
Abstract
Background
Crohn’s disease can cause strictures throughout the gastrointestinal tract. Endoscopic balloon dilatation is a well-established treatment, but recurrence is seen in up to three out of four cases. Infliximab is playing an increasingly important role in the modern systemic treatment of severe Crohn’s disease. Combining the anti-inflammatory effects of infliximab with the proven effect of endoscopic balloon dilatation could possibly improve outcome. In small studies, intralesional injections in perianal fistulas have been effective and endoscopic injection therapy in colonic strictures is feasible.
Objective
We wanted to assess whether serial intralesional injection of infliximab in small bowel strictures is feasible and reduces local inflammation.
Methods
We included six patients with Crohn’s disease and inflammatory small bowel strictures. They were treated with endoscopic serial balloon dilatation. Subsequent to each dilatation, 40 mg infliximab was injected submucosally. A modified simplified endoscopic score for Crohn’s disease was used for the involved area before the initial treatment and at the final follow-up after six months. Complications and development of symptoms were registered.
Results
Balloon dilatation and serial injection of infliximab were accomplished in five out of six patients. One patient completed the serial balloon dilatations and follow-up but received only one infliximab injection. The modified simplified endoscopic score for Crohn’s disease decreased in all patients. There were no adverse events registered and all patients described themselves as feeling well.
Conclusions
Combining balloon dilatation of strictures with serial intralesional injection of infliximab in Crohn’s disease of the small bowel is feasible and seems successful in reducing inflammation.
Introduction
Despite improved medical treatment, Crohn’s disease can cause strictures throughout the gastrointestinal (GI) tract and up to one-third of patients develop small bowel strictures. 1 Effective treatments are bowel resection of strictures or stricturoplasty. However, postoperative morbidity, i.e. bowel obstruction, anastomotic leak, wound infection and postoperative bleeding, is seen in 13–20% of patients and more than 50% of the patients will need recurrent surgery within 15 years due to new strictures.2–4 Repeated surgery may lead to short bowel syndrome and/or chronic obstruction because of adherences.5,6
Endoscopic balloon dilatation of Crohn strictures was introduced in the early 1990s and is now a well-established treatment with a complication rate of around 2% according to a meta-analysis. 7 Recurrence of strictures requiring a second dilatation is seen in 46% of patients.8,9 Efforts have been made to lower this rate including increasing the diameter of the balloon. In two series, a balloon enlargement lowered the relapse rate, but the number of intestinal perforations increased.10,11 In a placebo-controlled study, intralesional injections of corticosteroids in combination with balloon dilatation have been tried to reduce the inflammatory load but without significant effect. 12 Azathioprine has shown to reduce inflammatory changes at anastomotic sites, but the data available on optimizing medical treatment after endoscopic balloon dilatation are limited. 13
Biologics – including infliximab – are playing an increasingly important role in systemic treatment of severe Crohn’s disease and significance on efficacy is extensive.14,15 However, the effect of systemic infliximab in established stricturing disease is limited, leaving us with a challenging and heterogenic group of patients. 9 Small studies have shown effect of intralesional injections of infliximab in perianal fistulas in Crohn’s disease and endoscopic injection therapy in colonic strictures has also been shown to be possible.16–18 The feasibility and effect of serial infliximab injections in small bowel strictures have not been tested. Combining the long-term anti-inflammatory effects of infliximab with the immediate effect of endoscopic balloon dilatation could improve long-term outcome for patients with stricturing Crohn’s disease. This preliminary study aimed at testing the feasibility and effect of serial, intralesional injection of infliximab in combination with endoscopic balloon dilatation of small bowel strictures.
