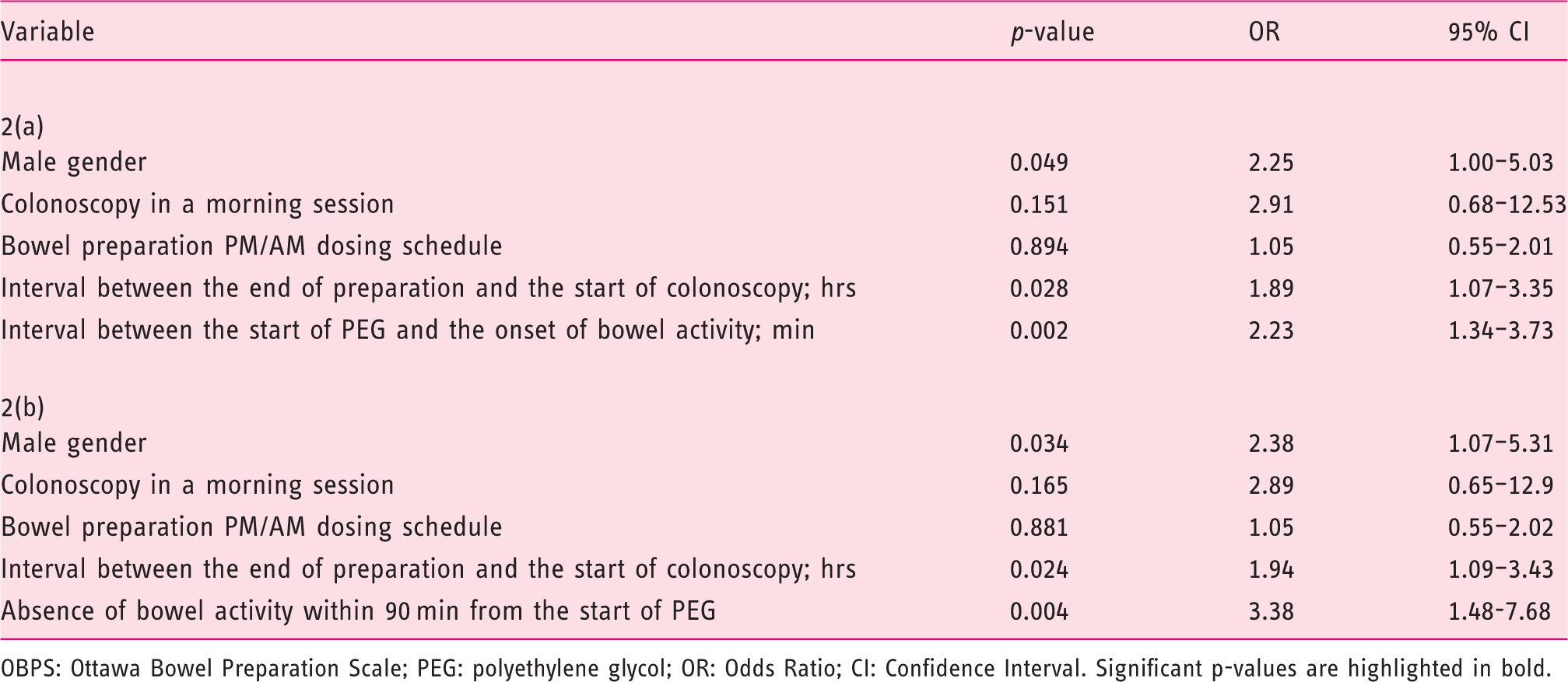
OBPS: Ottawa Bowel Preparation Scale; PEG: polyethylene glycol; OR: Odds Ratio; CI: Confidence Interval. Significant p-values are highlighted in bold.
