
Abstract
Background
Capsule endoscopy is a widely performed procedure for small bowel investigation. Once swallowed by the patient, the capsule transmits images to an external recorder over a digital radiofrequency communication channel. Potential electromagnetic interferences with implantable cardiac devices have been postulated. Clinical studies on the safety of capsule endoscopy in patients with cardiac defibrillators are lacking.
Objective
The aim of this study was to assess potential mutual electromagnetic interferences between capsule and defibrillators.
Methods
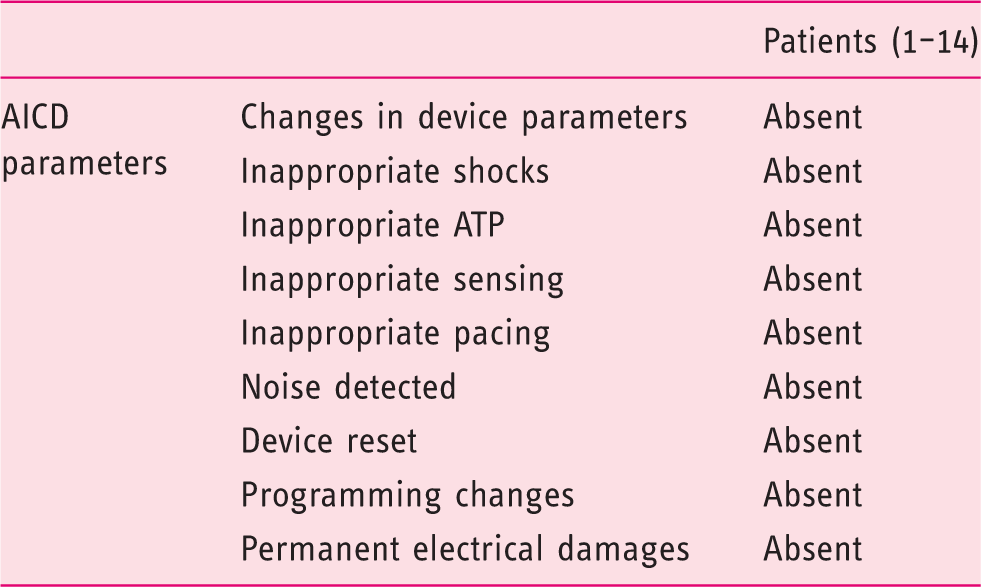
This study used the Given M2A video capsule system. Ten different types of defibrillators were tested in a clinical setting. Before capsule ingestion, defibrillator electrical therapies were switched off. During capsule endoscopy patients were monitored with cardiac telemetry. At the end of capsule endoscopy the following defibrillator’s parameters were analysed: change in device settings; inappropriate shocks; inappropriate anti-tachycardia therapy; inappropriate sensing or pacing; noise detection; device reset; programming changes; permanent electrical damages. Any technical problem related to capsule image transmission was recorded.
Results
Neither defibrillator malfunction nor interference in sensing or pacing was recorded; conversely, no capsule malfunction potentially caused by defibrillators was registered.
Conclusion
Our results suggest that capsule endoscopy can be safely performed in patients with cardiac defibrillators.
Introduction
Capsule endoscopy (CE) is one of the most performed endoscopic procedures for small bowel investigation and is considered one of the safest in clinical practice. 1 However, potential electromagnetic interferences (EMI) with implantable cardiac devices have been postulated.2,3 In fact, once swallowed by the patient, the capsule transmits images from the digestive tract to an external recorder over a digital radiofrequency communication channel (434.09 MHz). This could theoretically lead to malfunction of pacemakers (PM) and automatic implantable cardiac defibrillators (AICD). Conversely, the presence of an implantable electronic device (IED) could interfere with image transmission from the capsule to the recorder. Relatively few safety data are available on EMI between CE and IEDs. ‘In vivo’ studies are lacking, especially in patients with AICD. The aim of this study is to assess potential mutual EMI between CE and AICD in a clinical setting.