Methods
Six patients (one woman and five men) with long-standing Crohn’s disease, prior history of surgery due to strictures, active MRI- and endoscopy-verified inflammatory stricture, and recurrent symptoms of bowel obstruction were included into the study (Figure 1(a)). A patient synopsis is provided in the Appendix. Patients with fibrostenotic strictures without signs of inflammation endoscopically or at MRI and/or a previous history of systemic infliximab treatment were excluded. All patients were eligible for endoscopic balloon dilation according to the standard practice at our department and all patients had received two or more endoscopic balloon dilatations before enrollment in the study. No patients had multiple strictures and the length of the strictures was less than five cm. The study was approved by The Regional Committee on Biomedical Research Ethics (number H-D-2009-062) and the Danish Health and Medicines Authority. Written informed consent was obtained from all patients.
(a) Inflamed Crohn stricture located an ileocolic anastomosis. (b) Endoscopic submucosal injection of 10 mg of infliximab.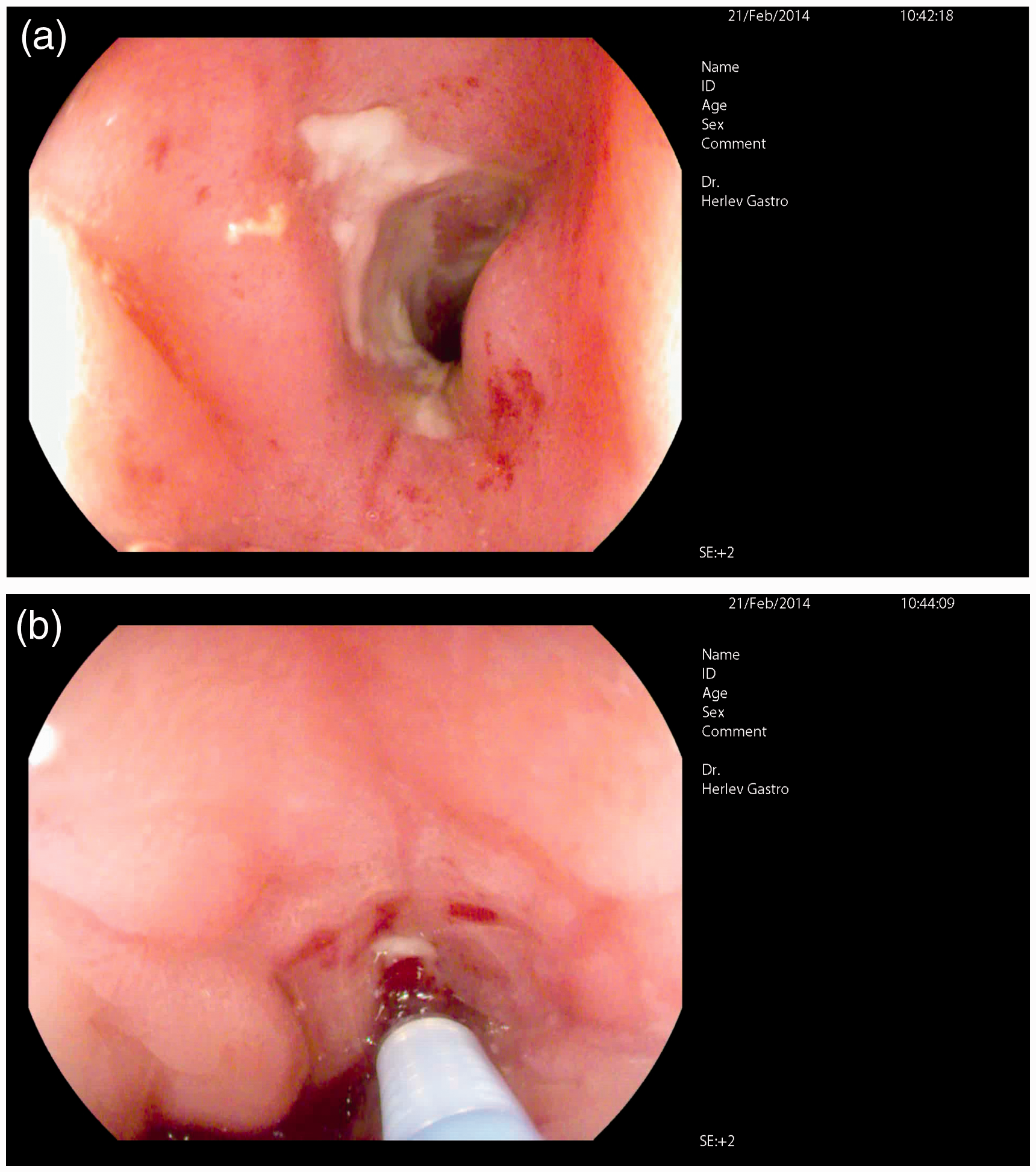
Patient demographics
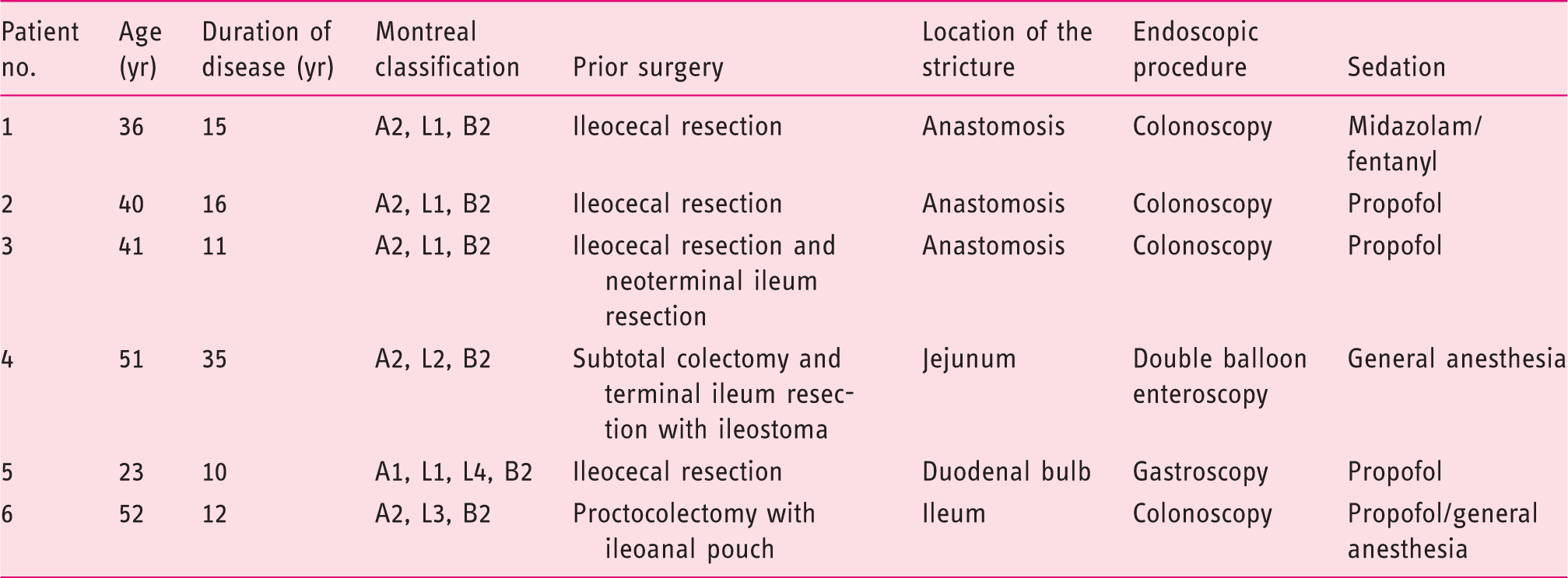
Choice of endoscopic procedure was based on localization of the lesion. Two patients were under general anesthesia, while the rest underwent conscious sedation with midazolam/fentanyl or propofol.