Discussion
We determined prospectively that, in patients complying with the recommended volume per interval ingestion of PEG, lack of bowel activity within 90 min from the start of the purgative was a predictor of inadequate bowel preparation. To our knowledge this is the first report demonstrating that a delayed purgative response to PEG may be interpretable as a surrogate of bowel preparation failure. Our results support “on demand” intensification of bowel preparation (e.g. use of an additive laxative) if no bowel activity occurs within a predetermined interval from the start of PEG. To date, only few studies record variables reflecting the individual purgative response such as the timing and frequency of defecation and stool character.15,16 Recently, Kim et al. determined that defecation frequency (>5 times) and liquid stool without solid material immediately before colonoscopy were predictive factors for adequate bowel preparation with PEG. 15 Comparisons between studies should be attempted cautiously due to significant heterogeneity, including differences in patients’ characteristics, timing of bowel preparation, dietary instructions and scales to assess colonic cleanliness. However, our data seem to be in agreement with previous series in which inadequate bowel preparation regarded >30% of all colonoscopies, highlighting the need for more dedicated bowel cleansing strategies.17–19 Our study prospectively validates in a European population the adverse impact of male gender on bowel preparation quality, previously outlined in series from the USA and Asia. Including 501 patients, Chan et al. determined that males had a 1.6 times risk of poor bowel preparation compared with females, 20 whereas this risk was 1.4 in a study with 10,921 subjects. 10 Advanced age has been advocated as another patient-related factor correlating with poor bowel preparation.10,17,20 However, including 300 outpatients undergoing screening colonoscopy, the mean age was 66.2 years in patients with inadequate preparation vs. 62.5 years in the adequate preparation group (p = 0.01). 21 Therefore, a relatively younger patient population (mean age: 60 years) may have precluded age associations in the present study.
A prolonged interval between the completion of PEG and the start of colonoscopy is another relevant predictor of inadequate colonoscopy preparation.22–24 Previous investigations have assessed the optimal time interval to determine satisfactory bowel preparation: <4 h in a study by Eun et al., 22 3–5 h in a study by Seo et al., 23 and 5–6 h in a more recent study. 12 Congruently, our data support performance of colonoscopy at 4–6 h from the end of bowel preparation. Indeed, the majority (68.4%) of patients with adequate bowel preparation had colonoscopy within 6 h from the completion of PEG, as compared with only 24.6% in the inadequate bowel preparation group. History of comorbidities, especially diabetes, is another poor predictor, and other factors such as unmarried status, Medicaid insurance and low health literacy have been linked to inadequate colonic preparation.17,21,25 However, we could not identify statistically significant associations with respect to comorbidities, even when diabetes was analysed separately, whereas socioeconomic factors were not assessed, precluding us from drawing conclusions.
There are limitations to the present study. Firstly, although we included only outpatients known to have better bowel cleansing,19,20 a disappointing one-third had inadequate bowel preparation. This may be due to the fact that a significant proportion (39.2%) received the whole preparation on the day before colonoscopy as, by the time of study enrolment (mid 2012), use of split dosing was not fully incorporated into our institutional practice. These patients had prolonged (> 8 h) preparation-to-colonoscopy intervals, resulting in worse OBPS (median: 7, range: 1–13) compared with those receiving split-dose or same-day schedules (median: 4, range: 1–12; p = 0.0001). However, both the dosing schedule of PEG and the interval to colonoscopy were adequately considered in the multivariate model, precluding an impact of “non-split” institutional practice to the main findings of the study. Secondly, similarly to previous investigations, we used an arbitrary OBPS cut-point to determine inadequate bowel preparation.12,22,23 Adequate colon cleansing should ideally be defined as one that permits the detection of all polyps >5 mm in size although, to the best of our knowledge, no data are available to link any bowel preparation scoring system to this definition. 26 Nevertheless, independent predictors determined in the present study remained significant even when slightly different OBPS cut-points were analysed. Thirdly, selection of patients based on strict compliance criteria (as indicated by the relatively high dropout rate of 26.3%) may limit the generalizability of the results to every day clinical practice. Lastly, due to the relatively small sample, factors influencing the quality of bowel preparation may not be adequately reflected.
In conclusion, using the validated Ottawa scale, we determined prospectively that the timing of onset of the purgative response to PEG may hold predictive relevance on the outcome of bowel preparation. Our study adds significantly to pertinent literature. It provides a novel parameter that can be easily evaluated in clinical practice, allowing the patient to self-monitor his/her bowel preparation. If the first bowel movement occurs >90 min from the initiation of PEG, then the quality of the obtained preparation should be expected to be inadequate. This should inform the patient, while bowel preparation is still ongoing, on the need to intensify his/her bowel cleansing protocol. Clearly, external validation is required to ensure the generalizability of our data. Nevertheless, the current study is intended to stimulate further research on the feasibility of tailoring bowel preparation according to the individual purgative response. This perspective remains to be addressed in future randomized studies.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicts of interest
None declared.