Methods
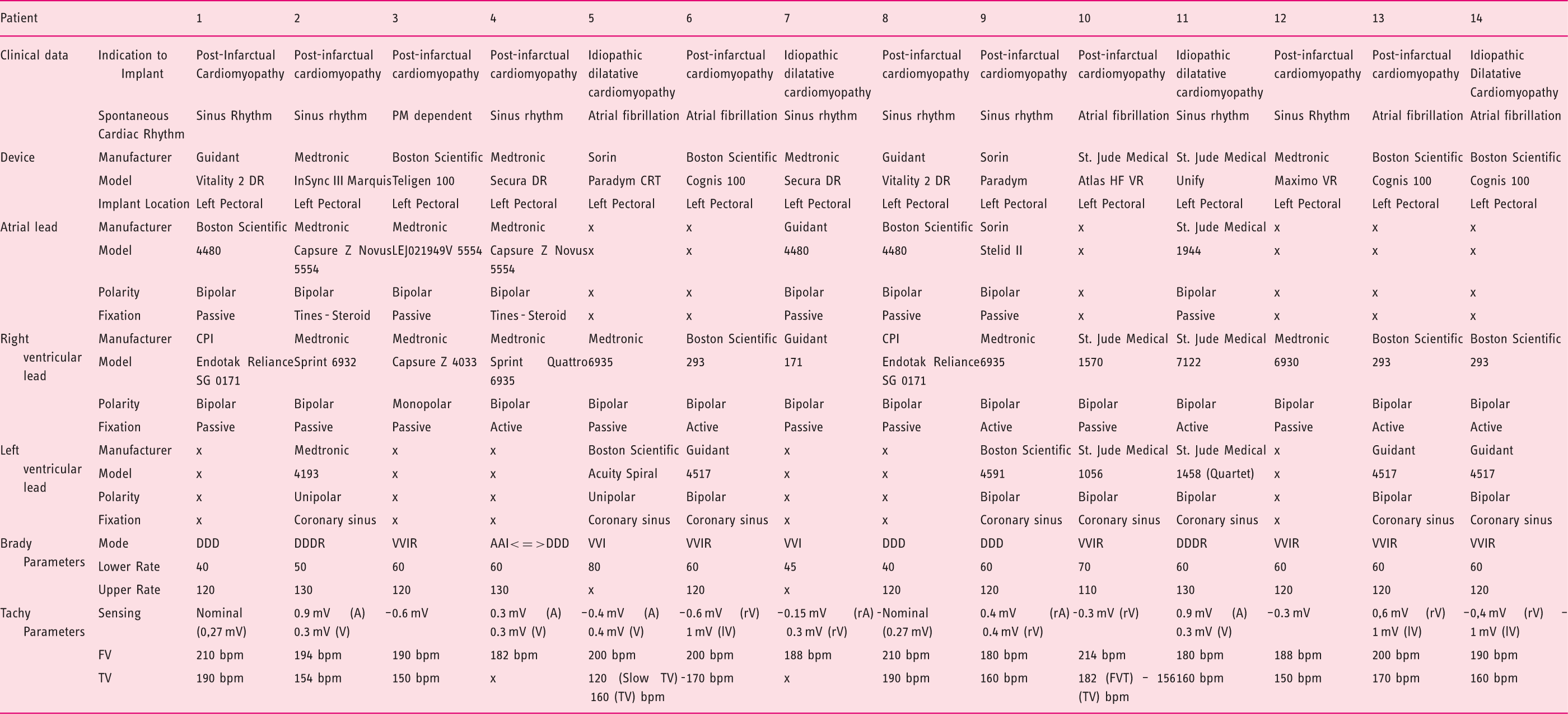
Between October 2008 and October 2011, 14 patients with AICD were prospectively studied by using the Given M2A video capsule system (Pillcam; Given Imaging Ltd, Yoqneam, Israel). Eleven patients were males. The mean age was 66.4 years. The indication for CE was obscure gastrointestinal bleeding (OGIB) in 13 cases (7 overt- and 6 occult-type) and clinical follow up in a patient with Peutz–Jeghers syndrome. All the patients gave their written informed consent. Patients swallowed the capsule in the morning after an overnight fast; a bowel cleansing with 2 litres of polyethylene glycol solution was administered in the afternoon before the procedure.
Patients’ clinical data and technical AICD details (A = atrium; V = ventriculum; r = right; l = left; bpm = beat per minute)
Results
Results of AICD control after CE
Discussion
The major endoscopic concern in patients with IED is the possibility to generate EMI during electrosurgical therapies. This can emerge into device malfunctions or damages and whatever consequent injuries on patients. 4 For this reason, particular precautions have to be taken in these subjects in order to minimize the risk of adverse events. 5 The effects of EMI can be very different and depend on factors related to the type and settings of the electronic emitting device (frequency and duration of the signal produced, distance between IED leads and source of electromagnetic signal, electrodes and filter configuration, selected sensitivity level, orientation of the pulse generators and leads with respect to the EMI source). EMI can lead to inappropriate inhibition or triggering of pacing activity, asynchronous pacing, resetting or reprogramming of the software device, permanent structural damages, and inappropriate anti-tachycardia therapy such as pacing or shocks, that could be life-threatening in PM-dependent patients and in patients with AICD. 6
A potential EMI cannot be excluded ‘a priori’ during CE, too. In fact, once ingested, the capsule generates electromagnetic waves by using the radio-frequency technology for the images transmission from the digestive tract to the external recording system worn by the patient. Even if the most recent CE guidelines do not consider the presence of a cardiac implantable device as an absolute contraindication, 7 the Food and Drug Administration and capsule manufacturers (Given Imaging, Israel and Olympus, Japan) recommend to avoid CE in patients with PM or AICD, because of a very limited clinical experience. In this study we report the use of CE in patients with 10 different types of AICD. Some of them were never been tested before for possible EMI. These devices were technically very heterogeneous in terms of models and polarity of ventricular and atrial leads, and bradycardia/tachycardia parameters. The mainstay of this series is the electrophysiological study performed during the whole duration of CE. In fact, the design of this ‘in vivo’ study allowed the ability to record every eventual EMI-induced AICD malfunction or EMI-related changes in devices parameters related to CE. The deactivation of the AICD electrical therapies during CE did not influence its ability to recognize EMI. In fact, this configuration (‘monitor only’) enables ventricular tachyarrhythmia detection but does not automatically deliver electrical therapy to the patient. The choice to set the AICD to the ‘monitor only’ mode was due to the intention of avoiding possible EMI-related inappropriate shocks. In order to ensure their safety, the patients were placed in Cardiac Care Unit and continuously monitored with telemetry during the endoscopic procedure. We opted for Mortara X12 as the monitoring patient system because we did not observe any interference of the ECG wireless transmission during CE in our previous clinical experience with this type of device.