The patients were treated with endoscopic serial balloon dilatation of a small bowel stricture (0, 2, and 6 weeks), and subsequent to each dilatation 40 mg infliximab was injected submucosally into the medial part of the stricture in four quadrants (10 mg in each quadrant) of the stricture (Figures 1(b) and 2). The dosing chosen for this study was based on the available literature at the initiation of the study.16–18 The length of the strictures was relatively short being less than 5 cm and dilatation was performed until a diameter of 15–18 mm was reached. Inflation time at the maximal diameter was one minute. After the procedure the lesion was not passed by the endoscope.
Endoscopic balloon dilatation of a small bowel Crohn stricture.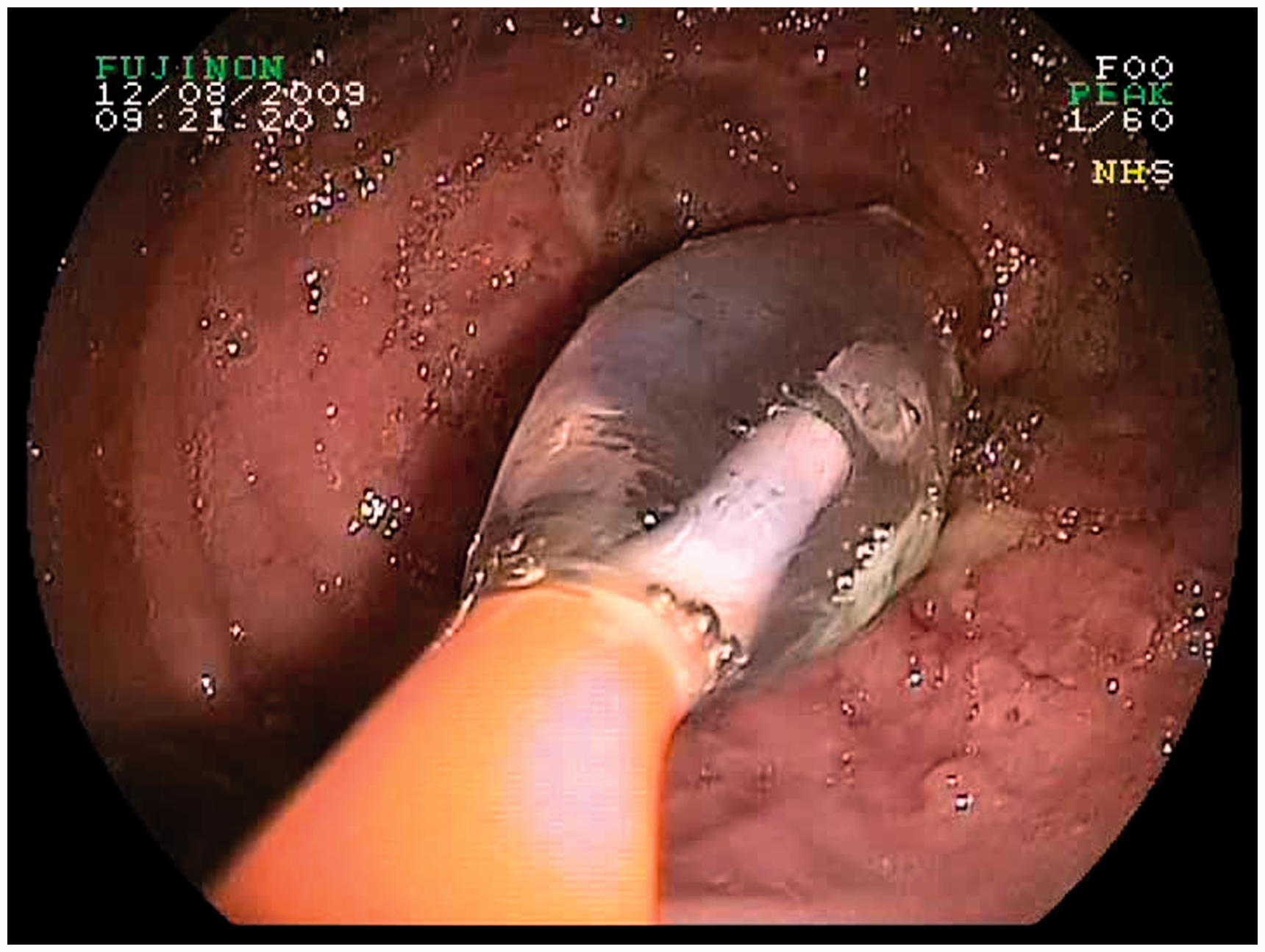
Modified simplified endoscopic score for Crohn’s disease before and after treatment
Results
In five out of six patients, serial balloon dilatation and serial injection of infliximab was accomplished. One patient was excluded from infliximab injections after one procedure due to positive HCV antibodies, but the serial balloon dilatation and follow-up assessment were completed. There were no complications registered. HCV is not a contraindication for systemic treatment with infliximab, but as this was a pilot study stricter safety rules applied.
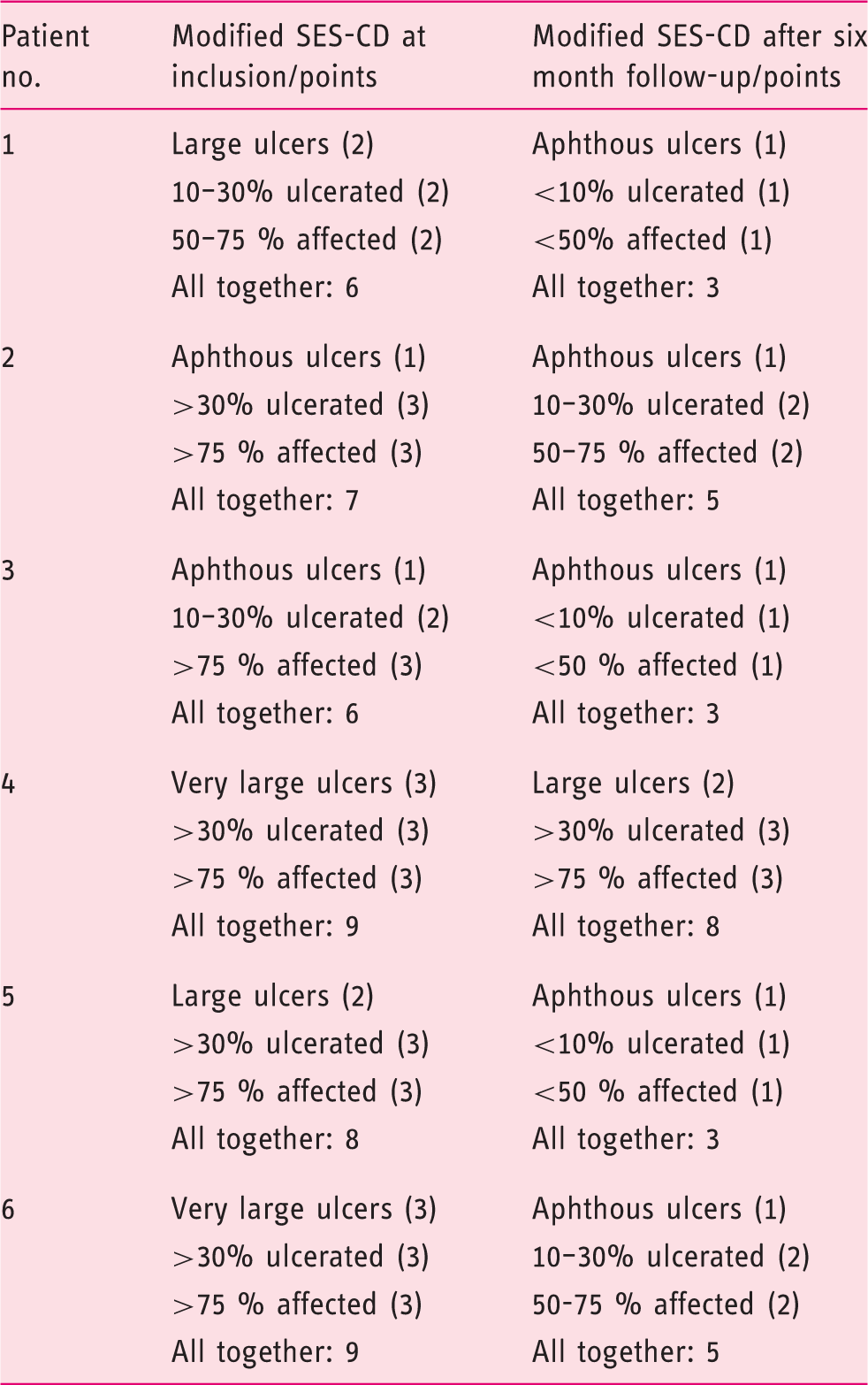
The modified SES-CD value decreased in all patients during the study by a mean of three points (one to five points) (Table 2 and Figure 3). The initial treatment was beneficial to all six patients and at the final follow-up at six months they all described relief of obstructive symptoms and no patients were referred to surgery during the follow-up period.