In all the cases no EMI between CE and AICD were observed, irrespectively to the AICD properties. The outcome was the same even when the distance between the two devices was very short and the electromagnetic fields generated from capsule and AICD could more easily overlap (especially during the oesophageal capsule transit). The radiofrequency wave originated by the capsule is a pulsed signal of about 434 MHz, composed of an active signal of transmission of 250 ms followed by a pause of 250 ms, too. A possible explanation of the absence of mutual EMI in this situation is the low power of this signal (1 µW). In fact, on the basis of studies on mobile phones, it has been argued that the power of electromagnetic signal from the capsule should be 1mW in order to generate EMI in this situation. 8
Data regarding possible interferences between CE and AICD are very limited, although abnormal EMI-induced functioning of these devices could lead to potentially life-threatening clinical injuries. Bandorski et al. tested in a laboratory setting eventual interactions between 45 AICDs and three different types of capsules (Pillcam SB and Pillcam Colon, Given Imaging; Endocapsule, Olympus): 8 no interferences were observed even the devices were placed in close proximity. Dubner et al. reported the first case of EMI between CE and AICD in an ‘in vitro’ study performed with a reusable external testing device (Test Cap, Given Imaging Ltd, Yoqneam, Israel) that reproduces, 9 at the same electromagnetic frequency, the data transmission of Pillcam capsule: an over-sensing (heart signals are seen, though do not exist) was recorded, potentially leading to inappropriate electric therapies delivery. However, no interferences were reported by the author when the Test Cap was used in a series of six AICD patients. In a recent retrospective multicentre investigation, Bandorski et al. reported the use of CE in 51 patients with PM and 11 patients with eight different types of AICD: 10 no impairment in cardiac devices function nor clinical adverse events were observed. However, cardiac telemetry was not performed in all the cases and specific data regarding AICD during CE are not available. Analogue limits are present in a retrospective series from Cuschieri et al.: 11 five patients with AICD undergoing CE were monitored with telemetry. However, it was not possible to verify concomitant interferences between the devices because in all the patients the cardiac device detection capability was switched off during the endoscopic procedure. Except for our preliminary findings, 12 complete data on AICD function during CE are available only in a few very small clinical studies,13–15 and in a case report involving a total number of 13 patients. 16 In all these studies, neither was cardiac telemetry abnormal functioning recorded during CE nor AICD damage reported at the post-procedural device checks.
In light of previous studies and our results, at present we perform CE in persons with AICD as out-patients, without requirements of preventive changes in AICD settings. We are still performing and strongly suggest AICD technical checks before and after CE, because of the high number of different AICD available on the market and the extreme variability of their functioning parameters. This is in order to verify the AICD stability and to collect, in an internal registry, as many data as possible regarding this field. In case of abnormalities at the AICD check prior to CE we propose the execution of CE as in-patient, with cardiac telemetry. We also perform an AICD control after CE in case of image corruptions during the view of CE video.
Conclusions
This study is the largest prospective series ever presented in order to investigate eventual EMI between CE and AICD. We studied 10 different types of AICD in a specifically designed clinical setting, instructed to perform a complete AICD control before, during and after CE. The results confirm the absence of mutual EMI between CE and AICD. In fact, in all the patients no AICD dysfunctions, interferences in sensing or pacing or dysrhythmias were found. Moreover, no electrical permanent injuries or changes in device setting were recorded. Conversely, the review of CE videos did not reveal interruptions, disturbances or loss of endoscopic images. This study suggests that CE can be safely performed in patients with different types of AICD. However, the small number of patients reported in the published data and the high heterogeneity of cardiac devices do not consent, in our opinion, to suggest definitive recommendations for managing CE in these patients.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest
The authors declare that there are no conflicts of interest regarding the publication of this article.