Modified simplified endoscopic score for Crohn’s disease before and after treatment. Size of ulcers (orange), extent of ulcerated surface (green), and proportion with other lesions (blue) are depicted.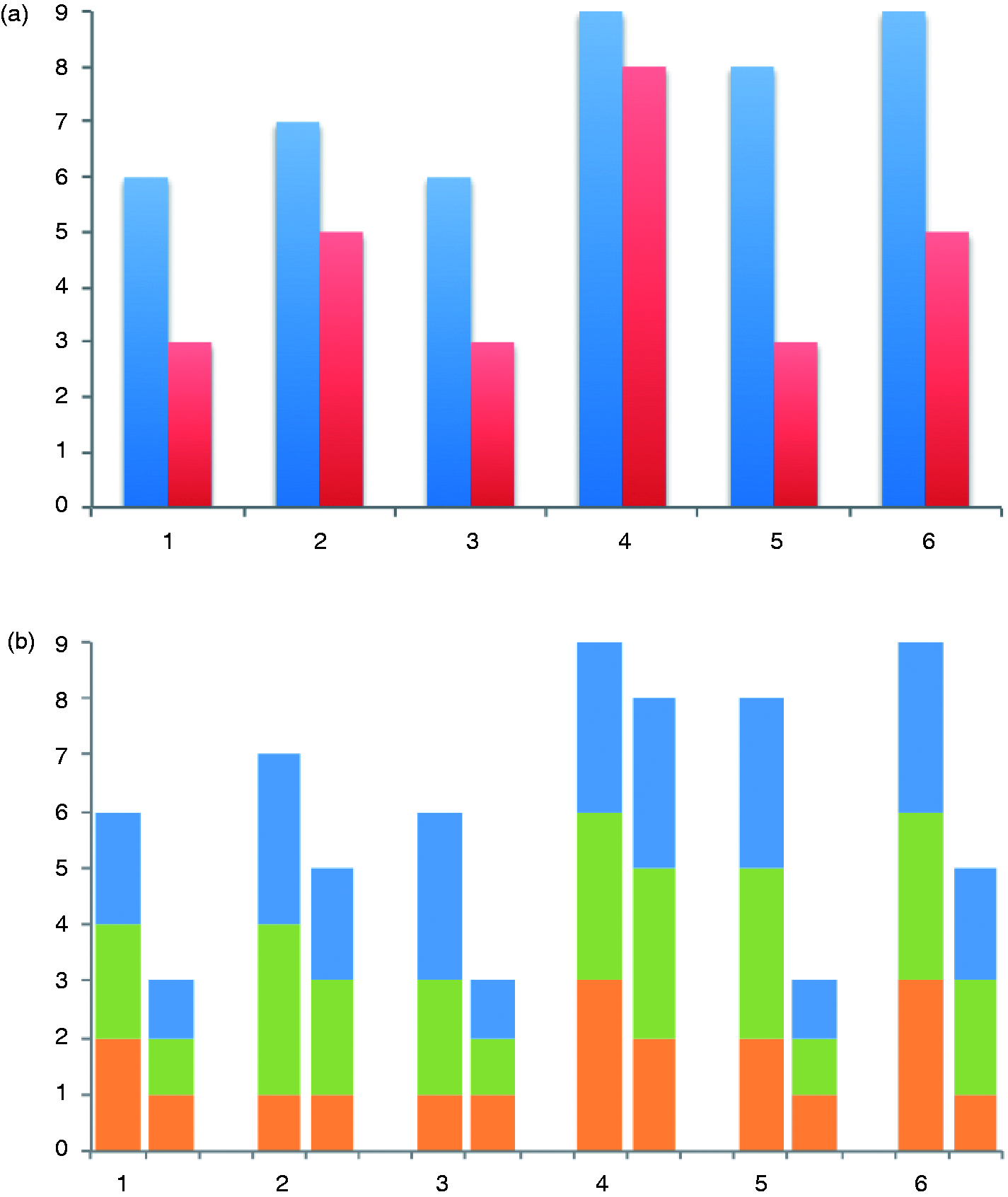
A case SP (number 1, Table 1) was a 36-year-old man with 15 years of Crohn’s disease. He had previously undergone ileocecal resection due to stricturing disease. During the last three years he had suffered intermittently from obstructive symptoms due to a recurring stricture located at the ileocolic anastomosis. It had been balloon dilated four times with no more than six month of symptomatic relief. Endoscopically, the stricture was severely inflamed with very large ulcerations involving more than 30% of circumference of the stricture and the extension of the inflammation was above 75%. Together his modified CD-SES score was nine. Otherwise the intestine was without signs of inflammation. After the serial balloon dilatation combined with intralesional infliximab injections his symptoms resolved and his modified CD-SES score dropped to five points. During the six-month follow-up there was no indication for re-dilatation.
Discussion
In this prospective case study we investigated the effect of serial infliximab injections combined with endoscopic balloon dilatation in inflamed small bowel Crohn strictures. We found the method to be feasible without adverse events and the procedure seemed to lower inflammation.
Medical treatment for Crohn’s disease has evolved rapidly in the last decades, especially with the introduction of the biological agents. 14 Infliximab – the first of these – is widely used and its effect is well established. Nevertheless, one in five patients develops bowel strictures, which often seem resistant to medication. 21 Surgical treatment with either bowel resections or stricturoplasty was the only treatment for bowel strictures until endoscopic balloon dilatation was shown to be a safe, minimally invasive alternative. 9 In selective patients without penetrating or fistulizing disease, the latter has now become the treatment of choice giving way to surgery only if the stricture is not amenable to endoscopic dilatation.
The primary drawback of endoscopic balloon dilatation of strictures is the high rate of recurrence.8,9 Repeated dilatation is clearly feasible and in some patients remains preferable to surgery. Nonetheless, minimizing this recurrence rate will certainly improve the value of endoscopic treatment. Several attempts to achieve this goal have been made including increasing balloon diameter. We inflated the balloon to a diameter of between 15 and 18 mm. As only small bowel strictures were included in the study, we routinely used a moderate diameter to minimize the risk of perforation. Couckuyt et al. found a positive correlation between passing the site of the lesion and symptomatic long-term relief. 11 However, complications have been reported as a result of advancing the scope past the site lesion. 22 In our clinic, we do not pass the site of the lesion unless we find it of diagnostic or therapeutic importance.
Intralesional steroid injections to reduce inflammatory load have been shown to be feasible and safe. However, a recent placebo controlled study failed to show convincing effect in relation to the number of relapses. 12 Combining colonic balloon dilatation with infliximab injections has been reported in a small study including three patients. The mean follow-up was 10 months and during this period no adverse reactions were described. Within two weeks the treatment led to endoscopic as well as clinical improvement. 18 Intralesional injections when treating perianal fistulas in Crohn’s disease have shown short-term effect.16–18 In conclusion, the anti-inflammatory effect and long-term results of local steroid injections are debatable. Our study was designed primarily to evaluate the feasibility and effect on intralesional inflammation, but during the follow-up no relapse was seen. Whether this was due to serial dilatations or infliximab injections remains unanswered.
In two small series with enteroscopic balloon dilatation of small bowel strictures using double balloon enteroscopy (DBE), the rate of success was around 80% and the number of complications reported were 1/9 and 0/8, respectively. During a mean follow-up of 10–21 months, 75% remained symptom free.23,24 Furthermore, small bowel dilatations of Crohn’s strictures are also feasible in pediatric patients. 25 Accordingly, it seems that not only is enteroscopic balloon dilatation of small bowel strictures in Crohn’s disease feasible and safe, it is also as efficient as colonic dilatations.23,24 We use DBE routinely in our clinic also in combination with balloon dilatation. 26 In the study one patient was treated using DBE; there were no complications related to these procedures.
In all patients, we registered a reduction in the modified SES-CD-index. Although, the results are preliminary, the combined treatment seems to lead towards a lower inflammatory load. Only one of six patients had concomitant treatment during the study (patient 5, azathioprine); hence, the decreased inflammation must be due to the local treatment. In Crohn’s disease, it seems that systemic treatment with anti-TNF inhibitors can reduce the risk of developing bowel strictures. The effect in patients with already known stricturing disease is more debatable, but a subset of patients will probably benefit from the treatment, wherefore systemic treatment can be tried before surgery or concomitant to endoscopic balloon treatment.27–32 None of the patients included is this study had previously received systemic infliximab treatment. Whether intralesional injections would have any synergistic effect on systemic responders remains unknown. The TNF-alpha antibody status and infliximab levels of the patients in our study were not examined after local injections, but it would be interesting to combine local and systemic infliximab treatment and correlate the effect with the presence of TNF-alpha antibodies. A plausible adverse event to local injections is formation of antibodies possibly taking away the opportunity of future systemic treatment. Future studies will have to address this problem and whether concomitant administration of immunomodulators can prevent antibody formation. In the study by Swaminath and Lichtiger, which showed benefits from combined intralesional injections and endoscopic balloon dilatation of colonic strictures, only one patient had responded to prior systemic infliximab infusions. 18
When using infliximab as systemic treatment for Crohn’s disease, initiation is by serial infusion in weeks 0, 2, and 6. We used precisely the same schedule introducing intralesional injection in combination with endoscopic balloon dilatation. To our knowledge, no studies have been conducted showing effect of either serial dilatations or serial infliximab injections. At the final follow-up at six months none of the patients had relapsed. Whether this finding can be maintained at a longer follow-up was beyond the scope of this study, but a prolonged effect without continued local injections would be unexpected. The medical regime after the serial dilatations was tailored individually: two patients not receiving anti-inflammatory treatments, one initiating methotrexate, and two beginning azathioprine. Additional analyses are needed to establish significance on how medical treatment is optimized after endoscopic balloon dilatations.
The main limitations in this study were the relatively small number of patients, the heterogeneously distributed location of the strictures in the small bowel, and the lack of a control group. These limitations call for further case/control or randomized trials to show whether serial intralesional infliximab injections improve the outcome of endoscopic balloon dilatation or whether serial balloon dilatation in itself can minimize the relapse rate in stricturing Crohn’s disease. Further, it would be interesting to compare single versus serial treatments. Future studies designed to evaluate if local infliximab injections will lower the need for re-dilations, should expand the follow-up period to at least one year – if possible longer.
In conclusion, combining balloon dilatation of strictures with serial intralesional injection of infliximab in Crohn’s disease of the small bowel is feasible. We speculate that it tends to lower the severity of the inflammation after six months, but larger and randomized studies should be undertaken before firm conclusions can be drawn. Currently, there is no firm evidence suggesting routine use of local infliximab treatment of Crohn’s strictures.
Footnotes
Funding
This work was supported by MSD Denmark.
Conflict of interest
The authors declare that there are no conflicts of interest.